Embed Size (px)
Citation preview

Biological Assessment for micro-AMS Thyroid Cancer Cells using Iodine-125
Daniel José Gonçalves Bidarra
Thesis to obtain the Master of Science Degree in
Biomedical Technologies
Supervisors: Prof. Patrícia Maria Cristovam Cipriano Almeida de Carvalho,
Dra. Maria Micaela Fonseca
Examination Committee
Chairperson: Prof. Raúl Daniel Lavado Carneiro Martins
Supervisor: Dra. Maria Micaela Fonseca
Member of the Committee: Dra. Maria Lurdes Barrela Patrício Gano
November 2014

ii

iii
“Os que se encantam com a prática sem a ciência são como os timoneiros que entram no navio sem timão nem bússola, nunca tendo certeza do seu destino”
Leonardo Da Vinci

iv

v
Acknowledgments
É sempre complicado agradecer algo a quem temos tanto a agradecer e no final de contas não
sabemos bem como fazê-lo mas aqui vai.
Primeiro que tudo, quero agradecer à minha familia, pais e irmãos por toda a força e incentivo que me
deram para que continuasse o meu trabalho e desse o meu melhor.
Em segundo lugar queria agradecer à minha orientadora, Dra. Micaela Fonseca, por todo o apoio e
compreensão e ajuda dada durante esta dissertação. Um agradecimento também à Prof. Patricia
Carvalho pela orientação e porque sem ela este trabalho também não teria sido possível.
Queria também agradecer ao Hugo Silva e à Cátia Santos por todo o companheirismo em dias e dias
no CTN e também a toda a ajuda por eles prestada.
Um agradecimento à Catarina Tavares, investigadora do IPATIMUP, porque sem ela este trabalho
também não era possível, pois foi uma peça fundamental nesta investigação e que também tanto me
ajudou.
O meu muito obrigado à Dra. Lurdes Gano, ao Prof. João Cruz, à Prof. Adelaide Jesus, à Rute e à
Catarina por todas as ajudas.
O meu agradecimento à minha amiga Leticia e companhia por todos os bons momentos e almoços, e
também à Nadine por toda a ajuda e disponibilidade.
E por último, mas talvez o mais importante, quero agradecer à Inês pelo seu enorme apoio e
compreensão, por toda a força que me deu e por ser a mulher que é que eu admiro tanto e que sem
ela isto não era mesmo possível.

vi

vii
Abstract
This project aims to find the best thyroid cells for biological sample preparation using iodine 125 (125I)
in study of the symporter NIS.
In the future, the choosen cells will be prepared for the µAMS (micro-Accelerator Mass Spectrometry)
technique, as µAMS could be an alternative to measure the quantity of iodine present inside de cell
with sensitivity higher than other existing technique even in small samples.
The use of 125I will allow knowing which radioactive activities could be given to the cellular cultures as
well as understand the cellular uptake mechanisms. The 125I uptake assay will be a reference protocol
for 129I.
When applying the 129I µAMS technique to biological samples, such as the thyroid gland, there is the
necessity of prepare specific standards and samples for a posterior use in µAMS facility. The use of 129I in studies of thyroid cancer therapy, through the implementation of high sensitivity analysis
technique - µAMS facility at CTN / IST.
Due to the µAMS high sensitivity and the low specific activity of the iodine-129, there are advantages
in using it in the future in preclinical research for clinical verification concerning the existence of an
inability to capture iodine-131 as well as in evaluation of the residual disease.
The inovation of this project lays in the association among well established experimental techniques
related to cellular manipulation and radioactive uptake assays with the physical and more
experimental nature of 129I-µAMS technique applied to biomedical science.
The combination of these two distinct areas may improve the follow-up for patients with thyroid cancer,
especially in those whose therapy became inefficient and there was a relapse of the disease.
In addition it may also contribute to the development of safer methods for patients and caregivers
through the use of less harmful isotopes and minimal radioactive doses, thus reducing all the concerns
related with radiological protection and safety.
Key-Words
Iodine, Thyroid, micro-AMS, Iodine-125

viii

ix
Resumo Este projeto visa encontrar as melhores células para a análise por AMS de células da tiróide e do
canal NIS usando iodo-125. Além disso, este projecto irá permitir a aplicação no futuro de iodo-129 no
seguimento de doentes com cancro da tiróide, recorrendo à implementação da capacidade de
analisar com alta sensibilidade da µAMS (micro espectrometria de massa de iões acelerados) na
instalação existente no CTN/IST.
A utilização do 125I irá permitir saber quais as actividades radioactivas que se podem dar às celulas da
tiróide, bem como, compreender os mecanismos celulares de captação de iodo radioactivo. O ensaio
de captação com 125I funcionará como o protocolo de referência para o 129I.
Ao empregar-se a técnica de µAMS com iodo-129 a amostras biológicas, tal como a glândula da
tiróide, manifesta-se a necessidade de utilizar uma técnica de referência em estudos de captação
com iodo radioativo, tal como a aplicação de iodo-125 para a análise in vitro de células da tiróide.
Devido à elevada sensibilidade da técnica de µAMS e à fraca atividade específica do iodo-129,
existem vantagens em utilizá-la em investigação pré-clínica para avaliar a incapacidade celular para a
captação do iodo-131, bem como na avaliação da doença residual.
O caráter de inovação deste projeto surge, não só da técnica de análise, mas também, da associação
entre as técnicas laboratoriais bem estabelecidas relacionadas com a manipulação de culturas
celulares e ensaios de captação radioativa com o caráter mais físico e experimental da aplicação da
técnica de µAMS com iodo-129 à área biomédica.
A associação destas duas áreas distintas poderá conduzir a resultados relevantes para a qualidade
do seguimento de doentes com cancro da tiróide, em especial aqueles em que a terapêutica se
tornou ineficaz e houve uma recidiva na doença, bem como, contribuir para o desenvolvimento de
métodos mais seguros para o doente e para os técnicos de saúde com recurso a isótopos com menor
grau de agressividade e com doses mínimas.
Palavras-Chave
Iodo, Tiróide, micro-AMS, Iodo-125

x

xi
Table of Contents
Acknowledgments……………………………………………………………………………………………..V
Abstract………………………………………………………………………………………..……………….VII
Resumo………………………………………………………………………………………………….………IX
List of Tables………………………………………………………………………………………..………...XV
List of Graphs……………………………………………………………………………….………….……XVII
List of Figures………………………………………………………………..………..………………….....XIX
Abreviations……………………………………………………………..…………..………..……………...XXI
Chapter 1 – Introduction…….……………………………………………………………………………….23
1.1 Motivation………………………………………………………………………………………………….23
1.2 Goals.………………………………………………………………………………………………………24
1.3 Statistics……………………………………………………………………………………………………25
1.3.1 Incidence………………………………………………………………………………………………….25
1.3.2 Mortality…………………………………………………………………………………………………...26
1.3.3 Risk Factors………………………………………………………………………………………………27
1.3.3.1 Gender and Age…………………………………………………………………………………….…28
1.3.3.2 Radiation Exposure…………………………………………………………………………….……..28
1.3.3.3 Low Iodine Diet…………………………………………………………………………….…………..28
1.3.3.4 Hereditary Conditions………………………………………………………………………………....28
Chapter 2 – State of the Art………………………………………………………………………………….29
2.1 Endocrine System…………………………….……………………..……………………………………..29
2.1.1 Thyroid Gland….………………….……………………………………………………………………...29
2.1.2 Physiopathology….…..…………………………………………………………………………………..30
2.1.2.2 FTC……………...………………………………………………………………………………………31
2.1.2.3 Hurthle Cell Tumor…………………………………...……………………………….……………….31

xii
2.1.2.4 PTC…………………………………………………………………………………….………………..31
2.1.2.5 Undifferentiated (Anaplastic) Carcinoma………………………………………………………...….31
2.1.2.6 MTC……………………………………………………………………………………………………..32
2.1.2.7 Non-Epitelial Carcinoma………………………………………………………………………..……..33
2.1.3 Causes of Thyroid Cancer………………………………………………………………………………33
2.2 125I - Radiodide Uptake Assay…………………………………………………………………………..34
2.2.1 Iodine125……………………………………………………………………………………………...….34
2.2.2 Genotype …………………………………………………..…………………………………………….35
2.2.3 Type of Cells – Cell Lines………………………………………………………………………………35
2.3 AMS………………….…………..………………………………………………………………………….36
2.3.1 History – Biomedical………………………….……………………………….…………………………36
2.2.2 AMS and micro-AMS ……………………………………………………………….………………...…37
2.2.3 AMS Biomedical Applications…………………………………………………………………………..39
2.2.4 AMS – 129I…………………………………………………………………………………………………40
2.2.6 Sample and Standard Preparation…………………………………………...…………………….….41
2.2.6.1 129I Sample and Standard Preparation……………………………………………………………...42
2.2.6.2 129I Standard Preparation…………………………………………………………………………….43
2.2.6.2 129I Sample Preparation………………………………………………………………………………49
2.2.6.3 129I Target Preparation………………………………………………………………………………..49
2.2.6.4 129I Sample Preparation – Biological Sample (Thyroid)……………..……………………………49
Chapter 3 – Experimental……………………………………………………………………………………53
3.1 125I Uptake Assay…………………………………………………………………………………………..53
3.1.1 Method of Preparation………………………………………………………………….………………..53
3.1.1.1 Materials……………………………………………………………………………….………………..54
3.1.1.2 Protocol (General)……………………………………………………………………………………..55
3.1.1.3 Experimental Setup…………………………………………………….…………………………......55

xiii
3.2 Method of Preparation - AMS Biological Sample (Thyroid)……………………………………………62
3.2.1 129I Radioactive Activity to Cells………………………………………………………………………..62
3.2.2 Sample Preparation at CTN/IST…………………………………………………………………….....63
Chapter 4 - Results and Discussion……………………………………………………………………….66
4.1 Iodine Uptake Assay……………………………………………………………………………………….66
4.1.1 First Experimental Assay………………………………………………………………………………..66
4.1.2 Second Experimental Assay……………………………………………………………………………72
4.2 Discussion…………………………………………………………………………………………………..77
4.2.1 First Experiment………………………………………………………………………………………….77
4.2.2 Second Experiment………………………………………………………………………………………78
4.2.3 Experimental Procedure…………………………………………………………………………………79
Chapter 5 – Conclusions…………………………………………………….………………………………81
5.1 125I Uptake Assay…………………………………………………………………………………………..81
5.2 AMS Sample Preparation………………………………………………………………………………….82
5.3 Final Conclusions – Future Prespectives………………………………………………………………..82
Bibliography…………………………………………………………………………………………………....83
Appendix A……………………………………………………………………………………………....……A-1

xiv

xv
List of Tables
Table 1.1: Thyroid - Estimated incidence, all ages: both sexes…….……..……………………………...25
Table 1.2: Thyroid - Estimated incidence, all ages: female…………………………...............................26
Table 1.3: Thyroid - Estimated incidence, all ages: male………………………………...………………..26
Table 1.4: Thyroid - Estimated mortality, all ages: both sexes………………………………..…………..26
Table 1.5: Thyroid - Estimated mortality, all ages: female…………………………………….…………..27
Table 1.6: Thyroid - Estimated mortality, all ages: male………………………………………..……….…27
Table 3.1: Studies Performed using Thyroid Cell lines in 125I Uptake Assays….…………..………..….61
Table 3.2: AMS Biological Sample Preparation Reagents…………………………………………...……63
Table 4.1: 125I Uptake Values of XTC-1 Thyroid Cells (cpm)…………..……………………………….....66
Table 4.2: 125I Uptake Values of XTC-1 Thyroid Cells with KClO4 (cpm)……..……………………..…..66
Table 4.3: 125I Uptake Values of K1 Thyroid Cells (cpm)………………………………………….………67
Table 4.4: 125I Uptake Values of K1 Thyroid Cells with KClO4 (cpm)……….….…………………….….67
Table 4.5: NaOH Absorbance values per specific solution concentrations- Standards………..……....68
Table 4.6: Absorbance values per specific solution concentrations - Standards NaOH…………..…...69
Table 4.7: Protein Concentration for K1 and XTC-1………………………………………………..………70
Table 4.8: Protein Quantification for K1 and XTC-1……………………………………………..…………70
Table 4.9: 125I Uptake Values of XTC-1 Thyroid Cells (cpm)……………………………….…....………..72
Table 4.10: 125I Uptake Values of XTC-1 Thyroid Cells with KClO4(cpm)………………..………..…….72
Table 4.11: 125I Uptake Values of K1 Thyroid Cells (cpm)…………….…...…………............................72
Table 4.12: 125I Uptake Values of K1 Thyroid Cells with KClO4(cpm)……………………..………...…..73
Table 4.13: Iodide Uptake in PCCL3 Thyroid Cell line (Concentration of NaI: 1mM)…...………….…..73
Table 4.14: Iodide Uptake in PCCL3 Thyroid Cell line (Concentration of NaI: 100µM) …….……..…..74
Table 4.15: NaOH (0.5M) Standards………………………………………………………………..……….75
Table 4.16: Total Protein Quantification for PCCL3 cells……………….………………………..………..76

xvi
Table 4.17: Protein Quantification per cpm for PCCl3 (1mM NaI)………...……...................................77
Table 4.18: Protein Quantification per cpm for PCCl3 (100µM NaI)…………………………………..….77

xvii
List of Graphs Graph 4.1: 125I Uptake for XTC-1 Thyroid Cells with and without KClO4………..……………………...67
Graph 4.2: 125I Uptake for XTC-1 Thyroid Cells with and without KClO4………..……………………..68
Graph 4.3: Concentration vs Absorbance (Standard NaOH) – Linear Regression..............................69
Graph4.4: Quantity of 125I Uptake per µg of Protein in PCCL3 (1mM NaI) with and without
KClO4………………………………………………………………………………………………….…………71
Graph 4.5: Quantity of 125I Uptake per µg of Protein in PCCL3 (100 µM NaI) with and without
KClO4…………………………………………………………………………….………………………………71
Graph 4.6: K1 cells cpm for quantity of protein with and without KClO4………………………..……….74
Graph 4.7: XTC-1 cells cpm for quantity of protein with and without KClO4……………………….……75
Graph 4.8: Protein Concentration vs Absorbance with Linear Regression………………………...……76

xviii

xix
List of Figures
Figure 2.1: Thyroid Gland Anatomy………………………………………………….……………….……...30
Figure 2.2: Combustion Process…………………………………………………………………..…………45
Figure 3.1: Ionization Chamber for Dose Calibration…………………………………………..…….…....54
Figure 3.2: Multi-Crystal LB 2111 Gamma Counter……………………………………………..…………54
Figure 3.3: Microplate UV-Vis Spectrophotometer……………………………………………....…………55
Figure 3.4: Stocks A, B and C (preparation and concentrations)……………………………..………….56
Figure 3.5: Preparation of solutions A and B…………………………….…………………………….……57
Figure 3.6: Preparation of NaI and KClO4 solutions………………….………………………..…………..58
Figure 3.7: Preparation of stock A; *D.C: Dose Calibrator………….…………………….………….……59
Figure 3.8: Preparation of stocks B1 and B2……………………………………………..…………………59
Figure 3.9: Preparation of stocks C1 and C2…………………………………..…………………...………60
Figure 3.10: AgIO3 Precipitate……………………………………………..…………………….……...……64
Figure A.1.1: Principle of functioning of µAMS for isotope 129I…………………………..………………A-1
Figure A.1.2:Tandem Accelerator at LATR-CTN/IST…………………….……………………………….A-2
Figure A.1.3: Ionization Chamber at LATR-CTN/IST………………….….………………………………A-3
Figure A.2.1: Nulcear reactions line –Quadrupole……………….……………………….…..……..……A-4
Figure A.2.2: Nuclear reactions line - End line view……………………………….………………..……A-4
Figure A.2.3: Inside view of the nuclear reactions line – Copper structure for beam
focusing…………………………………………………………………………………………………………A-5
Figure A.2.4: Nuclear reactions chamber inside in, with MOVD and MOVE detectors, beam stopper,
electron gun, collimator and silver plate…………………………………………………………….……....A-5

xx

xxi
Abreviations AMS – Accelerator Mass Spectrometry
AUSTRALIS – AMS for Ultra Sensitive TRAce eLement and Isotopic Studies
CCD – Charge-Coupled Device
DNA – Deoxyribonucleic Acid
ESA – Electrostatic Spherical Analyser
FTC – Follicular Thyroid Cancer
GDMS – Glow Discharge Mass Spectrometry
GM – Geiger-Muller
HBSS – Hank’s Balanced Salt Solution
HPLC – High Performance Liquid Chromatography
HPT – Hypothalamus-Pituitary-Thyroid axis
HVL – Half Value Layer
IC – Ion Chromatography
ICP-MS – Inductively Coupled Plasma – Mass Spectrometry
LA-ICP-MS – Laser Ablation - Inductively Coupled Plasma – Mass Spectrometry
LLNL – Lawrence Livermore National Laboratory
LSC – Liquid Scintillation Counter
MAPK – Mitogen Activated Protein Kinase
NBF – Negative Biofeedback System
NIS – Sodium Iodide Symporter
NIST – National Institute of Standards and Technology
PI – Phosphatidylinositol
PI3K – Phosphatidylinositol-3-Kinase
PTC – Papillary Thyroid Cancer
RIMS – Resonance Ionization Mass Spectrometry

xxii
RNA – Ribonucleic Acid
RNAA – Radiochemical Neutron Activation Analysis
SIMS – Secondary Ion Mass Spectrometry
TIMS – Thermal Ionization Mass Spectrometry
TSH – Thyroid Stimulating Hormone
VERA – Vienna Environmental Research Accelerator

23
Chapter 1
Introduction
The multiple thyroid pathologies are, frequently, associated with subtle and non-specific clinical
practice. The investigation to allow a more accurate diagnosis and following of these diseases became
an essential tool. Alternative therapies, new biomarkers and new techniques of detection have been
increasing to find new pathways for oncological cases without effective resolutions3,29.
The main function of thyroid gland is the production of essential hormones for energetic regulation,
growth, development and maturation of several organs.45For a normal hormone production it is
necessary a normal development of the gland, an appropriate running and regulation of the
biosynthesis mechanism and a normal iodine intake. The iodine is a halogen element present in the
human body, and due to its great affinity, the iodine radioactive isotopes are commonly used for
diagnosis - iodine-123 (123I), and for therapy - iodine-131 (131I) - of thyroid pathologies29.
Thyroid pathologies can be treated with antithyroid drugs, radioactive iodine (131I) or by surgical
removal of the thyroid glands. The administration of antithyroid drugs creates controversy due to
immunosuppressive effects in some patients, and the surgical ablation is becoming less used. Finally,
the radioiodine therapy is also a controversial option due to the radiation exposure of patients and all
the risks associated with this process, although, the therapy is more economical and easier. However,
the current problematic associated with treatment of thyroid pathologies is due to the cases of relapse
or regression of disease where the therapeutic applied no longer make effect, so it is necessary to find
alternatives24,29,34.
The initial goal of this investigation is to develop an alternative technique that permits the follow-up of
thyroid cancer patients by a radioactive method with high sensitivity in detection of iodine present
inside the thyroid cells. The technique selected was micro accelerator mass spectrometry (µAMS)
using 129I to do the measurement of biological samples (thyroid) for determination of the isotopic ratios 127I/129I, and by this way, determine the amount of radioactive iodine present in thyroid cells.
Unfortunately, the measurement of thyroid cells could not be performed because the µAMS system
present in LATR-CTN/IST was not operable for 129I. Although, it was possible to prepare 129I-biological
samples for AMS using human thyroid cells, an innovative approach never applied.
1.1 Motivation Most of the cases of thyroid cancer (≈ 80%) are successfully treated with radioactive iodine (RAI)
therapy with 131I, however for 20% of the cases there is a regression of the disease and in these cases
the therapeutic with radioactive iodine is no longer available.

24
The incapability of tumor thyroid cells to incorporate iodine is a complex process being the object of
investigation, as well as, the recurrence of the disease after therapy.
It is crucial to study and understand the cellular mechanisms activated in iodine uptake to in the future
find alternative therapeutics. The need of find an alternative therapy in these cases is crucial and
object of investigation. To understand why tumor thyroid cells stop to incorporate iodide, different tools
are applied. In this work, the sample preparation is developed in order to use µAMS technique in
thyroid cells for the first time. This technique is capable to detect if iodide is present in a cell or not,
even in small quantities (1-2 mg) due to its high sensitivity.
The application of 129I with µAMS in biomedical approaches is recent, and there is only one case in
Argentina, where it was used in measurement of 129I of bovine thyroids. Furthermore, the µAMS is an
unique technique in Portugal only exists in Lisbon in Campus Tecnológico e Nuclear (CTN/IST).
1.2 Goals The main goal of this investigation is to find the best thyroid cells for µAMS analysis and biological
sample preparation using iodine-125 (125I) in study of the NIS symporter. Besides that, apply these
cells, in the future, with accelerator mass spectrometry (AMS) using iodine 129 (129I).
The utilization of 129I µAMS in biological samples as thyroid cells has never been performed
previously. Due to this fact, it was necessary implement and adapt cellular culture manipulation
standard protocols for radioiodide therapy. One of the standards protocols applied in radioiodide
uptake assays is the 125I. The use of 125I will allow knowing which radioactive activities could be given
to the cellular cultures as well as understand the cellular uptake mechanisms. The 125I uptake assay
will be a reference protocol for 129I.
Besides that, the 129I has a large advantage due to the fact that is a long-lived radionuclide (15.7
million of years), which allows the administration of low doses and consent the manipulation of 129I as
a stable isotope with minimal safety and radiological protection concerns.
In order to accomplish the previous goals it is necessary to follow a work plan that implies intermediate
goals as:
i. Determination of the radioactive activity to be given to thyroid cells;
ii. Make a comparative study with 125I;
iii. Preparation of biological samples for 125I;
The preparation of biological samples for µAMS using 129I is a very recent approach and the use of
thyroid cells from cellular cultures with this technique was never been performed previously.
The experiments with 125I give us the knowledge necessary to know which is the radioactive activity
that can be administrated to the cells, how they react, if there is iodine uptake from cells and which is
the uptake percentage in normal and cancer cells.

25
1.3 Statistics According to the World Health Organization (WHO)15 for 2012 (GLOBOCAN), 8.2 million of people
died all over the world from cancer. From these, 39769 deaths were caused by thyroid cancer, and it
affects more than 298.000 people. The existence of thyroid nodules is common but thyroid cancer is
relatively rare. The overall incidence of cancer in cold nodules is just 5-15%. This value increases in
extreme ages. In general, thyroid carcinomas, clinically detectable, are only 1% of all human
cancers16.
In Europe16, there were 52.9 thousand cases in 2012 and caused more than 6.3 thousand deaths. In
Portugal, thyroid cancer affects more than 500 people (one third are women) and has a mortality rate
of 0.3% for both sexes16,17.
In comparison with Europe and the rest of the world, Portugal has lower values of incidence and
mortality, as illustrated in the following tables17.
1.3.1 Incidence
Table 1.1: Thyroid Cancer - Estimated incidence, all ages: both sexes77
POPULATION Numbers Crude Rate ASR (W) Cumulative risk World 298102 4.2 4.0 0.40 WHO Europe region (EURO)
62811 7.0 5.4 0.53
Europe 52956 7.1 5.2 0.52 European Union (EU-‐28)
37440 7.4 5.4 0.54
Southern Europe
13761 8.7 6.3 0.65
Portugal 576 5.4 3.2 0.37 ASR: Age Standardized Rate
Table 1.2: Thyroid Cancer - Estimated incidence, all ages: female78
POPULATION Numbers Crude Rate ASR (W) Cumulative risk World 229923 6.6 6.1 0.60 WHO Europe region (EURO)
48775 10.5 8.1 0.79
Europe 40672 10.6 7.8 0.77 European Union (EU-‐28)
27718 10.7 7.9 0.77
Southern Europe
9938 12.4 8.6 0.91
Portugal 449 8.1 4.6 0.53

26
Table 1.3: Thyroid Cancer - Estimated incidence, all ages: male79
POPULATION Numbers Crude Rate ASR (W) Cumulative risk World 68179 1.9 1.9 0.19 WHO Europe region (EURO) 14036 3.2 2.5 0.25
Europe 12284 3.4 2.5 0.26 European Union (EU-‐28)
9722 3.9 2.9 0.29
Southern Europe
3823 4.9 3.8 0.38
Portugal 127 2.4 1.6 0.19
1.3.2 Mortality
Table 1.4: Thyroid Cancer - Estimated mortality, all ages: both sexes80
POPULATION Numbers Crude Rate ASR (W) Cumulative risk World 39769 0.6 0.5 0.06 WHO Europe region (EURO) 7467 0.8 0.4 0.05
Europe 6334 0.9 0.4 0.04 European Union (EU-‐28) 3637 0.7 0.3 0.03
Southern Europe
1219 0.8 0.3 0.03
Portugal 93 0.9 0.3 0.04
Table 1.5: Thyroid Cancer - Estimated mortality, all ages: female81
POPULATION Numbers Crude Rate ASR (W) Cumulative risk World 27142 0.8 0.6 0.07 WHO Europe region (EURO)
5088 1.1 0.5 0.06
Europe 4267 1.1 0.4 0.05 European Union (EU-‐28)
2268 0.9 0.3 0.03
Southern Europe
762 1.0 0.3 0.04
Portugal 60 1.1 0.3 0.04

27
Table 1.6: Thyroid Cancer - Estimated mortality, all ages: male82
POPULATION Numbers Crude Rate ASR (W) Cumulative risk World 39769 0.6 0.5 0.06 WHO Europe region (EURO) 7467 0.8 0.4 0.05
Europe 6334 0.9 0.4 0.04 European Union (EU-‐28)
3637 0.7 0.3 0.03
Southern Europe
1219 0.8 0.3 0.03
Portugal 33 0.6 0.3 0.03
1.3.3 Risk Factors The amount of factors that could induce a thyroid cancer are not clear and there are very few risk
factors for this type of cancer. One patient with a clinical evaluation that reveals more than one risk
factor has a higher probability of having a thyroid cancer, but it is not possible to know how much each
factor contributes to cause cancer3.
The main risk factors for thyroid cancer are: gender and age, radiation exposure, iodine intake (low
iodine diet) and hereditary conditions and family history3,29.
1.3.3.1 Gender and Age
Thyroid cancer occurs almost three times more in women than in men. In terms of age, thyroid cancer
can appear in any age, but for women the risk peaks are earlier, between 40 and 50 years old3.
1.3.3.2 Radiation Exposure
In terms of radiation exposure there are several types that are considered as risk factors for thyroid
cancer: therapeutic radiation provided in medical treatments as therapy with radionuclides; radiation
fallout resulting from nuclear weapon tests and radiation from nuclear accidents3,29.
Low radiation levels from high natural background radiation are not considered as a high risk factor for
thyroid cancer. As well as, the geographic variations in natural background radiation in association
with the risk of developing a thyroid cancer remains equivocal3,29.
1.3.3.3 Low Iodine Diet
A diet with low amounts of iodine can lead to the development of follicular thyroid cancer (FTC). The
risk increases proportionally to radiation exposure.29In the United States and South Europe countries
as Portugal, Spain, Italy and Greece (mediterranean diet) people get enough iodine due to ingestion of
table salt and other aliments rich in iodine in their diet29.

28
1.3.3.4 Hereditary conditions and family history
The hereditary conditions are associated with medullary thyroid carcinomas (MTC). The risk of having
MTC increases in a person with a family history of MTC due to hereditary gene mutations. One third of
the MTC result of these abnormal genes, being named familial MTC (FMTC)3.
The changes in genes can lead to other endocrine complications. The association between FMTC and
other endocrine tumors can origin a multiple endocrine neoplasia type 2 (MEN 2). This neoplasia can
be divided into two subtypes: MEN2a and MEN2b. In the first one, there is the development of
pheochromocytomas*. In the second, both endocrine and neurological systems are affected with the
development of pheochromocytomas and neuromas3.
*Pheocromocytoma: a rare catecholamine-secreting tumor that may precipitate life-threatening hypertension.

29
Chapter 2
State-of-the-art
2.1 Endocrine System
The human body is constituted by several systems and organs that ensure its normal functioning. The
endocrine system is one of the regulatory mechanisms present in the human body, in parallel, with
neurological and muscle-skeletal systems54,66.
The endocrine system is essential to assure the normal functioning of cells and organs by controlling
and biofeedback mechanisms - Homeostasis. The homeostasis is dependent of a precise regulation of
organs and systems. The endocrine system in cooperation with neurologic system is responsible for
regulate and coordinate almost all structures of the human body54,66.
In terms of composition, the endocrine system is constituted by hormonal glands that are capable to
detect minimal hormonal variations in the bloodstream and regulate hormonal secretion. Histologically,
the endocrine glands have in its composition conjunctive tissue, made by epithelial cells aggregates,
rich in blood and lymphatic capillaries54,66.
The main endocrine glands are pituitary, thyroid, parathyroid, adrenals, pancreas, ovaries and
testicles. The pituitary is the principal gland that directly or indirectly influences the production and
release of other hormones. Hormones are chemical signals produced by endocrine glands and/or
endocrine cells present in other organs, whose segregations are released directly in bloodstream and
transported to target cells54.
The hormone secretion is mediated by a negative biofeedback mechanism (NFB),the endocrine
glands regulate their secretory activity by a pulsatile way with drastical variations overtime. Any
problem in NFB mechanism can originate hormonal dysregulations, and subsequently, endocrine
diseases induced by: hormonal excess, hormonal deficit or hormonal resistance66.
2.1.1 Thyroid Gland
The thyroid gland is an endocrine gland located in the lower third of the neck, below the larynx,
surrounding by the anterior trachea at C5-T1 vertebrae level, and between the sternum-thyroid and
sternum-hyoid muscles. It is a high vascularized organ, supplied by thyroid arteries and drained by
thyroid venous plexus. The hormone secretion is regulated by hypothalamus-pituitary-thyroid (HPT)
axis54.
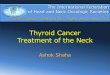
The thyroid gland is constituted by two lobules connected by an isthmus (Figure 2.1). Is one of the
largest endocrine gland with an approximate weight of 15-25 grams, being heavier in women.

30
Figure 2.1: Thyroid Gland Anatomy84
©2011 Pearson Eduction, Inc.
Histologically, the thyroid gland is enclosed by a layer of conjunctive tissue and formed by little
lobules. Each lobule is formed by dozens of small spherical vesicles named follicles. These are the
functional units of the gland,having the function of thyroid hormones synthesis.: T3 and T4.
Furthermore, the thyroid gland is mainly composed by two types of cells: the follicular cells, that form
circumferences trapping a substance in the center named colloid and the parafollicular cells (or C
cells)54,66.
The thyroid gland has a specific quality that differentiates it from other endocrine glands, which is the
capability of store large amounts of hormones, in an inactive way, inside of the extracellular
compartments (the colloid) instead of other endocrine glands that store few quantities of hormone at
intracellular compartments. In normal conditions, despite being superficial, the thyroid gland is not
palpable66.
2.1.2 Physiopathology
The thyroid gland is an endocrine gland with a large amount of pathologies: benign and malignant. For
example, hypothyroidism is a benign pathology, on the other hand, the thyroid cancer is a malignant
disease. The majority of thyroid cancers are constituted by two types of differentiated carcinomas:
papillary and follicular29.
The thyroid cancer can be classified taking in account the tissue origin: epithelial and non-epithelial.
Epithelial tumors affect follicular cells and origin the differentiated thyroid carcinomas: follicular thyroid
carcinoma (FTC), papillary thyroid carcinoma (PTC), undifferentiated (anaplastic) carcinoma, Hurthle
cell tumor with follicular cell differentiation, and also, the medullary thyroid carcinoma (MTC) that
involves the parafollicular cells. The non-epithelial tissue yields the sarcomas and the malignant
lymphomas. On the following paragraphs each type of thyroid cancer will be explained in detail29.

31
2.1.2.1 FTC The FTC is a malignant tumor that involves follicular cell differentiation. It is one of the most common
thyroid cancers, affecting mainly the iodide-deficient areas with a total percentage between 25 to 40%
of all thyroid cancers29.
Although, the FTC tumors can have different morphological and biological behavior, whereby, follicles
is not the only specific caractheristic of these tumors. . Asexample, some PTC tumors can exhibit
follicular structure29.
2.1.2.2 Hurthle Cell Tumor Hurthle cells are modified large follicular cells with large nuclei and granular cytoplasm. These cells
can be visualized in thyroid lesions as nodular goitre, Hashimoto’s thyroiditis, non-specific chronic
thyroiditis and follicular neoplasms29.
The classification of Hurthle cell tumors is controversial due to their biological behaviour. Some
authors consider them as a subtype of follicular neoplasms due to similar degree of invasion and
differentiation compared with other follicular neoplasms. On the other hand, other authors, considered
Hurthle cell tumors as independent tumors with specific cells (Hurthle cells) with different pathology
patern and behaviour. Hurthle cell carcinomas are characterized by invasion level and also by low
levels of radioiodine absorption3.
2.1.2.3 PTC The PTC is a malignant epithelial tumor with follicular differentiation. The PTC is, in fact, the most
common thyroid cancer, representing 90% of the total pediatric thyroid cancers29.
The PTC prognosis is excellent, about 90% at 20 years. In almost 20% of the cases, PTC is multifocal
and metastases are more frequent in the cervical region (lymph nodes) than in distant sites29.
2.1.2.4 Undifferentiated (anaplastic) Carcinoma The anaplastic carcinoma is a highly malignant tumor totally or partly undifferentiated, even though
with some epithelial differentiation. This carcinoma affects, principally, the older people being
caractherized by a fast growth of thyroid masses and a high level of invasion due to an increased
mitotic activity29.
Among all thyroid tumors, the anaplastic tumor is the one with the worse prognosis, presenting a high
mortality rate. Unfortunately, the therapeutic approaches available (surgery, radiotherapy and
chemotherapy) remain insufficient29.
2.1.2.5 MTC The MTC has origin in the parafollicular cells representing 5 to 10% of all thyroid cancers. The
neuroendocrine function of C cells is responsible for the production of peptide hormone calcitonin

32
(CT). The diagnosis and treatment follow-up can be accessed by measurement of CT levels. The MTC
arises from genetic modifications and can be divided into two subtypes: sporadic MTC (70%) and
familial MTC (FMTC). In MTC carcinomas, cancer cells do not have the ability of store iodine, so the
iodine uptake is absent3.
The FMTC, as referred previously, in association with other endocrine tumors yields the multiple
endocrine neoplasia type 2 (MEN2). This type of neoplasia has two subtypes: MEN2a
(pheochromocytomas) and MEN2b (pheochromocytomas and neuromas) 3.In terms of prognosis, the
most favourable is the MTC early diagnosed and treated with lower values of cervical lymph node
metastasis incidence, with approximately 100% of cure rate. An early detection of MTC carcinomas,
thus familial as sporadic form, allow a surgery intervention with high rate of success29.
2.1.2.6 Non-epithelial Tumors – Malignant Lymphoma The malignant thyroid lymphoma can appear as part of a systemic lymphoma or from primary non-
epithelial neoplasm. The majority of primary thyroid lymphomas arise from previous lymphocytic
thyroiditis with an estimated risk 40 to 80 times greater in comparison with residual population3.
2.1.3 Causes of Thyroid Cancer
The exact cause of thyroid cancer remains unknown, although can be associated with inherited
conditions. One of them is the DNA mutations. These changes can modify the normal functioning of
specific genes, such as, the oncogenes. The oncogenes are responsible for cell growth and division.
In cancer, the oncogenes are changed, promoting the cancer cells division and growth3.
In the other hand, cancer can promote alterations in tumor suppressor genes. The mutations in DNA
sequence can turn on oncogenes or turn off tumor suppressor genes.3The mutations in DNA
sequence can affect different genes. In the different thyroid cancers, there are specific genes that are
changed and develop a specific thyroid cancer. In PTC, can occur changes in the RET gene (PTC
oncogene), BRAF gene is mutated (cancers tend to grow and spread to other sites more quickly), and
alterations in NTRK1 and MET genes3. In the FTC, there are modifications in RAS oncogene. In the
anaplastic thyroid cancer, there are alterations in TP53 tumor suppressor gene and in CTNNB1
oncogene. And finally, in MTC there is a change in the RET gene3.

33
2.2 125I - Radioiodide Uptake Assay The radioiodide uptake assays are one of the therapeutic methods applied to thyroid cancer (see
chapter 1). The iodine isotope standard in radioimunoassays is the 125I.
2.2.1 Iodine-125
The 125I have a physical half-life of 60.1 days (λ125I = 0.0115 s-1) which is too long to do diagnostic
imaging but sufficient to do bioassays and therapy. 125I have gamma emission with maximum energy
of ~35 KeV (~0.035 MeV) and beta emission with energies between 4 KeV to 31 KeV. The specific
activity of 125I is 6.45x104 Bq/g (or 1.74x104 Ci/g)11,75.
In radiological terms, the 125I as others iodine isotopes will be fixed principally in thyroid gland where
NIS is present. The 125I can enter into the body by many ways as ingestion, inhalation or puncture
(endovenous administration) between others. The effective dose for ingestion is 1.04x101 mSv/MBq
and for inhalation is 6.53 mSv/MBq11,58,75.
In terms of radiation protection, even 125I have low gamma and beta energies, it is a volatile element
that must be handled carefully and applying security measures. The half value layer (HVL) for 125I is
less than 0.1 cm for lead and for steel11,58.
It is recommended the use of survey meters to monitories the 125I activity. The use of a Geiger-Muller
(GM) or a thin window probe is not sufficient to detect 125I because their typical efficiency is less than
1%. To detect 125I gamma rays must be used a survey meter with a thin crystal NaI scintillation probe
(typical efficiency 29-33%) or survey meters with higher efficiencies (±70%) as gamma counters or
liquid scintillation counters (LSC)11,58.
The use of physical protection (shielding) is only recommended when performed thyroid bioassays
with 125I activities of mCi or great. The bioassay must be done between 6 hours and three working
days, preferentially in the first 72 hours11,58.
This type of bioassays with the handling of radioactive mater needs security precautions as11:
1.Frequent hands monitorization and changing of gloves;
2.Use of whole body and ring dosimeters;
3.Use of remote handling tools;
4.Monitorization of self, work areas and floors after use unsealed 125I by a survey meter;
5.The work with unbound 125I must be done in a fume hood or in a well-ventilated area due to
volatile properties of 125I;
6.The solutions containing 125I must be kept at pH 7.0 and can not be frozen;

34
2.2.2 Genotype
The therapeutic and diagnostic methods applied for PTC and FTC cancers are based on surgery
followed by 131I ablation of remnant tumors and/or distant metastases. The radioiodine therapy is only
possible if thyroid cells express NIS. NIS is responsible for the introduction of iodine into the cell –
iodine uptake. NIS is a glycoprotein localized in thyroid follicular cell’s membrane functioning as a
channel that permits cells to incorporate iodine as iodide from the blood stream by the transport of two
sodium cations for each iodine anion that entries into the follicular cells. It is a transport that consumes
energy because occurred against normal cellular diffusion18,34.
Some thyroid carcinomas lost their capability to incorporate iodine and became resistant to therapy.
The problems related with this incapability to incorporate iodine are directly correlated with NIS. There
are three possibilities: no production of NIS by the cell nuclei, NIS is produced, but can not arrive to
cellular membrane remaining in the cytoplasm or NIS is present in the membrane but there are not
activated18.
Frequently, these carcinomas present mutagenesis of several genes that contribute, among others, to
alterations in NIS expression, one of these is BRAFV600E. Transcript or growth factors, proteins and
others biological components can be involved in this NIS impairment, such as TGFβ (transforming
growth factor beta) or mTOR (mammalian or mechanistic target of rapamycin)10,24,51.
In the PTC carcinomas, the most frequent genetic modification with the hallmarks of a conventional
oncogene is the mutation of gene BRAFV600E. In the presence of this mutation, there is a constant
stimulation of the mitogen activated protein kinase (MAPK), independently of the external stimulation
and the decrease in expression of NIS in comparison with other cases where the mutation is absent.
The MAPK is directly involved in cellular responses and, also, in regulation of cellular proliferation,
gene expression, mitosis, apoptosis, among others cellular processes. Without the presence of NIS,
the cells can not incorporate iodide which can lead to a radioiodide refractory metastatic disease. The
restoration of NIS can be partially provided by the MAPK inhibitors. Also, This process was tested in
some studies with thyroid tumor cell lines and xenographs, but still with controversial results. The
MAKP inhibitors effect on NIS re-expression, increases when mTOR inhibitors are present in the
treatment10.
The oncogene BRAFV600E induces the secretion of TGFβ. This factor controls cellular proliferation,
induces apoptosis and suppresses thyroglobulin and NIS expression. A high activity of TGFβ is
associated with nodal metastasis, invasion and BRAF status. The overexpression of TGFβ occurs
preferentially in the invasive front and NIS is expressed in tumor central regions. In tumors where this
oncogene is present, they have a more aggressive behaviour and less differentiation. Because that,
they do not respond to radioiodide treatment10.
The mTOR is a protein kinase that controls cell growth, proliferation and survival. Its catalytic domain
is almost identical to found in phosphatidylinositol (PI) 3-kinase (PI3K) lipid kinases family. The
inhibition of PI3K increases functional NIS expression in some cell lines as FRTL-5 rat thyroid cell line

35
and PTC lineages. On the other hand, the stimulation of PI3K leads to a decrease in mTOR activation
in several cell lines. This inhibition increases iodide uptake in thyroid cell lines as PCCL3 with thyroid
stimulating hormone (TSH) stimulated68.
The mTOR inhibition permits to counterbalance these two effects. So, in cells treated with TSH and
without insulin, the principal responsible for the increase in iodide uptake is mTOR. This happens due
to in the absence of insulin, the levels of NIS protein unchanged. However, NIS protein has a half-life
that declines from 5 to 3 days, changing protein levels in the plasma membrane. This suggests that
NIS protein translocates from the plasma membrane to intracellular compartments68.
2.2.3 Types of Cells – Cell Lines
To predict the behaviour of NIS and consequently the 125I uptake it is necessary to have thyroid cells
to mimic the intra-corporeal environment and the behaviour of differentiated thyroid cancers. There are
several thyroid cell lineages with different characteristics and specific properties according to the goal
of the investigation.
In this sense, some of the thyroid cell lines used in radioiodine uptake experiments are: PCCL3, C643,
Hth7, Hth74, SW1736, KAT18, OCUT-1, BCPAP, K1, WRO, FTC133, TPC1, FTC-133 and FTRL-
510,15,18,24,49,50,51.
In some experiments, cells were treated with several inhibitors15,24:
- MAPK kinase (MEK) inhibitor: RDEA119
- mTOR inhibitor: Temsirolimus (CCI779)
- Akt inhibitor: Perifosine
- HDAC inhibitor: SAHA (Suberanilohydroxamic Acid)
Additionally, to evaluate the radioiodide uptake in the presence of thyroid hormone was added to the
cells 20 mU/ml of bovine TSH in some experiments15,24.
In our experiment, were used three thyroid cell lines provided by IPATIMUP: K1, XTC-1 and PCCL3.
In literature, the PCCL3 cell line is, between these three types, the one that expresses a larger
quantity of NIS mRNA. K1 and XTC-1 are cell lines that express few quantities of NIS mRNA, and due
to this fact, is expectable that 125I uptake should be greater in PCCL3.
The cell incapacity to incorporate iodine could be associated to several reasons as: lower expression
of NIS mRNA in cytoplasm, NIS impossibility to arrive to the cellular membrane or NIS can arrive to
cellular membrane but it is not functional.
There were made two experimental assays to evaluate the 125I uptake from K1, XTC-1 and PCCL3
thyroid cell lines. In the first assay were used K1 and XTC-1 cells, and in the second assay the three
cell lines were applied. In both assays a NIS blocker were used – Potassium Perchlorate (KClO4).

36
The utilization of a blocker is useful to calculate the NIS specific uptake because KClO4 has
competitive interference with iodide in the entry into the cell trough NIS. The KClO4 is added to some
cells functioning as a negative control.
2.3 AMS
The AMS technique is one of the mass spectrometric techniques with higher sensitivity of detection of
isotopic ratios in samples with low amount of radioactive isotope. The 129I in the only iodine isotope
available for AMS, due to their long half-life (15.7 million of years). The applicability of AMS in
biomedical research is not a new approach, instead its use for thyroid cancer is limited to one study
performed by Negri et al, in 2012, in Argentina. They used bovine thyroids and measured the amount
of 129I present in thyroids. AMS was never been applied to human thyroid cells.
Before speaking about the AMS standards and samples preparation it is important to understand the
AMS technique and its specificities.
2.3.1 History – Biomedical
The history of mass spectrometry can only be explained after the discovery of the electron (cathode
rays) in 1897 by Sir J.J. Thomson at the University of Cambridge. After this, Thomson was inspired by
the work done by Wiens in cathode and positive rays using powerful electromagnets, where he did
experiments with positive rays directing them to an oscilloscope-like screen.
The positive rays deflections induced by the magnetic and electric fields were recorded, initially using
fluorescent material and later photographic films. Therefore, Thomson invented the first scanning
mass spectrometer for determination of mass-to-charge ratios4,20,52.
In 1938, Alvarez and Cornog performed the first mass spectrometry using accelerated ions. In their
experiment, they used 3H ions produced by bombardment of deuterium (2H) to deuterons at a 37-inch
cyclotron2.
Almost only 30 years later, in the seventies and eighties decades, the mass-spectrometric method
was used for direct detection of 14C and other long-lived isotopes in low-energy nuclear physics
laboratories. Only at this time, was proposed to use AMS for biomedical research applying 14C and 26Al (in neurological studies). Active work starts only in late 1988, at Lawrence Livermore National
Laboratory (LLNL) with the operations of bio-analytical tracing using AMS6,13,30 .
In the 1990s, AMS emerged as a useful tool for bio-analysis of quantification of 14C and other long-
lived isotopes in biochemical labeling and tracing studies. In 1990, was realized the first AMS
biomedical analysis by Turteltaub et al. They performed a precise and sensitive quantification of 14C
by AMS for analysis of biological samples contained enriched 14C-labeled carcinogens for toxicology
and cancer studies6,21,30,76.

37
In 1996, was elaborated an important analysis of human breath using AMS in Lund University,
Sweden. Other biological and biomedical studies were realized in this decade, such as, the first
nutrient studies in 1997 (University of California, Davis) and in 2000 (LLNL) about a long-term biologic
tracing of folic acid and β-carotene. Also, in 2002, was made the first AMS analysis in human mass
balance and high performance liquid chromatography (HPLC) metabolite to profile a pharmaceutical.
After this study, AMS became an important and useful tool for pharmacokinetic analysis, as in specific
bonding of labeled compounds and in human radiotracer studies using low levels of 14C6,13,30.
In 2004, Sandhu et al.applied AMS in “microdosing” studies to predict the drug´s behaviour in human
subjects – pharmacokinetic. The high sensitivity of AMS technique allowed the use of very low
concentrations of a specific drug at µg levels6,21.
More recently, AMS was utilized in DNA studies in measurement of damage level in DNA sequences,
in neurological disturbs (dementias) as Alzheimer´s or Parkinson´s diseases, in detection of
biomarkers, in nutritional studies, in forensic science and in biomedical studies applied tolichens and
bovine thyroids6,21,30,43,48,76.
2.3.2 AMS and µAMS
Analysis of long-lived radionuclides extends from radiobiology and health safety, environmental
decontamination and remediation to archaeology and forensics. Due to long-lived radionuclides
relative low specific activity is difficult to implement radiometric techniques based on registration of
emitted radiation. The mass spectrometric methods are the most indicated, although it is necessary to
adjust their characteristics to very low concentration of artificial radionuclides applied in bio-
assays14,33,45.
The conventional radioanalytical techniques as γ-spectrometry or liquid scintillation radiometry are
based on measurement of radionuclides activities. These techniques required a careful chemical
separation of the analyte which is time-consuming and often limited by high backgrounds and low
decay counting efficiency. Moreover, they have well established protocols for radioisotopes with half-
lives lower than 1000 years. These methods are not sensitive enough for the determination of long-
lived radionuclides in biological and environmental samples31,33,45.
Normally, the rare cosmogenic isotopes have half-lives between 103 and 2x107 years22, which is
problematic due to the incompability of the conventional decay counting techniques, as isotope ratio
mass spectrometry (conventional mass spectrometry) or decay production counting to measure or to
detect these isotopes. In the other hand, these isotopes are too short-lived on geological time scales62.
For the measurement of these low-abundant isotopes are desirable to have a technique with a high
isotopic abundance sensitivity, especially when the original matrix has isotopes more abundant than
them. This necessarily leads to the development of high sensitive methods – the Mass Spectrometric
methods9,23,74.

38
AMS: The AMS is a sensitive and selective method with advantageous characteristics for the analysis
of many long-lived isotopes22,54. The AMS technique has the advantage of suppress with a high level
of success all the molecular and isobaric interferences. The interferences can be resolved with a
particle accelerator, as explained later1,8,33.
The AMS and RIMS techniques have the advantage that there are not affected by molecular and
isobaric interferences and, moreover, they are extremely selective techniques in comparison with
other mass spectrometric methods14,23,33.
The limitation of AMS for electronegative elements and the achievement of a high sputtering yield to
form a negative secondary ion beam require a very complex sample preparation (different for each
element) 23,55,68.
In the conventional AMS in order to achieve high sensitivities it is necessary to maximize the current of
the secondary ion beam. The diameter of the primary beam is too large and, as a result, the sample is
completely destroyed, although for biomedical studies the ability to analyse spatially and in depth can
be an advantage5,23,33,68.
Due to the extension of the number of elements that can be measured by AMS, new approaches
emerged from the necessity of enlarging the capacity of elimination of the isobaric interferences.
Actually, the AMS technique can be divided into three segments based on dimensions and terminal
voltage of the Tandem accelerator. Very low-energy Tandems (terminal voltage of 0.5MV) are used
principally for 14C analysis. Low-energy tandems (2-3 MV) can be applied in long-lived radionuclides,
such as, 10Be, 26Al and 129I. The high energy Tandem accelerators (>5 MV) were used initially only for
nuclear physics research. Nowadays, they have been used for analysis of rare radionuclides. The high
energies can provide an effective separation of isobaric interferences using radionuclides such as the 36Cl and the 41Ca5,23,31,55.
SIMS: The first experiments with ion beams were performed using a primary ion beam for
bombardment of target materials. During these experiments were visualized the emission of
secondary ions from the surface of the solid material. The SIMS results from the utilization of these
secondary ions to form a beam5,33,36.
The SIMS technique permits to analyse the concentration distribution of a trace element on the
surface of a material by scanning with a primary beam the sample surface or measuring the three
dimensional distribution of a trace element by eroding the sample surface layer by layer with the
primary beam5,33,36.
Due to this capability to give information about the three dimensional structure of a trace element and
the low detection limit are characteristics that allows the applicability of SIMS in numerous fields of
research and in industry14,33,36.
The major problem is the molecular interferences due to the high mass resolution which cause the
sputtering of some particles from the sample with mass almost identical to the mass of the trace

39
element. Even with a mass spectrometer is difficult to eliminate such interferences due to the high
intensity of the molecular interferences33,36,66 .
To permit this type of measurements and attaching the best characteristics of AMS and SIMS, a new
technique emerged from the junction of these two mass spectrometric techniques - Accelerator SIMS
(ASIMS), Micro-AMS (µAMS) or Microbeam AMS33,36 .
The first experiments of ASIMS were performed in the late seventies s and beginning of eighties at
University of Toronto by measurements of platinum, iridium and osmium in minerals. In the mid-
eighties, was realized the first test measurements of trace elements in semiconductors in University of
Arizona in collaboration with Texas Instruments who had as result the improvement of detection limits
in comparison with the SIMS technique at the time [Ender, 1997a+d] 33,36.
In the late nineties, several facilities are built in the world: In Munich [Massonet, 1998] was added a
new dedicated ion source for Accelerator SIMS to the AMS facility and in Sydney [Sie et al., 1997a+d]
was built a new AMS system with a micro beam source with high lateral resolution for application in
geological research. This was the first microbeam AMS (µAMS) system in the world – AUSTRALIS
(AMS for Ultra Sensitive TRAce eLement and Isotopic Studies) 34,36,58-64.This is the system installed at
LATR/CTN-IST. The familiarization with a complex system as µAMS was crucial to understand its
functioning. Thus, during experimental work at LATR/CTN-IST, I participated in alignment of one line
of the µAMS system. In appendix A is illustrated this part of the µAMS system at LATR/CTN-IST: the
nuclear reations line33.
µAMS: The µAMS system result from the combination between SIMS and AMS systems being
composed of three fundamental components: low energy mass spectrometer (microbeam ion source
and low energy analysing system), Tandem accelerator and high energy mass spectrometer
(analysing magnet, electrostatic analyser and chamber detector). Each component will be explained
later in the 129I analysis36,55-61. The µAMS isotope analysis is made by a selection of multiple stages of
energy, momentum, velocity and atomic charge of the element analysed. At the end, these values
allow the identification of nuclear masses and charges in an ion detector8,33,58-64.
This analysis makes possible the identification of the isotopes of interest as well as the isotopic ratios
by measuring several parameters such as: energy, stopping power, range and velocity. The isotopic
ratios values achieve with µAMS are four to five orders of magnitude smaller than with conventional
mass spectrometry8,33,58-64.
2.2.3 Biomedical Applications
Since the initial development of this technique, AMS has been applied in multiple areas as
archaeology, oceanography, geosciences, biology and life-sciences/ biomedical research that have a
great expansion in the past few years6,11,20,24,26. AMS have the ability to measure small amounts of
rare isotopes, 20 µg to 1mg of radioisotope concentration per sample, and this is one of the reasons to
consider this technique useful for biomedical studies6,21.
The principal long-lived radionuclides measured by AMS are: 10Be, 14C, 26Al, 36Cl, 41Ca and 129I.

40
The isotope most used in AMS is 14C, not only in archaeology, environmental science, but also in
biomedicine29,35. Principally, due to the high sensitivity of the AMS system for detection of radiocarbon
which is the principal isotope for probe analysis. AMS is nowadays the predominant method for 14C-
dating as well as for biomedical applications where 14C is labelled to biological active compounds.29
Moreover, other isotopes have been quantified by AMS such as: 10Be, 14C, 26Al, 36Cl, 41Ca, 56Ni, 99Tc, 129I and 239Pu6,21 .
AMS and RIMS can be used for analysis of 41Ca to assess changes in bone metabolism. After 41Ca
labelled to the bone, using AMS or RIMS it is possible measure changes in urinary 41Ca excretion and
therefore in bone calcium balance. AMS is also, a well-established technique for determination of low-
abundant isotopes of heavy elements. For example, measurement of 240Pu/239Pu in tissue samples of
marine organisms using an ultra-high sensitivity AMS6,21.
The 129I, a long-lived isotope with a half-live of 15.7 million of years33 has been utilized in numerous
AMS applications: environmental tracer (seawater, freshwater, ground water, etc.), biology and
biomedicine (seaweed, lichens and thyroid), geology (loess, soil, coral, rock, and sediments), forensic
tool, nuclear non-proliferation (monitor radioactive discharges and nuclear safety diagnosis –
safeguards) and in nuclear activities (reactor operations, nuclear explosions and fuel reprocessing) 6,12,14,25,27,46,72.
In the past few decades, AMS has been used as monitor agent of sources of contamination, as
environmental as biological, using for this propose 129I. In this case, is made a 129I analysis in lichen,
thyroid and other environmental samples.44 One example is the use of AMS for retrospective
dosimetry of the 131I exposure after Chernobyl accident and the thyroid exposure to 131I was estimated
after the Chernobyl accident based on atomic ratio 129I/131I and in the 129I inventories46.
2.2.4 AMS – 129I
The 129I is a long-lived radionuclide, between iodine isotopes, the 129I is the only one with a long half-
life, 15.7 millions of years, and naturally occur in nature. The only stable isotope of iodine is 127I.
The 129I is produced in nature by the interaction of cosmic rays with xenon in the atmosphere, by
spontaneous fission of 235U and 238U. Also, the 129I can be a product of anthropogenic activities such
as: nuclear energy production, nuclear fuel reprocessing plants and nuclear explosions. These factors
have changed the abundance of 129I in Earth all over the years9,36.
This long-lived isotope naturally produced is mixed with the correspondingstable isotope (127I),
resulting in an equilibrium isotopic ratio. The isotopic ratios of 127I/129I have been changed, with values
of ~10-13 -10-12 before 1950 (after this year the anthropogenic production of 129I increased) to isotopic
ratios in order of 10-11 – 10-9 at the present. The human nuclear activities and some radioactive
accidents as Chernobyl, La Hague and Sellafiled increase the levels of 129I with measured isotopic
ratios 127I/129I between ~10-6-10-4 9,22,28.

41
The 129I have different concentrations in environment in comparison with his concentration in biologic
tissues, who leads to different isotopic ratios in open ocean surface water (1.2x10-10 to 9x10-10),
Northern Sea (5.1x10-7 to 1.5x10-6) and in thyroid glands (4x10-11 to 4x10-7)9,22,28.
Due to this long half-life and low abundance in Earth, nowadays, the measurements of 129I are perform
in most of the cases by AMS12,19. An AMS analysis from samples with 129I can be performed with only
a few milligrams of iodine sample (1-2 mg). For example, an iodine sample with a mass of 1 mg can
produce iodine beam currents of ~20 µA22,27,28.
An 129I AMS analysis started with the preparation of the samples. The sample preparation methods are
dependent of the type of the sample (geological, environmental or biological). According to the type of
the sample, the isotopic ratio 127I/129I and the optimization of the equipment are different. It is
necessary the use of standard samples with isotopic ratios 127I/129I well defined. Normally, these
standards are obtained commercially and posteriorly diluted, or they can be produced in situ19,22,27,50,71.
Depending on their origin, the samples need to be prepared using several methods.. Nevertheless, all
samples are mixed with a conductive element, normally silver (Ag+). The most common chemical
formula used for a 129I-AMS analysis is a precipitate of silver iodide (AgI)19,22,56,71.
The preparation methods of standards and samples are discussedin the following chapter.
2.3.6 Sample and Standards Preparation
The AMS system requires the utilization of reference materials or standards (as they are typically
named) and these are divided in two categories22,55,56,73:
1. Materials with a simple and well known chemical form, and a predetermined isotopic ratio that
permits the calibration and normalization of AMS measurements.
2. Natural origin materials as rocks, sediments, vegetation, biological materials, among others,
with known isotopic ratio and radioisotope activity, at low levels, to test extraction and analysis
procedures.
It is important that these standards be prepared with ratios that allows maintaining the AMS sensitivity
and avoid contaminations, and also, a count rate sufficient to allow 1% of statistical measurements22.
Due to the fact that these requirements are not well established for many radioisotopes, several AMS
facilities have started to produce their own standard material. The materials are prepared locally using
guidelines and with the maximum precautions by conventional radiometric counting, mass
spectrometric methods and/or standard gravimetric dilution to achieve their appropriate isotopic ratios.
Furthermore, some AMS facilities have produced their standards by serial dilutions of primary
standards (acquired from National Institute of Standards and Technology – NIST) or from other
laboratories22,72,73.

42
The performance of an AMS system can be achieved by utilising of background materials or blanks.
Blanks are materials with the same composition of standard materials, but without radioisotope. It is
possible to determine the inherent accelerator background and contamination. The contamination
derived from material processing and chemical preparation can be controlled and decreased by
preparing the blank as a natural sample material. Normally, natural “old” sample materials or high
quality reagent grade chemicals (commercially available) are used as blanks22,72,73 .
2.3.6.1129I Sample and Standard Preparation
For AMS measurements using 129I, the concentrations of 129I present in a sample can be determined
by AMS, AMS/IC (Ion Chromatography) or RNAA (Radiochemical Neutron Activation Analysis) 55,72,73.
AMS is used when the sample has a negligible concentration of stable iodine and the amount of
carrier added to the sample is known. The absolute concentration of 129I is calculated from the 129I/127I
ratio measured by AMS. A combination of AMS with IC (AMS/IC) can also be applied for the
determination of the concentration of 129I by isotopic ratio measurement and the content of stable
isotope (127I) by IC. The RNAA provides directly the concentration of each isotope (129I and 127I) 55,72,73.
AMS sample preparation is based on these methods, and some procedures are common to all
methods, as the determination of water content, which is realized using subsamples to avoid
contaminations or losses of iodine. Also, the determination of the chemical yields of the preparation
methods which is done using 125I as a tracer and detecting his γ energy of 35.5 keV in a Ge-detector72.
Before perform any sample preparation for AMS is necessary to explain some special demands19,73:
- A minimum of 1 mg of AgI is necessary to do an AMS measurement;
- Samples with isotopic ratios higher than 10-9 should not be used in AMS measurements to
avoid cross-contamination from other samples due to the memory effects of the ion source;
- It is necessary to add stable iodine (127I) as a carrier to the sample;
- The 127I carrier is added as iodine solution after reduction with alkaline NaHSO3 solution;
- The content of the carrier is determined by IC;
- AMS measures isotopic ratios, so it is not possible to get information about the absolute
concentration of 129I present in a sample;
- Sample with carrier added, the amount of 129I is obtain by 129I/127I isotopic ratio measure, the
amount of carrier added and the concentration of 127I present in the original sample material;
- Sample without carrier added, AMS gives information about the intrinsic isotopic ratio and with
the information of the concentration of 127I in the original sample, it is possible to know the
amount of 129I;
- In any case, to determine the concentration of intrinsic stable iodine present in the sample
material it is necessary to use an additional method;

43
- Standard addiction method is used for calibration;
2.3.6.2 129I Standard Preparation
In the preparation of standards for 129I-AMS, normally, iodine is prepared as a precipitate of silver
iodide (AgI). Although, iodine can be mixed with silver or niobium (Nb) powders. These are conductive
materials and some authors defend the use of Nb due to its lower 129I background. However,
nowadays, the most used is the AgI or the co-precipitate AgI-AgCl55,56,73,77.
The use of chloride (Cl-) is justified by the fact that potencies precipitation acting as a co-precipitating
agent. Chloride is added during sample preparation to co-precipitate the trace amount of iodine in AgI-
AgCl77.
Even using the co-precipitate AgI-AgCl, it could be useful the utilization of Nb powder. The co-
precipitate AgI-AgCl is a weak conductor material and unstable during heating and bombarding
withthe Cs+ microbeam.
Due to this fact, Nb powder can be added to the co-precipitate AgI-AgCl acting as an electrical
conductive reagent and allowing the stabilization of the target during the ionization step77.
The method of co-precipitation use 0.5 mg of Cl- as NaCl in a 15 mL centrifuge tube. Firstly, the iodine
is added to the tube and mixed with NaCl. After this, the mixed solution is diluted in a volume of 10 mL
of deionized water and 0.5 mL of 1.0 M of AgNO3. Finally, the components are separated by
centrifugation and the co-precipitate of AgI-AgCl is washed with deionized water77.
Iodine needs to be converted into iodide (I-) to be able to connect with silver (Ag+). The reduction is
possible using a sulphite agent as NaHSO3. After this is necessary to adjust pH < 5 and add silver
nitrate (AgNO3). The solution must maintain the acidic character because this is helpful to form
precipitates and avoid the adhesion of the precipitate (after formation) to tube surface77.
For samples with high iodine content as seaweed, thyroid, brine or lignite the method recently used is
the carrier-free method. In this method, the final result is a co-precipitate of AgI with silver chloride
(AgCl) – AgI-AgCl77.
The first step consists in reducing the iodide to iodate by the addiction of sulphuric acid (H2SO4) and
sodium hydrogen sulphite (NaHSO3). Then, the iodide is oxidized to molecular iodine (I2) by addiction
of sodium nitrite (NaNO2), and this I2 is extracted using carbon tetrachloride (CCl4)77.
The reduction of I2 is necessary, so it is performed after extraction and is called back-extraction. The I2
is back extracted by a sodium sulphite solution added to iodine solution.76The extraction and back
extraction processes are repeated until the color of CCl4 disappears which demonstrates the
progressive concentration and purification of iodine. Normally, this step is repeated 5-6 times77.
Next, the concentrate iodine is precipitated in silver iodide (AgI) after mixed with silver nitrate (AgNO3)
and ammonia (NH4) in a dark room. The precipitate is washed with ammonia and distilled water. After

44
dry in an oven, the AgI is mixed with Nb in a proportion of 1:2.5 (AgI:Nb) and pressed in a target
holder77.
2.3.6.2.1 Working Solutions77:
a) Dilution of a standard solution with 127I solution prepared from Woodward Iodine, Cª;
b) Two 129I working solutions – 129I standard solution (Isotopic Ratio < -12) plus NaCl solution (mass
ratios Cl:I of 2:1 and 4:1);
c) Six 129I working solutions – 129I standard solution (Isotopic Ratio < -10) plus NaCl solution (mass
ratios Cl:I of 10:1, 20:1, 40:1, 100:1, 200:1 and 1000:1);
d) Concentration of Cl in working solutions: 1.00 mg/mL;
All the standards solutions were prepared with deionized water (18.2 MΩ) and as the following:
There is used 0.5 mL of working solution in a 15 mL centrifuge tube with a radioactive activity of 200
Bq of 125I to each standard solution. Thereafter, were added 0.1 mL of 0.1 M of NaHSO3, 0.2 mL of 1M
of HNO3 and 10 mL of deionized water. At the end, with the iodine in iodide form, 0.1 mL of 1.0 mol/L
of AgNO3 is added to the solution and the co-precipitate AgI – AgCl is formed77.
The co-precipitate is centrifuged and washed with 3.0 M of HNO3 and deionized water. After this, the
co-precipitate is dried in a 1.5 mL centrifuge tube at a temperature of 60-70ºC, weighted and grounded
to a fine powder. The co-precipitate of AgI-AgCl is mixed with the Nb powder (2 to 5 times) and
pressed in a copper holder specifically for AMS target preparation77.
2.3.6.3 129I Sample Preparation
For AMS sample preparation exist four methods: a) Combustion (Gold-Standard), b) Tracer
Combustion, c) Carrier Combustion and d) Alkaline Leaching38,72,73.
The methods used for AMS sample preparation are based in one method – Combustion method –
applied in RNAA55,72.
a.Combustion Method
The combustion method was first described by Studier et al. (1962) and modified several years later
by Anderson (1978). This method was applied to three different samples (soil (70g), plant (7g) and
thyroid tissue (3g)) 55,72.
Firstly, the sample material is weighted and a specific radioactive concentration of 125I is added,
approximately 5 kBq. After this, the sample material is placed in a quartz tube that is over, another one
larger than him to allow matrix separation. Then the sample is carefully heated in an oxygen and

45
nitrogen flow with a Bunsen burner at least one hour. The temperature must increase slowly from
600ºC to 1000ºC to avoid violent reactions55,72.
The inner quartz tube is placed in a tube furnace held at a temperature of 1100ºC. The sample
remains there for three hours to complete the combustion process. After combustion, the iodine that
evaporates from the sample is absorbed by a charcoal trap55,72.
To separate the iodine from the charcoal trap, the charcoal is placed in a double quartz ampoule and
heated the lower part at a temperature of 1100ºC.This warmth causes iodine distillation in the upper
part of the double ampoule which is, simultaneously cooled with liquid nitrogen. After two hours the
upper part of the double ampoule is sealed and prepared to be irradiated. During two hours the
ampoule is irradiated together with the appropriate standard material55,72.
After irradiation, is performed the post-irradiation chemistry of samples and standards in order to purify
the iodine and separate it from other radioactive substances, in particular from bromine isotopes.
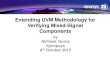
Finally, iodine is precipitated as AgI and measured by γ-spectrometry. The procedure is illustrated in
Figure 2.255:
Figure 2.2: Combustion Process55
a1. Combustion Process by Marchetti et al. 199738

46
The iodine separation is made by a combustion process. This specific process was developed by
Studier et al in 196738.
Marchetti utilized a quartz tube with tapered joints, and put quartz wool in one extremity of the quartz
tube. The tube was placed in a tube furnace with an auxiliary furnace at 1100°C. The tube end with
quartz wool was positioned in contact with the auxiliary furnace (downstream) and with a gas wash
bottle and the other extremity was connected to an oxygen cylinder. All the stock solutions were
prepared with double distilled water38.
The gas wash bottle was filled with 75 mL of 0.1 M of KOH (Potassium Hydroxide) and Na2SO3
(Sodium Sulphite). To this solution was added 1.5 g of bovine thyroid sample and 0.5 g of soil sample.
The auxiliary furnace was heated at 1000°C38.
The samples were weighed in porcelain and combustion boats with sample sizes between 0.5 to 1 g
for soil and 0.1063 g for thyroid sample38.
The combustion process began by placing the boat at the center of the tube furnace and opens the
oxygen bottle with a flux of 80 mL/min. Next, the temperature of the main furnace was increased to
1000°C38.
For soil samples, the temperature of the main furnace takes 20 minutes to reach the 1000°C. In the
case of the thyroid samples, the temperature was gradually raised, beginning at 180ºC, increasing the
value at 300ºC with a rate of 3ºC/min and, finally, to 1000ºC at a rate of 30ºC/min. Were prepared
aliquots of KI and KIO3 solutions containing 2.0 µg of iodine and were evaporated on, approximately, 1
g of sand or silica (SiO2). The process is the same as for soil samples38.
After the main furnace temperature arrived to 1000ºC, this was left here for 90 minutes. Experiments
made by Marchetti, demonstrates that using soils and KI solutions, after 60 minutes the amount of
iodine did not change significantly38.
Once the combustion process finished, the trapping solution was transferred to a volumetric flask with
a total volume of 100 mL, also, was added water to adjust the final volume and the solution was
homogenized38.
At the end, the quartz tubes of both samples were cleaned by heating them at 1000ºC with oxygen
flow during one hour38.
The combustion process is the principal step of this preparation. One of the main precautions is
assure that enough sodium sulphite is added to the trapping solution allowing the reduction of all
iodine species to iodide. Unless, a large excess is not desirable because this sulphite needs to be
oxidized for the iodination of the 3-pentanone. To verify this, at the end of the combustion process,
some samples were tested, reacting 1 mL of the trapping solution with 1-2 drops of a solution of
KMnO4 (0.1M). Similarly, the excess of water in the aqueous phase was tested by adding a solution of
K2Cr2O7 (0.5%) after extraction of iodine derivative38.
a1.1 Preparation of Iodine Derivative:

47
In a separation funnel (125 mL) was placed an aliquot of the previous solution (25 mL) for soils. For
thyroid samples were used several aliquots (2, 3 and 5 mL) that were diluted in the same volume
each. Then joins 1 mL of 3-pentanone (4% v/v), 1 mL of H2SO4 (5M) and 1 mL of H2O2 (30%). After
homogenization, the solution is left during 10 minutes to allow the iodination. Then, the 2-iodine-3-
pentanone was extracted in hexane (10 mL) by shaking the mixture vigorously for 2 minutes38.
a1.2 Measurement of Total Iodine:
The measurement of the iodine derivative was made by gas chromatography using helium (He) as
carrier and by 63Ni electron-capture detector with argon (Ar) as make-up gas doped with CH4 (5%).
The temperature of the injector was 150ºC and for the detector was 300ºC. The injection cycle profile
was 1 minute at 50ºC, ramp at 10ºC/min to 150ºC and 1 minute at 150ºC. Three injections per extract
were realized38.
In the case of soil samples, the area of each sample was determined by the average of the 6
corresponding areas of the extracts of two 25 mL aliquots. For thyroid samples, the area was
calculated from the average of 6 injections and each aliquot were treated individually38.
The standards were prepared from a dilution of a stock solution with a concentration of 1000 µg/mL of
iodine as KI. Were collected amounts of iodine with masses between 0.1 and 10 µg and put in a
volume of 25 mL with water and processed as performed for sample aliquots38.
The detection limit estimated was 0.02 µg of iodine in a 25 mL aliquot38.
a1.3 Sample Preparation:
For the sample preparation, was used a 200 mL beaker where was placed an aliquot of the trapping
solution and diluted with water making 100 mL in total. To precipitate iodine in silver iodide (AgI) was
added 5 mL of KI solution (1000 µg/mL iodine), 1 mL of concentrate HNO3 and 1 mL of AgNO3 (5%
m/v)38.
The beaker was covered with a watch glass and left in a dark place overnight allowing the formation of
the coagulate. Then, the supernatant was removed and the precipitate transferred to a borosilicate
test tube (10x75 mm) by a polyethylene transfer pipette. The remaining supernatant was cleared by
centrifugation38.
The precipitate was washed three times by resuspension in water, centrifuged and dried in an oven at
70ºC. After this, was mixed with the similar volume of Ag powder and loaded into a target holder for
AMS measurements. For soils, was used 50 mL aliquot and for thyroid samples 1 mL aliquot38.
b.Tracer Combustion Method

48
In the tracer combustion method is firstly prepared a solution containing a tracer. After determination
of the amount of 127I in the sample by IC, the same solution is used to prepare the 129I precipitate.55,73
The tracer solution is prepared by weighing the sample material and adding approximately 5 kBq of 125I (tracer). After combustion of the sample, the iodine evaporates and is absorbed as iodide in an
aqueous alkaline solution with a molar concentration of 0.3 mol/L of NaHSO355,73 .
The chemical yield of the combustion process is determined by measurement of the amount of 125I
present after combustion. The concentration of 127I present in the sample can be calculated after IC
analysis of an aliquot of the absorbing solution55,73.
The precipitation of iodide is performed by using the remaining solution and adding 3 mg of iodide
carrier. After this, the solution is mashed and added 6 mL of a solution of saturated barium nitrate
(Ba(NO3)2) that leaves to the precipitation of sulphate ions (SO32-and SO4
2-)54,72 . Then the solution is
centrifuged and the precipitate is separated from the supernatant. The supernatant solution is acidified
by addition of 0.5 mL of concentrate nitric acid (HNO3). Lastly, is added 5 mL of a solution of 0.1 mol/L
of silver nitrate (AgNO3) which leads to the precipitation of iodide in silver iodide (AgI)55,73.
c.Carrier Combustion Method
The carrier combustion method is useful in samples with very low concentration of iodine (better
handling and better yields) and, is more used in laboratories which cannot work with radioisotopes.
The procedure is similar to the described before with the difference of use 127I as carrier (3 mg) and
not any iodine isotope55,56,73.
d.Alkaline Leaching Method (only used in soils until now)
The alkaline leaching method is used, until now, only in soil samples. In this procedure are utilized 6g
of sodium hydrogen nitrate (NaHNO3) and 10 mg of carrier. The carrier is prepared from Woodward
iodine in a solution with 1 mL of water (H2O) and 0.3 mg of iodide carrier. The iodide carrier is a
product from sodium iodide (NaI) in 200 µL of H2O and 2 g of sample material (soil) that was prepared
in a nickel crucible. If is used another sample material, as plants or tissue, the amount must be less
than the used for soil samples55,73.
The crucible is covered and the alkaline leaching is performed with the addiction of NaHNO3 to the
previous solution. The temperature varies with the time: 1 hour – 150ºC; 2 hours – 200ºC and 3 hours
– 250ºC55,73.
After this time, the melt is extracted by addition of water and the solution is centrifuged. To perform the
reduction of all iodine species to iodide is added to the supernatant 0.1 mol/L of NaSO3 and 6.0 mol/L
of H2SO4. The solution is centrifuged one more time55,73.

49
After centrifugation, is added to the solution sodium nitrite (NaNO2) and the iodine formed is extracted
into chloroform to a separation funnel55,73.
In this separation funnel, the iodine is reduced by addiction of 0.1 M of NaHSO3 and 0.1 M of H2SO4
and the iodide formed is back-extracted into water. These purification methods of extraction and back-
extraction are performed more two times55,73.
To avoid the formation of silver sulphite (Ag2SO3) is essential to evaporate the sulphur dioxide (SO2).
The precipitation of iodide in silver iodide (AgI) is materialized with addiction of silver nitrate (AgNO3)
solution55,56,73.
2.3.6.4 129I-AMS Target Preparation
The target preparation is the final step before AMS analysis. For this isotope, the sample preparation
requires the next global steps: a) reduce the sample (previous prepared) to a fine powder, normally 2-
3 times the mass of the conductive material, b) the sample powder is mixed with the conductive
material (Ag or Nb), also as powder, c) this mixture is pressed in a copper holder specific for AMS
measurements19,27.
2.3.6.5 129I AMS Sample Preparation – Biological Sample (Thyroid)
Most of the AMS laboratories installed around the world that uses the 129I as a radionuclide, apply their
investigations to analysis of environmental and geological samples to determine the amount of 129I
present, measuring the 127I/129I isotopic ratio by AMS. For the conventional biomedical research the
utilization of 129I was discharged at the beginning due to this long half-life of ~ 15.7 millions of years.
The application of AMS to biomedical sciences is relatively recent with focus in 14C-AMS analysis21,30.
The analysis by AMS of biological samples using 129I still remains under scientific investigation due to
several factors. The main challenge concerns into production of AMS standards and samples with 129I.
According to the literature, this is the more challenging and motivating work area. As an example, was
applied 129I-AMS in biological samples as lichens and animal thyroids but never in human cells or
tissues27,43,44 .
Recently in 2012, in Buenos Aires (Argentina), a group of scientists studied the 129I content in animal
thyroids. They use thyroid samples from grazing animals (bovine animals) and prepare them to
determine the 127I/129I isotopic ratio using an AMS system43,44.
This was the first and unique (at the moment) investigation using thyroid samples from animals to
perform an AMS analysis43,44 .
The analysis of biological samples, such thyroids, by AMS is a complex procedure that implies several
steps. The crucial step is the sample preparation. A biological sample preparation is difficult because
in the other cases, for example, when was used geological samples, the mixture with conductive
element, normally a metal, that permits the sputtering of the sample is easy. The sample can be

50
reduced to a powder and mixture with a metal and easily pressed in a holder to give the property
shape for AMS analysis. Using biological samples it is different, due to the fact of exit a cope with life
beings where the most important is to maintain the conditions and do not change the biological
properties43,44.
One of the goals of our investigation is the preparation of biological samples for AMS from human
thyroid cells. This preparation was based on the protocol performed by Negri et al. in 2012. The
Argentine´s group made their investigation, collecting fresh thyroids from grazing animals (cattle) from
different areas of Argentina. The samples preparation was realized in TANDAR laboratory in Buenos
Aires and AMS measurement of 127I/129I isotopic ratio in Vienna Environmental Research Accelerator
(VERA). The 127I/129I isotopic ratio was obtained by AMS and the 127I content was determined by Gas
Chromatography (GC). The thyroids were selected from bovine animals with the same feed
conditions39,43,44.
The quantity of iodine present in a thyroid gland decrease over the time, whereby, is important to
collect the thyroid glands until, approximately, 100 days, which is the iodine biological half-life for
thyroid gland43,44.
The first step is to get the biological samples. Fresh thyroids collected for each cattle type (bovine
type) were weighted, frozen, and then, lyophilised, homogenised and chemically processed42,43.
The measurement of 129I content using the AMS technique implies the iodine extraction from samples,
in this case, from thyroid samples.
The method developed by Negri et al.41,42 was based on experiments realized at LLNL by Marchetti et
al. (1997)37, and adapted these to create a new protocol specific for AMS measurements using bovine
thyroid samples with low 129I concentration43,44.
2.3.6.5.1 Methodology
From thyroid samples previously prepared, are weighted 100 mg of dry-freezed thyroid. This is the
amount of thyroid that constitutes the biological sample for measurement. Next, the sample is oxidized
by adding a solution of peroxydisulfate43,44.
The derivatives for GC and AMS analysis are prepared in a separation funnel with a volume of 100
mL. In this funnel has prepared a solution that contains 200 µL of the previous solution (oxidized dry-
freezed thyroid sample), 25 mL of water, 1 mL of Pentan-3-one 4% (C5H10O), 1 mL of hydrogen
peroxide (H2O2) and 2 mL of sulphuric acid 5M (H2SO4). The derivatives are extracted with hexane
(CH3(CH2)4CH3)43,44.
As reference value, the recovery of iodine extraction method for GC is 75-80% using a standard from
NIST, the NIST-SRM-1459, a non-fat milk powder with a value of 3.38±0.02 µg/g43,44.
The determination of the amount of 129I is made to measure the 127I/129I isotopic ratio by AMS and then
subtracting the amount of 127I obtained by GC. To measure the 127I/129I isotopic ratio is necessary to
prepare a target available to be introduced in an AMS system43,44
The target is prepared in another separation funnel with a total volume of 250 mL. The first step, add
1.0g of sodium sulphite (Na2SO3) to the solution of oxidized dry-freezed thyroids to reduce the iodate

51
to iodide, this step is present only in the article of 2012. Then, 2 mL of potassium iodide (KI) with a
concentration of 1000 µg/mL in Merck Suprapur® solution is added as carrier. The pH is adjusted to 1
with addiction of acid nitric (HNO3) concentrate, and finally, 400 µL of silver nitrate (AgNO3) in a mass
concentration of 5% m/V to precipitate the solution in silver iodide (AgI). The precipitate is washed and
left in an oven drying overnight. After this time, is added silver (Ag+) to the precipitate and pressed in a
sample holder specific for AMS targets43,44.

52

53
Chapter 3
Experimental
3.1 125I Uptake Assay
3.1.1 Method of Preparation
The experimental setup was developed at CTN/IST – UCQR in laboratories specifics for biological
assays.
The 125I uptake assay was performed with three types of thyroid cells: K1, XTC-1 and PCCL3. In the
first assay were used K1 and XTC-1 cells, and in the second assay were applied the three types of
thyroid cells.
The iodide uptake only is possible if the cell has the capability to incorporate iodide and if NIS is
present and functional in the cellular membrane. NIS is a glycoprotein that needs two Na+ and one I- to
have a normal functioning. The quantity of Na+ needs to be higher than the quantity of I-.
In the iodide uptake assay was used a radioactive solution of Na125I and in order to achieve the Na+
needed for a normal NIS performance, a cold solution of NaI was added. Although, the amount of cold
NaI should be the sufficient to allow the functioning of NIS and does not interfere with radioactive
iodine (Na125I).
In the first assay was used only one concentration of cold NaI. In the second assay were applied two
different concentrations of cold NaI to access which is the best concentration to be given to the cells.
This difference between the two assays is justified, in literature, where there wasreported higher and
lower values of concentrations of cold NaI. This variability require test and assess which is the optimal
quantity of cold NaI for a specific radioactive activity of Na125I.
An 125I uptake assay include the determination of two parameters: the radioactive activity present in
thyroid cells by the measurement of emitted gamma rays in a gamma-counter, but also, the
quantification of the protein levels present in cells.
The assessment of the protein concentration in each well is important to normalize results. This
normalization, allow us to assure that differences between 125I uptake values are related to a variable
NIS function and not to a majorquantity of cells present in each well.
The protein quantification is based in Bradford method48. The protein levels present in cell were
achieved by a linear regression obtained from NaOH standards. All the process is described in
specific elsewhere 49.

54
3.1.1.1 Materials
A dose calibrator is a gas-filled ionization chamber which is used to calculate the radioactive activity
present in a radioisotope sample.
- Ionization Chamber for Dose Calibration
Figure 3.1: Ionization Chamber for Dose Calibration85
This chamber is filled with Argon gas and submitted to a voltage measuring the ionization produced by
the sample to be calibrated. This current is proportional to the activity of the measured radioisotope.
Before any measurement it is possible to select the radioisotope to be calibrated. In our case, the
ionization chamber was optimized to 125I a gamma emitter.
- Fume Cupboard
- Multi-Crystal LB 2111 Gamma Counter
Figure 3.2: Multi-Crystal LB 2111 Gamma Counter86

55
The multi crystal LB2111 gamma counter is a compact and easy-to-use instrument for applications
when gamma emitter isotopes are used. The most common are 125I, 57Co, 59Fe, 51Cr and 99Tc. Permits
the measurement of 12 samples at the same time that will be collocated in racks perfectly match with
the boreholes of the NaI detectors crystals that provides the best measuring geometry for γ-emitters,
covering an energy range up to 500 KeV. Each detector is surrounded by a thick lead (~12 mm) that
prevents cross-talk between samples. The counting of gamma rays is represented in cpm (counts per
minute).
- Microplate UV-Vis Spectrophotometer
Figure 3.3: Microplate UV-Vis Spectrophotometer87
The microplate spectrometer is used for direct quantification of nuclei acids using automated path
length correction and low UV measurements required for DNA and RNA quantification.
- Well Plates
- Micro Pipettes
- Beat and Gloves
- Freezer
3.1.1.2 Protocol (General)
1. Remove the cells medium from wells and wash with Hank´s Balanced Salt Solution
HBSS (37ºC);
2. Add 990 µL of HBSS only to the positive control wells and 990 µL HBSS plus KClO4
(100 µM) to negative control wells;
3. Add 10 µL of Na125I (approx. 15000 cpm) to each well;
4. Incubate for 45 minutes at 37ºC;
5. During this time, prepare sodium hydroxide (NaOH) solution and dial the tubes;
6. Remove cell buffer and wash with 500 µL of ice-cold HBSS;
7. Cells lyse with 500 µL of NaOH (0.5 M);
8. Scrape off and counting each tube in a gamma-counter;

56
3.1.1.3 Experimental Setup
First Experimental Assay
In the first experiment were used two types of thyroid cells, K1 and XTC-1, as was explained
previously. According to the literature, the quantity of mRNA NIS in XTC-1 cells is higher than in K1
cells [Tavares C. et al, unpublished]. Although, the total iodide uptake values expected from K1 and
XTC-1 thyroid cells are small. The counts between thyroid cells without NIS blocker and with NIS
blocker are similar.
The thyroid cells K1 and XTC-1 were prepared for the experiment In a laminar flow hood, the thyroid
cell lines were plated in 24-well plates (12x2) for 36 hours. The cells were cultured in plates with 12
wells. The 12 wells were divided in two, and added the two solutions (A and B) to half of the wells,
representing the positive and negative controls, respectively.
The activity of the radionuclide 125I in the experiment day was measured by a dose calibrator. A pre
selection of radionuclide was made and a radioactive concentration of 215 µCi/mL of Na125I was
measured. After, three stocks were prepared: A, B and C using cold NaI, Na125I radioactive solution,
NIS blocker KClO4 and HBSS. From solution C were prepared another two solutions to give to the
cells: solution A (positive control) and solution B (negative control).
Stocks Solutions Preparation
The stocks solutions were prepared based on dilution equation, Ci x Vi = Cf x Vf, where “C” is the
concentration or molar concentration (in m/L), the “V” is the solution volume, the “i” and the “f”
represents initial and final, respectively.
Preparation of stocks A, B and C:
Figure 3.4: Stocks A, B and C (preparation and concentrations)
Stock A
• 215 µCi/mL Na125I in [] 100 µM NaI + HBSS
Dilution
• 100 x Dilution (1 mM of NaI + HBSS)
Stock
B
• 1 µL Na125I + 1 mL NaI (1mM) +HBSS
Stock C
• 0.1 µCi/mL Na125I ([] 1 mM NaI + HBSS)

57
Preparation of solutions A and B:
Figure 3.5: Preparation of solutions A and B
The preparation of stock C and solution A were conducted on a trial-and-error basis by adding a drop
from Na125I solution in order to achieve 70.000 cpm. In the reference procedure performed by Souza
et al, a volume of 5 µL from stock C should have a value of 70.000 cpm. A volume of 5 µL was
collected from stock C and analysed in the gamma-counter with approximately 70.000 cpm.
The final concentrations were: 0.1 µCi/ml of Na125I; 1mM of NaI and 10 µM of KClO4.
The protein quantification was accessed by plating a twin well plate of K1 and XTC-1 cell by the
Badford method described in detail elsewhere48 The cells suspensions, have been transferred to
eppendorfs, and then stored for a sufficient period of time until will be safe to handle (≈ 590 days).
Second Experimental Assay
In the second assay were used the three types of thyroid cells: K1, XTC-1 and PCCL3. The K1 and
XTC-1 cells were compared with the first experiment. Among the three, PCCL3 are according to the
literature the most specific thyroid cell type and with a higher iodide uptake. In this experiment, beside
the iodide uptake assay and protein quantification, was applied to K1 cells a gene silencing. Little RNA
chains were added to K1 cells, and then were made a gene silencing to predict if without gene
expression the levels of protein were modified or not.
Proceedings were realized in a laminar flow hood:
- Remove cells medium excess
- Place cells in hothouse
Stock C
SoluGon A (PosiGve Control)
10 µL Stock C + 990 µL HBSS (100.000 - 150.000
cpm)
SoluGon B (NegaGve Control)
10 µLStock C + 990 µL HBSS
plus 10 µM KClO4

58
- Plating cells:
• K1 cells: 12 wells (6x2)
• XTC-1 cells: 8 wells (4x2)
• PCCL3 cells: 18 wells (9x2)
In PCCL3 cells were used two different concentration of cold NaI (1 mM and 100 µM). The K1 cells
were plated for 48 hours, and XTC-1 and PCCL3 were plated for 36 hours.
- After plating, each type of thyroid cell was counted in an optic microscope using a Neubauer
chamber or Hemacytometer.
- Preparation of NaI and KClO4 solutions:
Figure 3.6: Preparation of NaI and KClO4 solutions
In total there are 66 wells for counting (22 wells in triplicate: medium, washing liquid and cells lysate).
The radioactive concentration of Na125I was measured in a dose calibrator, pre-selected for 125I with
the value of 351 µCi/mL.
2 Solutions
NaI
Weight: 0.75 g Volume: 5 mL
Final Concentration:
1 M
1 mM 100 µM
KClO4
50 mL HBSS Final
Concentration 100 µM

59
Stocks Solutions Preparation
Stock A:
Figure 3.7: Preparation of stock A; *D.C: Dose Calibrator
Several factors can modify the radioactive concentration measured in the dose calibrator. One of them
is the intrinsic geometric effect associated to the dose calibrator. At first, the volume calculated was
28.5 ml, but due to vial geometric effect was necessary to add 30 µL to have the final concentration of
10 µCi/mL.
Figure 3.8: Preparation of stocks B1 and B2
NaI Stock
• Concentrated Stock NaI: 351 µCi/mL
Dilu:on • 30 x Stock Dilution V=28.5 mL
D.C* • Mesurement of radioactive concentration: 6 µCi/mL
Trial and Error
• Add 30 µL = 58.5 µL Total Volume
D.C. • 2º Mesurement: 10 µCi/mL
Stock A • C= 10 µCi/mL; V= 58.5 µL
Stock B
10 µL Stock A 1 mL 1mM NaI HBSS plus 100 µM KClO4
Stock B1
10 µL Stock A 1 mL 100 µM NaI
HBSS plus 100 µM KClO4
Stock B2

60
Figure 3.9: Preparation of stocks C1 and C2
- The stocks B1 – C1 and B2 – C2 were the solutions of use;
- There were collected 10 µL from stock C1 and C2, and measured in gamma-counter. For
stock C1 were measured 159.000 cpm and for stock C2 160.000 cpm;
A solution of NaOH used for cellular lyse was prepared from a standard solution of NaOH with a
concentration of 10 M solution in a total volume of 20 mL (1 mL of NaOH 10M + 19 mL of distilled
water). The final concentration of NaOH solution was 0.5M.
The final concentrations were: 10 µCi/ml of Na125I; 1 mM and 100 µM of NaI, and 100 µM of KClO4.
Only in PCCL3 cells were used two concentrations of NaI (1mM and 100µM). For K1 and XTC-1 cells
the NaI concentration used was the same of the first assay.
- The cells were incubated at 37ºC during 45 minutes to rest;
- After this time, the wells medium was removed and the cells were washed with 500 µL of ice-
cold HBSS;
- The cells were lysed with 500 µL NaOH (0.5M) during 15 minutes, scraped and transferred to
vials for measure in gamma-counter and for protein quantification;
Such as in the first assay, the protein levels were accessed by plating a twin well plate of K1, XTC-1
and PCCL3 cells by the Badford method48. At the end of the experimental assay, the cells
suspensions, were transferred to eppendorfs, identified, placed for storage and held for decay (at least
ten half-lives).
To calculate the 125I specific uptake was subtracted the cpm of samples with KClO4 to standard
samples (eliminate possible iodine that entry into the cell but not by NIS symporter, because KClO4 is
a NIS blocker). To normalization, the cpm from each sample was divided by the concentration of
protein present in each sample. Results are expressed as control percentages (%).
The protocol applied in this experiment followed the investigation made by Souza et al in 2010 in Brasil, and was compared with other studies made with 125I in thyroid cells. The resume is show in Table3.1:
Stock C
10 µL Stock A 1mM NaI
990 µL HBSS Stock C1
10 µL Stock A 100 µM NaI 990 µL HBSS
Stock C2