Embed Size (px)
Citation preview

TUBERCULOSIS
DR.MUHAMMAD USAMA KHANHAMDARD UNIVERSITY
ISALAMABADPAKISTAN

Introduction
TB remains one of the most common causes of death amongst infectious diseases worldwide.
Despite the fact that Mycobacterium tuberculosis colonizes few hosts other than man and survives only briefly when isolated in the environment, efforts to eliminate the disease have failed to date.
TB has staged a comeback in the US and other parts of the world because of shifts in the population considered endemic for TB, healthcare policies changes, ↑ in the number of immunocompromised individuals, and development of drug resistance.

TB Burden 2012
8.6 million people fell ill with TB in 2012, including 1.1 million cases among people living with HIV
In 2012, 1.3million people died from TB, including 320000 among people who were HIV-positive

Epidemiology of TB Pakistan…
Tuberculosis (TB) is a massive public health problem and according to World Health Organization, (WHO) Pakistan ranks 5th in the countries having high disease burden.
It contributes 26% of avoidable deaths among adults and children in our country.
The present annual incidence of open TB cases is estimated to be between 231/100,000 persons and subsequently about 361,000 new cases of TB are added every year in Pakistan
http://data.worldbank.org/indicator/SH.TBS.INCD

Epidemiology of TB… Four out of 5 TB patients in Pakistan still remain
undetected, untreated and inadequately managed. One untreated or poorly treated “open case” of TB can
make 10-15 people more patients in a year’s time. Lack of proper diagnostic equipment and skills, irrational
prescription and non-availability of essential anti TB drugs are among the major contributing factors of various complications including emerging resistance.
Multi Drug Resistant TB is a contributing factor to increasing costs, mortality and duration of treatment.
A simple TB case management incurs a cost of 6000 rupees for the treatment of 9 months while a MDR TB case, which requires treatment for 2 years, costs about 300,000 rupees
Etiology of TBTB is caused by M. tuberculosis, an
aerobic, non-spore-forming bacillus. Also called Acid-fast bacillus (AFB).M. tuberculosis replicates slowly (q 24hrs)
(20-40 minutes with other organisms).M. tuberculosis thrive well in environment
where O2 tension is high such as renal parenchyma, growing ends of bones.

Mycobacterium species include:M. tuberculosis complex: M. tuberculosis, M. bovis, M. africanumMycobacteria other than tuberculosis: Around 15 are recognised as pathogenic to humans and some causepulmonary disease resembling TB. They have been foundin soil, milk and water. They are also referred to asatypical mycobacteria.Mycobacterium leprae: The cause of leprosy.
Pulmonary (respiratory) TBextrapulmonary (non-respiratory) TB.
Sites of extrapulmonary disease include the pleura, lymph nodes, pericardium, kidneys,meninges, bones and joints, larynx, skin, intestines, peritoneum and eyes.
Pulmonary TB may arise from exogenous reinfection or endogenous reactivation of a latent focus remaining from the initial infection.

Transmission Tubercle bacilli are transmitted through the air by
aerosolized droplet nuclei that are produced when a person with pulmonary or laryngeal TB coughs, sneezes, speaks, or sings.
Droplet nuclei may also be produced by other methods such as bronchoscopy, endotracheal intubation, processing of secretions in labs and hospitals.
The nuclei, which contains one to 3 M. tuberculosis organisms, are small enough to remain airborne for long periods of time and to reach the alveoli within the lungs when inhaled.

Transmission… Tubercle bacilli are not transmitted on inanimate
objects such as dishes, clothing, or beddings, and organisms deposited on skin or intact mucosa do not invade tissues.
Several factors influence the likelihood of transmission of M. tuberculosis, including the number of organisms expelled into the air, the length of time an exposed person breathes the
contaminated air, and presumably the immune status of the exposed
individual.

Transmission… Family household contacts, especially children, and
people working or living in an enclosed environment (hospitals, prisons, nursing homes) with an infected person are at increased risk.
Individuals with impaired cell-mediated immunity are thought to be more likely to become infected with M. tuberculosis after exposure than persons with normal immune functions.
Most effective means of reducing transmission is by treating infected patients with effective chemotherapy.
Pathophysiology of TBLatent Infection vs. Active Disease (TB).Upon inhalation, droplet nuclei settle into the
bronchioles and alveoli of the lungs.Development of infection in the lungs will
depend on virulence and other factors. Individuals with latent TB infections are not
infectious and cannot transmit the organisms.

Pathophysiology of TB… The extent of the disease produced by M. tuberculosis in
humans depends on the size of the inoculum of bacteria inhaled (most common route of acquisition) and the immune status of the host at the time of initial infection and at a later time.
If the patient is immunocompromised at the time of initial infection, the disease will more likely progress into bacterial pneumonia at the site of implantation, known as primary progressive disease.
In the remaining group whose immune system is competent, the infection will usually be halted after a brief period of bacillary dissemination.

Pathophysiology of TB… In individuals who inhale a massive inoculum of
organisms, however, clinical disease may occur despite an intact immune system.
In immunocompetent individuals, the 1º infection is held in check due to the development of T cell-mediated hypersensitivity that usually occurs 4-8 weeks after initial infection.
At this time, the patient will demonstrate a positive reaction to a TST, and any remaining viable organisms within the body will be walled off in caseating granulomas.

Pathophysiology of TB… 1/10 persons with symptomatic 1º infection will at
some later date develop active TB (reactivation disease) because the immune system fails to contain the organism.
This most often presents as pulmonary tuberculosis (PTB), although extrapulmonary tuberculosis (CNS, renal, hepatic, GI, skeletal) is not uncommon.

Diagnosis of Tuberculosis
The most common form of TB in adults is post-primary pulmonary tuberculosis (PTB).
Has great epidemiological significance.
Based on clinical, radiological and/or bacteriological evidence.

Signs & Symptoms of PTB
Persistent cough (more than 2 weeks).Cough with blood-stained sputum
(hemoptysis).Dyspnea, chest pain, hoarseness of voice.Fever with night sweats. Loss of weight and loss of appetite.
Signs & Symptoms of PTB…
Consolidation. Pulmonary fibrosis.Stony dullness caused by pleural effusion.

Signs & Symptoms of PTB…

Laboratory InvestigationsSputum direct smear for AFB (3 specimens).C&S using egg-based media.Chest X-ray often reveals lesions in the
apical and posterior segments of the upper lobes (soft, usually little or no fibrosis).
Mantoux Test (Tuberculin PPD Skin Test) has some role in diagnosis.

Laboratory InvestigationsErythrocyte Sedimentation Rate (ESR) has
little role and cannot be recommended for routine use in the diagnosis and follow-up evaluation of patients.
Techniques utilizing PCR can give rapid results, but are expensive.

Diagnosis of Extra-pulmonary TB
Due to lympho-hematogenous dissemination during 1º TB infection.
Symptoms are often non-specific: anorexia, fever, weight loss.
Specific features related to the organ involved.
TB lymphadenitis, GU TB, TB of joints and bones, miliary TB.
High Risk GroupContacts of sputum positive TB cases. Persons with HIV infections. Immigrants from countries with high
prevalence.Persons in institutions such as prison or drug
rehabilitation centers. Persons with other risk factors (DM, silicosis,
prolonged corticosteroids and immunosuppressive therapies).

Treatment of Active TB
A. GOALS OF TREATMENT Cure the individual to prevent morbidity and
mortality. Prevent relapse of the disease. Minimize transmission of M. tuberculosis. Prevent emergence of MDR-TB.

Treatment of Active TB
B. Essential First Line Drugs
i. Isoniazid, INH (H)
ii. Rifampicin (R)
iii. Pyrazinamide (Z)
iv. Streptomycin (S)
v. Ethambutol (E)




Reserve Second Line Drugs

Treatment of Active TB
C. DOTS Regimen Directly observed treatment (DOT) is an
important element in the internationally recommended policy package for TB control.
DOTS remains at the heart of the Stop TB Strategy.

Treatment of Active TB
C. DOTS Regimen Directly observed treatment means that an
observer watches the patient swallowing their tablets, in a way that is sensitive and supportive to the patient's needs.
This ensures that a TB patient takes the right antituberculosis drugs, in the right doses, at the right intervals.

Treatment of Active TB
C. DOTS RegimenThe five elements of DOTS: Political commitment with increased and sustained
financing. Case detection through quality-assured bacteriology. Standardized treatment, with supervision and patient
support. An effective drug supply and management system. Monitoring and evaluation system, and impact
measurement.

Treatment of Active TB
D. Treatment Regimens Effective treatment of TB requires substantial
period (minimum 6 months) of intensive drug therapy with at least two (2) bactericidal drugs that are active against the organism.
The initial phase of treatment is crucial for preventing the emergence of resistance and for ultimate outcomes of therapy.

Treatment of Active TB
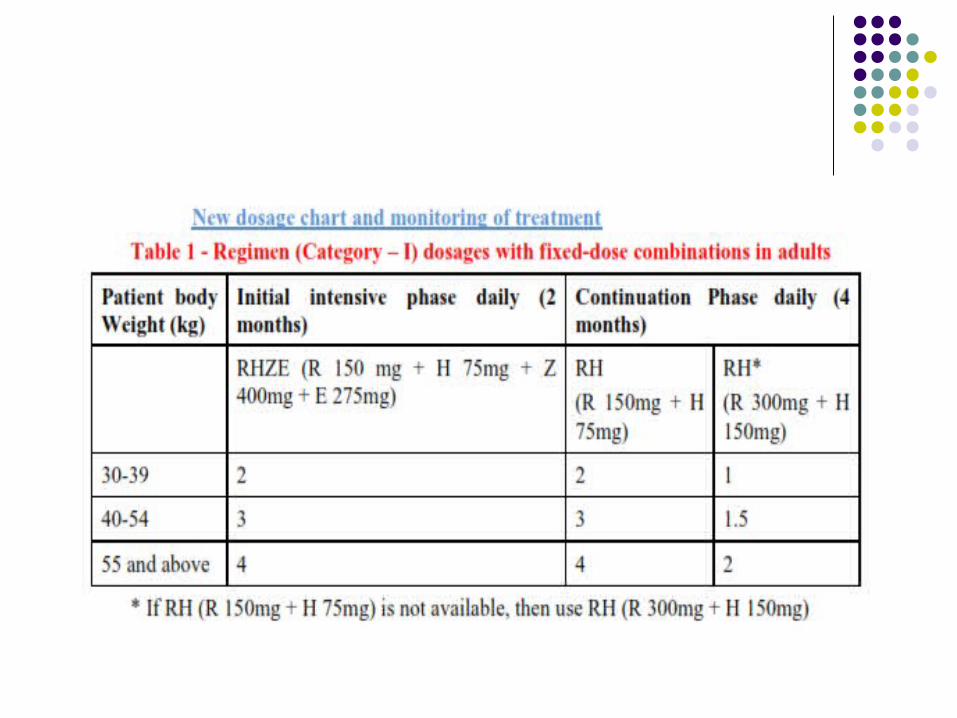
D. Treatment Regimens The course of treatment is divided into: Initial
(Intensive) Phase and the Continuation (Maintenance) Phase.
The 2-month Intensive Phase with 3 or 4 drugs is to rapidly convert the sputum and improve clinical symptoms.
The 4-month Continuation Phase with 2 or 3 drugs has a sterilizing effect to eliminate the remaining bacilli and prevent relapse.


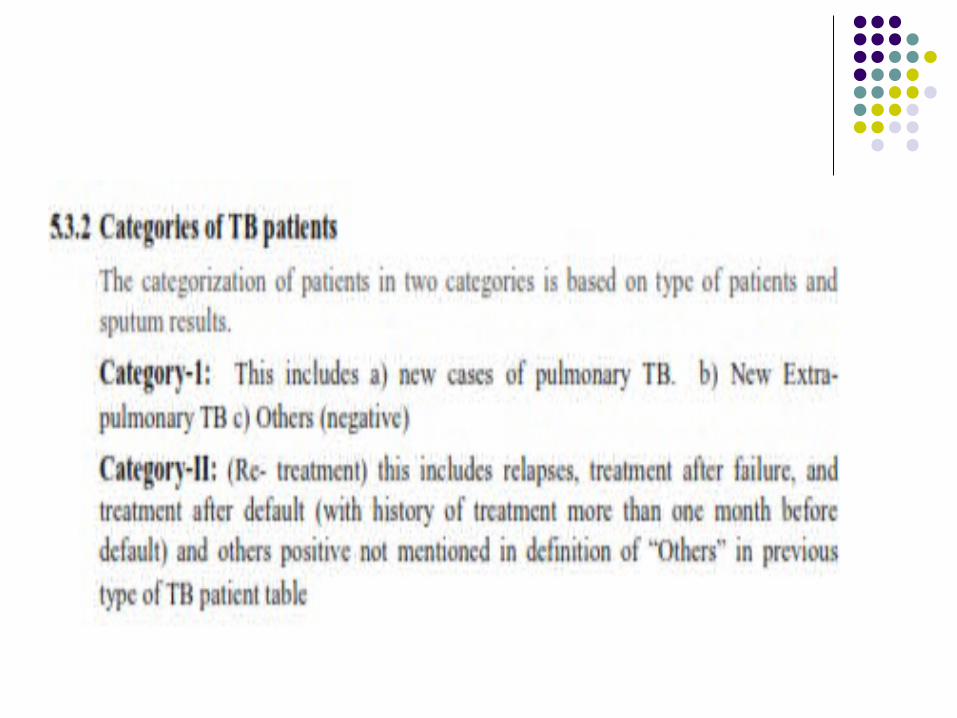
Type of TB patients
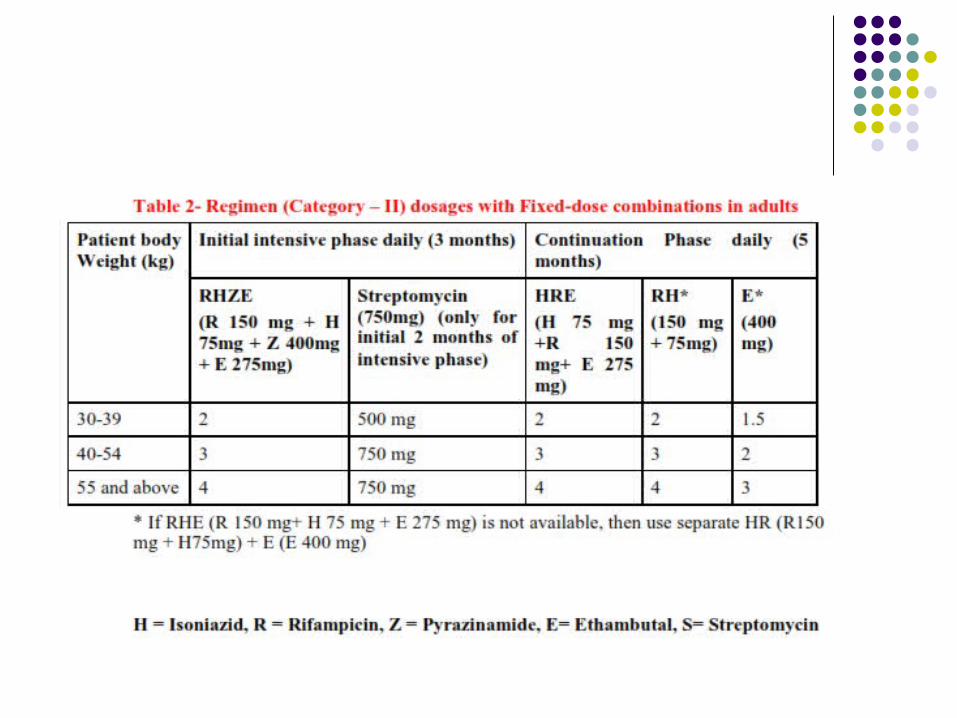

Category II: Treatment Failure, Relapse, Treatment after Default
DO NOT initiate conventional therapy as above. Send sputum sample for C &S. Refer case to Respiratory or Chest Physician. Treatment should be based on C&S results and
clinical response.

Category III: Chronic Case DO NOT initiate conventional therapy as above. Send sputum sample for C &S. Refer case to Respiratory or Chest Physician. Treatment should be based on C&S results and
clinical response.
Drug and Multidrug-Resistant TB (MDR-TB)
Anti-tuberculosis (TB) drug resistance is a major public health problem that threatens the success of DOTS.
MDR-TB is a specific form of drug-resistant TB due to a bacillus resistant to at least isoniazid and rifampicin, the two most powerful anti-TB drugs.
“MDR-TB” is not synonymous to “Chronic TB”.MDR-TB patients respond poorly to shortcourse
chemotherapy and need to be treated intensively and for up to 24 months with a regimen based on reserve antituberculosis drugs…

Therapeutic Options IN HIV/AIDS
Isoniazid, rifampin, pyrazinamide, and ethambutol for 2 months (daily or 5x/week), followed by isoniazid and rifampin for 4 months (daily, 5x/week, or 3x/week).
Alternatively, isoniazid, rifampin, and ethambutol for 2 months (daily or 5x/week), followed by isoniazid and rifampin for 7 months (daily or 5x/week)

Case M.W., a 36-year-old woman, is admitted to the hospital with a 2-month
history of cough, which has recently become productive. She is also experiencing fatigue, night sweats, and has lost 15 pounds. Other medical problems include diabetes mellitus, which is controlled with 10 units of NPH insulin daily, and poor nutritional status secondary to frequent dieting. M.W. works as a volunteer in a nursing home several days a week. Recently, it was discovered that two patients who she had been caring for had undiagnosed active tuberculosis.
M.W.'s physical examination was normal, but her chest radiograph revealed bibasilar infiltrates. A tuberculin purified protein derivative (PPD) skin test, sputum collections for cultures and susceptibility testing, and a sputum AFB smear were ordered as part of M.W.'s diagnostic workup. Initial laboratory test findings were within normal limits.
The result of her tuberculin PPD skin test, read at 48 hours, was a palpable induration of 14 mm. Her sputum smear was positive for AFB, and additional sputum cultures for M. tuberculosis were ordered to confirm the diagnosis of active TB disease.

Q. 1. What subjective and objective findings does M.W. have that are consistent with active TB disease?
Subjective Findings: M.W.'s history of cough (which gradually became productive),
bibasilar infiltrates, fatigue, and night sweats are consistent with the classic symptoms of active TB.
The cough may be nonproductive early in the course of the illness, but with subsequent inflammation and tissue necrosis, sputum is usually produced and is key to most of the diagnostic studies.
Anorexia from TB, along with frequent dieting, may have resulted in M.W.'s weight loss. Other symptoms of TB can include fever, pleuritic pain secondary to inflammation of lung parenchyma adjacent to the pleural space, and general malaise. Dyspnea is unusual unless there is extensive disease.

Objective Findings: M.W. has a chest radiograph consistent with a lower respiratory
tract infection. In pulmonary TB, nodular infiltrates are usually found in the apical or posterior segments of the upper lobes, but markings may be found in any segment.
M.W. also has a positive sputum smear for AFB, a positive PPD skin test (14 mm), and diabetes mellitus, which is a risk factor for TB. Although her laboratory test results are within normal limits, peripheral blood leukocytosis and anemia are the most common hematologic manifestations of TB.18 The white blood cell count is normal or slightly increased, and an increase in monocytes and eosinophils may be observed.

Q.2. What is tuberculin skin testing? How should
the results be interpreted in M.W.? Ans. 2. The tuberculin skin test (Mantoux method) has been used as a
diagnostic tool for infection with M. tuberculosis for decades, but a positive skin test is not necessary for the diagnosis of active TB disease.
The test is frequently referred to as the PPD test, which contains a protein prepared from a culture of the tubercle bacilli. The skin test is performed by injecting 0.1 mL of solution containing 5-TU PPD intracutaneously into the volar or dorsal surface of the forearm.
An induration ≥5 mm in diameter read 48 to 72 hours after injection is considered to be a positive reaction in an individual with a recent history of close contact with a person with active TB.
An induration ≥10 mm in diameter is considered to be a positive reaction in persons with clinical conditions that put them at increased risk for TB, such as diabetes mellitus, silicosis, chronic renal failure, malnutrition, leukemia, lymphoma, gastrectomy, jejunoileal bypass, and weight loss of >10% of ideal body weight.

Q. 3 Because M.W.'s Mantoux PPD skin test is positive, does this confirm her diagnosis of active TB?
Ans. 3 No. M.W.'s positive reaction to 5-TU PPD alone does not
confirm active TB disease. It merely signifies that she has previously been infected
with M. tuberculosis. To confirm the diagnosis of active TB disease in M.W. and other patients, M. tuberculosis must be isolated from sputum, gastric aspirate, spinal fluid, urine, or tissue biopsy, depending on the site of infection

Q.4. How should treatment be initiated in M.W pending the
results of the sputum culture and sensitivity?
Ans. 4 INH 5mg/kg max 300mg Rifampacin 600 mg Ethambutal 15-25 mg/kg/day Pyrazinamide 15-50 mg /kg/day

Q.5. What are the monitoring parameters for M.W therapy?
Ans.5 ESR Blood CP LFT’s Fundoscopic examination Extremities Urine

Q.6 What are the possible side effects of ATT treatment INH: GI Intolerance: -Nausea, abdominal pain common-Vomiting less common, Peripheral
neuropathy: -dose-related -<0.2% will have, rash, Hepatitis -10-20% of persons who take isoniazid will develop asymptomatic LFT increase -In most cases these will resolve with continued treatment
Rifampacin: GI side effects • Orange urine/body fluids (sweat) -harmless but may stain contact lenses, clothing-need to let patients know beforehand Hepatitis: -occurs in about 0.6% of patients, flu like syndrome
Pyrazinamide—Side Effects • GI symptoms • Arthralgias (joint pain) •Rash • Hyperuricemia (elevated uric acid) uric acid) -usually asymptomatic -may precipitate gout, kidney stones -TB medications do not usually require discontinuation Hepatitis dose related

Ethambutol— Side Effects • Optic neuritis:-blurred vision -”spots” in patient’s field of vision-red/green
color blindness• Dose related Dose related • Uncommon with intermittent tx • Drug should be discontinued • Usually reversible if stopped right away