Embed Size (px)
Citation preview

Community Dent Oral Epidemiol 1999; 27: 41–7 Copyright C Munksgaard 1999Printed in Denmark . All rights reserved
ISSN 0301-5661
P. K. DenBestenDivision of Pediatric Dentistry, DepartmentBiological mechanisms of dentalof Growth and Development, University ofCalifornia at San Francisco, San Francisco,California, USAfluorosis relevant to the use of
fluoride supplementsDenBesten PK: Biological mechanisms of dental fluorosis relevant to the use offluoride supplements. Community Dent Oral Epidemiol 1999; 27: 41–7. C Munks-gaard, 1999
Abstract – Fluorosis occurs when fluoride interacts with mineralizing tissues,causing alterations in the mineralization process. In dental enamel, fluorosis causessubsurface hypomineralizations or porosity, which extend toward the dentinal-enamel junction as severity increases. This subsurface porosity is most likelycaused by a delay in the hydrolysis and removal of enamel proteins, particularlyamelogenins, as the enamel matures. This delay could be due to the direct effectof fluoride on the ameloblasts or to an interaction of fluoride with the proteinsor proteinases in the mineralizing matrix. The specific mechanisms by which fluo-ride causes the changes leading to enamel fluorosis are not well defined; though Key words: enamel; fluoride; fluorosis,
review; supplementsthe early-maturation stage of enamel formation appears to be particularly sensitiveto fluoride exposure. The development of fluorosis is highly dependent on the Division of Pediatric Dentistry, Department
of Growth and Development, Box 0640,dose, duration, and timing of fluoride exposure. The risk of enamel fluorosis isUniversity of California at San Francisco, Sanlowest when exposure takes place only during the secretory stage, but highestFrancisco, CA, 94019, USA
when exposure occurs in both secretory and maturation stages. The incidence of Tel: π1 415 502 6383dental fluorosis is best correlated with the total cumulative fluoride exposure to Fax: π1 415 476 1499
E-mail: pkdb/itsa.ucsf.eduthe developing dentition. Fluoride supplements can contribute to the total fluorideexposure of children, and if the total fluoride exposure to the developing teeth is Accepted without peer review 9 Novemberexcessive, fluorosis will result. 1998
Exposure of the developing tooth organ to exces-sive amounts of fluoride can result in a mineraliza-tion defect of the enamel that is referred to as fluo-rosis. Fluorotic enamel has an altered structure andappearance that becomes more severe as theamount and duration of fluoride ingestion increase(1–3). The clinical appearance of dental fluorosis ischaracterized by bilateral opaque white areas in theenamel. With increasing levels of fluoride inges-tion, the enamel becomes striated, mottled, and/orpitted. In severe fluorosis, the opaque areas maybecome stained yellow to dark brown (4–7).
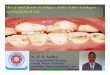
Histopathologically, nonpitted fluorotic enamelshows a subsurface porosity below a well-mineral-ized surface zone (Fig. 1) (8–11). This subsurfaceporosity is what produces the whiter, more opaqueappearance of the enamel. With increasingly severefluorosis, the porosity extends toward the dentinal-
41
enamel junction, and the enamel surface can breakdown after eruption, resulting in pitting of theenamel (7). Fejerskov and co-workers (1, 12, 13)have shown that the severity of dental fluorosis isdirectly related to the amount of fluoride in theenamel, and the subsurface porosity.
Models for studying fluorosis
Several studies have been done to determine themechanisms by which fluoride interacts with thedeveloping enamel to result in fluorosis. The mod-els used for study include tooth organ culture withboth short-term and long-term fluoride exposure(14–16), animal studies following single injectionsof fluoride (17–21), multiple injections of fluoride(22), and chronic ingestion of fluoride in food orwater. Human studies include epidemiologic anal-

DenBesten
Fig. 1. Polarized light micrograph of fluorosed enamel inwater. The well-mineralized (negatively birefringent) surfacelayer is indicated by the shorter arrows, and the hypomin-eralized (positively birefringent) subsurface layer, character-istic of fluorosed enamel, is indicated by the longer arrows.
yses to determine the critical time at which fluorideaffects the developing tooth to result in enamelfluorosis. The results of these studies suggest anumber of possible mechanisms, including a sys-temic effect of fluoride on calcium homeostasis; al-tered protein secretion; impaired matrix biosynthe-sis; direct effects on extracellular proteins and pro-teinases; and specific effects on cell metabolismand function.
Normal enamel development
It is necessary to understand the mechanisms con-trolling normal enamel formation to determinehow fluoride affects enamel development. Dentalenamel is formed by the ameloblasts, which arecells that differentiate from the dental lamina. Theameloblasts differentiate into polarized cells andbegin to secrete an extracellular matrix. The mor-phologic features of the ameloblasts and the ap-pearance of the extracellular matrix which theyproduce have been used to define the stages ofenamel development (23). Although various classi-fications for stages of enamel formation exist, thestages are most often identified as presecretory, se-cretory, transition, and maturation.
During the presecretory stage, the differentiatingameloblasts acquire their phenotype and prepareto secrete the organic matrix of enamel. In the se-cretory stage, the secreted protein consists primari-ly of amelogenins, which are hydrophobic proteinsthat are later removed from the maturing enamelmatrix. Other proteins, such as tuftelin, enamelin,ameloblastins, and metalloproteinases, are secreted
42
in lesser quantities. As the secretory stage contin-ues, these matrix proteins begin to be hydrolyzed.The cells then shorten into transition-stage amelo-blasts and begin to secrete proteinases, which begina rapid degradation of amelogenins.
The early-maturation stage follows, with ahighly porous matrix overlaid with maturation-stage ameloblasts. The maturation stage is charac-terized by modulating cycles of ruffle-borderedand smooth-bordered ameloblasts. These cells re-move the rest of the amelogenin from the maturingenamel matrix and direct the final mineralizationof the enamel. At the end of maturation, the cellslose their polarity and become the reduced enamelepithelium, which is lost from the surface of thetooth when the tooth erupts into the oral cavity.
Effects of fluoride on enameldevelopment
Effects on cell functionAt high levels of fluoride, a major effect appears tobe the reduced secretion of enamel proteins (16, 24,25). However, this effect of fluoride on secretory-stage enamel appears to be mostly reversible (25–27). The primary effects of fluoride occur duringthe early maturation stage, when fluoride canrapidly accumulate (25–28).
Chronic exposure of animals to high levels offluoride in their food or water causes multiple ef-fects on amelogenesis, including the induction ofabnormal modulation cycles within maturation-stage ameloblasts. The number of cycles decreasesin a dose-dependent manner with increasing levelsof fluoride exposure (27, 28) Alterations in themodulation of ameloblasts would affect the pro-cessing of the matrix proteins and subsequent min-eralization of the mature enamel.
Effects on matrix mineralizationThe beginning of enamel maturation is defined bya secondary influx of mineral ions and is charac-terized by a white opaque zone which was de-scribed in rat incisors by Hiller et al. (29) and latershown to be present in most species (30). The whiteopaque zone and the preceding transitional enamelare also characterized by a selective uptake offluoride (31), possibly because of the high degreeof hydration at this stage (32, 33) which would al-low free access to the tissue (34). The increased up-take of fluoride at this stage may partly explain thesusceptibility of early-maturation enamel to the ef-fects of fluoride. The relatively high concentrations

Fluoride mechanisms relevant to supplement usage
of fluoride that are found in the enamel matrix atthe transition/early-maturation stage of enamelformation could reduce the availability of ioniccalcium, resulting in reduced proteolytic activity atthis critical stage (35, 36).
A study by Bronckers and co-workers (16) of theeffects of fluoride on the mineralization of hamstermolars in tooth organ culture showed that fluoridein the medium irreversibly affected the existingmineralizing matrix by producing a rapid deposi-tion of crystals and disrupting their growth.Furthermore, fluoride in the medium interferedwith the deposition of crystals in the new matrix.However, when fluoride was removed from themedium, the newly formed matrix recovered andmineralized normally. These findings suggest thatfluoride may interfere with nucleating sites in thematrix, perhaps by labile binding of the fluoride tothe nucleating sites (35).
After exposure to fluoride, the nature of the min-eral component of enamel is altered. Fluorosedenamel has an increased concentration of magne-sium (30) and in bone mineral, fluoride increasesmanganese and decreases concentrations of car-bonate, citrate (37), and zinc (38). These changes inthe mineral chemistry could affect mineral-matrixinteractions and enzyme activity. For example, ithas been suggested that enamel proteins producedin the presence of fluoride may be more tightlybound to fluorapatite, thereby making them lessaccessible to degradation by enamel proteinases(39).
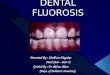
Studies using histochemical staining (40, 41),scanning electron microscopy (8, 9, 42, 43), andquantitative measurement of nitrogen (44) and car-bon (45, 46) have shown an increase in the amountof organic material in fluorosed enamel as a resultof fluoride ingestion. Studies on the effects of fluo-ride on developing enamel in rats have comparedthe protein composition of enamel in rats ingestinghigh levels of fluoride in drinking water with thatin normal rats. In the fluorosed enamel, amelogen-in proteins were retained longer in the maturationstage as compared to control enamel (47–49) (Fig.2).
The mechanism responsible for the delay in hy-drolysis and removal of amelogenin has not yetbeen determined. However, fluoride may alter thequantity or activity of extracellular proteinasesneeded to degrade enamel proteins during thematuration stage of amelogenesis (47, 50, 51).Although proteinases are present in the enamel inboth the secretory and the maturation stages, the
43
Fig. 2. Diagram of ameloblasts showing the cell morphologyat different developmental stages. The relative amount ofprotein in the enamel matrix corresponding to the ameloblastmorphology, is shown in the graph below. The protein con-tent of fluorosed enamel is higher at the transition and early-maturation stages of formation, as compared to normalenamel. RA, ruffle-ended ameloblasts; SA, smooth-endedameloblasts.
proteinases most active in the hydrolysis of amelo-genin are the serine proteinases, which are presentat the maturation stage (52–55). There is some evi-dence to suggest that the proteolytic activity of ser-ine proteinases is reduced in fluorosed enamel,compared to normal enamel (51). The delayed re-moval of amelogenin may be an important mecha-nism in the development of fluorosis by delayingthe growth of enamel crystals, so that when thetooth erupts, the enamel remains incompletelymineralized.
Metabolic factors influencing enamelfluorosis
Metabolic factors that affect the plasma levels offluoride and hence the severity of enamel fluorosisinclude body weight, rate of skeletal growth, andperiods of bone remodeling. Fluoride is rapidly ab-sorbed from the plasma by the bones of the devel-oping skeleton (56), owing to the large surface areaof loosely organized crystallites in the developingskeleton (57).
Rapid growth, resulting in increased absorptionof fluoride into the bone, may have several effects.Removal of fluoride from the blood stream mayinitially reduce the degree of enamel fluorosis byreducing the amount of fluoride available to thedeveloping enamel. However, if fluoride does ac-cumulate in the bone, a relatively large reservoir of

DenBesten
fluoride may be present in the bones of the devel-oping skeleton and may be released locally (58, 59).Angmar-Mansson and co-workers (17, 22) showedthat in rats given a single injection of fluoride, thesubsequently erupting enamel continued to showfluorosis after the serum fluoride levels hadreached baseline levels. This result indicates a con-tinuous local release of fluoride around the devel-oping ameloblasts, presumably from the surround-ing bone. Although the specific fluorotic lesionmay occur during the early-maturation stage oftooth enamel formation, the accumulation of fluo-ride earlier in tooth development may contributeto the level of exposure when enamel fluorosis be-gins.
The metabolic uptake of fluoride is also affectedby other factors, such as nutrition, altitude, and re-nal activity (3, 57). Calcium has been shown to in-hibit fluoride absorption (60), and certain diets,such as those high in protein, lower the gastric pHand result in increased fluoride resorption andhigher levels of fluoride in plasma (57, 61, 62).Fluoride supplements would be unlikely to affectsystemic calcium homeostasis, unless an underly-ing metabolic problem exacerbated the effects offluoride. Because fluoride is largely excretedthrough the renal tubules, any disturbances of re-nal function, such as renal insufficiency, can en-hance fluoride retention and result in fluorosis.
Exposure to fluoride – timing,duration and dose
The severity of fluorosis is related to the timing,duration, and dose of exposure to fluoride (1, 63).In both animal studies (64, 65) and human studies(66), fluoride has been shown to affect the matura-tion stage of enamel formation without previousexposure of enamel to fluoride in the secretorystage. In animal studies as well, fluoride exposureduring the secretory stage alone did not affectameloblast modulation in the maturation stage(27).
Epidemiologic studies support experimentalfindings that the transition and early-maturationstages of enamel formation are highly susceptibleto the effects of fluoride (36, 59, 67–70). The import-ance of timing in the development of enamel fluo-rosis was shown in a study by Ishii & Suckling (71).Investigators recorded the degree of fluorosis inchildren who were initially drinking 7.8 mg/Lfluoride in drinking water, which was subse-quently changed to 0.2 mg/L fluoride. They found
44
moderate to severe fluorosis of the upper leftcentral incisor in children aged 35 through 42months at the changeover, when the tooth wouldhave been in the maturation stage of formation. Incontrast, children aged 11 to 33 months at thechangeover (and thus mostly in the secretory stage)had very mild, questionable, or no fluorosis. Simi-larly, in a study by Pendrys & Katz (72) using theFluorosis Risk Index, fluoride supplements usedonly during the first year of life (secretory stage)held little risk of fluorosis.
These studies have led to the recommendationthat fluoride supplementation should begin afterthis critical period for enamel formation. Althoughthe secretory stage of enamel formation appears tobe affected only by high levels of fluoride, expo-sure to fluoride during this stage clearly increasesthe risk of fluorosis. Although these studies sug-gest that the maturation stage is most sensitive tothe effects of fluoride, the duration of exposure tofluoride before the early-maturation stage does af-fect the severity of enamel fluorosis (59, 71, 73).
The level of fluorosis in a population is relatedto the level of exposure to ingested fluoride for thatpopulation (2, 74). Some investigators have soughtto determine a threshold fluoride level belowwhich enamel fluorosis would not occur. Angmar-Mansson and co-workers (75) postulated that tem-porary peak values rather than elevated fastingvalues are responsible for the occurrence of enamelfluorosis and that the peak values must approachabout 10 mmol to alter enamel formation by theameloblasts. However, Myers (76) noted that thedistinct pattern of increasing prevalence of fluoro-sis with increasing levels of fluoride in the water isnot compatible with the concept of a thresholdlevel for the action of fluoride ion on the enamelorgan (76). The effects of fluoride ingestion appearto be cumulative during tooth formation (1, 2, 27,36, 69, 77).
Summary and conclusions
Excessive ingestion of fluoride results in the de-layed maturation of dental enamel, and subse-quently more porous surface enamel. It is notknown whether fluoride can accumulate in thecells and what local fluoride concentrations areavailable to developing ameloblasts. However, it isapparent that the dose and the duration of fluorideexposure are critical factors in the formation ofenamel fluorosis (1, 4, 5).
The risk factors can be summarized as follows:

Fluoride mechanisms relevant to supplement usage
– Lowest risk occurs with fluoride exposure onlyduring the secretory stage (∞15 months of age).
– Highest risk occurs with fluoride exposure dur-ing both secretion and maturation stages.
– Risk increases with increasing fluoride dose (i.e.,ingestion of fluoride from multiple sources, in-cluding fluoride supplements).The effects of fluoride are cumulative rather than
requiring a specific threshold dose. Therefore, thelonger the exposure to fluoride supplements, thegreater the risk of enamel fluorosis. Recommenda-tions for optimal doses of fluoride supplementsshould take into account the total ingestion offluoride from all sources.
References
1. Fejerskov O, Richards A, DenBesten PK. The effect offluoride on tooth mineralization. In: Fejerskov O, Ek-strand J, Burt BA, editors. Fluoride in dentistry. 2nd ed.Copenhagen: Munksgaard; 1996. p. 112–52.
2. Fejerskov O, Baelum V, Richards A. Dose-response anddental fluorosis. In: Fejerskov O, Ekstrand J, Burt BA,editors. Fluoride in dentistry. 2nd ed. Copenhagen:Munksgaard; 1996. p. 153–66.
3. DenBesten PK. Dental fluorosis: its use as a biomarker.Adv Dent Res 1994;8:105–10.
4. Sundstrom B, Myhrberg H. Light and scanning electronmicroscopy of fluorosed enamel from human permanentteeth. Caries Res 1978;12:320–9.
5. Sundstrom B, Arends J, Jongebloed WL, Bouchouchi M.Morphology of outer regions of fluorosed human decid-uous enamel. Caries Res 1980;14:381–8.
6. Fejerskov O, Thylstrup A, Joost Larsen M. Clinical andstructural features and possible pathogenic mechanismsof dental fluorosis. Scan J Dent Res 1977;85:510–34.
7. Fejerskov O, Yanagisawa T, Tohda H, Larsen MJ, Joseph-sen K, Mosha HJ. Posteruptive changes in human dentalfluorosis – a histological and ultrastructural study. ProcFinn Dent Soc 1991;87:607–19.
8. Sundstrom B, Jongebloed WL, Arends J. Fluorosedhuman enamel. A SEM investigation of the anatomicalsurface and outer and inner regions of mildly fluorosedenamel. Caries Res 1978;12:329–38.
9. Triller M. Structural and histochemical observations offluorotic enamel matrix. J Dent Res 1979;58(Spec IssB):1028–9.
10. Fejerskov O, Silverstone LM, Melsen B, Moller IJ. Histo-logical features of fluorosed human dental enamel. Car-ies Res 1975;9:190–210.
11. Newbrun E, Brudevold F. Studies on the physical proper-ties of fluorosed enamel. Archs Oral Biol 1960;2:15–20.
12. Thylstrup A, Fejerskov O. Clinical appearance of dentalfluorosis in permanent teeth in relation to histologicchanges. Community Dent Oral Epidemiol 1978;6:315–28.
13. Fejerskov O, Larsen MJ, Richards A, Baelum V. Dentaltissue effects of fluoride. Adv Dent Res 1994;8:15–31.
14. Bronckers ALJJ, Jansen LL, Woltgens JHM. A histologicalstudy of the short-term effects of fluoride on enamel anddentine formation in hamster tooth-germs in organ cul-ture in vitro. Arch Oral Biol 1984;29:803–10.
45
15. Bronckers ALJJ, Woltgens JHM. Short-term effects offluoride on biosynthesis of enamel-matrix proteins anddentin collagens and on mineralization during hamstertooth-germ development in organ culture. Arch Oral Biol1985;39:181–5.
16. Bronckers AL, Jansen LL, Woltgens JH. Long-term (8days) effects of exposure to low concentrations of fluo-ride on enamel formation in hamster tooth-germs in or-gan culture in vitro. Arch Oral Biol 1984;29:811–9.
17. Angmar-Mansson B, Lindh U, Whitford GM. Enameland dentin fluoride levels and fluorosis following singlefluoride doses: a nuclear microprobe study. Caries Res1990;24:258–62.
18. Kruger J. Autoradiographic assessment of the effect offluoride on the uptake of 3H-proline by ameloblasts inthe rat. Arch Oral Biol 1970;15:103–8.
19. Kruger BJ. Utilization of 3H-serine by ameloblasts of ratsreceiving sub-mottling doses of fluoride. Arch Oral Biol1972;17:1389–94.
20. Nordlund AL, Lindskog A, Ekstrand J, Hammarstrom L.Fluoride-induced cystic changes in the enamel organ ofthe rat molar. J Oral Pathol 1986;15:87–92.
21. Nordlund AL, Simmelink JW, Henell F, Hammarstrom L.Ultrastructure of fluoride-induced cysts in the rat molarenamel organ. Scand J Dent Res 1986;94:327–37.
22. Angmar-Mansson B, Whitford GM. Single fluoride dosesand enamel fluorosis in the rat. Caries Res 1985;19:145–52.
23. Nanci A, Slavkin HC, Smith CE. Development and calci-fication of enamel. In: Bonucci E, editor. Calcification inbiological systems. Boca Raton: CRC Pr; 1992. p. 313–43.
24. DenBesten PK. Effects of fluoride on protein secretionand removal during enamel development in the rat. JDent Res 1986;65:1272–7.
25. Zhou R, Zaki AE, Eisenmann DR. Morphometry and au-toradiography of altered rat enamel protein processingdue to chronic exposure to fluoride. Arch Oral Biol1996;41:739–47.
26. Lyaruu DM, de Jong M, Bronckers AL, Woltgens JH.Ultrastructure of in-vitro recovery of mineralization ca-pacity of fluorotic enamel matrix in hamster tooth germspre-exposed to fluoride in organ culture during the se-cretory phase of amelogenesis. Arch Oral Biol1987;32:107–15.
27. DenBesten PK, Crenshaw MA, Wilson MH. Changes inthe fluoride-induced modulation of maturation stageameloblasts of rats. J Dent Res 1985;64:1365–70.
28. Smith CE, Nanci A, DenBesten PK. Effects of chronicfluoride exposure on morphometric parameters definingthe stages of amelogenesis and ameloblast modulation inrat incisors. Anat Rec 1993;237:243–58.
29. Hiller CR, Robinson C, Weatherell JA. Variations in thecomposition of developing rat incisor enamel. CalcifTissue Res 1975;18:1–12.
30. Robinson C, Kirkham J. Enamel matrix components, al-terations during development and possible interactionswith the mineral phase. In: Fearnhead RW, Suga S, edi-tors. Tooth enamel IV. Amsterdam: Elsevier; 1984. p. 261–5.
31. Weatherell J, Deutsch D, Robinson C, Hallswarth AS.Fluoride concentrations in developing enamel. Nature1975;256:230–2.
32. Robinson C, Fuchs P, Deutsch D, Weatherell JA. Fourchemically distinct stages in developing enamel frombovine incisor teeth. Caries Res 1978;12:1–11.
33. Robinson C, Kirkham J, Hallsworth AS. Volume distribu-

DenBesten
tion and concentration of protein, mineral, and waterand eveloping dental enamel. Arch Oral Biol1988;33:159–62.
34. Bawden JW, Crenshaw MA, Takano Y, Hammarstrom L.Ion transport through the enamel organ – an update. JDent Res 1982;61:1552–4.
35. Crenshaw MA, Bawden JW. Fluoride binding by organicmatrix from early and late developing bovine fetalenamel determined by flow rate dialysis. Arch Oral Biol1981;26:473–6.
36. DenBesten PK, Thariani H. Biological mechanisms offluorosis and level and timing of systemic exposure tofluoride with respect to fluorosis. J Dent Res1992;71:1238–43.
37. Zipkin I, McClure FJ, Lee WA. Relation of the fluoridecontent of human bone to its chemical composition. ArchOral Biol 1960;2:190–5.
38. Kanwar KC, Singh M. Zinc, copper and manganeselevels in various tissues following fluoride administra-tion. Experientia 1981;37:1328–9.
39. Robinson C, Kirkham J. The effect of fluoride on the de-veloping mineralized tissues. J Dent Res 1990;69:685–91.
40. Shinoda H. Effect of long-term administration of fluorideon physico-chemical properties of the rat incisor enamel.Calcif Tissue Res 1975;18:91–100.
41. Yaeger JA. The effects of high fluoride diets on develop-ing enamel and dentin in the incisors of rats. Am J Anat1966;118:665–83.
42. Thylstrup A. A scanning electron microscopical study ofnormal and fluorotic enamel demineralized by EDTA.Acta Odontol Scand 1979;37:127–35.
43. Shinoda H, Ogura H. Scanning electron microscopicalstudy on the fluorosis of enamel in rats. Calcif Tissue Res1978;25:75–83.
44. Bhussry BR. Chemical and physical studies of enamelfrom human teeth: density and nitrogen content of mot-tled enamel. J Dent Res 1959;38:369–73.
45. Giambro NJ, Prostak K, DenBesten PK. Characterizationof fluorosed human enamel by color reflectance, ultra-structure, and elemental composition. Caries Res1995;29:251–7.
46. Shinoda H. Effects of long-term administration of fluo-ride on the enamel formation in rats. In: Suga S, editor.Mechanisms of tooth enamel formation. Tokyo:Quintessence: 1983. p. 273–84.
47. DenBesten PK, Crenshaw MA. The effects of chronichigh fluoride levels on forming enamel in the rat. ArchOral Biol 1984;29:675–9.
48. DenBesten PK. Effects of fluoride on protein secretionand removal during enamel development in the rat. JDent Res 1986;65:1272–7.
49. Dajean S, Menanteau J. A western-blotting study ofenamel glycoproteins in rat experimental fluorosis. ArchOral Biol 1989;34:413–8.
50. Suga. Histochemical observation or proteolytic enzymeactivity in the developing dental hard tissues of the rat.Arch Oral Biol 1970;15:555–8.
51. DenBesten PK, Heffernan LM. Enamel proteases in secre-tory and maturation incisor enamel of rats ingesting 0and 100 ppm fluoride in drinking water. Adv Dent Res1989;3:199–202.
52. Smith CE, Borenstein A, Fazek A, Nanci A. In vitro stud-ies of the proteinases which degrade amelogenins in de-veloping rat incisor enamel. In: Fearnhead RW, editor.Tooth enamel V. Yokahama: Florence; 1989. p. 286–9.
53. Overall CM, Limeback H. Identification and character-
46
ization of enamel proteinases isolated from developingenamel. Amelogeninolytic serine proteinases are associ-ated with enamel maturation in pig. Biochem J1988;256:965–72.
54. DenBesten PK, Heffernan LM. Separation by polyacryl-amide gel electrophoresis of multiple proteases in rat andbovine enamel. Arch Oral Biol 1989;34:399–404.
55. Simmer JP, Fukae M, Tanabe T, Yamakoshi Y, Uchida T,Xue J, et al. Purification, characterization, and cloningof enamel matrix serine proteinase 1. J Dent Res1998;77:377–86.
56. Ekstrand J, Foman SH, Ziegler EE, Nelson SE. Fluoridepharmacokinetics in infancy. Pediatr Res 1994;35:157–63.
57. Whitford GM. Determinants and mechanisms of enamelfluorosis. Ciba Found Symp 1997;205:226–41.
58. Angmar-Mansson B, Whitford GM. Environmental andphysiological factors affecting dental fluorosis. J DentRes 1990;69(Spec Iss):706–13.
59. Pendrys DG, Stamm JW. Relationship of total fluorideintake to beneficial effects and enamel fluorosis. J DentRes 1990;69(Specc Iss):529–38.
60. Whitford GM. Effects of plasma fluoride an dietarycalcium concentrations on GI absorption and secretion offluoride in the rat. Calcif Tissue Int 1994;54:421–5.
61. Whitford GM, Pashley DH. Fluoride absorption: the in-fluence of gastric acidity. Calcif Tissue Res 1984;36:302–7.
62. Whitford GM, Angmar-Mansson B. Fluorosis-like effectsof acidosis, but not NHπ4, on rat incisor enamel. CariesRes 1995;29:20–5.
63. DenBesten PK. Dental fluorosis: its use as a biomarker.Adv Dent Res 1994;8:105–10.
64. Richards A, Kragstrup J, Josephsen K, Fejerskov O. Den-tal fluorosis developed in post-secretory enamel. J DentRes 1986;65:1406–9.
65. Suckling G, Thurley DC, Nelson DG. The macroscopicand scanning electron-microscopic appearance andmicrohardness of the enamel, and the related histologicalchanges in the enamel organ of erupting sheep incisorsresulting from a prolonged low daily dose of fluoride.Arch Oral Biol 1988;33:361–73.
66. Ishi T, Nagaki H. Study of the correlation between thedegree of dental fluorosis and the duration of fluoridepresent in drinking water. In: Fearnhead R, Suga S, edi-tors. Tooth enamel IV. Amsterdam: Elsevier Science;1984. p. 338–41.
67. Evans RW. An epidemiological assessment of the chrono-logical distribution of dental fluorosis in human maxil-lary central incisors. J Dent Res 1993;72:883–90.
68. Evans RW, Darvell BW. Refining the estimate of the criti-cal period for susceptibility to enamel fluorosis in humanmaxillary central incisors. J Public Health Dent1995;55:238–49.
69. Ishii T, Suckling G. The severity of dental fluorosis inchildren exposed to water with a high fluoride contentfor various periods of time. J Dent Res 1991;70:952–6.
70. Burt BA. The changing patterns of systemic fluoride in-take. J Dent Res 1992;71:1228–37.
71. Ishii T, Suckling G. The appearance of tooth enamel inchildren ingesting water with a high fluoride content fora limited period during early tooth development. J DentRes 1986;65:974–7.
72. Pendrys DG, Katz RV. Risk of enamel fluorosis associatedwith fluoride supplementation, infant formula, and fluo-ride dentifrice use. Am J Epidemiol 1989;130:1199–208.
73. DenBesten PK, Thariani H. Biological mechanisms offluorosis and level and timing of systemic exposure to

Fluoride mechanisms relevant to supplement usage
fluoride with respect to fluorosis. J Dent Res1992;71:1238–43.
74. Hodge HC. The concentration of fluorides in the drink-ing water to give the point of minimum caries with maxi-mum safety. J Am Dent Assoc 1950;40:436–9.
75. Angmar-Mansson B, Ericsson Y, Ekberg O. Plasma fluo-ride and enamel fluorosis. Calcif Tissue Res 1976;22:77–84.
47
76. Myers HM. Dose-response relationship between waterfluoride levels and the category of questionable dentalfluorosis. Community Dent Oral Epidemiol 1983;11:109–12.
77. Holm AK, Andersson R. Enamel mineralization distur-bances in 12-year-old children with known early expo-sure to fluorides. Community Dent Oral Epidemiol1982;10:335–9.