Embed Size (px)
Citation preview

Biennial Analysis of Serious Case Reviews 2003- 2005 and
2005-7
Ruth GardnerUniversity of East Anglia (with University of Warwick)

A typical serious case review(death or serious injury of a child where abuse or neglect is
a factor)
“[mother] had a series of violent partners…, suffered with mental health problems, anxiety and depression and was misusing alcohol. The family changed address frequently….all three children witnessed serious domestic abuse… [mother] failed to attend a number of medical appointments with the children.”
• Biennial Analysis of Serious Case Reviews 2003-5 (161 cases) and 2005- 2007 (189 cases)

Research Questions (2005-7)• To identify common themes and trends across
review reports, using an ecological-transactional approach and drawing out the implications for policy and practice;
• To explore the way in which reviews are commissioned and scoped, how they are published and how key messages are disseminated locally; discover what mechanisms are put in place locally to implement the findings and to monitor their implementation;
• To capture the learning from this first phase so that it can feed into a longer term project to develop and implement a revised method of conducting national reviews.

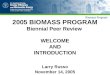
The SCRs - 189 cases (2005-7) & methodology
Layer 1 = 464All notifications to child
protection database CSCI/DCSF
Layer 3 = 40Small sample
Overview reports, chronologies, sometimes IMRs
Layer 2 = 189all SCRs
Minimal information about each case from
DCSF/CSCI
Layer 1. Find the SCRs
Layer 2. Describe the cases
Layer 3. Examine 40 cases in detail. 24 Interviews about SCR process.

Layer 1: Which cases become serious case reviews?

189 SCRs – where from? (2005-7)Type of notification (as stated on
national child protection database reports) 464*
“Death of a child looked after”
124
“Serious Harm to a child”
54
“Serious Case Review confirmed”
135
“Serious Case Review possible but not yet
confirmed”151
No101
SCR13
?10
No43
SCR7
?4
No81
SCR42
?28
No4
Yes127
?4SCR
?

Findings: Layer 2 cases 161 cases 2003-5, 189 cases 20005-7

Death or serious injury cases?
• 66% death Reason for SCR: A’s stepfather had a criminal record and was in
care of the council when younger. The council also wants to ensure the circumstances of death undergo a thorough review. (suicide)
• 34% serious injury These children are (now) subject to full care orders. There is a
long history of neglect and concern that the developmental delay experienced by these children could have been minimised if agencies had worked together earlier and worked effectively. The SCR will investigate the concerns raised in the course of care proceedings.
Same proportions of death/ serious injury 2003-5 and 2005-7

Age of child at time of incident2003-2005
11%
11%
10%
23%
46%
>16yrs11-15yrs6-10yrs1-5yrs<1yr
age categories
9%
16%
7%
20%
47%
>16yrs 11-15yrs 6-10 yrs 1-5yrs <1yr
age categories
2005-2007

Ethnicity 2005-7
2%5%
8%
13%
72%
Other Ethnic GroupAsian/Asian BritishBlack/Black BritishMixedWhite
Ethnicity
Similar ethnic proportions in both studies, but fewer Black/ Black British children 2005-7 than 2003-5, more mixed race children.92% of ethnicity recorded 2005-7, 84% in 2003-5.

Child Protection Plans/ Legal Status (2005-7 n=189)
• 17% of children with a cp plan at time of incident (12% in 2003-5).
- 11 physical abuse, - 7 sexual abuse - 7 emotional abuse - 30 neglect. (Some children in combined categories).
• In 1/3 of families either the index child or sibling had current or past cp plan.
“L was living with mother and three older half siblings, history of domestic disputes with ex-partners and of substance misuse by mother.” (at home with CP plan)
• 11% on a care order, 2% supervision order , 5% ‘looked after’

Analysis: Layer 3 cases 40 cases (2005-7) 47 cases (2003-5)

Interacting factors 2003-3 (n=47 )
Child factors and experiences
Family and environmental factors
Practice/professionals, agency factors
Very young babies (prematurity, admissions to hospital, types of injury)Middle years children largely missing (protected?) Older child, hard to help (self neglect, chronic illness, sexual exploitation, ‘going missing’,bullying,Suicide
Co-morbidity of Domestic violence,Substance misuse,Mental ill healthFathers, hostility, criminal convictionsPatterns of hostility and cooperation Family History, eg neglect, previous child death,Poverty, poor living conditions, Frequent moves accidents, fires
Child not seen/ heardAgency context, capacity, ‘organisational climate’Preoccupation with thresholds e.g. CP threshold not metProfessional anxiety, reluctance to act and challengeSupervisionEthnicity challenges
Neglect, ‘start again syndrome’Keeping track of families

inter acting factors 2005-7 (n=40)Family and environmental factors
Practice/professionals, agency factors
Chaos, overwhelmed families with low expectations
Unsupported families or negative support
“toxic trio” (dv, mental ill health, substance misuse etc)
Men: Good dads, bad dads, men not known about
‘Accidents waiting to happen’
House fires, multiple moves, poor living conditions
Large families
Overwhelmed workers, low expectations
Unsupported workers, Professional uncertainty
‘other people’ are seeing the child
Efforts not to be ’judgemental’ ,
Fixed views, men, neglect
‘off the radar’ cases
Thresholds and boundary disputes
Lack of cultural sensitivity / over sensitivity.

The missing child• During both police and CSC enquiries into the
allegations it appears that the children were either not seen or spoken to in any detail and no direct work was undertaken during CSC involvement.
• The last date that X was seen by any professional prior to her death (at age 11 months) was for her 6 week check and first immunisations at her GP surgery. Health professionals continued to visit the family home seeing other family members, but not X.
• There were lost opportunities to speak to the young person about his perceptions and feelings; therefore there is little understanding of the “child’s world”. The core assessment was not shared with (him), nor were his views sought; he was of an age and understanding to have the core assessment discussed with him directly.
• Child also missing from the SCR – eg about MARAC or MAPPA processes, not the child or child’s needs.

Child factors/experiences• Child missed, lost , isolated, assaulted • ‘Ecological niches’ for children of different
ages• Prematurity, low birth weight, neonatal
abstinence syndrome • Illness, complex health needs, disability• ‘Hard to help’ • Suicide • Unhappiness not known about • Bullying• Risk taking behaviour, substance misuse,
sexual exploitation• History of neglect and rejection

Children: Ecological Niches1. a pre-school, family based environment, with a neo-natal
sub-environment; 2. a middle childhood, somewhat protected, mixed school
and family niche; 3. an adolescent, risk exposed, transition to adulthood
niche.Helps us understand risks of harm/ protective factors from
the environment, from others, and also for the older children, from within themselves.
“The types of homicide suffered by children are related to the nature
of their dependency and to the stage of their integration into the adult world. Among the factors that may well change across childhood and across these niches are the victim-offender relationship, the locale where the homicide occurs, the nature of the weapon, the motives involved, and the contribution the victim makes to the crime in terms of risk taking and provocation. These homicide variations provide a good case for assuming the importance and utility of a developmental perspective on child victimizations…” (Finkelhor 2008:40).

Pre School Age Niche• 26 children – 17 babies. This age group most vulnerable to
death from abuse (internationally).• Physical vulnerability of these young children mean that
many die from force and violence that would not kill an older child. Older children, no longer so dependent, can physically move, run out of the way or fend for themselves.
• 1/3 born premature – lasting impact. 6:17 babies had hospital admissions (1 x 9), 3 to A&E at least once.
“ Pre-school victims of homicide appear to be mostly cases of fatal child abuse that occur as a result of a parent’s attempts to control a child or angry reactions to some young child’s aversive behaviour – uncontrollable crying, hitting parent or siblings, soiling himself or herself, or getting dirty, for example (Finkelhor 2008:39).

Middle Childhood• 4 children aged 6-10 (2 known to CSC)• Small number reflects the lower level of emotional and
physical demands children of this age make on their caregivers.
• Higher level of protection offered by their environment - school.
• But: children of this age at A&E most often with unexplained injuries linked to maltreatment (Woodman et al 2008). Rarely subject of SCR but still maltreated.
• Some history of problems with eyes, ears, speech and language. Not uncommon - but delay in treatment causes problems. Some links between hearing problems and behavioural difficulties, particularly in combination with other family problems.

Adolescence• 10 young people aged 11-17 years. 7
suicides.
• Patchy school attendance - numerous house moves, truancy or school exclusions (2 had left school)
• 5 with low level services: eg carer for disabled brother at home, and struggled at school and in home community where he was bullied.
• 5 well known to agencies and had profiles characterised by risk taking behaviour, substance misuse and sexual exploitation.

inter acting factors 2005-7 (n=40)Family and environmental factors
Practice/professionals, agency factors
Chaos, overwhelmed families with low expectations
Unsupported families or negative support
“toxic trio” (dv, mental ill health, substance misuse etc)
Men: Good dads, bad dads, men not known about
‘Accidents waiting to happen’
House fires, multiple moves, poor living conditions
Large families
Overwhelmed workers, low expectations
Unsupported workers, Professional uncertainty
‘other people’ are seeing the child
Efforts not to be ’judgemental’ ,
Fixed views, men, neglect
‘off the radar’ cases
Thresholds and boundary disputes
Lack of cultural sensitivity / over sensitivity.

Chaotic families: Professional responses & behaviour
Too much to achieve, low expectations, ‘success’ is
getting through the door, muddle about confidentiality
Overwhelmed, chaotic families, ‘negative’ family support,
drugs, violence, mental ill health,
criminality.
Fixed views about Family, men, neglect
silo practice.
Efforts not to be judgemental, whole picture not seen, separate ‘specialisms’ offer support.
Invisible children

Known to children’s social care?
2003-5 (n=47)• 55%
•Family known in past: 87%
•NB Almost half not known to CSC at time of incident in both studies
2005-7 (n=40)• 53%
•Family known in past: 78%
“Child protection does not come labelled as such” (Laming 2003)

Overwhelming,
Efforts not to be judgemental“ a tendency towards justification and reassurance
that all was well, rather than more objective consideration and investigation of what had occurred”
• “x presented as a pleasant young woman who had complex needs and professionals felt compassionate towards her and she was given repeated chances to improve matters and to reduce and manage her drug use”
There is no reason to doubt her honesty in terms of her intentions. It is right that professionals should be supportive of such intentions. However such support should be matched by a critical awareness of the difficulties facing a person with a dependency on drugs in reducing their consumption”

Fixed views • ‘Neglect case’ as a mindset – physical
injury missed (eg case 03 two s47 enquiries for physical injury)
• Men - ‘good’ dads or ‘bad’ dads (eg father’s
concern about ex wife’s parenting discounted no checking of ‘improvement’ in spite of past history of extreme dv, (start again syndrome)
• Uncertainty (confidentiality), assumptions that others are seeing the child
• rigid specialisms, silo practice• These preoccupations shift the focus
away from the child/ren

Additional theme:
SCR doesn’t provide enough information to decide – ‘was it preventable’? Why aren’t the right questions asked?
• Limited information about the family (eg parents’ past)
• Limited information about the family’s environment eg poverty
• Limited information about the agencies’ capacity and ‘climate’
• Limited information about the child

Layer 3 contd: The serious case review process

The SCR process - delay
• Only 2 of the 106 reviews from 2005-2006 were completed within 4 months. Not a manageable time scale
• Challenging court proceedings as a reason for delay: - LSCB has authority to insist that SCR should not
be held up, and to assert that the SCR process is an important part of its safeguarding role.
- A presumption that the SCR process go ahead, and be published, unless discussions with CPS and coroner reveal a good reason for delay.
- If delay is reasonable, negotiations should allow action plan to be implemented (although report publication might be delayed).
- The agency that requires the delay (eg CPS) should provide written reasons for submission (to GO/Ofsted).

Negative SCR cycle
Deference to media.SCR as PI
Lack of supervisionBlame culture returns
Fear of families/ blame/
litigation Defensive practice &
SCRs
Practitioners & families
excluded from SCR process.
Child largely absent &out of mind

Impact of SCR on Practitioners (from regional seminars)
• Feelings of failure, guilt or being made a scapegoat (21)
• Fear, anxiety (20)• Threatening, threatened (8)• Stressful (6)• Emotional impact ( 8• ‘upset’, ‘traumatic’, ‘devastating’, ‘under
scrutiny’ and ‘vulnerable’ • Added stress of media involvement; “the
media wants a scapegoat, but we want lessons learned”.

Impact on practitioners (contd) The impact is profound and long lasting.
I am emotionally scarred by this. Loss of professional confidence
I guess, initially, it made me completely lose all my confidence. It made me question my trust in any of my judgements. I almost started to doubt my clients’ histories, and became quite suspicious, although that has improved over time.
Good support valued “what helped was just being able to share with colleagues”.

A positive SCR cycle
‘Open to learning’ Agency context
included. Full information –
agency context, family, household.
Involvement of practitioners,
& families.
Publication of exec summary.
Media strategy. Creative ways of
disseminating learning
Child at heart of the SCR

Impact on practitioners• Restored professional confidence and
ability to challenge: It is every professional’s responsibility to
say “No, I disagree”. Wherever they sit in the hierarchy, at the end
of the day they are just a person. And at the end of the day it is about the child.
• Practitioners/clinicians feel excluded(practitioners) are excluded from the whole
process, our actions are scrutinised (which is understandable) and then we're left to get on with it, with little support during the process and at the time the report is published.

A Positive practice cycle
Support and trust in teams
Clear lines of communication with other agencies.
Confident professional judgement
and sustained challenge
Good working relationshipswith children & families.
Reflective, challenging supervision.
Child seen, kept in mind, understood

Conclusions• There are no simple or easy answers to
the challenge of protecting children, only a relentless focus on doing the best we possibly can, at every level and in every service. But Laming’s full and frank analysis does not provide a guarantee against the combination of failings and circumstances that led to the death of Baby P. The unpredictability of human nature and the restrictions on the current system mean the scale of the task is immense. (Eaton, Bromley-Derry, Myers The Guardian 2009)

ConclusionsThe children • …the more you try to see the world from the child’s point of
view and the safer you make him feel, the better his behaviour is likely to be and the more likely you are to find ways of further improving it’ Perry and Szalavitz 2008:245
The workers • One of the greatest lessons I’ve learned in my work is the
importance of simply taking the time, before doing anything else, to pay attention and listen. Because of the mirroring neurobiology of our brains, one of the best ways to help someone else become calm and centred is to calm and center ourselves first – and then just pay attention’ (Perry and Szalavitz 2008:244-245)
• “..ultimately the safety of a child depends on staff having the time, knowledge and skill to understand the child or young person and their family circumstances.” (Lord Laming 2009:10)

Tomorrow’s SCR?• Same issues locally and nationally eg
loss of focus on the child; drift; neglect not
regarded as significant; poor quality control.
Questions to get us going
? What was “true for you” in these findings
? How could case R/V ( inc SCRs) be used HERE & NOW for more effective learning
? Revision of WT- how could SCRs be improved
ISSUES/STRENGTHS/GAPS/ACTIONS