Embed Size (px)
Citation preview

ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2018
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Science and Technology 1712
Bioactive Coatings andAntibacterial Approaches forTitanium Medical Implants
OSCAR JANSON
ISSN 1651-6214ISBN 978-91-513-0424-3urn:nbn:se:uu:diva-358253

Dissertation presented at Uppsala University to be publicly examined in Häggsalen,Ångströmlaboratoriet, Lägerhyddsvägen 1, Uppsala, Friday, 12 October 2018 at 09:15 forthe degree of Doctor of Philosophy. The examination will be conducted in English. Facultyexaminer: Professor Pentti Tengvall (University of Gothenburg).
AbstractJanson, O. 2018. Bioactive Coatings and Antibacterial Approaches for Titanium MedicalImplants. Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty ofScience and Technology 1712. 63 pp. Uppsala: Uppsala University. ISBN 978-91-513-0424-3.
The aim of this thesis was to characterize and manufacture coatings and surfaces withantibacterial properties and retained or enhanced bioactivity and biocompatibility. The aimwas also to study the optimal composition and parameters of mixtures for debridement ofbacterial biofilms on titanium surfaces. The mixtures contained TiO2 particles and H2O2 andwere irradiated by light to activate reactive oxygen species (ROS) formation.
In the first part of the thesis, characterization of a thin, multifunctional hydroxyapatite (HA)coating was performed. The coating was applied to anodized cancellous bone screws with thepurpose of stimulating local bone formation without bonding too firmly and providing localantibacterial effect. Specifications of the coating included a thickness of around 1 µm, highcrystallinity, Ca/P ratio close to the theoretical value of 1.67 and comprise the functional groupsof HA. Additionally, the adhesion of the coating to the substrate should be stronger than thecohesion of the coating. Characterization results showed that the coating met the specificationfor all criteria.
In the second part of the thesis, titanium discs were soaked in H2O2 and subsequently inNaOH and Ca(OH)2 to acquire an antibacterial surface that at the same time is bioactive andbiocompatible. The surface demonstrated bioactive properties, assessed by soaking in phosphatebuffered saline for seven days in 37°C and examined in scanning electron microscopy and X-ray diffraction.
The third part of the thesis consisted of studying the ROS generation of TiO2/H2O2 mixturesirradiated with UV-Vis light, and to study the antibacterial effect of these mixtures on S.epidermidis Xen 43 and Pseudomonas aeruginosa biofilms on titanium surfaces. The generationof ROS from different TiO2 crystalline forms and different H2O2 concentrations under light UV-Vis irradiation was determined by rhodamine B degradation. It showed that rutile and 1-3.5mM H2O2 resulted in the highest degradation of all combinations with almost 100% degradationunder 365 nm light and 77% degradation under 405 nm light after 10 min.
The debridement of the S. epidermidis and P. aeruginosa biofilm discs showed that 0.95 M(3%) H2O2 was the most effective parameter for disinfection of the discs. The addition of TiO2
particles showed a significant extra effect in one of the three studies.
Keywords: Bioactivity, antibacterial, titanium, hydrogen peroxide, hydroxyapatite, biomaterial
Oscar Janson, Department of Engineering Sciences, Applied Materials Sciences, Box 534,Uppsala University, SE-75121 Uppsala, Sweden.
© Oscar Janson 2018
ISSN 1651-6214ISBN 978-91-513-0424-3urn:nbn:se:uu:diva-358253 (http://urn.kb.se/resolve?urn=urn:nbn:se:uu:diva-358253)

To my family


List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Janson, O.*, Sörensen, J.*, Procter, P., Strømme, M., Engqvist, H., Welch, K. Development of a novel multifunctional hydrox-yapatite coating for orthopedic implants. Submitted.
II Janson, O., Gururaj, S., Pujari-Palmer, S., Karlsson Ott, M., Strømme, M., Engqvist, H., Welch, K. Titanium surface modi-fication to enhance antibacterial and bioactive properties while retaining biocompatibility. Submitted.
III Hulsart-Billström, G.*, Janson, O.*, Engqvist, H., Welch, K., Hong, J., Thromboinflammation as bioactivity assessment of H2O2-alkali modified titanium surfaces. Submitted.
IV Janson, O., Unosson, E., Strømme, M., Engqvist, H., Welch, K. (2017) Organic degradation potential of a TiO2/H2O2/UV-vis system for dental applications. Journal of Dentistry, 67(2017):53–57
V Janson, O., Strømme, M., Engqvist, H., Welch, K. Debride-ment of Bacterial Biofilms by TiO2/H2O2 Solutions and Visible Light Irradiation. International Journal of Biomaterials,vol. 2018: Article ID 5361632, 8 pages, 2018.
* These authors contributed equally to this work and are joint first authors
Reprints were made with permission from the respective publishers.

Author contribution
Paper I Part of experimental work and part of writing. Paper II Part of planning, part of experimental work and major part of
writing. Paper III Part of planning, part of experimental work and part of writ-
ing. Paper IV Part of planning, all experimental work (except specific sur-
face area analysis) and part of writing. Paper V Major part of planning, all experimental work and major part
of writing.

Contents
1.Introduction ................................................................................................ 11
2. Aims and objectives .................................................................................. 13
3. Theoretical background ............................................................................ 14 3.1 Osseointegrated implants ................................................................... 14 3.2 Osseointegration ................................................................................. 15 3.3 Bioactive surfaces .............................................................................. 16 3.4 Platelet-, coagulation- and complement-activation ............................ 17 3.5 Implant infection ................................................................................ 18 3.6 Antibacterial approaches for titanium implants ................................. 18
3.6.1 Photocatalytic activity ................................................................ 20 3.6.2 H2O2 ............................................................................................ 21
4. Methods .................................................................................................... 24 4.1 Biomimetic coating ............................................................................ 24 4.2 Surface modification .......................................................................... 24 4.3 Scanning electron microscopy (SEM) ................................................ 25 4.4 Energy dispersive X-ray spectroscopy (EDS) .................................... 25 4.5 X-Ray Diffraction (XRD) .................................................................. 25 4.6 Focused Ion Beam (FIB) .................................................................... 26 4.7 Fourier Transform Infrared spectroscopy (FTIR) .............................. 26 Adhesion assessment ................................................................................ 27 4.9 Surface roughness .............................................................................. 27 4.10 PBS soaking as bioactivity assessment ............................................ 28 4.11 Whole blood study ........................................................................... 28 4.12 Rhodamine B (RhB) degradation study ........................................... 29 4.13 Antibacterial tests ............................................................................. 30
4.13.1 Direct contact test ..................................................................... 30 4.13.2 Biofilm inhibition test ............................................................... 30 4.13.3 Biofilm removal ........................................................................ 30
4.14 Biocompatibility ............................................................................... 31

5. Results and discussion .............................................................................. 33 5.1 Characterization of HA coating .......................................................... 33 5.2 Bioactivity .......................................................................................... 37 5.3 Antibacterial effect ............................................................................. 42 5.4 Biocompatibility ................................................................................. 50
6. Conclusions ............................................................................................... 52
7. Future work ............................................................................................... 53
8. Svensk sammanfattning ............................................................................ 54
9. Acknowledgement .................................................................................... 56
10. References ............................................................................................... 57

Abbreviations
Ca(OH)2 Calcium hydroxide Ca/P Calcium/phosphorous ratio CP-Ti Commercially pure titanium EDS Energy dispersive X-ray diffraction EDTA Ethylenediaminetetraacetic acid EPS Extracellular polymeric substance FIB Focused ion beam FTIR Fourier transform infrared spectroscopy HA Hydroxyapatite HDF Human dermal fibroblast H2O2 Hydrogen peroxide HO2• Hydroperoxyl radical MAA Metabolic activity assay NaOH Sodium hydroxide •OH Hydroxyl radical O2
- Superoxide radical PBS Dulbecco´s phosphate buffered saline PDGF Platelets derived growth factor PVC Polyvinyl chloride RhB Rhodamine B ROS Reactive oxygen species SBF Simulated body fluid SEM Scanning electron microscopy TAT Thrombin-antithrombin TCC Terminal complement complex TiO2 Titanium dioxide Ti64 Titanium alloy Ti-6Al-4V TGF-β Transforming growth factor β TSB Tryptic soy broth UTHA Ultrathin hydroxyapatite UV-Vis Ultraviolet-visible XRD X-ray diffraction


11
1.Introduction
The average human life expectancy in the world has increased drastically during the last hundred years. A higher amount of elderly people than ever, live an active lifestyle and the demand of replacing worn out joints or lost teeth is increasing.
One of the first known implants is dated back to the Mayan population 600 AD who used seashells to restore missing teeth. Radiological studies have shown prominent bone formation around the seashell, similar to around modern dental implants [1].
In the end of the 19th century and beginning of the 20th century, Lane and others started to use screws and plates of steel to fixate bone fractures [2]. The first successful hip joint replacement was performed in 1938 by Smith-Petersen with a mold made of vitallium [3].
One of the earliest osseointegrated implants, was an iridio-platinum im-plant placed in the jaw-bone of a patient by Greenfield in 1913 [1]. In the following decades, a continuous evolution of implant materials and tech-niques took place, before Brånemark implanted the first osseointegrated titanium implant in 1965 [4]. Titanium has since then been used as an im-plant material in for example teeth, hip and knee implants and bone screws. The field of biomaterial implants is an emerging field with need for research to meet the demand to counteract the problems that it is facing. One such problem is implant-associated infections.
Peri-implantitis is an infectious disease affecting dental implants; it is caused by bacterial biofilms formed by periodontal pathogen around the dental implant abutment and approaching the screw, leading to inflammation and associated bone loss. A meta-analysis has estimated the prevalence of peri-implantitis to 22% of all patients with dental implants [5]. This has led to large cost for dentistry and much suffering for the patients. The economi-cal and societal demand for an effective treatment solution for peri-implantitis is thus very high. Similar issues can be found with orthopedic implants. For example, the reoperation rate caused by deep infection two years after hip implant surgery is between 1-2% [6]. But the cost and com-plications of a revision surgery are much higher than for dental implants.
Antibacterial coatings and surfaces can be classified as either passive or active. Passive coatings are coatings that do not release any antimicrobial substances from the surface. Examples can be surfaces with a specific crystal phase, texture or roughness that impede the bacteria from attaching. An ac-

12
tive coating is a coating that releases an antimicrobial substance. For exam-ple, a hydroxyapatite coating loaded with antibiotics, or antibacterial coat-ings with inorganic ions such as silver and copper can be considered active antibacterial coatings.
Hydrogen peroxide (H2O2), hydroxyl radical (•OH) and superoxide radi-cal (O2
-), also known as reactive oxygen species (ROS), are predominately used as bactericides in this thesis. Reactive oxygen species are used by the immune system to eliminate pathogens but can also lead to damage to the cells, if not scavenged by antioxidants.
A fast and strong integration of the implant into the bone are crucial for a successful implantation. The cells of the host are competing with bacteria to colonize the surface; therefore it is important to create a surface that supports osteoinduction.
Titanium in itself mediates good osseointegration, however the anchorage is not through a chemical bond, rather a physical bond and often accompa-nied with a non-mineral layer separating the implant surface from the bone. Therefore titanium implants can be covered by bioactive coatings like hy-droxyapatite (HA). Methods to make the surface directly bioactive by modi-fication of the native oxide layer have been extensively studied. In this thesis the oxide layer is modified by soaking in H2O2, NaOH and Ca(OH)2.
The disposition of the thesis is as follows: In the first paper, a hydroxyap-atite coating on titanium cancellous bone screw was characterized. In paper II, the bioactivity, biocompatibility and antibacterial properties of H2O2 and alkali modified surfaces were studied. The thromboimflammatory responses of these surfaces were studied in paper III. The ROS generation from light irradiated TiO2 and H2O2 mixtures were studied in paper IV, and finally the antibacterial ability against biofilms of these mixtures was studied in paper V.

13
2. Aims and objectives
The first general aim and objective for this study was to create surfaces or coatings with the ability to prevent bacterial biofilm formation on the im-plant and at the same time have a proper bioactivity and biocompatibility.
The specific aim of paper I was to characterize a hydroxyapatite coating on cancellous bone screws with respect to thickness, crystallinity, Ca/P ratio, functional groups and adhesion to the substrate.
The specific aim of paper II was to produce a Ti-peroxy gel layer on commercially pure titanium (CP-Ti) grade 2 discs, which on degradation release H2O2. The objective was to obtain antibacterial effect without pro-voking cytotoxicity. The aim was also to incorporate alkali ions in the Ti-peroxy gel layer, which possibly could produce a bioactive surface.
In paper III, the specific aim was to study the thromboinflammatory re-sponse in human whole blood to the surface produced in paper II, to assess if the surface may be bioactive. The second general aim and objective for this study was to explore the opti-mal parameters for debridement of biofilm-coated CP-Ti grade 2 discs, with H2O2 and photocatalysis of TiO2 particles.
The specific aim of paper IV was to study which parameters with regards to TiO2 particle type, H2O2 concentration and wavelength of light, generated the most reactive oxygen species (ROS). With the departure from the param-eters that generated the most ROS in the paper IV study, the aim in paper V was to explore which parameters are most effective to remove biofilms of the bacteria strains Staphylococcus epidermidis Xen 43 and Pseudomonas aeruginosa from sandblasted and acid etched CP-Ti discs.

14
3. Theoretical background
3.1 Osseointegrated implants The term osseointegration was coined by P. I. Brånemark after observing that titanium fused very strongly to bone [4]. Osseointegrated implants can be hip implants, knee implants, bone screws and plates, dental implant and other implants that integrate to the bone.
For an implant to be successful it must attain certain criteria. The first cri-terion is that it must have the appropriate mechanical properties needed to endure the forces required for that application. The second criteria is that it must be corrosion resistant for the time period it is implanted, and the third criteria is that it must lack cytotoxicity, mutagenicity, immunogenicity and carcinogenicity [7]. It is mainly titanium’s ability to osseointegrate, non-corrosive properties, high strength to density ratio and biocompatibility that make titanium such a popular material for implants in almost all parts of the body. The most relevant implants for this thesis are dental implants and bone screws.
Stainless steel and cobalt chrome are two other materials that are used as implants in the body. The drawbacks of these materials are that they emit ions such as Ni, Co and Cr [8], that can hinder integration. They also have a much higher elastic modulus than bone which can lead to stress shielding. No other metal has as high strength to density ratio as titanium. Titanium exhibits excellent biocompatibility, due to its thin native oxide layer, that is formed when titanium is exposed to air. The oxide layer is roughly 5 nm thick and amorphous and consists of a mixture of TiO, TiO2, Ti2O3 and Ti3O4 [9]. It works as a passivating layer that preclude titanium ions from interacting with blood and other bodily fluids which can corrode the material [7].
Titanium exist in two allotropic phases, the α-phase which has a close packed hexagonal structure (cph) and the β-phase which has a body centered cubic structure (bcc). Titanium used in implants can be divided into unal-loyed or α-phase, β-phase and α + β-alloys. The α-phase exists below 883°C and above that temperature it transforms to the β-phase [10]. Alloying with aluminum, oxygen and nitrogen can stabilize the α-phase at lower tempera-tures and molybdenum, iron, vanadium, chromium and manganese stabilizes the β-phase. Commercially pure titanium consists of the α-phase and is most-ly used in dental implants.

15
There exist four grades of CP-Ti with increasing oxygen content, which increase the tensile strength and decrease the ductility. In dental implants the ductility is important for designing implants with screw threads. The strength is not as important as in load bearing orthopedic implants. Titanium alloy Ti-6Al-4V (Ti64), which is an α + β alloy is the most commonly used alloy for load bearing applications. The biocompatibility is better in pure titanium than in alloys [11], which make it desirable to use pure titanium when high forces is not present.
3.2 Osseointegration Osseointegration is defined as the direct connection between living bone and an implant on the light microscopic level [9]. Osseointegration is accom-plished as a result of the immune system responding to the surface by creat-ing a foreign body response. Surface proteins and the complement system activates the process by forming fibrin and engage granulocytes, mesenchy-mal stem cells and macrophages [12].
The evolution of the osseointegration process has been described by Ter-heyden et al. as follows [13]. Seconds after an implant surgery, the serum proteins: albumin, fibrinogen and fibronectin, adhere to the implant surface. The bleeding is stopped by platelets, and platelets release thromboxin, plate-let-derived growth factor (PDGF), transforming growth factor alpha and transforming growth factor beta (TGF-β) to stimulate cell division of fibro-blasts. Fibrin creates a network called the blood clot. Hours after the surgery, the inflammatory phase starts by bradykinin, released from the platelets, which increases the permeability of the blood vessels. Polymorphonuclear leukocytes are diffused through the endothelial cells of the blood vessels and eliminate bacteria through release of ROS. Macrophages dominate the late inflammatory phase by phagocytosis of bacteria and necrotic cells. Days after the surgery, perivascular cells, which are mesenchymal stem cells on blood vessels, differentiate into osteoblasts and fibroblasts. Osteoclasts are large multinucleated cells that dissolute the bone substance through acidic values and proteolytic enzymes. The dissolved bone releases bone morpho-genic protein, TGF-β and PDGF which recruit osteoblasts. Osteoblasts form new bone through expression of proteins such as type I collagen as well as release of calcium phosphates and carbonates. The proliferation phase ends with the formation of woven bone. Weeks after surgery osteocytes are re-modeling the woven bone to lamellar bone.
Usually osseointegration of implants are successful, but for older patients or patients with diabetes who suffers from poor bone quality or osteoporosis there is a need to increase the fixation of the implant.

16
3.3 Bioactive surfaces Bioglass was invented by Dench in 1969. It was a new type of ceramic mate-rial with highly negatively charged surfaces that exhibited bioactivity [14]. Kokubo et al. incorporated alkali ions on TiO2 surfaces to form a bioactive layer by making the surface negatively charged, thereby forming a bioactive titanium surface [15,16]. According to the ESB consensus conference 1987, a bioactive material is “one which has been designed to induce specific bio-logical activity” [17]. However, in the interaction between an implant and bone, the definition has been stated by Kokubo and Takadama to be a mate-rial that bonds to bone [18]. More specifically, they state that a material that is able to form apatite when implanted in the body or in a simulated body fluid is able to form bone. Titanium-hydroxyl groups on the surface attracts Ca2+ ions and form amorphous calcium titanate, which subsequently form amorphous calcium phosphate and finally crystalline HA [19]. The apatite layer on the bioactive implant interact with collagen fibrils to bond with the host bone [14].
The negatively charged surfaces lead to superhydrophilicity which is fa-vorable for bioactivity, and binds calcium and phosphate ions, creating a HA layer [20]. Negatively charged surfaces can be made by soaking in solutions with alkali ions. Ion exchange between the surface and the bone leads to a chemical bond [21], making the difference between the cement line and the material surface indistinguishable [22]. Bioactive titanium is osteoconduc-tive i.e. it works as a scaffold for osteoblasts, and calcium incorporated into titanium surfaces have been shown to induce differentiation of osteoblasts from mesenchymal stem cells [23]. The bioactive surface can also recruit osteochondral progenitor cells, this is mediated by the coagulation and com-plement system that trigger growth factors such as TGF-β, and these in turn signaling to the osteochondral progenitor cells to mature into osteoblasts [24].
An untreated titanium surface is bioinert [25], which means that it is non-reactive with foreign bodies and non-biodegradable by tissues [26]. When coated with hydroxyapatite (HA), which is the inorganic component of bone, a chemical bond is established between the coating and the bone [27]. The biggest advantage is that the fixation occurs faster than without coating [28]. The chemical formula of HA is Ca5(PO4)3OH, but is often written as Ca10(PO4)6(OH)2 because the unit cell comprises two HA molecules. The Ca/P ratio of HA is 1.67 and is an important value when assessing the phase purity.
The most common technique used to coat hydroxyapatite on implants is plasma spraying. The drawback of this coating technique is that it creates a dense HA layer with low porosity [29]. Because of the high temperature needed, the coating also has a thickness of up to 50-75 µm [28]. The high thickness can make the hydroxyapatite coating crack. With physical vapor

17
deposition it is possible to coat a thinner layer. But because of the line-of- sight limitation of this method, it has problems coating complex surfaces geometries such as screw threads.
The biomimetic hydroxyapatite coating procedure enables formation of bonelike apatite crystals with high bioactivity and good resorption [30]. Fur-thermore, the coating method can coat complex surfaces at low temperature and biological pH [29]. The nucleation of apatite is stimulated by a local supersaturation in the PBS, caused by release of OH- from the oxide layer, which yields a slight increase in pH of the PBS [31]. Amorphous apatite is formed which subsequently transforms to crystalline HA [31].
3.4 Platelet-, coagulation- and complement-activation Blood is the first substance that comes into contact with the implant during implantation.
High molecular weight proteins like albumin, globulin and fibrinogen are the first substances that attach to the surface. The attachment depends on the properties of the surface. These initially attached proteins constitute the sur-face that platelets, coagulation system and complement system are exposed to. Platelets aggregate on the surface and are later activated by thrombin, generated from the coagulation system. The platelets also augment the coag-ulation cascade by releasing factor V and fibrinogen. A blood clot is formed that reduces the healing time. The formation of bone goes through the fol-lowing stages; blood clot formation, inflammation, granulation tissue for-mation, cartilagous callus formation, cartilage mineralization, and woven bone formation remodeling [32].
Thrombin-antithrombin (TAT) is a complex that is formed to control the rate of coagulation; it consists of thrombin and the anticoagulant antithrom-bin. It is a common marker for analyzing if the coagulation system is acti-vated.
When the platelets are activated by thrombin, they release granules which consist of growth factors. These growth factors trigger mesenchymal stem cells to differentiate into osteoblasts, osteoclasts and osteocytes. Therefore is platelet activation an important part in bone formation.
The complement system contributes primarily to the recruitment of the immune system and inflammation. C3a is an anaphylotoxin that is formed from cleavage from C3. It plays an important role in inflammatory process-es.
The terminal complement complex (TCC) consists of the C5b that attach-es to C6, C7, C8 and C9. It forms a complex that is very effective in pene-trating the membrane of pathogens, leading to cell lysis. If no cell mem-branes are present, protein S binds to the complex and makes it inactive in

18
the solution. The TCC has been reported to increase bone fracture healing [33].
3.5 Implant infection A bacterial biofilm is a bacterial community encased in an extracellular pol-ymeric substance (EPS) [34]. The EPS consists of polysaccharides, proteins and DNA [35]. The formation of a biofilm is advantageous for the bacteria as they obtain a higher resistance against antimicrobials [36]. The biofilm attach to a surface initially by van der Waals forces and hydrophobic effects as the hydrophobic bacteria have reduced repulsion to the surface [37,38]. Subsequently, it anchors with cell adhesion structures. The antibiotic re-sistance of biofilms has been reported to be up to 100-1000 times higher compared to planktonic bacteria [39]. The reason for this is reduced penetra-tion of the antibiotics, activation of a stress response, physiological hetero-geneity of the biofilm population and presence of persister cells [40]. The bacteria in the biofilm are living in a dormant state and are released when it is overpopulated [41]. The formation of biofilms is favored by rough envi-ronments such as shearing or by subinhibitory concentrations of antibiotics. Because of the protected environment in the biofilm, implant infections caused by bacterial biofilms can be very difficult to get rid of and can cause chronic infections. On dental implants the biofilm consists of several hun-dreds of different strains [42], but on joint prostheses the biofilm consists most often of monospecial staphylococcal biofilms [43].
A bacterium can sense the presence of a surface and express the adhesion protein, which glue the bacteria to the surface. The bacteria communicate with each other by a signal system called quorum sensing [44]. This control the nutrient distribution and movement of bacteria within the biofilm com-munity.
Up to 80% of all infections are caused by biofilms [45], and 60-70% of nosocomial infections are associated with implantation of a biomedical de-vice [46]. Biofilm infected implants cause implant loosening and if the bac-teria enter the bloodstream, they can cause infections in other parts of the body. For instance, oral bacteria can cause endocardial inflammation, aspira-tion pneumonitis and diabetes [47,48].
3.6 Antibacterial approaches for titanium implants The attachment of biofilms on bone anchored medical implants can impair the osseointegration, and therefore it is important to have the implant free from biofilm to achieve good osseointegration. Antibacterial approaches can be designed to either prevent biofilm formation or remove existing biofilms.

19
The difficulty in achieving a preventive antibacterial surface is that the sur-face must be able to be biocompatible with the surrounding human tissue, produce a mechanical or chemical bond to the bone and at the same time be able to repel bacteria [49].
Many different implant coatings have been fabricated to kill bacteria or impede biofilm formation. Some examples are; coatings loaded with antibi-otics, coatings comprising non-antibiotic organic antimicrobial agents, coat-ings containing inorganic antimicrobial agents, adhesion resistant coat-ings, modification of physical and chemical surface properties, anti-adhesive polymer coatings, biofunctionalization with antibacterial bioactive polymers, and coatings delivering nitrogen monoxide [50].
For already attached bacteria the most effective methods used today are mechanical methods like brushing with curettes or mechanical methods combined with chemical methods. Today there does not exist a broad spec-trum antimicrobial chemical debridement method [51]. The chemical meth-ods used are sodium hypochlorite, H2O2, chlorhexidine, citric acid or essen-tial oils [52]. Drawbacks with mechanical debridement include damage of the implant surface, which can impede re-osseointegration, especially if the debridement tool is made of a harder material than titanium such as stainless steel [53]. The best results are reached by a combination of mechanical and chemical debridement.
Titanium dioxide particles have the advantage that they both have a me-chanical effect when used together with, for example, a titanium brush and the ability to generate ROS, both in dark and particularly when exposed to light. In an application they could be embedded in a hydrogel and light could be applied with a dental lamp of appropriate power and wavelength [53]. Hydrogen peroxide, which in itself is an effective disinfectant, has been shown to have synergistic effects when in contact with TiO2 and to enhance the photocatalytic effect for the rutile crystal phase in particular [54–56]. Photocatalytic TiO2 particles have been used either as coating of the surface to prevent biofilm formation [57], or immersed in the biofilm [58]. The pho-tocatalytic approach to eliminate bacterial biofilms can be realized either extracellularly by oxidation of peptidoglygan, polysaccharides and phospho-lipids in the EPS [59], or intracellularly (nucleic acid, enzymes and coen-zymes) [60,61]. The main oxidizer of the EPS is •OH, but O2
- and hydro-peroxyl radicals (HO2•) can also cause damage to the bacterial cell mem-brane.
The purpose of the bioactive antibacterial surface for prevention of bio-film formation is to prevent biofilm from forming in the initial weeks after surgery that is most critical for biofilm formation. At this point, the bacteria reaching the surface are still in a planktonic state and more susceptive for antibacterial substances. After this period, with increased host tissue integra-tion, the infection risk is considerably reduced [62].

20
The best way to prevent biofilm formation on biomedical implants is to have a sterile implant during the surgery. A proper surgical implantation resulting in a fast and complete osseointegration also play a crucial part in maintaining an infection free surface. Having a completely sterile environ-ment during surgery is very difficult to obtain; moreover hematogenous spread of bacteria can result from bacteria originating from infection sites in other parts of the body [62]. Likewise in a revision surgery, remaining bacte-ria from a previous infection is almost unavoidable. Therefore a great deal of research has been conducted with the aim of finding an implant surface that has antibacterial properties but at the same time exhibits bioactive and bio-compatible qualities.
3.6.1 Photocatalytic activity Electrons are occupied in orbitals. In a single molecule in the ground state the electrons reside in the highest occupied molecular orbital and can be excited to the lowest unoccupied molecular orbital by addition of energy from for example UV light. In bulk metal the electrons can move freely be-tween the atoms. On the other hand, insulators, for example a crystal, have a large band gap between the valence band and the conduction band that is normally impossible for the electrons to overcome. However, in a semicon-ductor the bandgap is small enough for the electrons of the valence band to overcome, if enough energy is added by, for instance, UV light. When an electron is excited to the conduction band an electron-hole pair is formed (equation 1). The excited electron in the conduction band can react with surface-adsorbed oxygen (O2) by donating an electron to the O2 thereby pro-ducing O2
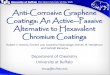
- (equation 2). The corresponding valence band hole can oxidize water (H2O) or hydroxyl ions (OH-) to result in •OH (equations 3 & 4) (for a schematic description, see figure 1.).
TiO2 + hν → e- + h+ (1) e- + O2 → O2
- (2) h+ + H2O → •OH (3) h+ + OH- → •OH (4)
The •OH are highly reactive and can attack the lipid layer of the cell mem-brane of bacteria leading to cell death [63].
Photocatalysis has becoming increasingly interesting for use in applica-tions such as solar cells for energy conversion, self-cleaning surfaces and also water and air purification [64]. Research has furthermore been conduct-ed for potential use in biomedical applications for treating cancer [65] and as an antibacterial agent in dental applications [66].

21
Titanium dioxide is a semiconductor and has three common allotropes: rutile, anatase and brookite. Anatase and brookite have a bandgap of approx-imately 3.2 eV and rutile 3.0 eV. Anatase and brookite are more active pho-tocatalysts than rutile because they possess more active sites and have lower recombination rates, while rutile is less photocatalytic but the photocatalytic effect can be increased when rutile is subjected to low concentrations of H2O2 [55,56,67]. A combination of anatase and rutile, such as Evonik P25, has been shown to exhibit a higher photocatalytic effect than pure crystal particles. This is a result of the electrons being transferred between the two crystal structures, thereby utilizing the lower band gap of rutile to extend the photocatalytic effect into the visible region. At the same time, recombination is avoided when the electrons are transferred to the more stable anatase crys-tal [68]. In biomedical applications it is desirable to use visible light because it induces no harm to the tissue. Rutile has a bandgap of approximately 3.0 eV, which means that light of up to 410 nm can produce a charge separation.
Figure 1. A schematic description of the photocatalytic charge separation into an excited electron in the conduction band and hole in the valence band. The conduc-tion band electron reduces oxygen (O2) to generate superoxide radicals (O2
-) and the valence hole oxidize water (H2O) and hydroxyl ions (OH-) to generate hydroxyl radicals (•OH). These radicals can attack the bacterial cell wall.
3.6.2 H2O2
When titanium is exposed to air, it forms a thin oxide layer, as has been de-scribed in Section 3.1. When this layer is oxidized by H2O2 (as shown in figure 2), it grows thicker and forms a nano-porous TiO2 layer on top [69]. Tengvall et al. have comprehensively investigated the interaction between H2O2 and titanium [70–76]. The studies were mainly performed with TiCl

22
powder which together with H2O2 form a gel [70], but also on titanium sur-faces [72]. When H2O2 comes in contact with titanium, a yellow layer which consists of the following titanium-peroxide complex, is formed [70]: Ti4+(OH-)2O - Ti4+(OH-)2O - Ti4+(OH-)x – TiO2 · nHH2O Where x = 1 or 2. The titanium-peroxy radical (Ti4+O2
-) is an important component of this gel, therefore it is called a Ti-peroxy gel [75]. The Ti-peroxy gel formation has been associated with the excellent biocompatibility of titanium. Superoxide radicals reduce the oxidized metal (M) ions (in this case titanium ions) of the Fenton reaction (equation 5), leading to a cyclic continuous production of •OH [71]. When O2
- are trapped inside the TiOOH adduct of the Ti-peroxy gel layer, the •OH formation is quenched.
Mn+ + H2O2 → M(n+1)+ + •OH + OH- (5) Hydrogen peroxide is released from the Ti-peroxy gel layer by hydroperoxyl anion separation from the Ti-complexes with subsequent proton uptake or by H2O absorption of Ti-peroxides [75].
The bactericidal properties of Ti-peroxy gel has been investigated by Tengvall et al. on Escherichia coli bacteria, but amorphous titania was only shown to be bactericidal in the presence of myeloperoxidase [75]. Myelop-eroxidase is released in vivo by neutrophils, and produces the highly reactive hypochlorous acid together with H2O2 [77]. Hypochlorous acid is effective in eliminating pathogens such as bacteria in the human body. It plays also a crucial part in the respiratory burst by forming ammonium chloride and chlo-ramines which are oxidizing thiols both extracellularly and intracellularly. Hydrogen peroxide can act as an antibacterial agent, it is not reactive by itself, but can by oxidation, form highly reactive •OH. This is leading to lipid peroxidation of the bacterial cell wall and subsequently to cell death. Alter-natively, H2O2 can diffuse through the cell wall and by the Fenton reaction react with iron from iron sulphur clusters or hemoglobin, thereby forming •OH that can destroy the DNA of the bacterial cell [78–81]. However several bacteria such as S. epidermidis contain catalase which is an enzyme that neutralizes H2O2. Despite this, H2O2 has been shown to be an effective disin-fectant against Streptococcus mutans [82], Staphylococcus epidermidis [82–85], and E. coli [86].
Hydrogen peroxide can be photolyzed and form two •OH when exposed to light with wavelengths below 360 nm (equation 6). It can also be formed via catalysis from O2
-• according to equation 7 & 8. H2O2 + hν → 2•OH (6) O2
-• + H+ → HO2• (7) 2HO2• + 2•OH → 2H2O2 + O2 (8)

23
Figure 2. A titanium disc (dark oval near the bottom of the tube) after soaking in 30% H2O2 (w/w) for 1 h at 37°C.

24
4. Methods
4.1 Biomimetic coating The biomimetic hydroxyapatite coating in paper I was manufactured by pre-treatment in NaOH for 10 min at 70°C, followed by soaking in PBS with added calcium and magnesium ions for 3 days in 70°C. A 4 L container was used for soaking the screws in PBS, and the volume of PBS was adjusted depending on the number of screws to be coated, to ensure that the volume per screw always was the same for all screws.
4.2 Surface modification Table 1 shows the modifications steps of the sample groups and control group used in paper II. Before the modification steps the surfaces were cleaned by sonication in acetone, ethanol and Milli-Q water for 15 min each. Ti_Control, Ti_H2O2 and TiAuto_Ca were also used for the whole blood study in paper III. TiAuto_Ca was there denoted Ti_Ca.
Table 1. Outline of the surface modification procedures used in papers II and III.
Sample group
Surface treatment Final treatment
H2O2 (30% w/w)
NaOH (5 M)
Ca(OH)2 (0.1 mM)
Ti_Control - - - -
Ti_H2O2 1h - - -
Ti25 1h 15 min - -
Ti25_Ca 1h 15 min 15 min -
Ti200 1h 15 min - 200°C, 1 h
Ti200_Ca 1h 15 min 15 min 200°C, 1 h
TiAuto 1h 15 min - Autoclave
(125°C, 1h)
TiAuto_Ca 1h 15 min 15 min Autoclave
(125°C, 1h)

25
4.3 Scanning electron microscopy (SEM) In contrast to a light microscope an SEM use electrons instead of light to image the surface of a specimen. This enables higher magnification because of the lower wavelength of the electrons compared to visible light.
The electron beam scans the surface and the amount of electrons received by the detector reveals the topography of the surface. There are two types of detectors used in SEM. The secondary electron detector receives electrons that have been released from the K shell after interaction with low energy electrons. These electrons reside from atoms approximately 1 nm from the surface and yield a clear contrast of the topography. A backscatter detector receives electrons of higher energy that have been back scattered against the atoms. Atoms of higher atomic weight scatter more effectively than lighter atoms. The resolution is dependent on the interaction volume and the size of the electron spot, which in turn depends on the wavelength of the electron and the electron-optical system that produce the beam. In papers I, II and IV a LEO 1530 or 1550 SEM (Zeiss, Oberkochen, Germany) was used and operated at 5 or 10 kV and the secondary detector was used. The inspected surfaces were coated with a thin Au/Pd layer to avoid charging effects.
4.4 Energy dispersive X-ray spectroscopy (EDS) In materials science, EDS is commonly used to evaluate the composition of the surface of a material. The EDS detector is placed in an SEM. Electrons are accelerated to the surface and excite the electrons of the material`s at-oms. When the electrons are de-excited an X-ray that has the same energy as the difference between the higher and the lower electron shell is emitted. A higher acceleration voltage produces a deeper interaction volume. If the en-ergy is too low the electron cannot excite an electron to a higher shell. The smallest detection signal is normally defined as three times the standard de-viation of the background count. When the X-ray reaches the detector an electron-hole pair is formed. A voltage is applied to separate the charge car-riers and the signal is proportional to the energy of the X-ray photon. In pa-pers I and II, EDS was used to characterize the composition of the surfaces.
4.5 X-Ray Diffraction (XRD) A crystal is a solid material that consists of atoms, molecules or ions ordered in a microscopic structure, forming a lattice that extends in all directions. The smallest unit of a crystal is called a unit cell. The lattice planes are usu-ally denoted h, k and l and are perpendicular to the x, y and z axis of the unit cell respectively. X-ray diffraction is applied to reveal the crystal structure of

26
a crystalline material. The sample is exposed to a monochromatic X-ray beam and the intensities are recorded at every orientation of the crystal. Eve-ry compound has a unique diffraction pattern. The scattering of the X-rays is measured and the crystal structure of the material can be calculated from equation 9 which is known as Bragg’s law. In equation 9, d is the distance between the atomic planes, θ is the angle between the incoming X-ray and the crystal lattice, λ is the wavelength of the X-ray and n is an integer.
2d Sinθ = nλ (9)
When the atomic planes have the same distance between them as the wave-length of the incoming X-ray there is an interference that produces a double magnitude of the X-ray wavelength. When this is observed the length and angle of the crystal structure can be identified. A high intensity corresponds to high electron density and thereby a higher possibility to identify the crys-tal structure. The diffraction angle reveals where in the unit cell the high density area is located. In paper I, the crystallinity of the HA coating was assessed. In paper II, thin film XRD was used to assess if HA was present on the surface or not with a Siemens D5000 grazing incidence X-ray diffrac-tometer (GI-XRD; Bruker AXS GmbH, Karlsruhe, Germany).
4.6 Focused Ion Beam (FIB) Because of the sputtering capacity of a FIB, it is used as a micro- and na-nomachining tool. It can also be used at low beam current to image surfaces. In contrast to SEM that uses electrons as beam source, FIB normally uses gallium ions. A FIB is commonly used for preparation of transmission elec-tron microscopy samples, which have to be very thin. A drawback of FIB is that it is damaging to the surface. In paper I it was used to cut a cross sec-tion of the hydroxyapatite coating to enable measurement of the thickness of the coating.
4.7 Fourier Transform Infrared spectroscopy (FTIR) The bonds of molecules vibrate and rotate with the absorption of certain infrared frequencies that are characteristic for that bond. By analyzing these vibrations the identity of the molecules in a sample can be revealed. In an FTIR measurement, light with a wide range of infrared frequencies are irra-diated through the sample. This is repeated several times with the frequen-cies of the light modified every time. A computer then transforms the signal to sinusoidal frequencies. The algorithm used to calculate the absorption at each wavelength is a Fourier transform. Obtaining spectra from a wide range

27
of wavelengths results in a higher signal to noise ratio than dispersive spec-troscopy. In paper I, FTIR was used to study the functional groups of the hydroxyapatite coating.
Adhesion assessment The adhesion of the ultrathin hydroxyapatite (UTHA) coating in paper I was assessed by three different methods. The first method was a scratch test in which a spherical tip of Al2O3 was applied to the surface with increasing load from 0 to 100 N during the movement of the tip. The critical pressure at the point of delamination was obtained from equations 10 and 11, where FN is the critical load. E´ is the weighted modulus for the substrate and the tip calculated by equation 11, and R is the radius of the tip.
p0 = -0.578 /
(10)
∗ (11)
The second method was Rockwell indentation which usually is a method to measure hardness, but can also be used to assess the adhesion of a coating. The adhesion of the hydroxyapatite coating was assessed by examining cracks and/or delamination on and off the hydroxyapatite surface, when sub-jected to an indentation force of 100 kgf applied with a conical diamond tip (Rockwell test maschine, Werzeugmaschinen-Kombinat, Leipzig.)
The last method to assess the coating adhesion was screw insertion. A cancellous screw with the UTHA coating was inserted 10 mm into predrilled holes of polyurethane foam which mimic human cancellous bone. The screw was inserted with a hand driven torque screw driver (Bahco model 6973N). The measurement was performed in both “dry” and “wet” conditions, where the “wet” condition was obtained by soaking the foam in PBS in 37°C for 30 min to mimic in vivo conditions.
4.9 Surface roughness Surface roughness is quantified as the deviation of the normal vector of the surface. There are many different roughness parameters but the most com-mon is Ra, which is also used in this thesis. Ra measures the amplitude of the deviation. The surface roughness influence the bone response strongly, with moderately rough surfaces with a Ra = 1-2 µm showing the strongest bone response [87]. The roughness of the surfaces in paper II was measured with

28
an optical profilometer (WYKO NT1100) in the visible shift interferometry mode.
In paper III the surfaces were ground and polished to exhibit a smooth surface, considering the strong influence of surface roughness on platelet activation. The surface roughness was assessed in a contact profilometer (Dektak XT Advance).
4.10 PBS soaking as bioactivity assessment Bioactivity assessment by soaking in simulated body fluid was first applied by Kokubo et al [88]. The optimal mineral content of the SBF has been up-dated several times. Forsgren et al. employed calcium and magnesium en-riched PBS to coat titanium plates with hydroxyapatite and obtained excel-lent results [89].
The containers used for soaking in PBS were 50 ml centrifuge tubes and the surface for assessment or coating was placed facing down. This approach was conducted to secure that the apatite formed was bonded to the surface and not just precipitated on the top of the surface [90]. The soaking time in paper II was 7 days at 37°C and the PBS was replaced once during that time, to secure fresh access of minerals. The mechanism of hydroxyapatite formation is the same as described in Section 4.1.
4.11 Whole blood study All surfaces in contact with blood except the test and control samples were covered with 0.5 g/cm2 heparin. Twenty ml of blood was obtained through heparinized tubes into a centrifuge tube from 5 healthy donors (figure 3 a). A total of 1.4 ml blood was inserted into each well of a slide with the sample on top retained by a clamp (figure 3 b & c), and two samples from each test group was used for each donor. The slide was rotated at 22 revolutions/min for 1 h at 37°C (figure 3 d). A zero blood sample denoted “initial” was set aside without incubation and collected in Eppendorf tubes with a final con-centration of 4 mM etylenediaminetetraacetic acid (EDTA). The other sam-ples were also collected in EDTA-filled Eppendorf tubes after the incubation (final concentration 4 mM). The blood samples were analyzed in a cell coun-ter (XP-300 Hematology Analyzer Sysmex Corporation, Japan). The sample discs were fixated in glutaraldehyde, ethanol and hexamethyldisiloxane (for details see ref. [91]), and analyzed in SEM. The remaining blood after the platelet analysis was analyzed in enzyme-linked immunosorbent assay for TAT, C3a and TCC.

29
Figure 3. a) Blood sampling from a donor, b) blood filled wells with test discs on top, c) blood filled wells with polyvinyl chloride (PVC) control on top attached by a clamp, d) the incubation chamber.
4.12 Rhodamine B (RhB) degradation study In paper IV, the ROS generation of a TiO2/H2O2 mixture, comprising RhB and irradiated by light during 10 min, was assessed. The amount of degraded RhB was examined by monitoring the decrease in absorbance or fluores-cence after the light irradiation. The original objective was to continuously measure the absorbance every 15 s for 60 min to obtain a kinetic reaction coefficient as performed by Unosson et al. [92]. However the TiO2 particles obstructed the light beam of the absorbance spectrometer, making such measurement unattainable. Instead 10 min was chosen as a time point to monitor the organic degradation potential. Although the measurement time is longer than is practical in a clinical setting, it offers an adequate assessment of ROS generation obtained by the photocatalytic effect of the different TiO2/H2O2 mixtures. Rhodamine B is also a fluorescent dye and the fluores-cence was measured in the second round of experiments in paper IV.

30
4.13 Antibacterial tests
4.13.1 Direct contact test In paper II, two different tests were performed to measure the antibacterial effect of the modified titanium surfaces. The first experiment was a direct contact test. This method is an effective method to assay the antibacterial effect on planktonic bacteria on solid surfaces because it is independent of solubility and diffusion [93]. The test was performed by applying a drop of bacteria solution to the surface of the modified titanium discs, followed by incubation at 37°C for 45 min. The incubated discs were subsequently ana-lyzed with luminescence spectroscopy during 7 h. The luminescence meas-urement was made possible because of the employment of the gene modified strain S. epidermidis Xen 43, which is bioluminescent. The lux gene inserted in the genome of metabolically active organisms offers a way of real time quantification of the bioluminescent microorganism [94]. Bioluminescent light producing microorganisms are very sensitive for subtle changes in cell viability. They are also a favorable option for high throughput screening and low cost because no extra substances are needed.
4.13.2 Biofilm inhibition test Assessment of bacterial biofilm presents a bigger challenge than planktonic bacteria for obvious reasons.
The second antibacterial test, used in paper II, was a biofilm inhibition test where the bacteria were grown on the surface during 16 h. The non-adherent bacteria were then washed away with PBS and the discs were rein-cubated with fresh tryptic soy broth (TSB) and measured for luminescence once every hour for 9 h. The luminescence signal is proportional to the amount of planktonic bacteria in the solution. The assumption made was that the amount of released bacteria from the biofilm is proportional to the amount of biofilm bacteria.
4.13.3 Biofilm removal In paper V, biofilms of S. epidermidis Xen 43 were grown on grit blasted and acid etched CP-Ti discs during 8 h at 37°C. The discs were subsequently decontaminated with the treatment conditions displayed in table 2.
After the decontamination step the discs were immersed in TSB and measured once every hour for up to 18 h, and between the measurements the discs were incubated at 37°C. Pseudomonas aeruginosa was chosen as a strain to test the antibacterial activity against gram negative species, and because it is not bioluminescent a metabolic activity assay (MAA) was per-

31
formed. In the MAA, the blue, non-fluorescent dye resazurin was used as an indicator of the metabolism. When it is metabolized by bacteria it transforms to resorufin which is a pink, fluorescent dye. After the cleaning procedure the discs were immersed in TSB and resazurin and assessed for fluorescence once per hour for 6 h and between the measurements the discs were incubat-ed at 37°C in an orbital shaker with a rotation speed of 250 rpm. The fluo-rescence excitation and emission peaks of resazurin are 530 and 590 nm respectively. Five calibration curves with planktonic bacteria from OD 0.02, corresponding to approximately 1.6 x 107 cells/mL, down to zero were ob-tained to compare how much bacteria that were removed from the biofilm. The MAA was also performed on S. epidermidis Xen 43 as a reference. One disc from each test group was fixated according to the description in Section 4.11 and examined with SEM.
Table 2. Description of the treatment conditions for the debridement of the S. epi-dermidis Xen 43 or P. aeruginosa biofilm-covered CP-Ti discs, used in paper V. Exposure time was 1 min for all treatment conditions.
Sample
designation
Concentration rutile
(g/l)
Concentration H2O2
(mM)
Light, intensity: wavelength
(mW/cm2:nm)
Ethanol (Positive control) - - Ambient light
PBS (Negative control) - - Ambient light
0_Hi_Amb - 950 Ambient light
R_Hi_Amb 0.5 950 Ambient light
R_Hi_Li 0.5 950 2.1:405
R_Low_Li 0.5 2 2.1:405
4.14 Biocompatibility To assess the biocompatibility of the modified surfaces, the viability of two different cell lines were examined. The first one was human dermal fibro-blasts (HDF), which simulates the biocompatibility with the soft tissue. The other one was MC3T3 preosteoblasts which simulates the biocompatibility with the bone. The discs were immersed in cell culture and incubated for 1 h at 37°C. The medium was subsequently removed and 50 µl of cell suspen-sion was added dropwise to each disc. The cells were allowed to attach to the discs during 1 h at room temperature, before 450 µl of cell culture was added to the disc-containing wells. The samples were incubated at 37°C and meas-urements of the viability were made after 24 h and 72 h. One hour before the viability measurements at 24 h and 72 h, the culture media was replaced with 350 µl fresh media, containing 5% alamarBlue® and incubated for 1 h at 37°C. After the measurement at 24 h, the discs were washed with PBS to remove alamarBlue®, and 500 µl of fresh media was added to the cell-cultured discs. The fluorescence measurements were made with 100 µl of the

32
solution in a black well plate in a Tecan Infinite M200 plate reader (570 nm excitation, 590 nm emission).

33
5. Results and discussion
5.1 Characterization of HA coating In paper I, an UTHA coating was manufactured and characterized. The thickness was in the order of 1 µm and the coating has the ability to be load-ed with pharmaceutics for increased implant fixation or antibiotics. It can also be removed without damaging the bone. The UTHA coating was manu-factured with a biomimetic coating method, i.e., the HA crystals were formed by nucleation from a PBS solution supersaturated in respect to calci-um and phosphate ions. A FIB was used to reveal the thickness of the coat-ing.
As seen in the SEM images in figure 4 the coating was approximately 1 µm thick.
Figure 4. a & b) Scanning electron micrographs of flaked hydroxyapatite. c & d) Focused ion beam cut hydroxyapatite revealing the thickness of the ultrathin hy-droxyapatite coating. Note that the images are taken at a 52° incidence angle.
The XRD spectra in figure 4 showed peaks characteristic for HA.

34
Figure 5. The X-ray diffraction patterns for UTHA, thick HA and a reference pow-der. The UTHA coating was too thin to obtain an HA XRD signal. Therefore a thick HA coating was also manufactured by soaking in PBS for 9 days instead of the 3 days for the UTHA coating.
Energy dispersive X-ray spectroscopy showed a Ca/P ratio of the UTHA coating of 1.68 ± 0.15 which is very close to the theoretical value of 1.67. Precipitated powder filtered from the PBS solution showed a Ca/P ratio of 2.03 ± 0.25.
As seen from the FTIR spectra in figure 6, only the precipitated powder displayed an OH peak, PO4 peaks were observed with all specimens.

35
Figure 6. The FTIR spectra of the UTHA coating, a thick HA coating on CP-Ti discs, and precipitated powder filtered from the PBS soaking solution after three days. Hydroxyl groups are clearly observed for the precipitated powder and phos-phate groups are observed for all three specimens.
A scratch test was performed to measure the adhesion of the HA coating to the implant. The HA coating was smeared out and flattened which indicates that the adhesion to the implant was stronger than the cohesive forces within the coating, see figure 7.

36
Figure 7. Scanning electron micrograph of the UTHA coating after scratch tested by an alumina sphere. Smearing and flattening can be seen.
A Rockwell indentation test was also performed to test the adhesion of the UTHA coating. As can be seen in figure 8 a, no damage was made to the coating at or near the indentation crater which indicates good adhesion. Scanning electron microscopy examination revealed a similar flattening of the coating as was observed with scratch testing, see figure 8 b.
Figure 8. a) Optical image of a Rockwell indentation on UTHA coating, b) scanning electron micrograph of an edge of an indentation.
The SEM images of screw insertion in polyurethane foam, displayed in fig-ure 9, showed no detachment of the coating from the threads. This result additionally supports the strong adhesion displayed in the Rockwell and scratch tests.

37
Figure 9. Scanning electron micrographs of the thread of a UTHA coated cancellous screw after insertion in polyurethane foam previously soaked in PBS at 37°C.
5.2 Bioactivity Titanium has a thin native oxide layer. By soaking in 30% H2O2 this layer can be made thicker and O2
-• can be trapped in the amorphous oxide. When implanted in the body, this layer can slowly leak out H2O2 which reduces the

38
risk for infections. If the patient has impeded bone quality, for example oste-oporosis, the osseointegration needs to be enhanced by soaking in alkali ions to yield a bioactive surface.
In paper II the oxide surface was sequentially soaked in NaOH and Ca(OH)2 for 15 min each and, as can be seen in figure 11, yielded a hydrox-yapatite layer when subsequently soaked in PBS for 7 days. Soaking in NaOH, with treatment times of 24 h and subsequent heat treatment is a common procedure to acquire crystalline sodium titanate [19]. Forsgren et al. performed a much shorter NaOH soaking of only 10 min on an anodized titanium surface and still managed to precipitate hydroxyapatite on the sur-face when subsequently soaking the sample in PBS [89]. This anodized tita-nium had a thick titanium oxide layer and therefore it was assumed that it would be possible to acquire the same bioactivity with similarly short soak-ing times also with a titania layer formed from H2O2 soaking. Furthermore, Ca2+ ions have been shown to additionally increase the bioactivity by its double positive charge, which increases the ionic activity potential of the PBS solution more than Na+ ions do [95]. The applications for this bioactive and antibacterial layer are mainly dental implants, spinal cages and bone screws [19].
Figure 10 shows the amorphous sodium and calcium titanate layers on top of the H2O2 oxidized layer. There is a clear trend that the coverage of the layer increases with Ca2+ and heat treatment and heat and pressure (autoclav-ing).

39
Figure 10. Scanning electron micrographs of CP-Ti discs after the different treat-ments. a) Ti_Control, b) Ti_H2O2, c) Ti25, d) Ti25_Ca, e) Ti200, f) Ti200_Ca, g) TiAuto, h) TiAuto_Ca.
In figure 11, the XRD patterns show the strongest HA peak for TiAuto_Ca, and there is a clear trend that Ca2+ and heat treatment/autoclaving promote bioactivity.

40
Figure 11. The X-ray diffractograms of the test groups and Ti_Control after soaking in PBS for 7 days. A reference diffractogram is included to show the HA peaks. Dot (•) denotes Ti peaks.
When soaked in whole human blood and incubated for 1 h at 37°C, the mod-ified titanium discs Ti_Ca and Ti_H2O2 displayed coagulation and adhesion of blood to the surface that was similar to the Ti control surface as can be seen from the SEM images in figure 12. The polyvinyl chloride (PVC) sur-face that functioned as a negative control exhibited distinctly less adhesion and coagulation. As displayed in figure 13, the platelet aggregation, coagula-tion and complement activation were similar for the modified surfaces and the Ti control, which displayed a significant increase compared to the initial value. The PVC surface demonstrated a significant increase in complement activation, but no coagulation activation which resulted in the absence of platelet activation.

41
Figure 12. Scanning electron micrographs of the test surfaces after incuba-tion in whole blood for 1 h at 37°C. a & b) Ti_Ca, c & d) Ti_H2O2, e & f) Ti, g & h) PVC. The panel to the right shows a magnification of the framed area to the left. The titanium surfaces showed similar amount of adhered blood cells in contrast to the PVC surface which displayed very limited adhesion.

42
Figure 13. Amount of cells or proteins left after 1.4 ml blood comprising 0.50 IU heparin/ml was incubated in PVC wells with the test or control specimens on top and rotated for 60 min at 37°C. a) Platelets as percentage of value in blood before incubation, b) amount thrombin-antithrombin (TAT) µg/L, c) amount C3a µg/L, d) amount terminal complement complex (TCC) AU/mL. (*p <0.05, **p < 0.01; ANOVA with Tukey multiple comparison test)
5.3 Antibacterial effect To assess the antibacterial effect of the modified surfaces, a direct contact test and a biofilm inhibition test were performed with S. epidermidis Xen 43, which is a bioluminescent strain. The bacterial growth was assessed with a luminescence spectrometer. As can be seen in figure 14, bacterial cells on TiAuto_Ca and Ti_H2O2 exhibited a 70% and 93%, respectively, decrease in bacterial viability compared to bacterial cells on Ti_Control, in the direct contact test. The biofilm inhibition test yielded a 65% and 83% decrease in bacterial viability for biofilms grown on TiAuto_Ca and Ti_H2O2, respec-tively, compared to Ti_Control.

43
Figure 14. Antibacterial assessment showing the luminescence of the biolumines-cent strain S. epidermidis Xen 43 on sample discs, corresponding to the bacterial viability. a) After a 45 min direct contact test, b) after 5 h of incubation following the 45 min direct contact test. Different letters denotes statistically significant differ-ence (one-way ANOVA, Tukey post hoc, p < 0.05). c) Biofilm inhibition during 9 h, d) biofilm inhibition after 6 h incubation (one-way ANOVA, Tukey post hoc, p < 0.05).
In paper IV we monitored the ROS generation to find the optimal parame-ters with regards to TiO2 particle type, H2O2 concentration and energy (wavelength) of irradiated light. The optimal parameters were used in paper V for debridement of bacterial biofilms. Figure 15 shows that TiO2 particles and light irradiation of 365 and 405 nm, had a large positive influence on the ROS generation.

44
Figure 15. Degradation of RhB after 10 min irradiation with light of 365, 405 and 470 nm wavelength, or in darkness, for solutions of 0 or 0.5 g/l TiO2 and 0 or 1.9 M H2O2. Error bars denotes standard deviation for three measurements. Groups with different letters are significantly different at p < 0.05 within the same H2O2 and TiO2 concentration. Groups with different numbers are significantly different at p < 0.05 within the same irradiation wavelength.
The RhB experiments displayed in figure 16 and 17 confirmed the increase in ROS generation of rutile in combination with H2O2 at concentrations be-tween 1 and 3.5 mM. At H2O2 concentrations of 19.6 mM and higher, the organic degradation was decreased because H2O2 reacts with •OH, forming the less reactive HO2• according to equation 12.
H2O2 + •OH → H2O + HO2• (12)

45
Figure 16. Degradation potential of four TiO2 particle types, measured by the degra-dation of RhB after 10 min irradiation with light of 365 nm wavelength. Different letters denotes significant difference within the same particle type and different numbers denotes significant difference within the same H2O2 concentration at p < 0.05.

46
Figure 17. Degradation potential of four TiO2 particle types, measured by the degra-dation of RhB after 10 min irradiation with light of 405 nm wavelength. Different letters denote significant difference within the same particle type and different num-bers denote significant difference within the same H2O2 concentration at p < 0.05.
In paper V we used as a starting point the results from paper IV which showed that rutile combined with 2 mM of H2O2 generated the highest amount of ROS. We also included 0.95 M H2O2 because it has been shown in earlier studies to be effective against bacteria and is part of a common treatment against peri-implantitis [52]. The results in paper V showed that 0.95 M was the most effective parameter against both S. epidermidis Xen 43 and P. aeruginosa. Particles only produced an additional effect in one of the experiments, the luminescence experiment with S. epidermidis Xen 43, as shown in figure 18. Light irradiation did not show any statistically signifi-cant extra effect at the p < 0.05 level. As can be seen in figure 19, the posi-tive control (Ethanol) did not remove the bacterial biofilm but merely killed the bacteria.

47
Figure 18. Regrowth of S. epidermidis Xen 43 after decontamination treatment. A) Luminescence intensity during 18 h incubation for 4 test groups, positive (Ethanol) and negative (PBS) control. B) Time to reach a luminescence intensity of 2 000 for 3 test groups and Ethanol. (PBS and R_Low_Li reached an intensity of 2 000 before the first measurement after 8 h, and were thereby excluded). Groups with different letters are significantly different at p < 0.05.
Figure 19. Scanning electron micrographs of S. epidermidis Xen 43 on discs after decontamination treatments of the 4 test groups, positive (Ethanol) and negative (PBS) control.
The MAA with S. epidermidis, as showed in figure 20, indicated that R_Hi_Li was the most effective debridement treatment. As can be seen in figure 21, due to the poor adhesion of the S. epidermidis biofilm, a large portion of the biofilm was removed already at the washing step, which could contribute to the large variability in the recorded data.

48
Figure 20. Regrowth of S. epidermidis Xen 43 after decontamination treatments. A) Fluorescence during 6 h incubation for 4 test groups and positive (Ethanol) and negative (PBS) control. B) Fluorescence after 3 h incubation, different letters indi-cate significant difference (p < 0.05). Groups with an asterisk are significantly dif-ferent (p < 0.05), from the negative control (PBS).
Figure 21. Scanning electron micrographs of S. epidermidis Xen 43 on discs after decontamination treatments of the 4 test groups, positive (Ethanol) and negative (PBS) control.
The MAA with P. aeruginosa indicated that the debridement treatments comprising 3% H2O2 were the most effective (figure 22). Figure 23 shows that a substantial amount of rutile particles are left after the debridement treatment.

49
Figure 22. Regrowth of P. aeruginosa after decontamination treatment. A) Fluores-cence during 6 h incubation for 4 test groups and positive (Ethanol) and negative (PBS) control. B) Fluorescence after 6 h incubation, different letters indicate signifi-cant difference and asterisk indicate significant difference from PBS, both at p < 0.05.
Figure 23. Scanning electron micrographs of P. aeruginosa on discs after decontam-ination treatments of the 4 test groups, positive (Ethanol) and negative (PBS) con-trol.
The effective removal of biofilms with 3% H2O2 is also supported by the literature [83–85]. A study by Kim et al. [58], used rutile particles under 405 nm irradiation and managed to obtain a 4-log reduction after 20 min. In that study the particles were immersed in the biofilm, enabling the generated radicals to disrupt the biofilm. Visible light on its own, has been shown to be bactericidal against P. aeruginosa and S. aureus [96], and to be able to re-duce biofilms of Listeria monocytogenes [97], and Streptococcus mutans [98].

50
The results of the different cleaning solutions in paper V, where 3% H2O2 exhibited the strongest antibacterial effect were not unexpected con-sidering the ability of H2O2 to penetrate the EPS of bacterial biofilms. How-ever considering the strong ROS generation of rutile combined with 2 mM of H2O2 seen in paper IV, a stronger effect with these cleaning parameters was expected. The weak effect on the biofilm with these cleaning parameters can be explained by the short lifetime of •OH, which likely only resulted in oxidation of the bacteria directly in contact with the catalyst. In the RhB degradation study in paper IV, the RhB dye adhered to the surface, thus enabling the short lived radicals to oxidize the dye and thus perhaps overes-timating the antibacterial effect one could expect on a biofilm.
A limitation in this study was that the adhesion of the biofilm was rela-tively weak and thus a significant portion of the biofilm was detached just through washing by pipetting.
Another limitation with this experiment was that the radical generation is limited to the close proximity of the particle surface. In the bacteria studies in paper V it is likely that very few of the particles came in close contact with the biofilm so that they would be able to oxidize the biofilm. In an ap-plication where the particles and H2O2 are incorporated or mixed in a hydro-gel, the effect might be better if the hydrogel is applied in a very thin layer. This would enable the particles to be in close contact with the bacterial bio-film, thereby facilitating oxidation of the EPS by •OH. Both the surface of the particles and the surface of the bacterial biofilm are negatively charged which further complicates a close contact between particles and biofilm.
5.4 Biocompatibility
The Ti_H2O2 surfaces were toxic against both cell types because the cells had a proliferation of less than 70 % compared to the control at both time points, as can be seen in figure 24. The Ti_CaAuto surfaces elicited a de-crease in proliferation on HDF cells after 72 h, but further studies need to be performed to evaluate if the proliferation is statistically significantly below the cytotoxicity level, which is 70% of the control specimen [99].

51
Figure 24. Viability assessment of human dermal fibroblast and MC3T3 pre-osteoblasts on surface modified titanium discs after 24 h and 72 h incubation. The control group was a well containing no sample disc. Different letters denotes signifi-cant difference across the time points within each cell type (p < 0.05), analyzed with one-way ANOVA and Tukey post hoc (n=6).

52
6. Conclusions
The UTHA coating showed characteristics with regards to thickness, compo-sition and adhesion which make it suitable as a coating that can obtain strong fixation and with the possibility to be removed at a later point in time with-out damaging the bone. It also has excellent properties due to its porosity to be loaded with pharmaceuticals like antibiotics or bisphosphonate.
The titanium surface soaked in a sequence of solutions of H2O2, NaOH and Ca(OH)2 with subsequent autoclaving, showed bioactivity by exhibiting apatite formation on the surface after soaking in PBS for 7 days at 37°C as displayed by XRD.
The surface also induced a platelet, coagulation and complement activa-tion similar to non-modified titanium surfaces. This further supports the bioactive properties of the surface.
Furthermore, it displayed a 70% and 65% decrease in bacterial viability of S. epidermidis Xen 43 on a direct contact test and biofilm inhibition test respectively. In biocompatibility testing, MC3T3 cells proliferated at the same rate as the control while human dermal fibroblasts decreased with 28% compared to the control after 72 h incubation, so further testing is required to more definitely ascertain biocompatibility.
A mixture of rutile particles and 2 mM H2O2 produced a 77% RhB degra-dation after 10 min of 405 nm light irradiation, which suggested a possibly effective cleaning or debridement protocol for dental applications using light irradiation not harmful to sensitive tissues. However, the low concentration of H2O2 was however not as successful against bacterial biofilms of S. epi-dermidis Xen 43 and P. aeruginosa where instead 3% H2O2 displayed the best effect with little or no enhancement with the addition of TiO2 particles or light irradiation.

53
7. Future work
The adhesion of the putative calcium titanate layer on the surface modified discs should be examined in further studies as should the amount of H2O2 or other ROS released from the surface. A future step in the development of this implant surface is to perform an in vivo study. Screws with this modified titanium surface could be implanted in an animal model such as a rat model to evaluate if the bioactivity and antibacterial effect also is present in vivo.
In paper V, 3 % H2O2 was shown to be the most effective debridement solution. However, there were several limitations in this study such as non-ideal attachment of the biofilm. Therefore it would be interesting to grow the biofilm in a bioreactor during a longer time to ensure a more representative and well attached biofilm. This may reveal if the •OH created by rutile and low concentrations of H2O2 are able to remove the biofilm or kill the bacteria within the biofilm.

54
8. Svensk sammanfattning
Titan är ett av de vanligaste materialen i medicinska implantat för personer som skadat leder eller blivit av med tänder. Implantaten ger en bra minsk-ning av smärta och ökad rörelsefunktion. Titan existerar i olika faser, α och β, eller i en kombination av de bägge faserna, α + β. Alfa-fas används i tan-dimplantat, medan α + β eller β-fas används i ortopediska implantat. Anled-ningen till att just titan är så vanlig som implantatmaterial är att det är bio-kompatibelt och att det har bra mekaniska egenskaper. Framför allt har titan en elasticitet som är nära bens elasticitet och styrkan i förhållande till densi-teten är hög.
Bioaktivitet definieras som förmågan hos ett material eller en medicin att interagera med kroppen. Ett bioaktivt implantat har förmågan att bilda en kemisk bindning mellan implantatytan och benvävnaden. Normalt sett skap-ar titanimplantat en bra fixering till ben, men hos äldre patienter, diabetespa-tienter eller andra med nedsatt bentäthet kan implantatets förmåga att binda till ben behöva förbättras.
I den första delen av avhandlingen genomfördes en karakterisering av en ca 1 µm tjock, porös hydroxyapatitbeläggning. Beläggningen formades bio-mimetiskt på benskruvar av titan, genom doppning i en minerallösning med liknande sammansättning som mänskligt blodplasma. Syftet med denna be-läggning är kunna ladda den med antibiotika och läkemedel för att minska infektionsrisken och öka beninbindningen. Det som oftast är avgörande för hur framgångsrik en implantatbeläggning blir, är hur bra beläggningen håller ihop och hur hårt den fäster till substratytan. Vi såg att vi fick en bra täck-ning av hela ytan och att förhållandet mellan kalcium och fosfor på hydroxy-apatiten var nära den optimala på 1.67. Röntgendiffraktion visade att be-läggningen var kristallin och reptest samt Rockwellindentation visade en bra adhesion till den underliggande titanytan. Ett vanligt problem med implantat är att det kan uppstå infektioner. För att undvika att infektioner inträffar kan implantatytan beläggas med antibakteri-ella medel. Vi etsade titandiskar av grad 2 med väteperoxid (H2O2) för att öka tjockleken på det mycket tunna naturliga oxidlagret som finns på titan. Det bildades då ett amorft lager av titanperoxidkomplex som har visat sig kunna släppa ut H2O2 när det långsamt degraderas under förhållanden lik-nande de som finns i kroppen. Detta lager kan också användas till att ladda natrium- och kalciumjoner i, för att skapa en superhydrofil yta som är bioak-tiv och kemiskt kan binda till ben.

55
Studien visade att en yta med H2O2, natrium och kalcium samt autoklave-rad under 125 °C, uppvisade bioaktivitet in vitro genom att kristallisera hyd-roxyapatit på ytan vid doppning i PBS. Den visade också antibakteriell för-måga mot S. epidermidis Xen 43 vid ett direktkontakttest och biofilminhibe-ringstest. Cytotoxicitetstest visade ingen cytotoxisk effekt mot MC3T3 pre-osteoblaster, mot mänskliga hudfibroblaster var spridningen ganska stor och fler test behöver göras för att klargöra om cytotoxisk effekt föreligger eller inte.
För att mäta hur väl ytan kan växa in i ben mättes även trombocytinbind-ning, koagulations- och komplementaktivering till ytan efter att ha inku-berats i människoblod från friska donatorer. Trombocyter som blir aktive-rade vid ytan skickar ut tillväxtfaktorer som aktiverar bengenerering, aktive-ringen sker med hjälp av det intrinsiska koagulationssystemet och komple-mentsystemet. Vi såg en signifikant ökning av trombocytinbindning, koagulations- och komplementaktivering vilket styrker att den modifierade ytan har en god bioaktivitet.
Periimplantit har ökat drastiskt de senaste åren pga. ökat antal tan-dimplantat. Periimplantit innebär att tandköttet runt implantatet blir inflam-merat och att käkbenet där implantatet är förankrat tappar kontakt med im-plantatet. Det bildas plack på implantatet som består av bakterier inneslutna i ett skyddande polysackaridlager, en s.k. biofilm. Denna biofilm måste av-lägsnas om benet ska kunna integreras mot implantatytan igen. I dagsläget används bl.a. natriumhypoklorit, klorhexidin och H2O2 som kemiska dekon-tamineringsmetoder och de kompletteras ofta med mekaniska metoder som borstar och kuretter. Problemet med de här metoderna är att de inte alltid ger ett tillräckligt bra resultat och kan skada implantatytan, vilket försvårar åter-integration. Reaktiva syreföreningar (RSF), är molekyler som är mycket reaktiva. De saknar en parad elektron vilket gör att de väldigt lätt drar till sig elektroner från andra molekyler t.ex. lipider som finns i cellens väggar. Detta gör att de kan vara väldigt effektiva på att eliminera bakterier utan att riskera att bakterierna blir resistenta mot dem. Genom att belysa titandioxidpartiklar (TiO2-partiklar), som är halvledare, kan man generera en stor mängd RSF. I kombination med H2O2 som själv är en RSF kan den fotokatalytiska effekten ökas ytterligare.
Detta arbete visade genom mätning av degraderad rhodamin B, att TiO2 av kristallfasen rutil tillsammans med låga koncentrationer H2O2 (1-3.5 mM) och belysning med ljus av 365 eller 405 nm våglängd, genererade betydligt fler RSF än andra kombinationer. I test med bakteriearterna S. epidermidis Xen 43 och P. aeruginosa i biofilm växt på titandiskar av grad 2, visade sig 0.9 M H2O2 vara mest effektivt för dekontaminering. Vi såg delvis en viss ytterligare förbättring med TiO2-partiklar, medan ljusbelysning inte gav nå-gon ytterligare dekontaminerande effekt.

56
9. Acknowledgement
There are many people during the years of my PhD study here at Uppsala University that I would like to thank. First I want to thank my main supervi-sor Ken, your support in planning and analyzing experiments as well as cor-recting manuscripts has been invaluable. I am grateful to have been able to receive your experience and knowledge. My assistant supervisor and boss Håkan, thank you for having the patience and believing in me. I want to thank Maria for introducing me to Håkan and the project and for being a fantastic co-writer. Philip, who initially was my assistant supervisor and later co-author for sharing your great knowledge and company.
Gry, for great collaboration in the whole blood study. Erik, for helping me out in the beginning of my PhD project. Shiuli and Marjam, for helping me understand cell tests. Satwik, for help with cell tests and bacteria tests. Alejandro, for keeping the lab in great order and collaboration with experi-ments. Lee, for interesting discussions about bacteria. Camilla, Amina and Susanne for donating blood to the whole blood study. David, for being a nice office mate. Also I want to thank my old office mates Petra, Pontus and Ishtiaq. I want to thank all the present and old members of the MiM group: Luimar, Anna, Le, Jun, Torbjörn, Cecilila, Michael, Celine, Charlotte, Dan, Wei, Caroline, Ingrid, Song, Maria, Marjam, Johanna, Mirjam, Bing, Tao, Yixiao, Ernesto, The Tribogroup and Elmingroup and MST group. Also the Nanogroup for letting me use their lab.
I want to thank Stenbjörn for bringing me to Uppsala University by hiring me as a summer worker in the molecular biomimetics group 2013. Patricia and the rest of the molecular biomimetics group that prepared me for the PhD studies and introduced me to Uppsala. David, Håvard, Hanna, Manuel and all the other in Oslo University, thanks for nice company during conferences and during my visits in Oslo.
Jaan, for sharing your knowledge about blood, coagulation and comple-ment system. Jonatan, for help with computer problems. Ingrid, Sara and Maria for help with administrative tasks. Joakim in the workshop, for ar-ranging with titanium discs. Jan-Åke and Victoria and the other in the clean-room staff. Uddeholms resestipendium and ScSB travel grant for economic support for traveling to conferences. Finally, thanks to my parents who sup-port me in everything I do.

57
10. References
[1] C.M. Abraham, A Brief Historical Perspective on Dental Implants, Their Surface Coatings and Treatments, Open Dent. J. 8 (2014) 50–55. doi:10.2174/1874210601408010050.
[2] R.A. Brand, Sir William Arbuthnot Lane, 1856–1943, Clin. Orthop. Relat. Res. 467 (2009) 1939–1943. doi:10.1007/s11999-009-0861-3.
[3] M.N. Smith-Petersen, Evolution of Mould Arthroplasty of the Hip Joint, J Bone Jt. Surg Br. 30–B (1948) 59–75.
doi:10.1097/01.blo.0000246557.19973.43. [4] P.I. Brånemark, B.O. Hansson, R. Adell, U. Breine, J. Lindström, O. Hallén,
A. Ohman, Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period, Scand. J. Plast. Reconstr. Surg. Suppl. (1977).
[5] J. Derks, C. Tomasi, Peri-implant health and disease. A systematic review of current epidemiology, J. Clin. Periodontol. 42 (2015) S158–S171. doi:10.1111/jcpe.12334.
[6] T.S. Hip, A. Register, Any Health Problems You Wish To Declare?, 2016. doi:10.18158/SJy6jKyrM.
[7] D.M. Brunette, P. Tengvall, M. Textor, P. Thomsen, Titanium in Medicine, Springer Berlin Heidelberg, Berlin, Heidelberg, 2001. doi:10.1007/978-3-642-56486-4.
[8] M. Geetha, A.K. Singh, R. Asokamani, A.K. Gogia, Ti based biomaterials, the ultimate choice for orthopaedic implants – A review, Prog. Mater. Sci. 54 (2009) 397–425. doi:10.1016/j.pmatsci.2008.06.004.
[9] T. Albrektsson, P.-I. Brånemark, H.-A. Hansson, J. Lindström, Osseointegrated Titanium Implants : Requirements for Ensuring a Long-Lasting, Direct Bone-to-Implant Anchorage in Man T., Direct. 6470 (1981) 155–170. doi:10.3109/17453678108991776.
[10] Donachie MJ Jr, Titanium: A technical guide, 1988. [11] S.G. Steinemann, Titanium - The material of choice?, Periodontol. 2000. 17
(1998) 7–21. doi:10.1111/j.1600-0757.1998.tb00119.x. [12] R. Trindade, T. Albrektsson, P. Tengvall, A. Wennerberg, Foreign Body
Reaction to Biomaterials: On Mechanisms for Buildup and Breakdown of Osseointegration, Clin. Implant Dent. Relat. Res. 18 (2016) 192–203. doi:10.1111/cid.12274.
[13] H. Terheyden, N.P. Lang, S. Bierbaum, B. Stadlinger, Osseointegration - communication of cells, Clin. Oral Implants Res. 23 (2012) 1127–1135. doi:10.1111/j.1600-0501.2011.02327.x.
[14] J.R. Jones, Reprint of: Review of bioactive glass: From Hench to hybrids, Acta Biomater. 23 (2015) S53–S82. doi:10.1016/j.actbio.2015.07.019.
[15] T. Kokubo, Formation of biologically active bone-like apatite on metals and polymers by a biomimetic process, Thermochim. Acta. 280–281 (1996) 479–490. doi:10.1016/0040-6031(95)02784-X.

58
[16] H.-M. Kim, F. Miyaji, T. Kokubo, T. Nakamura, Preparation of bioactive Ti and its alloys via simple chemical surface treatment, J. Biomed. Mater. Res. 32 (1996) 409–417. doi:10.1002/(SICI)1097-4636(199611)32:3<409::AID-JBM14>3.0.CO;2-B.
[17] M. Bohner, J. Lemaitre, Can bioactivity be tested in vitro with SBF solution?, Biomaterials. 30 (2009) 2175–2179. doi:10.1016/j.biomaterials.2009.01.008.
[18] T. Kokubo, H. Takadama, How useful is SBF in predicting in vivo bone bioactivity?, Biomaterials. 27 (2006) 2907–15.
doi:10.1016/j.biomaterials.2006.01.017. [19] T. Kokubo, H.M. Kim, M. Kawashita, T. Nakamura, Bioactive metals:
Preparation and properties, J. Mater. Sci. Mater. Med. 15 (2004) 99–107. doi:10.1023/B:JMSM.0000011809.36275.0c.
[20] S. Tugulu, K. Löwe, D. Scharnweber, F. Schlottig, Preparation of superhydrophilic microrough titanium implant surfaces by alkali treatment, J. Mater. Sci. Mater. Med. 21 (2010) 2751–2763. doi:10.1007/s10856-010-4138-x.
[21] N. Sykaras, a M. Iacopino, V. a Marker, R.G. Triplett, R.D. Woody, Implant materials, designs, and surface topographies: their effect on osseointegration. A literature review., Int. J. Oral Maxillofac. Implants. 15 (2000) 675–690.
[22] J.E. Davies, N. Baldan, Scanning electron microscopy of the bone-bioactive implant interface, J. Biomed. Mater. Res. 36 (1997) 429–440. doi:10.1002/(SICI)1097-4636(19970915)36:4<429::AID-JBM1>3.0.CO;2-G.
[23] R. Sawada, K. Kono, K. Isama, Y. Haishima, A. Matsuoka, Calcium-incorporated titanium surfaces influence the osteogenic differentiation of human mesenchymal stem cells, J. Biomed. Mater. Res. - Part A. 101 A (2013) 2573–2585. doi:10.1002/jbm.a.34566.
[24] J. Hong, J. Andersson, K. Nilsson Ekdahl, G. Elgue, N. Axén, R. Larsson, B. Nilsson, Titanium Is a Highly Thrombogenic Biomaterial: Possible Implications for Osteogenesis, Thromb. Haemost. 82 (1999) 58–64. doi:10.1055/s-0037-1614630.
[25] S. Sobieszczyk, Surface modifications of ti and its alloys, Adv. Mater. Sci. 10 (2010) 29–42. doi:10.2478/v10077-010-0003-3.
[26] A. Gristina, H.H. Sherk, The Classic: Biomaterial-Centered Infection, Clin. Orthop. Relat. Res. 427 (2004) 4–12.
doi:10.1097/01.blo.0000145156.89115.12. [27] W. Xia, C. Lindahl, J. Lausmaa, H. Engqvist, Biomimetic hydroxyapatite
deposition on titanium oxide surfaces for biomedical application, Adv. Biomimetics. (2011) 429–452. doi:10.5772/574.
[28] L. Sun, C.C. Berndt, K.A. Gross, A. Kucuk, Material fundamentals and clinical performance of plasma-sprayed hydroxyapatite coatings: A review, J. Biomed. Mater. Res. 58 (2001) 570–592. doi:10.1002/jbm.1056.
[29] P. Habibovic, F. Barrere, Biomimetic hydroxyapatite coating on metal implants, J. Am. Ceram. Soc. 85 (2002) 517–522. doi:10.1111/j.1151-2916.2002.tb00126.x.
[30] S. Leeuwenburgh, P. Layrolle, F. Barrre, J. De Bruijn, J. Schoonman, C.A. Van Blitterswijk, K. De Groot, Osteoclastic resorption of biomimetic calcium phosphate coatings in vitro, J. Biomed. Mater. Res. 56 (2001) 208–215. doi:10.1002/1097-4636(200108)56:2<208::AID-JBM1085>3.0.CO;2-R.
[31] H.B. Wen, J.G.C. Wolke, J.R. de Wijn, Q. Liu, F.Z. Cui, K. de Groot, Fast precipitation of calcium phosphate layers on titanium induced by simple chemical treatments, Biomaterials. 18 (1997) 1471–1478.
doi:10.1016/S0142-9612(97)82297-1.

59
[32] H.T. Shiu, P.C. Leung, C.H. Ko, The roles of cellular and molecular components of a hematoma at early stage of bone healing, J. Tissue Eng. Regen. Med. 12 (2018) e1911–e1925. doi:10.1002/term.2622.
[33] C. Ehrnthaller, M. Huber-Lang, P. Nilsson, R. Bindl, S. Redeker, S. Recknagel, A. Rapp, T. Mollnes, M. Amling, F. Gebhard, A. Ignatius, Complement C3 and C5 deficiency affects fracture healing, PLoS One. 8 (2013) 1–15. doi:10.1371/journal.pone.0081341.
[34] L. Hall-Stoodley, J.W. Costerton, P. Stoodley, Bacterial biofilms: From the natural environment to infectious diseases, Nat. Rev. Microbiol. 2 (2004) 95–108. doi:10.1038/nrmicro821.
[35] H.C. Flemming, J. Wingender, The biofilm matrix, Nat. Rev. Microbiol. 8 (2010) 623–633. doi:10.1038/nrmicro2415.
[36] A. Corbin, B. Pitts, A. Parker, P.S. Stewart, Antimicrobial penetration and efficacy in an in vitro oral biofilm model, Antimicrob. Agents Chemother. 55 (2011) 3338–3344. doi:10.1128/AAC.00206-11.
[37] R. Briandet, J.M. Herry, M.N. Bellon-Fontaine, Determination of the van der Waals, electron donor and electron acceptor surface tension components of static Gram-positive microbial biofilms, Colloids Surfaces B Biointerfaces. 21 (2001) 299–310. doi:10.1016/S0927-7765(00)00213-7.
[38] H. Takahashi, T. Suda, Y. Tanaka, B. Kimura, Cellular hydrophobicity of Listeria monocytogenes involves initial attachment and biofilm formation on the surface of polyvinyl chloride, Lett. Appl. Microbiol. 50 (2010) 618–625. doi:10.1111/j.1472-765X.2010.02842.x.
[39] M.D. Macià, E. Rojo-Molinero, A. Oliver, Antimicrobial susceptibility testing in biofilm-growing bacteria, Clin. Microbiol. Infect. 20 (2014) 981–990. doi:10.1111/1469-0691.12651.
[40] J.D. Chambless, S.M. Hunt, P.S. Stewart, A three-dimensional computer model of four hypothetical mechanisms protecting biofilms from antimicrobials, Appl. Environ. Microbiol. 72 (2006) 2005–2013. doi:10.1128/AEM.72.3.2005-2013.2006.
[41] J.B. Kaplan, Biofilm Dispersal: Mechanisms, Clinical Implications, and Potential Therapeutic Uses, J. Dent. Res. 89 (2010) 205–218.
doi:10.1177/0022034509359403. [42] M. Basavaraju, V.S. Sisnity, R. Palaparthy, P.K. Addanki, Quorum
quenching: Signal jamming in dental plaque biofilms, J. Dent. Sci. 11 (2016) 349–352. doi:10.1016/j.jds.2016.02.002.
[43] W. Zimmerli, A. Trampuz, P.E. Ochsner, Prosthetic-Joint Infections, N. Engl. J. Med. 351 (2004) 1645–1654. doi:10.1056/NEJMra040181.
[44] Y. Sakuragi, R. Kolter, Quorum-sensing regulation of the biofilm matrix genes (pel) of Pseudomonas aeruginosa, J. Bacteriol. 189 (2007) 5383–5386. doi:10.1128/JB.00137-07.
[45] T. Coenye, H.J. Nelis, In vitro and in vivo model systems to study microbial biofilm formation, J. Microbiol. Methods. 83 (2010) 89–105.
doi:10.1016/j.mimet.2010.08.018. [46] J.D. Bryers, Medical biofilms, Biotechnol. Bioeng. 100 (2008) 1–18.
doi:10.1002/bit.21838. [47] M.S. Terpenning, G.W. Taylor, D.E. Lopatin, C.K. Kerr, B. Liza Dominguez,
W.J. Loesche, Aspiration pneumonia: Dental and oral risk factors in an older veteran population, J. Am. Geriatr. Soc. 49 (2001) 557–563.
doi:10.1046/j.1532-5415.2001.49113.x.

60
[48] G.W. Taylor, Bidirectional Interrelationships Between Diabetes and Periodontal Diseases: An Epidemiologic Perspective, Ann. Periodontol. 6 (2001) 99–112. doi:10.1902/annals.2001.6.1.99.
[49] D. Campoccia, L. Montanaro, C.R. Arciola, A review of the biomaterials technologies for infection-resistant surfaces, Biomaterials. 34 (2013) 8533–8554. doi:10.1016/j.biomaterials.2013.07.089.
[50] L. Zhao, P.K. Chu, Y. Zhang, Z. Wu, Antibacterial coatings on titanium implants, J. Biomed. Mater. Res. - Part B Appl. Biomater. 91 (2009) 470–480. doi:10.1002/jbm.b.31463.
[51] R. Bürgers, C. Witecy, S. Hahnel, M. Gosau, The effect of various topical peri-implantitis antiseptics on Staphylococcus epidermidis, Candida albicans, and Streptococcus sanguinis, Arch. Oral Biol. 57 (2012) 940–947. doi:10.1016/j.archoralbio.2012.01.015.
[52] M. Gosau, S. Hahnel, F. Schwarz, T. Gerlach, T.E. Reichert, R. Bürgers, Effect of six different peri-implantitis disinfection methods on in vivo human oral biofilm, Clin. Oral Implants Res. 21 (2010) 866–872.
doi:10.1111/j.1600-0501.2009.01908.x. [53] S. Petter Lyngstadaas Håvard J. Haugen, US 2013/0115248 A1, (2013). [54] Y. Kakuma, A.Y. Nosaka, Y. Nosaka, Difference in TiO2 photocatalytic
mechanism between rutile and anatase studied by the detection of active oxygen and surface species in water, Phys. Chem. Chem. Phys. 17 (2015) 18691–18698. doi:10.1039/C5CP02004B.
[55] T. Hirakawa, K. Yawata, Y. Nosaka, Photocatalytic reactivity for O2•− and
OH• radical formation in anatase and rutile TiO2 suspension as the effect of H2O2 addition, Appl. Catal. A Gen. 325 (2007) 105–111.
doi:10.1016/j.apcata.2007.03.015. [56] J. Zhang, Y. Nosaka, Mechanism of the OH Radical Generation in
Photocatalysis with TiO2 of Different Crystalline Types, J. Phys. Chem. C. 118 (2014) 10824−10832. doi:10.1021/jp501214m.
[57] G. Rajagopal, S. Maruthamuthu, S. Mohanan, N. Palaniswamy, Biocidal effects of photocatalytic semiconductor TiO2, Colloids Surfaces B Biointerfaces. 51 (2006) 107–111. doi:10.1016/j.colsurfb.2006.06.003.
[58] C.H. Kim, E.S. Lee, S.M. Kang, E. de Josselin de Jong, B. Il Kim, Bactericidal effect of the photocatalystic reaction of titanium dioxide using visible wavelengths on Streptococcus mutans biofilm, Photodiagnosis Photodyn. Ther. 18 (2017) 279–283. doi:10.1016/j.pdpdt.2017.03.015.
[59] K. Sunada, Y. Kikuchi, K. Hashimoto, A. Fujishima, Bactericidal and detoxification effects of TiO2 thin film photocatalysts, Environ. Sci. Technol. 32 (1998) 726–728. doi:10.1021/es970860o.
[60] K. Hirakawa, M. Mori, M. Yoshida, S. Oikawa, S. Kawanishi, Photo-irradiated titanium dioxide catalyzes site specific DNA damage via generation of hydrogen peroxide, Free Radic. Res. 38 (2004) 439–447. doi:10.1080/1071576042000206487.
[61] K.S. Yao, D.Y. Wang, J.J. Yan, L.Y. Yang, W.S. Chen, Photocatalytic effects of TiO2/Fe thin film irradiated with visible light on cellular surface ultrastructure and genomic DNA of bacteria, Surf. Coatings Technol. 201 (2007) 6882–6885. doi:10.1016/j.surfcoat.2006.09.066.
[62] H.J. Busscher, H.C. Van Der Mei, G. Subbiahdoss, P.C. Jutte, J.J.A.M. Van Den Dungen, S.A.J. Zaat, M.J. Schultz, D.W. Grainger, Biomaterial-associated infection: Locating the finish line in the race for the surface, Sci. Transl. Med. 4 (2012). doi:10.1126/scitranslmed.3004528.

61
[63] P.C. Maness, S. Smolinski, D.M. Blake, Z. Huang, E.J. Wolfrum, W.A. Jacoby, Bactericidal activity of photocatalytic TiO2 reaction: Toward an understanding of its killing mechanism, Appl. Environ. Microbiol. 65 (1999) 4094–4098. doi:10.1111/j.1574-6968.1985.tb00864.x.
[64] K. Nakata, A. Fujishima, TiO2 photocatalysis: Design and applications, J. Photochem. Photobiol. C Photochem. Rev. 13 (2012) 169–189.
doi:10.1016/j.jphotochemrev.2012.06.001. [65] J.W. Seo, H. Chung, M.Y. Kim, J. Lee, I.H. Choi, J. Cheon, Development of
water-soluble single-crystalline TiO2 nanoparticles for photocatalytic cancer-cell treatment, Small. 3 (2007) 850–853. doi:10.1002/smll.200600488.
[66] Y. Cai, M. Strømme, A. Melhus, H. Engqvist, K. Welch, Photocatalytic inactivation of biofilms on bioactive dental adhesives, J. Biomed. Mater. Res. - Part B Appl. Biomater. 102 (2014) 62–67. doi:10.1002/jbm.b.32980.
[67] K. Sahel, L. Elsellami, I. Mirali, F. Dappozze, M. Bouhent, C. Guillard, Hydrogen peroxide and photocatalysis, Appl. Catal. B Environ. 188 (2016) 106–112. doi:10.1016/j.apcatb.2015.12.044.
[68] D.C. Hurum, A.G. Agrios, K. a Gray, T. Rajh, M.C. Thurnauer, Explaining the Enhanced Photocatalytic Activity of Degussa P25 Mixed-Phase TiO2 Using EPR, J. Phys. Chem. B. 107 (2003) 4545–4549.
doi:10.1021/jp0273934. [69] F. Variola, J.H. Yi, L. Richert, J.D. Wuest, F. Rosei, A. Nanci, Tailoring the
surface properties of Ti6Al4V by controlled chemical oxidation, Biomaterials. 29 (2008) 1285–1298. doi:10.1016/j.biomaterials.2007.11.040.
[70] P. Tengvall, H. Elwing, I. Lundström, Titanium gel made from metallic titanium and hydrogen peroxide, J. Colloid Interface Sci. 130 (1989) 405–413. doi:10.1016/0021-9797(89)90117-3.
[71] P. Tengvall, H. Elwing, L. Sjöqvist, I. Lundström, L.M. Bjursten, Interaction between hydrogen peroxide and titanium: a possible role in the biocompatibility of titanium, Biomaterials. 10 (1989) 118–120.
doi:10.1016/0142-9612(89)90043-4. [72] P. Tengvall, I. Lundström, L. Sjöqvist, H. Elwing, L.M. Bjursten, Titanium-
hydrogen peroxide interaction: model studies of the influence of the inflammatory response on titanium implants, Biomaterials. 10 (1989) 166–175. doi:10.1016/0142-9612(89)90019-7.
[73] P. Tengvall, B. Wälivaara, J. Westerling, I. Lundström, Stable titanium superoxide radicals in aqueous Ti-peroxy gels and Ti-peroxide solutions, J. Colloid Interface Sci. 143 (1991) 589–592. doi:10.1016/0021-9797(91)90291-F.
[74] P. Tengvall, L. Bertilsson, B. Liedberg, H. Elwing, I. Lundström, Degradation of dried Ti-peroxy gels made from metallic titanium and hydrogen peroxide, J. Colloid Interface Sci. 139 (1990) 575–580.
doi:10.1016/0021-9797(90)90131-7. [75] P. Tengvall, E.G. Hörnsten, H. Elwing, I. Lundström, Bactericidal properties
of a titanium-peroxy gel obtained from metallic titanium and hydrogen peroxide, J. Biomed. Mater. Res. 24 (1990) 319–330.
doi:10.1002/jbm.820240305. [76] P. Tengvall, I. Lundström, Physico-chemical considerations of titanium as a
biomaterial, Clin. Mater. 9 (1992) 115–134. doi:10.1016/0267-6605(92)90056-Y.
[77] S.J. Klebanoff, Myeloperoxidase: friend and foe, J. Leukoc. Biol. 77 (2005) 598–625. doi:10.1189/jlb.1204697.

62
[78] J.E. Repine, R.B. Fox, E.M. Berger, Hydrogen peroxide kills Staphylococcus aureus by reacting with staphylococcal iron to form hydroxyl radical, J. Biol. Chem. 256 (1981) 7094–7096.
[79] Y. Kikuchi, K. Sunada, T. Iyoda, K. Hashimoto, A. Fujishima, Photocatalytic bactericidal effect of TiO2 thin films: dynamic view of the active oxygen species responsible for the effect, J. Photochem. Photobiol. A Chem. 106 (1997) 51–56. doi:10.1016/S1010-6030(97)00038-5.
[80] J.A. Imlay, S.M. Chin, S. Linn, Toxic DNA damage by hydrogen peroxide through the Fenton reaction in vivo and in vitro., Science. 240 (1988) 640–642. doi:10.1126/science.2834821.
[81] J.D. Baldeck, R.E. Marquis, Targets for hydrogen-peroxide-induced damage to suspension and biofilm cells of Streptococcus mutans, Can. J. Microbiol. 54 (2008) 868–875. doi:10.1139/W08-078.
[82] E. Unosson, E.K. Tsekoura, H. Engqvist, K. Welch, Synergetic inactivation of Staphylococcus epidermidis and Streptococcus mutans in a TiO2/H2O2/UV system, Biomatter. 3 (2013) e26727. doi:10.4161/biom.26727.
[83] E. Henderson, S. Schneider, F.C. Petersen, H.J. Haugen, J.C. Wohlfahrt, K. Ekstrand, A. Ekfeldt, Chemical debridement of contaminated titanium surfaces: An in vitro study, Acta Odontol. Scand. 71 (2013) 957–964. doi:10.3109/00016357.2012.734423.
[84] E. Gustumhaugen, J. Lönn-Stensrud, A.A. Scheie, S.P. Lyngstadaas, A. Ekfeldt, S. Taxt-Lamolle, Effect of chemical and mechanical debridement techniques on bacterial re-growth on rough titanium surfaces: An in vitro study, Clin. Oral Implants Res. 25 (2014) 707–713. doi:10.1111/clr.12130.
[85] D. Wiedmer, F.C. Petersen, J. Lönn-Stensrud, H. Tiainen, Antibacterial effect of hydrogen peroxide-titanium dioxide suspensions in the decontamination of rough titanium surfaces, Biofouling. 33 (2017) 451–459. doi:10.1080/08927014.2017.1322585.
[86] M.J. Flores, R.J. Brandi, A.E. Cassano, M.D. Labas, Chemical disinfection with H2O2 - The proposal of a reaction kinetic model, Chem. Eng. J. 198–199 (2012) 388–396. doi:10.1016/j.cej.2012.05.107.
[87] A. Wennerberg, T. Albrektsson, A.T. Wennerberg A, Suggested guidelines for the topographic evaluation of implant surfaces., Int. J. Oral Maxillofac. Implants. 15 (2000) 331–344.
[88] T. Kokubo, Bioactive glass ceramics: properties and applications, Biomaterials. 12 (1991) 155–163. doi:10.1016/0142-9612(91)90194-F.
[89] J. Forsgren, F. Svahn, T. Jarmar, H. Engqvist, Formation and adhesion of biomimetic hydroxyapatite deposited on titanium substrates, Acta Biomater. 3 (2007) 980–984. doi:10.1016/j.actbio.2007.03.006.
[90] P. Li, P. Ducheyne, Quasi-biological apatite film induced by titanium in a simulated body fluid, J. Biomed. Mater. Res. 41 (1998) 341–348. doi:10.1002/(SICI)1097-4636(19980905)41:3<341::AID-JBM1>3.0.CO;2-C.
[91] O. Janson, M. Strømme, H. Engqvist, K. Welch, Debridement of Bacterial Biofilms with TiO2/H2O2 Solutions and Visible Light Irradiation, Int. J. Biomater. 2018 (2018) 1–8. doi:10.1155/2018/5361632.
[92] E. Unosson, K. Welch, C. Persson, H. Engqvist, Stability and prospect of UV/H2O2 activated titania films for biomedical use, Appl. Surf. Sci. 285 (2013) 317–323. doi:10.1016/j.apsusc.2013.08.057.
[93] E.I. Weiss, M. Shalhav, Z. Fuss, Assessment of antibacterial activity of endodontic sealers by a direct contact test, Dent. Traumatol. 12 (1996) 179–184. doi:10.1111/j.1600-9657.1996.tb00511.x.

63
[94] C. Vuong, S. Kocianova, J. Yu, J.L. Kadurugamuwa, M. Otto, Development of real-time in vivo imaging of device-related Staphylococcus epidermidis infection in mice and influence of animal immune status on susceptibility to infection, J. Infect. Dis. 198 (2008) 258–61. doi:10.1086/589307.
[95] S. Yamaguchi, H. Takadama, T. Matsushita, T. Nakamura, T. Kokubo, Apatite-forming ability of Ti-15Zr-4Nb-4Ta alloy induced by calcium solution treatment, J. Mater. Sci. Mater. Med. 21 (2010) 439–444. doi:10.1007/s10856-009-3904-0.
[96] J.S. Guffey, J. Wilborn, In Vitro Bactericidal Effects of 405-nm and 470-nm Blue Light, Photomed. Laser Surg. 24 (2006) 684–688.
doi:10.1089/pho.2006.24.684. [97] X. Li, M.J. Kim, W.S. Bang, H.G. Yuk, Anti-biofilm effect of 405-nm LEDs
against Listeria monocytogenes in simulated ready-to-eat fresh salmon storage conditions, Food Control. 84 (2018) 513–521.
doi:10.1016/j.foodcont.2017.09.006. [98] G.F. Gomez, R. Huang, M. MacPherson, A.G. Ferreira Zandona, R.L.
Gregory, Photo Inactivation of Streptococcus mutans Biofilm by Violet-Blue light, Curr. Microbiol. 73 (2016) 426–433. doi:10.1007/s00284-016-1075-z.
[99] ISO/EN10993-5, Biological evaluation of medical devices-Part 5: Tests for in vitro cytotoxicity, 3 Ed (2009) 42.

Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Science and Technology 1712
Editor: The Dean of the Faculty of Science and Technology
A doctoral dissertation from the Faculty of Science andTechnology, Uppsala University, is usually a summary of anumber of papers. A few copies of the complete dissertationare kept at major Swedish research libraries, while thesummary alone is distributed internationally throughthe series Digital Comprehensive Summaries of UppsalaDissertations from the Faculty of Science and Technology.(Prior to January, 2005, the series was published under thetitle “Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Science and Technology”.)
Distribution: publications.uu.seurn:nbn:se:uu:diva-358253
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2018