Embed Size (px)
Citation preview

Annals ofthe Rheumatic Dieaws 1990; 49: 863-870
Surgery for the rheumatoid wrist and hand
S H Norris
Surgery for rheumatoid arthritis of the handand wrist has improved the lot ofmany with thiscondition over the past several years, and thereis no doubt that surgery can make an enormousdifference to the course of the disease. Pain,deformity, poor function, and cosmesis are allindications for surgery. There are, however,many patients who are denied access to surgerywho would benefit from it.
PATTERNS OF DISEASEProgression of the rheumatoid process at thewrist produces a number of recognisable defor-mities, which occur in a more or less constantfashion.The disease at the wrist may affect the
radiocarpal, mid-carpal, and radioulnar joints(fig 1). At the radioulnar joint the tendon ofextensor carpi ulnaris has a significant role. ' Inthe normal wrist the tendon crosses the extensorsurface of the distal ulna, but in the rheumatoidwrist it comes to lie on the volar surface of thelina as the distal ulna begins to subluxate onthe radius. Thus the tendon behaves as a flexorof the wrist rather than as an extensor. This hasthe effect of causing an imbalance between theradial and ulnar extensors, and the radiocarpaljoint becomes pulled into radial deviation.
This deformity has grave implications for themetacarpophalangeal (MCP) joints. As the wristbecomes pulled into radial deviation so thefingers start to become pulled into ulnar devia-tion. This is only one of the causes of ulnar driftof the MCP joints, but a very important one,which may easily be attended to surgically.2Furthermore, as the tendon slips from itsposition on the back of the ulna so it loses itsrole as a stabiliser of the distal ulna, permittingmore dislocation. The dislocation of the ulna,together with the severe erosions on the lowerend of this bone, puts the extensor tendons ofthe fingers at considerable risk of rupture.
This clinical picture-(a) subluxation of thedistal ulna; (b) radial deformity of the wrist; (c)dropped fingers from extensor tendon rupture(fig 2)-is known as the caput ulnae syndrome.At the radiocarpal joint progressive stretching
of the joint capsule together with joint erosionresults in ulnar displacement of the proximalcarpal bones with secondary radial deviation ofthe hand. At the same time the scaphoid and thelunate slip into a palmar position on the radius.In some cases the radius and the lunate becomespontaneously fused. This produces a degree ofpain relief, but restricts movement.
CLINICAL FEATURESPatients with wrist disease present in a varietyof ways. The most common is significant dorsalswelling resulting from extensor tendonsynovitis. In most cases this will produce painon movement of the digits. There will often beassociated subluxation of the distal ulna. Wristmotion may be preserved, depending upon thedegree of articular cartilage damage. Progressionof the disease will result in the deformities
Northern GeneralHospital, SheffieldS H NorrisCorrespondence to:7 Endcliffe Grove Avenue,Sheffield S1O 3EJ.
Figure I Radiograph ofthe wnist showing severe erosivechanges anddmage to the radiocarpal, mid-carpal, andcarpometcarpaljonts.
Figure 2 The extensor tndons to the middle, ring, and littlefingers have ruptured.
863
on Novem
ber 16, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.49.S
uppl_2.863 on 1 October 1990. D
ownloaded from

Nomris
described above. Rupture of the extensortendons is a grave complication.
SURGICAL TREATMENTBoth soft tissue and bony procedures are ofbenefit for the rheumatoid wrist
Synovectomy not only relieves pain andswelling but can also damp down the arthritis.It is indicated in early disease when conservativemeasures have failed. The procedure is per-formed through a straight dorsal incision toprevent necrosis of the skin flaps. The skin ofpatients with rheumatoid arthritis can be verythin, especially if the patient is being treatedwith steroids, and a curved incision is verysusceptible to flap necrosis even if the flaps donot seem to have been undermined to anysignificant extent. The dorsal retinaculum isdivided and reflected in both directions, ratherlike the pages of a book, to expose the dorsaltendons beneath.
Inflamed synovium is stripped from thetendons and often it can be seen that thesynovium has eroded into the structure of thetendon, which is in imminent danger of rupture.Such areas are weaknesses in the tendon and asmuch synovium as possible should be removed.At the same time as synovectomy of the
extensor tendons the wrist joint is opened andsynovectomy performed. A complete clearanceof the wrist is impossible but, nevertheless, aproportion of the synovium can be cleared awayand this will contribute to pain relief.
Reflection of the dorsal retinaculum towardsthe ulnar side of the wrist allows the distalradioulnar joint to be opened. The ulna is oftensubluxated and the end of the bone is commonlysharp, pitted, and eroded. It is easy to see howan extensor tendon already weakened by infil-trating synovium will rupture by passing overthe sharp distal ulna.
DARRACH S PROCEDUREThe patient with a dislocated ulna with pain onrotation of the wrist may benefit from anexcision of the distal 1 cm of the ulna, known asDarrach's procedure. Although this operationhas been shown by several authors to providegood relief of pain,'5 the expected result is notalways forthcoming. Newman found that in60/o of patients there was no change in wristfunction and in 12% there was actually adeterioration in function, though there wasrelief of rest pain in 77%.6 Pain on rotation ofthe forearm was improved in 86% and the rangeof rotation increased in 90%. Eighty eight percent graded their result as excellent or fair.An alternative to the Darrach procedure has
recently been devised by Bowers.7 The radialaspect of the distal ulna is resected in such a waythat impingement between the two bones isprevented throughout the range of rotation ofthe forearm. The gap left by the resected ulnamay be filled either by repair of the dorsalcapsule or by tendon interposition. The advan-tage of this procedure is that the ulnar ligamentcomplex is not disturbed and as the distal ulnahas not been totally resected the wrist does not
lose its ulnar support. One of the problems withthe Darrach procedure is that the carpus canslide further in an ulnar direction if the ulnarligament constraints are removed. Bowers con-sidered that the procedure was of value in 85%of patients operated upon.A similar procedure described by Watson et
al8 also entails hemiresection of the ulna, andthe distal ulna is shaped to conform to the shapeof the distal radius. No soft tissue interpositionis used in this procedure.
Associated radial deviation of the carpus withulnar translocation should be treated bystrengthening ulnar extension of the wrist. Thiscan be accomplished by transferring extensorcarpi radialis brevis to the ulnar side of the wristand using this tendon to stabilise extensor carpiulnaris in a dorsal rather than a volar position.
ARTHROPLASTY AND ARTHRODESISIn more severe disease of the wrist the surgicaloptions are either arthrodesis or arthroplasty.The choice of surgery should not be based uponradiographic signs only as it is surprising howmuch radiologically apparent damage somepatients can tolerate before a request is made forsurgical relief.Although several types of wrist implant have
been devised, the two most commonly used areSwanson's flexible silastic implant9 and Meuli'sthree component metal-polythene-metal pros-thesis.'0 Summers and Hubbard have reviewedtheir experience of these two devices andconcluded that both afford a pain free jointwhich is stable and provides a solid platform forthe hand with a reasonable range ofmovement. "The Meuli prosthesis perhaps provides a greaterrange of movement than the Swanson implant,but the technique of insertion is more critical.Both prostheses have their inherent dangers ofdislocation and loosening and, in addition, thereis the risk of cement failure with the Meulidevice.The results of wrist arthroplasty must be
compared with the results of arthrodesis.Arthrodesis of the wrist in rheumatoid arthritisis an excellent operation. Problems of union areseldom encountered, the operation is relativelyquick and safe to perform, and the results arepredictable.Many different types of wrist fusion have
been described. Millender and Nalebuff's tech-nique is perhaps the most popular.'2 Stability isachieved by passing a Steinmann pin throughthe second or third metacarpal joint into thedistal end of the radius. In many cases this is allthat is required, especially if the wrist isseverely eroded. Autologous bone grafting isseldom necessary and by destroying the adjacentsides of the wrist most joints can be persuadedto fuse. Arthrodesis is from the radius down tothe capitate. Immobilisation of the joint inplaster for six weeks will ensure that union takesplace in most patients.
Other techniques of arthrodesis include theuse of staples, Kirschner wires, and plates toachieve the same results. It must be rememberedthat fusing the wrist of a patient with rheuma-toid arthritis is not the same as performing this
864
on Novem
ber 16, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.49.S
uppl_2.863 on 1 October 1990. D
ownloaded from

Sw2gery for the rhmumatoid wrist and hand
operation on a young man with post-traumaticosteoarthritis. Heavy plates are not necessaryand merely make the skin incision difficult toclose, increasing the risk of skin breakdown.The wrist is normally arthrodesed in a neutralposition, though if both wrists are being treatedit may be preferable to stiffen one joint in a fewdegrees of flexion to enable the patient toattend to personal hygiene.An alternative to formal wrist arthrodesis is
fusion of the radiolunate joint. This procedureis indicated for treatment of pain emanatingfrom the radiocarpal joint if the mid-carpal jointis preserved. This joint sometimes fuses spon-taneously with resolution of pain. Nalebuff andGarrod suggest that perhaps one third of patientsbeing considered for wrist fusion might besuitable for this operation. 3 Linscheid andDobyns reported good results for 13 of 16patients undergoing localised wrist fusion.'4
EXTENSOR TENDON RUPTUREExtensor tendon rupture is one of the majorcomplications that can befall the rheumatoidpatient and it can be both predicted andprevented.Rupture has to be distinguished from two
other conditions. The first is a failure of digitextension owing to chronic dislocation of theMCP joints and the second is the comparativelyrare condition of posterior interosseous nerveentrapment.The most commonly injured tendons are
extensor pollicis longus, where it passes overLister's tubercle, and the tendons to the littleand ring fingers. The tendons to the middle andindex fingers are less often ruptured.
Dorsal subluxation of the ulna associatedwith tenderness on resisted extension of thethumb and fingers must alert the doctor to thepossibility of tendon rupture. Thickening of thedorsal synovium is present and dorsal displace-ment of the distal ulna is nearly always anaccompanying feature.Prevention of rupture is by dorsal tenosyno-
vectomy (see above). Treatment of establishedrupture is by synovectomy and tendon transfer.The preferred transfers for a single tendon
rupture are either end-to-side repair using thenext-door extensor tendon or transfer ofextensorindicis proprius. End-to-side repair will providegood results but without such good individualfunction.'5 Multiple ruptures pose a severeproblem. Extensor indicis proprius is not strongenough to extend more than a single digit so analternative must be found. Flexor sublimis fromthe ring finger can be rerouted to the dorsum ofthe hand and will provide satisfactory extensionto more than one digit ifso desired. Occasionally,in cases of quadruple tendon rupture, it may benecessary to use two flexor tendons.'6
Metacarpophalangeal joint surgeryThe MCP joints are the most common site ofrheumatoid arthritis affecting the hand. Swell-ing of the MCP joints, ulnar drift with progres-sive volar subluxation of the base of theproximal phalanx, and, eventually, dislocation
with an inability actively to extend the joints arethe hallmarks of the condition. Apart fromprogressive deformity pain is a common feature.The early radiological appearances are of softtissue swelling and erosions, progressing inlate cases to dislocation and destruction ofthe joints.
SYNOVECTOMYThe role of synovectomy has long been acontentious issue. There is no doubt that insome patients the course of the disease can beslowed down by performing synovectomy at anearly stage. It must be remembered, however,that patients not infrequently show spontaneousremission, and this affects the assessment ofresults.
Synovectomy is indicated for patients whopresent with pain and persistent swelling of theMCP joints in which there are minimal radio-graphic changes and little deformity. Soft tissuereconstruction with synovectomy is performedfor patients who have ulnar drift with dislocationof the extensor tendons but do not haveradiological erosions. Before a synovectomy isperformed, however, patients should be given atrial of medical treatment for not less than threeto six months. If the MCP joint synovitis settlesdown with this treatment regimen then surgeryis no longer necessary.
Ellison, Kelly, and Flatt reviewed the resultsof surgical synovectomy of the digital joints inrheumatoid arthritis.'7 Surgical synovectomywas performed on 390 joints in 67 patients. Themean follow up was for 4-5 years. There was asignificant improvement in pain relief, withonly nine patients having recurrence of painpostoperatively. Twenty nine of the 67 patientsshowed no progression of deformity, whereassome progression of deformity was seen in theremaining 38. Radiographic progression of thedisease was seen to a moderate degree in 37patients, of whom nine could be described ashaving an early synovectomy, three synovectomyat an intermediate stage of the disease, and 25 alate synovectomy. Ten patients showed markeddeterioration of the radiographic appearance;five of these had undergone synovectomy at anintermediate stage and four for late disease. Ofthe 20 patients who showed no radiographicprogression, 14 had had operations for earlysynovitis. The radiographic progress is thereforeclearly related to the stage of the disease atwhich the synovectomy is performed. Recur-rent synovial swelling was seen in one or morejoints in 20 patients. Two thirds of the patientswho showed recurrent synovial swelling wereoperated on at an intermediate or late stage ofthe disease.The MCP joints can be approached either
through a transverse incision across their dorsumjoints or, alternatively, individual longitudinalincisions some 3 to 4 cm in length can be used.Each joint is opened on the radial side by carefuldivision of the sagittal band, which must becarefully delineated from the underlying capsuleand the band must be carefully preserved forsubsequent suture.Some 60% of the synovial membrane can be
865
on Novem
ber 16, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.49.S
uppl_2.863 on 1 October 1990. D
ownloaded from

Norris
removed surgically. If the joint is flexed andtraction applied the synovium lying in thevolar recesses of the joint can be reached. It isimportant to curette beneath the collateralligaments and to remove the tongue of synoviumwhich extends proximally along the dorsum ofthe joint between the distal end of the meta-carpal and the extensor tendon.
Ulnar driftHarrison stressed the importance of thealignment of the middle finger in identifyingulnar drift.l" If the index and ring fingers areheld in full extension any ulnar deviation is seenas the middle finger flexes and extends. Aftersynovectomy the extensor tendons are relocatedby reefmg of the sagittal bands. Ulnar drift ofthe metacarpals without significant joint erosionis eminently treatable surgically. Relocation ofthe extensor tendons provides some of thenecessary correction of this deformity, whichcan also be corrected by dividing the intrinsictendons on the ulnar sides of the index, middle,and ring fingers from their attachment to theextensor mechanism, rerouting them across theweb spaces, and reattaching them to the extensorexpansion on the radial side of the middle,ring, and little fingers respectively. This isknown as crossed intrinsic transfer.The concept of crossed intrinsic transfer was
introduced by Straub,19 20 who described trans-fer of the tendon into the lateral band of theadjacent finger. Ellison, Flatt, and Kelly suturedthe intrinsic tendon to the radial collateralligament of the adjacent finger for fear ofcausing a swan-neck deformity.2' The indexfinger is held in a corrected position by proximalreattachment of the radial collateral ligament.
Persistent volar subluxation of the proximalphalanx may be treated by the Harrison slingtechnique.'8 A 4 cm slip of extensor tendon 5mm wide is detached proximally and freeddistally to the distal portion of the MCP joint.This is passed through a drill hole made in thedorsal cortex of the proximal phalanx. Thetendon is passed through the drill hole andsutured back on itself. This provides a strong
Fge3 Seerely deformed hands, which arefreefrom pain and not suitable forreconstructon.
extensor force holding the base of the proximalphalanx in its relocated position.
INTERPOSITION ARTHROPLASTYIn late cases with joint destruction and dis-location reconstruction of the MCP joints bymeans of silastic arthroplasty is necessary. Painaccompanied by irretrievable articular carilagedamage, volar subluxation, or dislocation is theindication for surgery. There are many patients,however, who cope very well with severelydeformed hands, who are often free from pain,and for whom sophisticated surgery is irrelevant(fig 3).The most widely used implant is the Swanson
designed silicone-rubber spacer. Its functiondepends upon a supporting fibrous capsuledeveloping after joint resection. Vahvanen andViljakka performed a retrospective analysis in32 rheumatoid patients who had undergone 107Swanson MCP joint implants and reported animprovement in hand function in 27 (84%).22 Aprospective study by Bieber et al with 210 jointsinserted in 55 rheumatoid hands showed initiallygood correction of deformity with improvementin the range of joint movement.23 When thesepatients were assessed in the long term at anaverage of 5 25 years there was some deterior-ation in function, though most remained betterthan before the operation. In the early post-operative evaluation ulnar drift improved froman average of 25 degrees to less than 5 degreesand the preoperative extension deficit improvedfrom 56 to 10 degrees. In the long term theamount of ulnar drift had increased to 12degrees and the extension deficit to 22 degrees.Grip strength did not seem to increase.
Silastic interposition arthroplasty is per-formed through similar incisions as describedfor synovectomy. Once the joint has beenopened and the synovium excised the metacarpalhead is excised through the neck. The intra-medullary cavity of the proximal phalanx isbreached with a sharp awl and then reamedusing small hand-held reamers to clear a cavitylarge enough for the stem of the prosthesis. Thecanal of the metacarpal is reamed in a similarfashion. The correct size of implant is selectedby using trial prostheses. The selected implantshould be large enough to allow easy insertionand it should allow a reasonable range of flexionup to 70 degrees without dislocation of thestem.Once all four implants have been inserted
ulnar drift is corrected by crossed intrinsictransfers and tightening of the radial collateralligament of the index finger. The Harrison loopreconstruction of the extensor tendon may alsobe performed. An abduction deformity of thelittle finger can be corrected by resecting alength of the tendon of abductor digiti minimi.Swanson published his results of flexible
implant arthroplasty in 3915 implants, of which3867 were for the MCP joints and 148 for theproximal interphalangeal (PIP) joints.24 Thirtytwo of the joints dislocated after the operationand there was an infection in 27, requiringremoval in five. The range of movement at theMCP joints averaged 58 degrees. Most patients
866
on Novem
ber 16, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.49.S
uppl_2.863 on 1 October 1990. D
ownloaded from

Surgevyfor the rheumatoid wrst and hand
had a range of movement of between 40 and 70degrees. Follow up ranged from six months tofive years.
Postoperative careThe postoperative care of a hand which hasundergone reconstructive surgery to the MCPjoints is most important and a critical part of theprocedure. For the first two weeks post-operatively the hand is supported in a handdressing with the MCP joints in about 30degrees of flexion, with 30 degrees of flexion atthe interphalangeal joints.
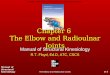
After two weeks extension of the MCP jointscan be maintained with a dynamic extensionsplint for daytime use and treatment, and thefingers should be rested at night on a simplepaddle splint. After a further six weeks it isrecommended that a metacarpal radial abductionsplint should be used, which allows normalusage of the MCP joints but at the same timeulnar deviation of the fingers is resisted (figs 4Aand B).
Proximal interphalangeal jointsSeveral patterns of rheumatoid disease of thePIP joints may be seen. Chronic thickening andinflammation of the joint is due to synovialproliferation, which causes gradual stretchingand bulging of the capsule (fig 5). Boutonniereand swan-neck deformities occur in a proportionof patients. The radiological changes are similarto those seen in the MCP joints.
SYNOVECTOMYSynovectomy of the PIP joints is a usefuloperation for proliferative synovitis that hasfailed to respond to medical treatment onceagain. It is important to give medical treatmenta trial before embarking on synovectomy asoften the synovial proliferation can be aborted
Figure 4 (A) Metacarpal radial abducton splmtfrom the dorsum; (B) the same splintviewedfron thefront.
Figure S Chronic thickening of the proxi'malinterphalangeal joint ofthe index finger.
by a good medical regimen. Injections of localanaesthetic and steroid can also be useful tocontrol synovitis.
Synovectomy gives good relief of pain andthere is usually only ashight loss of PIP jointmovement. Its major disadvantage is recurrenceof the synovitis. Wilde suggested that as manyas 30% of patients undergoing PIP joint syno-vectomy have some degree of recurrence ofsynovial sweling.2Emlison et al had a recurrencerate of 24%.17 Ansell et al reviewed 115 syno-vectomies in 56 patients.26 In 83 fingers therewas no change in the range of movement and in17 the range improved. Pain relief made theprocedure worthwhile in all the cases. A reviewof these cases at five years showed that there hadbeen no radiological change in 37 joints, mildimprovement in nine, and slight deterioration in66.27 In 60% there was good relief of pain andsome improvement in grip.
It is very difficult to achieve complete removalof the synovium by surgical means. Theoperation is performed through a posterolateralapproach, and one of the collateral ligamentsshould be divided to remove as much of thesynovium as possible.
SWAN-NECK DEFORMITYSwan-neck deformity is characterised by hyper-extension of the PIP joint with flexion of thedistal interphalangeal (DIP) joint. The deformitymay start at either the PIP or DIP joints.At the DIP joint there is gradual stretching or
a frank rupture of the attachment of theextensor tendon to the base of the distalphalanx. This results in a mallet deformity ofthe distal joint and causes an extensor tendonimbalance, which expresses itself at the PIPjoint with a hyperextension deformity.
If the deformity originates at the PIP jointthere is a gradual stretching of the volar plate.As the hyperextension deformity increases thereis not infrequently rupture of the superficial
867
on Novem
ber 16, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.49.S
uppl_2.863 on 1 October 1990. D
ownloaded from

Nomis
flexor tendon, and this allows the hyperextensiondeformity to become worse. The flexion defor-mity at the DIP joint in these cases is secondary.Four stages are recognised:Type 1. There is full passive movement of the
PIP joint. The functional loss in these patientsis related to the loss of the DIP joint extension.Type 2. Restriction of PIP joint flexion is
influenced by the position of the MCP joint.Flexion of the PIP joint is restricted if the MCPjoint is extended. Flexion of the MCP jointfacilitates flexion of the PIP joint.Type 3. There is significant restriction of PIP
joint movement. The joint spaces are preserved.Type 4. End stage deformity. There is
significant loss of articular cartilage with acomplete loss of active and passive PIP jointmovement.
BOUTONNIERE DEFORMITYThe boutonniere deformity is characterised by aflexion deformity of the PIP joint with anextension deformity at the DIP joint. There isoften an associated hyperextension deformity ofthe MCP joint.
Synovial proliferation within the PIP jointresults in stretching of the joint capsule. Thecentral slip of the extensor tendon stretches andthe PIP joint assumes a flexed position as it isno longer supported on its dorsal aspect. Thelateral bands adopt a more and more volarposition and this accentuates the flexion defor-mity of the PIP joint. In addition, as the lateralbands become tense they cause an extensiondeformity of the DIP joint. As the flexiondeformity of the PIP joint increases the patientcompensates by hyperextending the fingers atthe MCP joint in order to maintain as muchindependence of finger movement as possible.
In the early stages both the swan-neck andboutonniere deformities are passively correct-able. As the condition deteriorates so thedeformities become fixed.
Stage 1. There is a 10-15 degree flexiondeformity and the extensor lag of the PIP jointcan be corrected passively. As the PIP jointdeformity is corrected it is obvious that there islimited flexion of the DIP joint. The patient'sfunctional loss is related as much to the lack ofDIP flexion as to the lack of PIP extension.
Stage 2. There is a 30-40 degree flexiondeformity. The MCP joint is extended and theboutonniere deformity is no longer passivelycorrectable.
Stage 3. The deformity is fixed with severeloss of articular cartilage.
SURGERY FOR SWAN-NECK AND BOUTONNIEREDEFORMITIESSoft tissue procedures for swan-neck andboutonniere deformity are not often indicatedbut may be useful if the condition of thearticular surfaces is good.28 29
Available procedures for the correction ofswan-neck deformity include fusion of the DIPjoint, dermodesis, flexor tenodesis of the PIPjoint, and reconstruction of the retinacularligaments. Distal interphalangeal joint fusion is
indicated only if the swan-neck deformityoriginates at that joint. The joint should befused in full extension.
Both dermodesis and the flexor tendon pro-cedures have been popularised by Nalebuff.Dermodesis entails the excision of an ellipse ofloose skin over the flexor aspect of the PIP jointand closure of the defect. Its long term resultsare poor, but it may be usefully combined withflexor tenodesis in which one slip of thesublimis tendon is used as a passive check-reinagainst full extension of the PIP joint, by beingpassed around a pulley in the fibrous flexorsheath and sutured back to itself.
Reconstruction of the retinacular ligamentwas devised by Littler.30 The ulnar lateral bandis freed from the extensor tendon proximallybut is left attached distally. The tendon ispassed volar to Cleland's ligament to bring it tothe volar side of the axis of PIP joint movement.The band is sutured to the fibrous flexor tendonsheath with enough tension to prevent extensionof DIP and PIP joints. This procedure shouldcorrect both the DIP and PIP joint deformities.
Soft tissue procedures for correction of theboutonniere deformity include extensor teno-tomy and reconstruction of the extensor mech-anism. Extensor tenotomy is a fairly simpleprocedure to perform and is carried out to allowflexion of the DIP joint. This takes the tensionoff the proximal joint to some extent and can beeffective in correcting the deformity of the PIPjoint as well as the deformity at the DIP joint.There are many operations described to
reconstruct the extensor tendon mechanism inboutonniere deformity, though the results arenot predictable. Most patients respond best toeither PIP joint fusion or PIP joint arthroplasty.If arthroplasty is selected it is important toreconstruct the extensor tendons as well as toreplace the joints.
Granowitz and Vainio reviewed the results ofPIP joint arthrodesis.3' They studied 122operations in 65 patients. There were eight non-unions, five due to poor placement of theKirschner wires and two in cases of amyloid.Three of the eight patients with non-unionrequired refusion. Six fingers were found to befused in ulnar deviation. In 14 cases theoperation was combined with MCP joint arthro-plasty.
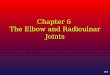
Flexor synovitisSynovitis on the flexor surface of the hand maybe manifest in the flexor sheaths as thickeningaffecting flexion of the digits, and some patientsexperience triggering. The flexor sheaths maybe painful on movement. Median nerve entrap-ment due to proliferative synovitis in the carpaltunnel is not uncommon (fig 6).
Surgical synovectomy of the flexor tendons isa rewarding procedure and one of the 'bestbuys' in rheumatoid hand surgery. Triggering iseliminated and flexion of the fingers improved.
Similarly, decompression of the median nerveis a simple operation-, which rids the patient ofpainful neurological symptoms. Decompressionof the nerve, however, must be accompanied bysynovectomy of the flexor tendons.
868
on Novem
ber 16, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.49.S
uppl_2.863 on 1 October 1990. D
ownloaded from

Swrgery for the rhenatoid wrist and hand
Figure 6 Severe wasting ofthe median nerve owing to longstandingflexor snovitis at thewrist.
Thumb deformities in rheumatoid arthritisThe most commonly encountered deformity ofthe thumb is a boutonniere deformity of theMCP joint, resulting in the so called Z defor-mity. This deformity is caused by synovitis ofthe joint and there is attenuation and virtualrupture of extensor pollicis brevis where itinserts into the base of the proximal phalanx.There is stretching of the collateral ligamentsand, eventually, the proximal phalanx dislocatesfrom the metacarpal. There is often a severehyperextension deformity of the carpometa-carpal (CMC) joint and a concomitant extensiondeformity of the interphalangeal joint of thethumb. Five varieties of thumb deformity aredescribed.Type 1. Boutonniere deformity.Type 2. Flexion deformity of the MCP joint
with hyperextension deformity of the inter-phalangeal joint. There is an associated sub-luxation or dislocation of the CMC joint.Type 3. Swan-neck deformity resulting from
disease at the CMC joint. Synovitis and erosionofthe articular surfaces, together with stretchingof the joint capsule, allows-the joint to becomesubluxated in a dorsal and radial direction. Asthe joint subluxates the metacarpal develops anadduction deformity.Type 4. Gamekeeper's thumb, characterised
by an abduction deformity of the MCP joint,resulting from stretching of the ulnar collateralligament. Secondarily, there is an adductioncontracture of the metacarpal.Type 5. This results from stretching of the
volar plate of the MCP joint. The MCP jointhyperextends and as it does so there is secondaryflexion of the interphalangeal joint as thetension on the flexor tendon increases.
SURGICAL TREATMENT OF THUMB DEFORMITYEarly type 1 deformity consists of a mild degreeofMCP swelling and subluxation and this is notaccompanied by deformity at either the proximalor the distal joints. Synovectomy and re-construction of the extensor tendons is required.Nalebuff has described a rerouting procedurefor the extrinsic extensors which will preventthe joint from resubluxating.32 Harrison hasalso described a similar procedure in whichextensor pollicis longus is tenodesed to the baseof the proximal phalanx.33
Late subluxation of the MCP joint withcartilage erosion but without significant associ-ated joint disease is best managed by MCP jointarthrodesis. If the CMC joint is diseased andstiff, however, replacement of the MCP joint isa better alternative as this will preserve mobilityof the thumb.
Severe deformity of both the MCP andinterphalangeal joints of the thumb with anintact CMC joint is an indication for arthrodesisof both the MCP and interphalangeal joints.Whereas the boutonni&e deformity is mainly
at the MCP joint, swan-neck deformity isprimarily due the gradual dorsal and radialsubluxation of the CMC joint. As the jointerodes and subluxates the metacarpal becomesadducted. Progressive adduction of the meta-carpal results in hyperextension of the MCPjoint in an effort to maintain extension andabduction of the thumb.
Hemiarthroplasty of the CMC joint is thepreferred operation for early deformity, thoughsurgery is indicated only after a trial of conser-vative treatment including adequate splintage.Complete replacement of the trapezium in therheumatoid patient is associated with a highincidence of dislocation.
Hyperextension of the MCP joint may betreated by MCP joint replacement. Severeadduction contracture of the CMC joint withpainful fixed extension of the MCP joint is besttreated by means of CMC joint replacementcombined with fusion of the MCP joint.Type IV deformity with weakness of the
ulnar collateral ligament in early disease withoutsignificant joint destruction of the articularcartilage is treated by means of ligament recon-struction in the same way as chronic rupture istreated in non-rheumatoid patients. In latercases either arthrodesis or joint replacement isnecessary.Type V deformity is managed either by
arthrodesis of the MCP joint or by volarcapsulodesis in a position of flexion.
1 Swanson A B. The ulnar head syndrome and its treatment byimplant resection arthroplasty. J Bone joint Surg [Am]1972; 54: 906.
2 Boyce T, Youm Y, Sprague B L, Flatt A E. Clinical andexperimental studies on the effect of ECRL transfer in therheumatoid hand. Journal ofHand Surgery 1978; 3: 390-4.
3 Rana N A, Taylor A R. Excision of the distal ulnar inrheumatoid arthritis. J Bone joint Surg [Br] 1973; 55:96-105.
4 Jackson I T, Milward T M, Lee P, Webb J. Ulnar headresection in rheumatoid arthritis. Hand 1974; 6: 172-80.
5 Rasker J J, Veldhuis E F, Huffstadt A J, Nienhuis R L.Excision of the ulnar head in patients with rheumatoidarthritis. Amn Rheum Dis 1980; 39: 270-4.
6 Newman R J. Excision of the distl ulna in patients withrheumatoid arthritis. J Bone joint Surg [Br] 1987; 69:203-6.
7 Bowers W H. Distal radioulnar joint arthroplasty: the
869
on Novem
ber 16, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.49.S
uppl_2.863 on 1 October 1990. D
ownloaded from

Norris
hemiresection-interposition technique. J Hand Swag [Am]1985; 10: 169-78.
8 Watson H K, Ryu J Y, Burgess R C. Matched distal ulnarresection. J Hand Surg [AmI 1986; 11: 812-7.
9 Swanson A B. Flexible implant arthroplasty for arthriticdisabilities of the radio-carpal joint. A silicone rubber intra-medullary stemmed flexible hinge implant for the wristjoint. Orthop Clin North Am 1973; 4: 383-94.
10 Meuli H Ch. Meuli total wrist arthroplasty. Clin Orthop 1984;187: 107-11.
11 Summers B, Hubbard M J. Wrist joint arthroplasty inrheumatoid arthritis: a comparison between the Meuli andSwanson prostheses. J Hand Surg [Br] 1984; 9: 171-6.
12 Millender L H, Nalebuff E A. Arthrodesis of the rheumatoidwrist. An evaluation of 60 patients and a description of adifferent surgical technique. J Bonejoint Surg [Am] 1973;55: 1026-34.
13 Nalebuff E A, Garrod K J. Present approach to the severelyinvolved rheumatoid wrist. Orthop Clin NorthAm 1984; 15:369-80.
14 Linscheid R L, Dobyns J H. Radio-lunate arthrodesis. JHand Surg [Am] 1985; 10: 821-9.
15 Nalebuff E A. Surgical treatment of tendon rupture in therheumatoid hand. Surg Clin North Am 1969; 49: 811-22.
16 Nalebuff E A, Patel M R. Flexor digitorum sublimis transferfor multiple extensor tendon rupture in rheumatoid arthritis.Plast Reconstr Surg 1973; 52: 530-3.
17 Ellison M R, Kelly K J, Flatt A E. The results of surgicalsynovectomy of the digital joints in rheumatoid arthritis. JBone joint Surg [Am] 1971; 53: 1041-60.
18 Harrison S H. The importance of the middle (long) fingerrealignment in ulnar drift. Journal ofHand Surgery 1976; 1:87-91.
19 Straub L R. The rheumatoid hand. Clin Orthop 1959; 15:127-39.
20 Straub L R. The aetiology of finger deformity in the handaffected by rheumatoid arthritis. Bulktin of the Hospital forJoint Diseases 1960; 21: 322-9.
21 Ellison M R, Flatt A E, Kelly K J. Ulnar drift of the fingers
in rheumatoid disease. Treatment -by crossed intrinsictransfer. I Bone joint Surg [Am] 1971; 53: 1061-82.
22 Vahvanen V, Viliakka T. Silicone rubber implant arthroplastyof the metacarpo-phalangeal joint in rheumatoid arthritis: afollow-up study of 32 patients.I HandSurg[Am] 1986; 11:333-9.
23 Bieber W J, Wieland A J, Volenec-Dowling S. Siliconerubber implant arthoplasty of the metacarpophalangealjoints for rheumatoid joints. J Bonejoint Surg [Aml 1986;68: 206-9.
24 Swanson A B. Flexible implant arthroplasty for arthriticfinger joints. J Bone joint Surg [Am] 1972; 54: 435-55.
25 Wilde A H. Synovectomy of the proximal interphalangealjoint of the finger in rheumatoid arthritis. JBoneJoint Surg[Am] 1974; 56: 71-8.
26 AnsellBM, Harrison S H, LitdeH, Thomas B. Synovectomyofthe proximal interphalangeal joints. BrJI Plast Surg 1970;23: 380-5.
27 Ansell B, Harrison S H. A 5 year follow-up of synovectomy ofthe PIP in rheumatoid arthritis. Hand 1975; 7: 34-6.
28 Soutter W A. The problem of boutonniere deformity. ClinOrthop 1974; 104: 116-33.
29 Nalebuff E A, Millender L H. Surgical treatment of swan-neck deformity in rheumatoid arthritis. Orthop Clin NorthAm 1975; 6: 733-52.
30 Littler J W. Restoration of the oblique retinacular ligamentfor correcting hyperextension defornity of the proximalinterphalangeal joint. In: Tubiana R, ed. La main rheuma-toide. Paris: Expansion Scientifique Francaise, 1969:155-7.
31 Granowitz S, Vainio K. Proximal interphalangeal jointarthrodesis in rheumatoid arthritis. Acta Orthop Scand1966; 37: 301-10.
32 Nalebuff E A. Restoration of balance in the rheumatoidthumb. In: Tubiana R, ed. La main rheumatoide. Paris:Expansion Scientifique Francaise, 1969: 197-206.
33 Harrison S H, Swannell A J, Ansell B M. Repair of extensorpollicis longus using extensor pollicis brevis in rheumatoidarthritis. Ann Rheum Dis 1972; 31: 490-2.
870
on Novem
ber 16, 2020 by guest. Protected by copyright.
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.49.S
uppl_2.863 on 1 October 1990. D
ownloaded from