Embed Size (px)
Citation preview

Biomechanics of the Distal Radioulnar Joint
ANDREW K. PALMER, M.D.,* AND FREDERICK W. WERNER, M. MECH. ENG.**
The distal radioulnar joint is an intricate part ofwrist function. The radius and hand move in relationto, and function about, the distal ulna. Significantloads are transmitted to the forearm unit throughthe distal ulna via the triangular fibrocartilage. Theanatomic relations between the distal radius andulna and the ulnar carpus are precise, and evenminor modifications in these relations leads to sig-nificant load-pattern changes. The authors can onlyspeculate on the clinical ramifications of such load-pattern modifications. Since M. DeSault’s disser-tation on dislocation of the distal radius, publishedin 1791, much has been written on injuries to, andafflictions of, the radiocarpal area. Although injuriesand afflictions in this area undoubtedly have notchanged throughout the years, an increasing varietyof ulnar wrist syndromes and treatment programsare being recognized. This phenomenon attests notonly to the need for continuous investigations ofwrist problems but also to the great excitement thatpresently exists in the field. Better understandingof the anatomy and newer knowledge of the bio-mechanics of the distal radioulnar joint should her-ald an ulnar wrist renaissance.
Primate evolution has been characterizedby an increase in mobility of the hand. Thisincreased mobility is the result of two majorskeletal modifications: (1) gradual withdrawal
of the ulna from its primitive articulation, withthe pisiform and triquetrum resulting in in-
creased hand adduction and (2) the establish-ment of an ulnar head articulation with thedistal radius, with the inferior radioulnar jointresulting in enhanced pronation and suN-nation.’5
t-’rom a functional point of view, Milcht8
believes that the wrist is a compound jointcomposed of the radiocarpal, the intercarpal,the meniscal carpal, and the radioulnar joints.
In l~his complicated apparatus, the ulnar headfoFms the pivotal point in relation to whichthe normal position of other bony landmarksare determinecl and about which all motionsof the wrist are believed to occur. Essential toan understanding of the wrist joint proper isa clear understanding of the distal radioulnar
joint. A thorou.gh understanding of the normalfun~ction of the distal radioulnar joint is es-sential to any evaluation of distal radioulnarand perhaps radiocarpal and intercarpal dys-function. Sucih an understanding can resultfrom an integration of the pertinent anatomy
and bidmechanics of this area. /
From the Department of Orthopedic Surgery, The StateUniversity of New York, Upstate Medical Center, Syra-cuse, New York.
* Associate Professor of Orthopedic Surgery, State Uni=versify Hospital, Upstate Medical Center, Syracuse, NewYork.
** Assistant Frofessor of Orthopedic Surgery, StateUniversity Hospital, Upstate Medical Center, Syracuse,New York.
Reprint requests to Andrew K. Palmer, M.D., De-partment of Orthopedic Surgery, State University of NewYork, Upstate Medical Center, 750 East Adams Street,Syracuse, NY 13210.
Received: June 28, 1983.
ANATOMY
qThe distal ulna is covered with articular
cartilage over its most dorsal, volar, and radialaspects where it articulates with the sigmoidor ulnar notch, of the radius (Fig. 1). Distally,beneath the Wiangular fibrocartilage complex(TFCC), the ulnar head is also covered witharticular cartilage (Fig. 2).
Descriptions of the ligamentous anatomyabc)ut the di~al radioulnar joint have histor-
El
(ben,TFC

Joint
H. ENG.**
articulation, with¯ resulting in in-(2) the estabtish-ulation with the’ radioulnar jointation and supi-
~f view, Milch~szompound joint. the intercarpal,adioulnar joints.~, the ulnar head:lation to whichbony landmarkshich all motions~cur. Essential to,t joint proper is~istal radioulnarng of the normal:lnar joint is es-listal radioulnarintercarpal dys-Lding can resultrtinent anatomyao
t with articular¢olar, and radialith the sigmoidFig. 1). Distally,.rtilage complex;o covered with
ntous anatomyint have histor-
Numb~¢ 187July/August, 1984
FIG. 1. The distal radial ulnar joint involves thearticulation &the sigmoid notch (sn) of the radiusand the ulnar head.
FIG. 2. The ulnar head is covered with articularcartilage on its dorsal, radial, palmar, and distal(beneath the triangular fibrocartilage complex--.TFCC) surfaces.
Biomechanics of Distal Radioulnar Joint 27
R
FIG. 3. The component parts of the TFCC: themeniszus homalog (MH), prestyloid recess, articulardisc (AD), ulnar collateral ligament (UCL), radiou.lnar ligaments (RUL). H -- hamate; = capi.tate; TZ = trapezoid; TP = trapezium; S= scaphoid; L = lunate; TQ = triquetmm; R = ra-dius; U = ulna. (Reprinted with permission fromPalmer, A. K., and Werner, F. W.: The triangularfibrocartilage complex of the wrist~Anatomy andfunctidn. J. Hand Surg. 6:153, 1981.)
ically been conflasing,t.3,5.t4A6-|9,2t,22,24,26,28-DO
The triangular fibrocarfilage complex is a termthat has been introduced by Palmer and Wer-
,neras to describe the ligamentous and carti-laginous structure that suspends the distal ra-dius and ulnar carpus from the distal ulna.The TFCC incorporates the poorly definabledorsal and volar radioulnar ligaments, the ul-nar collateral ligament, and the meniscushomaJlog, as well as the clearly definable ar-ticular disc and extensor carpi ulnaris sheath(Fig. 3). The complex arises from the ulnaraspect of the lunate fossa of the radius (Fig.4). It courses toward the ulna, where it willinsert :into the caput ulna and base of the ulnarstyloid. It flows distally (joined by fibers arising

28 Palmer and WemerClinical OrI~opae~ics
an~l Relate<~ Researctl
FIG. 4. The triangular fibrocarfilage complex(TFCC) suspends the radius and carpus above thedistal ulna. T = triquetrum; L = lunate; S = scaph-oid. (Reprinted with permission from Palmer,A. K., and Werner, F. W.: The triangular fibro-cartilage complex of the wrist--Anatomy andfunction. J. Hand Surg. 6:153, 1981.)
from about the ulnar aspect of the ulnar sty-loid--the ulnar collateral ligament), becomesthickened (the meniscus homalog), and insertsdistally into the triquetrum, hamate, and baseof the fifth metacarpal (Fig. 4). The dorsal andvolar aspects of the horizontal portion of 1:heTFCC are thickened (average, 4-5 mm). Theauthors believe that these thickenings repre-sent the dorsal and volar radioulnar ligaments(Fig. 5).
Dorsally there is weak attachment of theTFCC to the carpus, except dorsal laterally,where the complex incorporates the floor ofthe sheath of the extensor carpi ulnaris (Fig.6). Volarly, the TFCC is very strongly attached
to the lunotriquetral interosseous ligament andthe triquetrum (the ulnotriquetral ligament),with weaker inconstant attachments to the lu-nate (the ulnolunate ligament), hamate, andbase of the fifth metacarpal (Fig. 6).
BIOMECHANICS
KINEMATICS
Forearm rotation of up to 150° occurs atthe distal radioulnar joint with the distal radiusand iits fixed distal member (the hand) rotatingabout the ulnar head.~-8"29 The ulnar head isnot, as once thought, immobile during rota-tion &the forearm. Modest lateral movementof the ulnar head, in a direction opposite tothat taken by the distal radius, of up to 8° or
~ CAPtTATE
FiG. 5. Lateral section of the wrist showing theTFCC to be thinned in its midportion between thelunate and ulna and thickened both dorsally andpalmarly. (Reprinted with permission from Palmer,A. K., and Wemer, F. W.: The triangular fibro-cartilage complex of the wrist--Anatomy andfun(nion. J. Hand Surg. 6:153, 1981.)

ClinicalanO Re~ate(~ Reseatctl
osseous ligament andtriquetral ligament),ttachments to the lu-:ment), hamate, andpal (Fig. 6).
~,NICS
tICS
p to 150° occurs at¯ ~th the distal radius~r (the hand) rotating9 The ulnar head is
mobile during rota-~st lateral movementirection opposite totdius, of up to 8° or
the wrist showing theidportion between thezed both dorsally and:mission from Palmer,The triangular fibro-wrist--Anatomy and~3, 1981.)
Number 187July/August. 1984
9° during pronation and supination has beendemonstrated by Ray et al. 27 Bunnell3 andothers26’28"3° have shown that the head of theulna moves slightly dorsally in pronation andslightly toward the palm in supination. Theauthors have shown that the ulnar head movesdistally in relation to the distal radius in pro-nation and proximally in supination, thus al-tering apparent ulnar variance.22
In summary, the radius rotates about thedistal ulna during forearm rotation as theforearm axis moves laterally in space.5’2°’27 Theulnar head normally glides in the sigmoidnotch of the radius from a dorsal distal po-sition to a volar proximal position as the fbre-
FIG. 6. Lateral section of the wrist showing weakattachment of the TFCC dorsally to the sheath, ofthe extensor carpi ulnaris (ECU) and triquetrum(TRIQ), and strong palmar attachment to the tri-quetrum. Also shown are the pisiform (PIS) andhamate (HAM). (Reprinted with permission fi:omPalmer, A. K., and Werner, F. W.: The triangularfibrocartilage complex of the wrist--Anatomy andfunction. J. Hand Surg. 6:153, 1981.)
Biomechanics of Distal Radioulnar Joint 29
]FIG. 7. The forearm is fixed in neutral rotationand the wrist is stabilized (third metacarpal pin)with loads of 22.5 N (5 Ibs) applied to the extensorand flexor tendons. Miniature load cells have beencentered in the midaspects of the radius and ulnafor measuring axial loads. (Reprinted with per-mission from Palmer, A. K., and Werner, F. W.:The triangular fibrocartilage complex of the wrist~Anatomy and function. J. Hand Surg. 6:153, 1981.)
ar-m moves from full pronation into full su-pir~ation.
KINETICS
The loads borne l~y the normal wrist jointduring activities of daily living are not knownbut are presumed to be great. Brand et al.~
have calculated that the potential tension-pro-ducing force of muscles of the arm is ap-proximately 500 kg. To evaluate the role ofthe: distal ulna and TFCC in this load trans-mission, the authors originally studied five

3O Palmer and Werner
TABLE 1. Axial Load Borne by theRadius and Ulna as a Percent of the
Total Load ( 100%)w 1981 Data*
TFCC Distal UlnaIntact Excised Excised
Radius 60% 95% 100%Ulna 40% 5% 0%
" (Reprinted with permission from Palmer, A.K.. andWerner. F.W.: The triangular fibrocartilage complex ofthe wrist--Anatomy and function. J. Hand Surg. 6:153,1981.)
forearms."-5 In this study, the forearms werefixed in neutral forearm rotation, radioulnardeviation, and flexion and extension. Min-iature load ceils were implanted in the mid-aspect of the radius and ulna and a fixed load(22.2 N) was simultaneously applied through
the ~vrist motors (Fig. 7). The axial loads, transmitted by the radius and ulna, were thensimultaneously recorded in the intact wrist,with the TFCC excised and with the distalulna excised. Table 1 represents the results ofthis study as recorded in 1981.
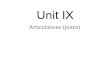
In response to critiques of the authors’ data,the authors modified their experimentalmodel,a Their present model involves the useof fresh cadaver upper extremities with pre-served elbows, which allows for simultaneousforearm rotation and wrist loading (Fig. 8).Improved load ceils that more accuratelymeasure the load applied at the distal radioul-nat joint are now used. Table 2 gives the resultsof furtlher loading experiments on 16 speci-mens with the authors’ new experimentalmodel. This new data more accurately rep-resents the loads borne by the TFCC and distalulna.
FIG. 8. A cadaver upper extremity is mounted such that forearm rotation is preserved. Load cells (LC)are mounted in the distal radius and ulna and load is applied via the wrist motors.

The axial loads, asand ulna, were thenin the intact wrist,and with the distal"esents the results of1981.ofthe authors’ data,their experimental~del involves the use.~tremities with pre-ws for simultaneousist loading (Fig. 8).~t more accuratelyat the distal radioul-ble 2 gives the resultsments on 16 speci-new experimental
lore accurately rep-the TFCC and distal
Number 187July/August, 1984 Biomechanics of Distal Radioulnar Joint 31
TABLE 2. Axial Load Borne by the Radiusand Ulna as a Percent of the Total Load
(100%). 1983 Data Utilizing RevisedExperimental Model (Fig. 8)
TFCC Distal UlnaIntact Excised Excised
Radius 81.6% 93.8% 100%Ulna 18.4% 6.2% 0%
Approximately 82% of the load applied inthe experimental model is borne by the distalradius and 18% by the distal ulna. Removalof the TFCC decreased the load borne big thedistal ulna by approximately 12% and rernovalof the distal ulna totally unloads the distalulna. Furthermore, the authors have shownthat radial deviation of the wrist decre.asedand ulnar deviation increased the load borneby the ulna.3z
In summary,, this data suggests that the ra-dius, through its articulation with the lateralcarpus, carries approximately 80% of the ,axialload of the forearm, and the ulna, through itsarticulation with the medial carpus (via theTFCC), 20%. Changes in the forearm wristunit as might be seen when the TFCC is, ex-cised or the distal ulna excised (Darrach pro-cedure) could be expected to dramatically andunphysiologically increase radial loading.
ULNAR VARIANCE
Ulnar lengthening or radial shortening isnow commonly used in the treatment ~f
FIG. 9. Shortening ofthe ulna by 2.5 mm result,,;in a drop in ulnar load to 4%. Lengthening of theulna by 2.5 mm results in an increase in ulnar loadto 42%. Similar, though less dramatic, changes areseen in wrists tested after the TFCC has been re.-moved.
Kienb6ck’s disease, and ulnar shortening isused in the treatment of degenerative perfo-.rations of the TFCC.~’-’3 To evaluate these sur-..gical procedures, the effect of ulnar length-.ening and shortening on forearm load trans-mission has been studied with a similarexperimental model to that used for the au-thors’ previous load studies.3z The load borneby the..ulna was measured as the ulna waslengthened by 2.5 mm at 0.5-mm incrementsand shortened by 2.5 mm at 0.5-mm incre-m.ents. Changes in the length of the ulna re-sulted in dramatic changes in the force borneby the distal ulna (Fig. 9). Ulnar shorteningof 2.5 mm resulted in a drop of the forcebprne by the distal ulna from an average of18% of the total force to 4%. Ulnar lengtheningof 2.5 mm resulted in an increase in the forceborne by the distal ulna to 42% of the totalforearm force (Table 3). A similar, though lessdramatic, variation in the force borne by thedistal ulna was seen .when the ulna was short-
TABLE 3. Percent Axial Load Borne by the Radius and Ulna as the Ulna is Lengthenedand Shortened in the Intact Wrist and in the Wrist after TFCC Excision
Ulnar Length Variation
Intact TFCC Excised
~’ i:~ - ’~."-2.5 tara 0 +2.5 mm -2.5 ram 0 +2.5 ram
~ " "~: Ulna4.3% 18.4% 41.9% 3% 6.2% 21.8%

32 Palmer and Werner
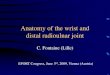
Pressure ~ ~Sensitive ~Film
FIG. 10. An illustration of Fuji pressure sensitivefilm being inserted into the radioulnar carpal joint.Two registration pins are present on the distal radialarticular surface. H = hamate; C = capitate; Td= trapezoid; Tm = trapezium; S = scaphoid; L= lunate; T = triquetrum; P = pisiform; R = radius;U = ulna.
ened and lengthened in the wrist where,’ theTFCC had been surgically removed (Tab]re 3).
LOAD DISTRIBUTION
In a continuation of this work, the actualpressures between the articular surfaces of theradius and ulna (TFCC) and the carpus ihave
been measured, by the use of Fuji PrescalePressure Sensitive Film (PSF).31 Figure 10 il..lustrates the orientation of the PSF within the:wrist after access to the joint was gained viaa dorsal incision. The average maximum.pressures developed at three locations for threeulnar lengths in six fresh specimens are givenir, t Table 4. These locations are the articulation.between the ulna and lunate, the radius andlunate, and the radius and scaphoid. As canbe seen, lengthening of the ulna produces adramatic increase in pressure on the ulnar
head (the ulnolunate articulation). This con-.fi~rms the authors’ previous data on ulnarlengthening and ulnar load transmission. Re-.moval of the TFCC causes a shifting of pres-.sure centrally to the radiolunate articulation,thus unloading not only the ulnolunate butthe radioscaphoid articulation.
In summary., this data illustrates that smallchanges in relative ulnar length significantlyalter toad patterns across the wrist. Thus, whena Colles’ fracture settles 2.5 mm, one can ex-pect an increase in ulnar axial load of ap-proximately 40%. Development of these ab-normal load patterns, the authors believe,greatly increases the risks of secondary de-generative arthrosis at the contact stress point.
DISTAL ULNAR STABILITY
No one would argue that the extensor ret-inaculum, the pronator quadratus, a--~d the
TABLE 4. Peak Articular Pressure (l~/mmz) at the Ulnolunate, Radiolunate, andRadioscaphoid Articulation in the Intact Wrist and in the Wrist after TFCC Excision,
with Ulnar Length Variations, ~s Measured with Fuji Pressure Sensitive Film
Ulnolunate Radiolunate Radius-ScaphoidArticulation Articulation A rticulation
Intact0 1.4 3.0 3.3
+2.5 mm 3.3 1.5 3.4-2.5 mm 0.34 4.1 3.6
TFCC Removed0 0.76 3.9 2.4
+2.5 mm 3.2 3.4 3.6-2.5 mm 0.0 3.9 2.5

:" Fuji Prescale~t Figure 10 il-
PSF within thewas gained viatge maximumations for threemens are giventhe articulationthe radius andapho.id. As cantna produces a; on the ulnarion). This con-data on ulnarmsmission. Re-;hifting of pres-tte articulation,ulnolunate but
I.
:rates that small,,th significantlyrist. Thus, whenlm, one can ex-:ial load of ap-mt of these ab-mthors believe,r secondary de-tact stress point.
ABILITY
:he extensor ret-dratus, and the
unate, and3C Excision,.ve Film
~s-Scaphoid:iculation
3.33.43.6
2.43.62.5
Nurn0~" 187July/August, 1984 Biomecllanics of Distal Radioulnar Joint 33
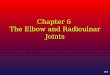
geometry of the sigmoid notch of the radiuscontribute to the stability of the distal ra-dioulnar joint, but the role that the dorsal andvolar radioulnar ligaments, the triangular fi-brocartilage, and/or the ulnar collateral liga-ment play in stabilizing this joint is contro-versial. The authors believe that the dorsaland volar radioulnar ligaments, the triangularfibrocartilage, and the ulnar collateral liga-ments are not anatomically separable struc-tures, so the previous statement appears to bea moot point. In order to study the role thatthe entire complex (the TFCC) plays in sta-bilizing the distal radioulnar joint, a biome-chanical study that evaluated the effect of theTFCC on dorsal, palmar, and lateral distalulna stability was undertaken.25 Each wrist:was evaluated in neutral forearm rotation, 75°
of pronation, and 75 o of supination after ap-,plying a 44.5-N load to the distal ulna (Fig.,11). Table 5 expresses the authors’ data aspercent displacement toward dislocation of thedistal ulna in the intact wrist and after se-.quentially cutting the pronator quadratus, the;capsule, and finally the TFCC. Table 6 ex..presses .the authors’ data from a similar ex.-periment on lateral displacement of the distalulna in the intact wrist and after division ofthe TFCC, capsule, pronator quadratus, and "the interosseous membrane.
The amount of displacement of the distal
TABLE 5. Results of Force Analysis
NG. 1 I. For analysis of the stabil~ing ~otentiNof the TFCC on the distal ~dioulnar joint, ~inswere cemented into the distal and ~roximN radiusin v~ing ~ositions of fore~ robson, and a forcew~ applied to the dis~ ulna in a do~l,or lateral mode a~er segmented sectioning of re-st~Nng gravures. ~s~lacement of the utn~ headin relation to ~e radiN ~iculation w~ me~ured.(Re~Nnted ~th ~e~i~ion from Palmer, A. K.,and Wemer, F. W.: The tfiangut~ fibroc~agecomplex of the ~st~Anatomy and function. J.Hand Surg. 6:153, 1981.)
ulna both dorsally and palmarly on a fixedradius~n neutral forearm rotation, 75 o of pro-nation, and 75° of supination was minimally
of the Distal Radioulnar Joint* **
Percent Displaceraent Toward Dislocation
Neutral 75° Pronation 75° Supination
Order of Cuts Dorsal Vohzr Dorsal Volar Dorsal Volar
Intact 44 24 14 10 18 18Pronator quadratus cut 44 27 21 10 22 31Capsule cut 46 2’,3 126 10 24 36TFCC cut 200 140 1:55 40 200 200
] * Displacement is expressed in terms of percent dislocation of the distal radioulnar joint, with 100% represenUngthe position at which the inferior surface of the ulna was flush with the surface of the radius (dorsal dislocation)
{palmar dislocation). In all cases the experiment was stopped unless either a load of 44.5 N (I0 lbs) had beenreached or the ulna had displaced 100% beyond the distance requitx.’d for dislocation (200% displacement).
¯ * (Reprinted with permission from Palmer, A.K., ;rod Werner. F.W.: The triangular fibrocartilage complex of thewrist--Anatomy and function. J. Hand Surg. 6:153, 1’981.)

34 Palmer and Werner
TABLE 6. Results of the Force Analysis of the Di’stal Radioulnar Joint to LateralDisplacement of the Ulna in Terms of Centimeters of Displacement
from the Sigmoid Notch of the Radius* **
Lateral Displacement of Distal Ulna (cm)
Pronator InterosseousForearm Rotation Intact TFCC Cut Capsule Cut Quadratus 5lembrane Cut
Neutral 0.36 0.46 0.46 0.81 2.5075° pronation 0.30 0.48 0.69 0.81 2.5075° supination 0.23 0.28 0.30 2.50 2.50
* The experiment was stopped at 2.5 cm 0f disptacemertt since there appeared to be no soft-tissue restraints to ulnardisplacement at this point.
** (Reprinted with permission from Palmer, A.K., and Werner. F.W.: The triangular fibrocartilage complex of thewrist--Anatomy and function. J. Hand Surg. 6:153, 1981.)
affected by sectioning the pronator quadratusor the distal radioulnar joint capsule. Furthersectioning of the TFCC leads to dislocationof the joint both dorsally and palmarly in allpositions, except for volar displacement of thedistal ulna when the wrist was in full prona-tion.
Lateral displacement of the ulna on the fixedradius was relatively unaffected by sectioningof the TFCC, capsule, and, in neutral and the75 ° pronated position, the pronator quadratus.In full supination, release of the pronatorquadratus resulted in marked (2.5 cm) dis-placement. Further release of the interosseousmembrane led to marked displacement inneutral and 75° pronation.
It appears from these distraction studies thatin all positions the TFCC is a major stabilizerof the distal radioulnar joint.
REFERENCES
1. Bowers, W. H.: Distal radioulnar joint. In Green,D. P. (ed.) Operative Hand Surgery. New York,Churchill Livingstone, 1982, p. 743.
2. Brand, P. W., Beach, R. B., and Thompson, D. E.:Relative tension and potential excursion of musclesin the forearm and hand. J. Hand Surg. 3:209, 1981.
3. Bunnell, S.: Surgery of the Hand, ed. 3. Philadelphia,J. B. Lippincott, 1956.
4. Chao, E. Y.: Personal communication, 1980.5. Cooper, A., and Bransby, B.: Treatise of Dislocations,
ed. 5. Philadelphia, Lea and Blanchard, 1844, p. 417.
6. Dameron. T. B.: Traumatic dislocation of the distalradioulnar joint. Clin. Orthop. 83:55. 1972.
7. DeSa,alt, M.: Extrait d’un mrmoire de M. DeSaultsur la luxation de l’extr~mit~ inferieure du radius. J.Chir. 1:78. 1791.
8. Destot. 1~. Injuries of the wrist: A radiological study.Atkinson, F. R. B. (trans.). New York, Paul B. Hoeber,Inc., 1926. -.
9. Hamlin, C.: Traumatic disruption of the distal ra-diouhaar joint. Am. J. Sports Med. 5:93, 1977.
10. HeiNe, K. B., Freeh~er, A. A., and Van’t Hof, A.:Isolated traumatic dislocation of the distal end of theulna or distal radio-ulnar joint. J. Bone Joint Surg.44:1387, 1962.
11. Hergenroeder, P. T., and Gelberman, R. H.: Distalradioulnar joint subtuxation secondary to excision ofthe ra~ial head. Orthopedics 3:649, 1980.
12. Hui, F. C., and Linscheid, R. L.: Ulnotriquetml aug-menmtion tendodesis: A reconstructive procedure fo__rdorsal subluxation of the distal radioulnar joint. J.Hand¯ Surg. 7:230, 1982.
13. Johnson, R. K., and Shrewsbury, M. M.: The pronatorquachatus in motions and in stabilization of the radius
~ and ulna at the distal radioulnar joint. J. Hand Surg.1:205, 1976. ~
14. Kaphm, E.: Functional and Surgical Anatomy of theHand.. Philadelphia, J. B. Lippincott, 1953, p. 101.
15. Lewis, O. J.: Evolutionary changes in the primatewrist and inferior radioutnar joints. Anat. Rec.151:275, 1965.
16. Liebolt, F. L.: A new method for relmir of the distalradioulnar joints. Anat. Rec. 151:275, 1965.
17. Mikic, Z. D.: Galcazzi fracture-dislocation. J. BoneJoint Surg. 57:1071, 1975.
18. Milch, H.: So-called dislocations of the lower end ofthe ulna. Ann. Surg. 116:282, 1942.
19. Mohiuddin, A., and Janjua, M. Z.: Form and functionof radioulnar articular disc. Hand 14:61, 1982.

¯ Clinical Ort~o~aeorcsan(: Re~ate~ Researct~
Joint to Laterallacement
Inlerosseotts
Membrane Cttt
2.502.502.50
ft-tissue restraints to ulnar
¯ ocartilage complex of the
ic dislocation of the distalhop. 83:55. 1972.mfmoire de M. DeSault:t~ inferieure du radius. J.
*fist: A radiological study.few York. Paul B. Hoeber.
~ruption of the distal ra-"ts Med. 5:93, 1977... A., and Van’t Hof. A.:~n of the distal end of the3int. J. Bone Joint Surg.
;elberman, R. H.: Distal: secondary, to excision ofs 3:649, 1980.L L.: Ulnotriquetral aug-~nstructive procedure foristai radioulnar joint. J.
,,ry, M. M.: The pronator;stabilization of the radiuslnar joint. J. Hand Surg.
~urgical Anatomy of theppincott, 1953, p. I01.changes in the primateaar joints. Anat. Rec.
:1 for repair of the distal151:275, 1965.
are-dislocation. J. Bone
ions of the lower end oft, 1942.[. 7_.: Form and functionHand 14:61, 1982.
Number 187July/August. 1984 Biomechanics of Distal Radioulnar Joint 3520. Morrey, B. F., Chao, E. Y., and Hui, F. C.: Biome-
chanical study of the elbow following excision of theradial head. J. Bone Joint Surg. 61:63, 197!).
21. Morrissy, R. T., and Natebuff, E. A.: Dislo~mtion ofthe distal radioulnar joint: Anatomy and clues toprompt diagnosis. Clin. Orthop. 144:154, 1’979.
22. Palmer, A. K., Glisson, R. R., and Werner; F. W.:Ulnar variance determination. J. Hand Surg. 7:376,1982.
23. Palmer, A. K., and Neviaser. R. J.: Triangular fibro-cartilage complex abnormalities--Results of surgicaltreatment. Presented at the 50th Annual M~eting ofthe American Academy of Orthopedic Surgeons, An-aheim, CA, March 1983.
24. Palmer, A. K., Skahen, J., Werner, F. W., and Glisson,R. R.: The extensor retinaculum of the wrist: Ananatomic and biomechanical study. Presented at the38th Annual Meeting of the American Society forSurgery of the Hand. Anaheim. CA, March 19~3.
25. Palmer, A. K., and Werner. F. W.: The triangularfibrocartilage complex of the wrist~Anatomy andfunction. J. Hand Surg. 6:153, 1981.
26. Palmer, A. K., Werner, F. W., and Glisson, R. R.:Personal communication, 1982.
27. Ray, R. D., Johnson, R. J., and Jameson, R. M.:Rotation of the forearm~An experimental study ofpronation and supination. J. Bone Joint Surg.33A:993, 1951.Rose-Innes, A. P.: Anterior dislocation of the ulna atthe inferior radio-ulnar joint. J. Bone Joint Surg,42B:515, 1960.Slater, N., and Darcus, H. D.: The amplitude of fore-arm and humeral rotation. J. Anat. 87:407, 1953.Vesely, D. G.: The distal radioulnar joint. Clin. Or-thop. 51:75, 1967.Werner, F. W., Glisson, R. R., and Palmer, A. K.:Pressure distribution in the radioulnar ca~al joint.Presented at the Second Annual Murray Day. Syr-acuse, NY, May 1982.Werner. F. W.. Palmer, A. K., and Glisson, R. R.:Forearm load transmission: The effect of ulnarlengthening and shortening. In Cracchiolo, A. (ed.):Transactions of the 28th Annual Meeting of the Or-thopedic Research Society, New Orleans, LA, January1982, p. 273.
28.
29.
30.
.31.
32.