Embed Size (px)
Citation preview

BIOGRAPHICAL SKETCH
Biographical sketch: F. John Gillingham
E. A. C. PEREIRA, P. M. SCHWEDER, A. L. GREEN & T. Z. AZIZ
Department of Neurological Surgery, The West Wing, The John Radcliffe Hospital, Oxford and Oxford Functional
Neurosurgery, Nuffield Department of Surgery, University of Oxford
Francis John Gillingham (Fig. 1) was born on 15th
March 1916 in Dorchester. He studied at Hardye’s
School, Dorset then at St. Bartholomew’s Hospital
Medical College of London University, graduating in
1939. After house officer positions in Bart’s and the
Lord Mayor Treloar Cripples’ Hospital, Alton,
Hampshire, he joined the Royal Army Medical
Corps. Appointed General Duties Officer at the
Oxford Military Hospital at St Hugh’s College, he
managed head injuries under Colonel Hugh Cairns
and Group Captain Symonds. In 1941, Gillingham
was deployed for 18 months in Cairns’ field surgical
unit, a ‘‘crash course’’ in all aspects of neurosurgical
trauma as well as general military surgery.
The young lieutenant then embarked from Liver-
pool via the Cape of Good Hope to serve from the
Battle of El Alamein onwards including the ferocious
Northern Italian campaign. Gillingham recalls that
‘‘in one battle in North Italy we had 1556 patients in
56 days and 6063 overall in three years.’’1 He later
returned to Oxford under Sir Hugh Cairns and
married Judy Irene Jude in 1945. Cairns, a brilliant
administrator, arranged the wedding locally in
Oxford followed by a reception at his home, such
that Gillingham could continue his busy clinical
service until up to the wedding, resuming it after the
briefest of honeymoons nearby. Nevertheless, the
demands of Cairns and later Norman Dott still
allowed time to see four sons raised and enjoy
grandchildren in retirement.
After Oxford, he returned to Bart’s, training under
Sir James Paterson Ross and Mr. John O’Connell. In
1950, he was appointed Consultant Neurosurgeon in
Edinburgh, Deputy Director of the Department of
Surgical Neurology and Senior Lecturer in Surgical
Neurology at the University of Edinburgh. In 1962,
he was named Reader and, in 1963, became
Professor of Surgical Neurology at the University of
Edinburgh. Academic and clinical neurosurgery at
Edinburgh prospered under him with the establish-
ment of a 18-bed head and spinal injuries research
unit, expanded to 30 beds as required, at the Royal
Infirmary and a 65-bed elective surgery and stereo-
tactic neurology service at the Western General
Hospital.2
In 1955, he was elected a Fellow of the Royal
College of Surgeons of Edinburgh. In 1960 he
became its Morison Lecturer and was elected to its
council in 1968.In 1980 he resigned the Edinburgh
Chair of Neurosurgery to take up his position as
President of the Royal College of Surgeons of
Edinburgh. He was made a Fellow of the Royal
Society of Edinburgh in 1970.
Gillingham was one of three surgeons younger than
28 years of age who together performed almost 4000
field operations for missile injuries during wartime.
He kept meticulous notes in three dimensions of each
patient’s injury and operation performed. Inspired by
Gordon Holmes’ wartime discoveries, an interest in
functional neurosurgery arose from detailed diagrams
of bullet and shrapnel trajectories correlated with
clinical findings, leading to postulates on the necessity
of functioning midbrain structures for consciousnessFIG. 1. Frances John Gillingham, PRCS(Ed), CBE, FRSE.
Correspondence: Professor T. Z. Aziz, Department of Neurological Surgery, The West Wing, The John Radcliffe Hospital, Oxford, OX3 9DU.
Tel: þ44 (0) 1865 234605. Fax: þ44 (0) 1865 231885. E-mail: [email protected]
Received for publication 7 January 2009. Accepted 9 January 2009.
British Journal of Neurosurgery, April 2009; 23(2): 143–146
ISSN 0268-8697 print/ISSN 1360-046X online ª The Neurosurgical Foundation
DOI: 10.1080/02688690902736993
Br
J N
euro
surg
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
5/14
For
pers
onal
use
onl
y.

that later came to be known as the reticular activating
system. An enduring interest in neurosurgical trauma
and the prevention of head injury led to implementa-
tion of a head injury assessment scale in Edinburgh
prior to others’ establishment of the Glasgow Coma
Scale.As Cairns had done for motorcyclists’ crash
helmets,3–5 Gillingham became a prominent cam-
paigner for the introduction of the car seatbelt
legislation and in 1979 he was the recipient of the
Clark Foundation Award for Services to Road Safety.
In 1982, he was made a Commander of the Most
Excellent Order of the British Empire.
Gillingham spent 12 years alongside Norman
McOmish Dott, one of the great triumvirate, along-
side Sir Hugh Cairns in Oxford and Sir Geoffrey
Jefferson in Manchester, the apostles of Cushing,
who definitively established neurosurgery as a speci-
alty in Great Britain. Like Dott who first taught him
to wrap and clip cerebral aneurysms, Gillingham was
a brilliant and pioneering vascular neurosurgeon. As
well as establishing the optimal time between sentinel
bleed and rupture to clip cerebral aneurysms and
minimise haemorrhage, pioneering use was made of
wrapping, coiling and papavarine lavage.6,7 Dott and
Gillingham also related arterial pulsations to cere-
brospinal fluid flow in normal cisterns and suggested
a vasogenic origin for subarachnoid cystic collec-
tions.
Gillingham was introduced to stereotactic surgery
by Guiot, who had visited Edinburgh to learn
aneurysmal surgery from Dott and Gillingham.8
Guiot’s 1953 telegram to Gillingham read ‘‘I have
something interesting to show you – come over.’’
Gillingham obeyed and four days were spent
performing freehand pallidotomies under local
anaesthesia using a subfrontal approach to the
anterior perforated substance.9 Gillingham’s wealth
of experience in aneurysmal surgery led him to adapt
Guiot’s stereotactic method to an occipitoparietal
approach to avoid striate arteries (Fig. 2).10 Thus the
Guiot-Gillingham stereotactic apparatus was devised
(Fig. 3).
In 1960 he published results from stereotactic
‘‘thermal electrocoagulation lesions of the globus
pallidus, internal capsule and thalamus either sepa-
rately or in combination’’ in 60 patients.11 ‘‘Of these
patients 53, or 88%, had tremor and/or rigidity
abolished or significantly reduced without complica-
tions.’’ On his modification of Guiot’s stereotactic
apparatus he stated
that the merits of this method lie in the relatively
short operative procedure and in its accuracy and
simplicity. Its principles are based on the fact that
the globus pallidus and thalamus bear a reasonably
constant anatomical relationship to the anterior
and posterior commissures, the intercommissural
line, and the mid-sagittal plane of the head. . . . The
method used has evolved progressively, and is
unique, in allowing the creation of lesions in the
globus pallidus, internal capsule, or thalamus with
one electrode track at different depths.
The Guiot-Gillingham frame’s conception pre-
ceded Hassler’s discovery of the thalamus as a target
for tremor and Gillingham attributed to serendipity
that his posterior approach enabled multiple targets
to be lesioned in a single pass.12
Despite impressive clinical outcomes, Gillingham
noted some inaccuracy to his lesions given observa-
tions that relationships between basal ganglia struc-
tures and commissural landmarks were highly
variable.13,14 David Whitteridge, his neurophysiolo-
gist colleague at Edinburgh, had demonstrated to
him in 1961 how microelectrode recording could
distinguish between grey and white matter and thus
delineate the lateral geniculate nuclei in the cat.15
He immediately saw its utility for distinguishing
functionally between deep brain structures and
FIG. 2. Gillingham (left) preparing for a stereotactic thalamotomy
in 1968 (after Housepian, 2004).24
FIG. 3. The Guiot-Gillingham stereotactic apparatus using a
posterior rather than a coronal approach (after Gillingham et al.,
1960).11
144 E. A. C. Pereira et al.
Br
J N
euro
surg
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
5/14
For
pers
onal
use
onl
y.
developed the technique for humans as did Guiot.16
Fundamental physiological insights were gained from
the first human microelectrode recording studies in a
quest to improve lesion accuracy and clinical efficacy,
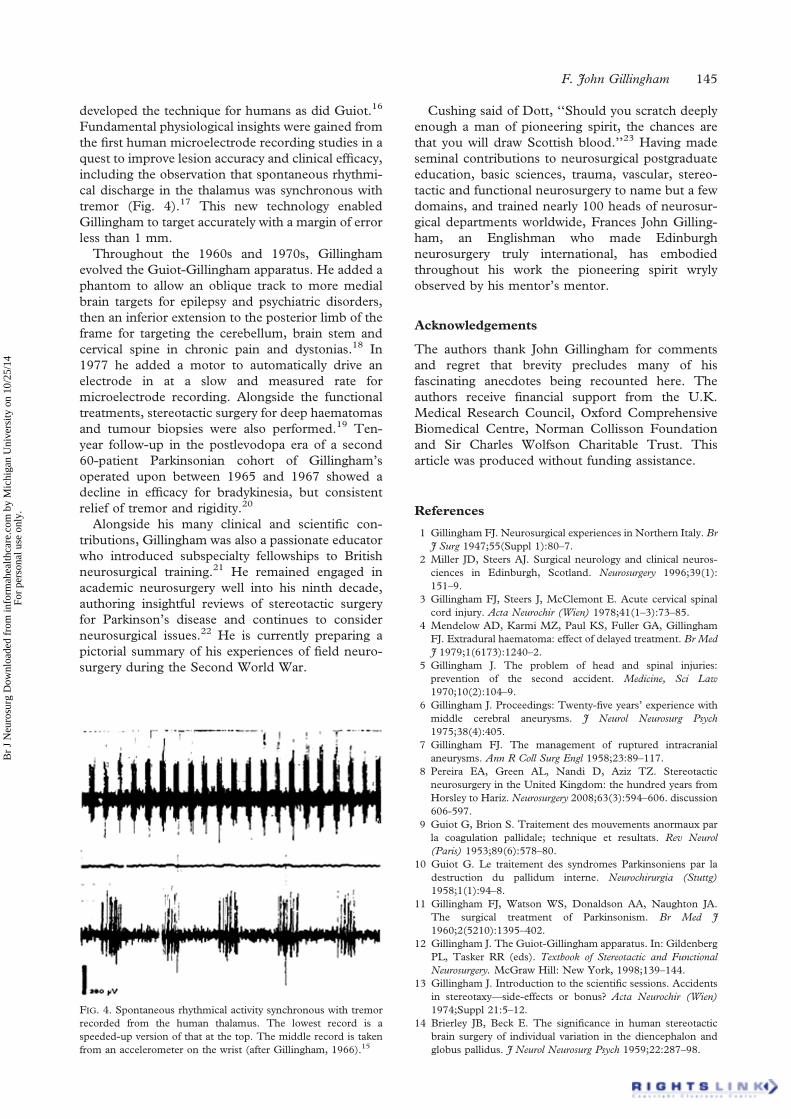
including the observation that spontaneous rhythmi-
cal discharge in the thalamus was synchronous with
tremor (Fig. 4).17 This new technology enabled
Gillingham to target accurately with a margin of error
less than 1 mm.
Throughout the 1960s and 1970s, Gillingham
evolved the Guiot-Gillingham apparatus. He added a
phantom to allow an oblique track to more medial
brain targets for epilepsy and psychiatric disorders,
then an inferior extension to the posterior limb of the
frame for targeting the cerebellum, brain stem and
cervical spine in chronic pain and dystonias.18 In
1977 he added a motor to automatically drive an
electrode in at a slow and measured rate for
microelectrode recording. Alongside the functional
treatments, stereotactic surgery for deep haematomas
and tumour biopsies were also performed.19 Ten-
year follow-up in the postlevodopa era of a second
60-patient Parkinsonian cohort of Gillingham’s
operated upon between 1965 and 1967 showed a
decline in efficacy for bradykinesia, but consistent
relief of tremor and rigidity.20
Alongside his many clinical and scientific con-
tributions, Gillingham was also a passionate educator
who introduced subspecialty fellowships to British
neurosurgical training.21 He remained engaged in
academic neurosurgery well into his ninth decade,
authoring insightful reviews of stereotactic surgery
for Parkinson’s disease and continues to consider
neurosurgical issues.22 He is currently preparing a
pictorial summary of his experiences of field neuro-
surgery during the Second World War.
Cushing said of Dott, ‘‘Should you scratch deeply
enough a man of pioneering spirit, the chances are
that you will draw Scottish blood.’’23 Having made
seminal contributions to neurosurgical postgraduate
education, basic sciences, trauma, vascular, stereo-
tactic and functional neurosurgery to name but a few
domains, and trained nearly 100 heads of neurosur-
gical departments worldwide, Frances John Gilling-
ham, an Englishman who made Edinburgh
neurosurgery truly international, has embodied
throughout his work the pioneering spirit wryly
observed by his mentor’s mentor.
Acknowledgements
The authors thank John Gillingham for comments
and regret that brevity precludes many of his
fascinating anecdotes being recounted here. The
authors receive financial support from the U.K.
Medical Research Council, Oxford Comprehensive
Biomedical Centre, Norman Collisson Foundation
and Sir Charles Wolfson Charitable Trust. This
article was produced without funding assistance.
References
1 Gillingham FJ. Neurosurgical experiences in Northern Italy. Br
J Surg 1947;55(Suppl 1):80–7.
2 Miller JD, Steers AJ. Surgical neurology and clinical neuros-
ciences in Edinburgh, Scotland. Neurosurgery 1996;39(1):
151–9.
3 Gillingham FJ, Steers J, McClemont E. Acute cervical spinal
cord injury. Acta Neurochir (Wien) 1978;41(1–3):73–85.
4 Mendelow AD, Karmi MZ, Paul KS, Fuller GA, Gillingham
FJ. Extradural haematoma: effect of delayed treatment. Br Med
J 1979;1(6173):1240–2.
5 Gillingham J. The problem of head and spinal injuries:
prevention of the second accident. Medicine, Sci Law
1970;10(2):104–9.
6 Gillingham J. Proceedings: Twenty-five years’ experience with
middle cerebral aneurysms. J Neurol Neurosurg Psych
1975;38(4):405.
7 Gillingham FJ. The management of ruptured intracranial
aneurysms. Ann R Coll Surg Engl 1958;23:89–117.
8 Pereira EA, Green AL, Nandi D, Aziz TZ. Stereotactic
neurosurgery in the United Kingdom: the hundred years from
Horsley to Hariz. Neurosurgery 2008;63(3):594–606. discussion
606-597.
9 Guiot G, Brion S. Traitement des mouvements anormaux par
la coagulation pallidale; technique et resultats. Rev Neurol
(Paris) 1953;89(6):578–80.
10 Guiot G. Le traitement des syndromes Parkinsoniens par la
destruction du pallidum interne. Neurochirurgia (Stuttg)
1958;1(1):94–8.
11 Gillingham FJ, Watson WS, Donaldson AA, Naughton JA.
The surgical treatment of Parkinsonism. Br Med J
1960;2(5210):1395–402.
12 Gillingham J. The Guiot-Gillingham apparatus. In: Gildenberg
PL, Tasker RR (eds). Textbook of Stereotactic and Functional
Neurosurgery. McGraw Hill: New York, 1998;139–144.
13 Gillingham J. Introduction to the scientific sessions. Accidents
in stereotaxy—side-effects or bonus? Acta Neurochir (Wien)
1974;Suppl 21:5–12.
14 Brierley JB, Beck E. The significance in human stereotactic
brain surgery of individual variation in the diencephalon and
globus pallidus. J Neurol Neurosurg Psych 1959;22:287–98.
FIG. 4. Spontaneous rhythmical activity synchronous with tremor
recorded from the human thalamus. The lowest record is a
speeded-up version of that at the top. The middle record is taken
from an accelerometer on the wrist (after Gillingham, 1966).15
F. John Gillingham 145
Br
J N
euro
surg
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
5/14
For
pers
onal
use
onl
y.

15 Gillingham FJ. Neurosurgery. Br J Surg 1966;53(10):
833–36.
16 Guiot G, Hardy J, Albe-Fessard D. Delimination precise des
structures sous-corticales et identification de noyaux thalami-
ques chez l’homme par l’electrophysiologie stereotaxique.
Neurochirurgia (Stuttg) 1962;5:1–18.
17 Gaze RM, Gillingham FJ, Kalyanaraman S. Porter RW,
Donaldson AA, Donaldson IM. Microelectrode recordings
from the human thalamus. Brain 1964;87:691–706.
18 Gillingham FJ, Campbell D. Surgical interruption of the
conduction pathways for the control of intractable epilepsy.
Acta Neurochir Suppl (Wien) 1980;30:67–74.
19 Kalyanaraman S, Gillingham FJ. Stereotaxic biopsy. J Neuro-
surg 1964;21:854–8.
20 Kelly PJ, Gillingham FJ. The long-term results of stereotaxic
surgery and L-dopa therapy in patients with Parkinson’s
disease. A 10-year follow-up study. J Neurosurg 1980;53(3):
332–37.
21 Gillingham FJ. Surgical training in the EEC–the training of a
specialist. Acta Neurochir (Wien) 1982;61(1–3):17–24.
22 Gillingham J. Forty-five years of stereotactic surgery for
Parkinson’s disease: a review. Stereotact Funct Neurosurg
2000;74(3–4):95–8.
23 Rush C, Shaw JF. With sharp compassion : Norman Dott Freeman
surgeon of Edinburgh. Aberdeen University Press: Aberdeen,
1990; xvii, 314.
24 Housepian EM. Stereotactic surgery: the early years. Neuro-
surgery 2004;55(5):1210–14.
146 E. A. C. Pereira et al.
Br
J N
euro
surg
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mic
higa
n U
nive
rsity
on
10/2
5/14
For
pers
onal
use
onl
y.