-
8/13/2019 Best Practices for Complex Liability Claims
1/62
Provider Best Practicesfor Complex Liability Claims
Educate | Navigate | Connect
APA Results
-
8/13/2019 Best Practices for Complex Liability Claims
2/62
Content
Overview
Industry Dynamics
Action steps to take beginning at the point of registration
on
employment injury claims
The impact of state and federal laws
Why facilities and providers may not be maximizing recoveries
on
liability claims
Training opportunities for liability claim handling
2
20
13AdvancedPatientAdvoca
cy
-
8/13/2019 Best Practices for Complex Liability Claims
3/62
Overview
Liability claim processing boils down to the following
elements:
Training up-front data acquisition staff
Classifying accounts correctly upon point of service
Identifying administrative inefficiencies with insurance claim
handling practices that
create financial loss
Garnering insurance details of each injury encounter
Using forensic analysisin an administrative wayto resolve open
claims for
injured patient
Working with patients, next-of-kin, employers, insurance
companies, and
attorneys to take a medical claim and do all the legwork to get
it paid by
a liability-based insurer
3
2013AdvancedPatientAdvocacy
-
8/13/2019 Best Practices for Complex Liability Claims
4/62
Industry Dynamics
4
2013AdvancedPatientAdvocacy
-
8/13/2019 Best Practices for Complex Liability Claims
5/62
Industry Conditions
High Self-Pay = Growing Trend for Facilities
Self-pay and bad debt are often difficult
classificationshospitals genuinely
want to avoid these areas. They often become default zones for
patients who
present with no coverage at time of encounter.
Hospitals often have multiple collections vendors on boardwith
only an
8-25% rate of return(high-end estimate).
Self-pay percentages of overall revenue should not go beyond 20%
of
overall hospital A/R, but often does
Increased education of liability claim handling assists
facilities
across the board
5
-
8/13/2019 Best Practices for Complex Liability Claims
6/62
State Negligence Rules: Motor Vehicle Accidents
No-Fault States: Advantages
Personal Injury Protection provision
exists on policies, in addition to
MedPayprovision as purchased by
motorists
Florida, Hawaii
Kansas, Kentucky
Massachusetts, Michigan
Minnesota, North Dakota
New Jersey, New York
Pennsylvania
Utah
Tort States: Advantages
Comprises the remainder of the country
aside from true no-fault states
Individual must be found at fault in
an accident = multiple avenues ofinsurability (either patients
own policy,
or at-fault policy, with insurance
subrogation to occur behind the
scenes.)
More investigation; more coordination;but with skilled
follow-up, the
hospital can achieve strong
returns.
6
2013AdvancedPatientAdvocacy
-
8/13/2019 Best Practices for Complex Liability Claims
7/62
Overall Conditions for WC Policies
Reimbursement Rates Each state WC Board determines
reimbursement rates
Outpatient Fee Schedules are
around 60-65% reimbursement
nationally
Inpatient payment structures are
often reasonable and achievable --
with appeals and close follow-up
between hospital and payer
Escalating to the state WC Board
works to the hospitals advantage
Timeliness rules vary state to state
Employment Rates
Researching top employers and safety
statistics in each region is helpful to
understand local WC demographics and
patterns
Employability is a big factor; for example,
Florida may have more MVAs than
Workers Comp. However, large
employers in FL will very often have more
WC accidents:
Wal-Mart
Publix Grocery
Home Depot
7
2013AdvancedPatientAdvoc
acy
-
8/13/2019 Best Practices for Complex Liability Claims
8/62
Macroeconomic Environment
United States Injury/
Fatality Rate
Total uninsured: 16.7% = 50.7 mmpeople
MVA injuries: 2.22 mm injuries (2011)
MVA fatalities: 32,367 (2011)
WC injuries: 2.9 mm injuries (2011)
WC fatalities: 4,609 (2011)
Personal injuries
Dog bites: 800,000 med visits
Falls: 200,000 children
Falls: 2.3 mm older adults (2010)
Hospital Outlook
Reduced reimbursements: CMS
Expanded future coverage through PPACA
Aging population increasing
Declining birth rate; future generations
bearing increased CMS costs
Immigrant population showing trends of
declining birth rate
Commercial health payers increasing
deductibles and out-of-pocket expenses
8
2013AdvancedPatientAdvocacy
-
8/13/2019 Best Practices for Complex Liability Claims
9/62
The Present and Future
9
-
8/13/2019 Best Practices for Complex Liability Claims
10/62
Times Have Changed
Insurance companies want to know the thought processes
physicians use to
reach medical decisions.
Payments for liability injuries, such as Workers Compensation
injuries, are
rarely paid without medical justification.
Clinical documentation and well-completed forms can assist
providers in
meeting complex insurance and state-driven requirements.
-
8/13/2019 Best Practices for Complex Liability Claims
11/62
-
8/13/2019 Best Practices for Complex Liability Claims
12/62
Lifecycle of a Liability Claim
12
2013AdvancedPatientAdvocacy
-
8/13/2019 Best Practices for Complex Liability Claims
13/62
1. Patient presents to physician with chief complaint
2. The collection of data for a medical claim begins at this
time during check-in
3. Frontline representatives collect and document
insurance information
4. The most important aspects of the medical claim cycle
occur between the time the patient arrives at the
provider and the time the medical claim is generated. It
can be the shortest part of the entire revenue lifecycle,
but also the most important.
Lifecycle of a Liability Claim
Note:Many points
exist in the
cycle for a
claim to get
lost or goawry.
-
8/13/2019 Best Practices for Complex Liability Claims
14/62
5. During the patients evaluation, the physician isresponsible
for documenting the details of the
encounter.
6. Coders assign numeric codes for chief complaint,
other diagnoses, external forces if applicable, and
procedures rendered. (Example: 847.0 for neck
sprain; E812.0 for motor vehicle accident that
may occur.) Note: MVAs may occur in the course
and scope of an individuals employment.
7. Billers identify payer, speak with claims adjuster,
and ship bill and records to correct address.
Lifecycle of a Medical Claim, Briefly
-
8/13/2019 Best Practices for Complex Liability Claims
15/62
The quality and accuracy of billing information and clinical
documentation
(as it flows through each department) has the single greatest
impact on
the quality of the claim.
Payer follow-up is critical to reimbursement
Receipt of claim and accompanying records
Adjudication
Payment determination
Exceptions escalated
Denials explained clearly and justified by payer
Lifecycle of a Medical Claim, cont inued
-
8/13/2019 Best Practices for Complex Liability Claims
16/62
Best PracticesOverview on Claim Handling to Achieve Greater
Performance
16
-
8/13/2019 Best Practices for Complex Liability Claims
17/62
Data elements to garner:
Employer name pertinent to injury
Employer address and main phone number
Date of Accident
Basic Injury, Body Part(s) affected
Employer HR/Manager/Foreman name and number
Patient unable to communicate:
If patient was brought in with coworkers or supervisor, gather
same data Employer must file accident report with insurance carrier
and state industrial
accident board
Do not default financial class to Self Pay
Registration:
On-the-Job Injuries
NOTE:If insurance
carrier is known atpatient encounter,
call insurancefor service
authorization assoon as possible
-
8/13/2019 Best Practices for Complex Liability Claims
18/62
Data elements to garner:
Policyholder of vehicle
Role of patient (driver, passenger, cyclist,pedestrian)
Patient address and main phone number
Date of Accident
Where/How injury occurred
Insurance company known?
Drivers auto insurance company name
Other partys auto insurance name
Own health insurance as secondary plan
Attorney data if applicable
18
Registration: MVAs
Patient unable to communicate:
Gather data from next of kin as
appropriate
Request police report post-discharge
Place call/send questionnaire to
patients home for accident and
insurance details
Do not default financial class to Self
Pay
-
8/13/2019 Best Practices for Complex Liability Claims
19/62
MVA: Secret Coverage to Obtain
19
-
8/13/2019 Best Practices for Complex Liability Claims
20/62
Registration:Personal Injuries
Data elements to garner:
Geographic location of injury (address ofwhere injury occurred)
-the key to liability isif the injury occurred NOTat patients
own
home; although sometimesthere could beliability propensity on
leased property.
How injury occurredExamples: neighborspitbull bit patient, or
slip/fall at grocery store
Patient address and main phone number
Owner/Entity Contact Data
Date of Accident
Health plan as secondary (Plan B option)
Attorney data if patient has hiredrepresentation
Patient unable to communicate:
Gather data from next of kin asappropriate
Request ambulance or police report (iffirst responders were on
the scene)post-discharge
Place call/send questionnaire topatients home for accident
and
insurance details
Do not default financial class to Self
Pay
-
8/13/2019 Best Practices for Complex Liability Claims
21/62
Tricky ExamplesShout Out Your Answers
Elderly woman suffers a herniated disc while liftinga bag of
soup cans at her church food pantry.
Liability or Medicare? Both? Neither?
A man riding a dune buggy flips over and suffersa broken rib and
collarbone.
Motor Vehicle or Health plan? Both? Neither?
A woman riding a motorcycle oversteers and grazes the side of
her body, andsuffers road rash.
Motor Vehicle or Health plan? Both? Neither?
A man transferred from another facility has MS and old
orthopedic injuriesfrom his job as a postal worker.
Workers Compensation or Health plan? Both? Neither?
21
-
8/13/2019 Best Practices for Complex Liability Claims
22/62
The Significance of Clinical Documentation
Substantiates services
Charges will be understood at the insurancecompany
Validates necessity of treatment
Speeds up bill payment when packagedtogether particularly for WC
claims
Nurses notes
Physicians report
History and Physical
Lab reports
Radiology reports
* Denotes Where allowed by state/county law;
ensure signed authorization on file by patient
Tips:1. Marry medical records with bills for WC claims 100%of
the time at first submission
2. Send liens, lien letters, or request Letters ofProtection to
attorneys that request medical records toensure they are aware of
medical charges in advance offinal settlements*3. Issue your
invoice for medical records where allowedby state law and hospital
policy
Therapy:
Physical
Behavioral
Speech
Durable Medical Equipment
Implantable Device Invoices
Itemization of all services rendered
-
8/13/2019 Best Practices for Complex Liability Claims
23/62
At the Insurance CompanyBehind the Curtain:
What Happens to the Bill Form and Records
23
2013Adva
ncedPatientAdvocacy
-
8/13/2019 Best Practices for Complex Liability Claims
24/62
Electronic submission (secure 837-5010 format)
Mandated/encouraged states:
Texas
California
Minnesota
Illinois
New York
Dependent on payer capability
Some are set up to accept electronic submissions
Paper Submission
Red 1500s or UBs
Black and White forms acceptable; sometimes rejected
forreadabilityensure legibility
Fax Directly to Insurance Adjuster
Note:Always indicate
in your host
system the
submission date
and location ofwhere the bill
and records were
sent. This
includes the
specific
adjusters name.
Work Comp Claim Submission Methods
-
8/13/2019 Best Practices for Complex Liability Claims
25/62
Many major Property and Casualty insurers have
standalone data centers
Central mailing point
Mail opened and categorized by type
All mail is scanned into their system
Claim numbers found if not on documents
Document sent electronically to each appropriate adjuster
across the country
Employer must file accident report.
Sometimes data centers are within the US or off-shored
It is not customary to contact data centers directly for claim
status
Insurance Company Data Centers
Critical tips:
1. Having claimnumbers ondocuments beforemailing saves anaverage
of 21 days ofprocessing at theinsurance company(really!)
2. If no claim numberwas opened or found,claim will be
rejectedas such.
.
-
8/13/2019 Best Practices for Complex Liability Claims
26/62
Medical bills (claim forms)
Red paper is scanned
Red lines are dropped out by scanners
pixel interpretation
Raw data is automatically fed to billreview systems
Less errors, but still imperfect
Black and white bills are manually dataentered
Slower processing time
Prone to more errors in data entry
Always double check EOBS forinsurance- rep errors.
Data Centers, continued
-
8/13/2019 Best Practices for Complex Liability Claims
27/62
Example UB
-
8/13/2019 Best Practices for Complex Liability Claims
28/62
Resulting EOB with errors
-
8/13/2019 Best Practices for Complex Liability Claims
29/62
Determination
Adjuster Reviewand/or
Automated Rules Engine
Based on accident report and
severity of injury, adjuster will set up
rules that will automatically OK to
Pay certain services, taking the
human element out of manual
examination
Usually done with lower balance,
less complex claims
The role of the adjuster is
threefold:
Own claim from start to finish
Examine claim validity and
any evidence of fraud
Reduce insurance loss by
predicting value of overall
claim
Adjudication
-
8/13/2019 Best Practices for Complex Liability Claims
30/62
Managed Care departments exist
in the Property/Casualtyinsurance environment!
Line-by-line re-pricing of billsoccurs using various methods
PPO contracts
Fee schedule
Usual and Customaryguidelines
Nurse case management
DRG (not line-by-lineanalysis; rather a fixedcode)
Many other methodologies
A Few Words on Silent PPOs
When a claim is paid, anExplanation of Benefits (EOB)is issued
with the check
The rationale of paymentshould indicate if a contractual
agreement was accessed fordiscounts
Does your facility have acontract in place with thepayer
mentioned on the EOB?
Challenge the insurer if not!
Bill Review and Pricing
-
8/13/2019 Best Practices for Complex Liability Claims
31/62
-
8/13/2019 Best Practices for Complex Liability Claims
32/62
Reimbursement MethodsHow a Claim is Paid (or Not)
32
2013Adva
ncedPatientAdvocacy
-
8/13/2019 Best Practices for Complex Liability Claims
33/62
Types of Reimbursement: National Overview
APCs
Capitation
Case rate
DRG
Day Differentials
Service Differentials
Fee Schedule and
Timely Pay FeeSchedules
All methodologiesoperate under
various contracts,policies, and
guidelines, that alldepend on stateand federal laws.
Flat Rate
Per Diem
Managed Care stop loss
outliers Case based outliers
Reinsurance stop loss
Percentage stop loss
At Charges Sliding scale
discounts
-
8/13/2019 Best Practices for Complex Liability Claims
34/62
Diagnosis-related groups: A classification system that
categorizes patients who
are medically related, with respect to diagnosis and treatment.
They are statisticallysimilar in length of hospital stay. Its a
lump-sum, fixed-fee based on diagnoses. Fees aremade by a research
team, which determine national averages. DRG numbers go from001 to
900. Variables in DRG classification:
Principal Diagnosis; Secondary diagnosis (up to eight)
Surgical procedures (up to six)
Comorbidity (pre-existing conditions) and complications
Age and sex
Discharge status
Number of hospital days for a specific diagnosis
Day Differential: First day paid at higher rate, cascading down
each following day.
Service Differential: Hospital receives a flat per-admission
reimbursementfor the service. A prorated payment can be made (e.g.,
50% ICU, 50%medical services) Services are defined in the
contract
Courtesy: Marilyn Fordney; Medical Administrative Procedures
Breaking the Methodologies Down
-
8/13/2019 Best Practices for Complex Liability Claims
35/62
Ambulatory Payment Classifications (APCs): Based on PROCEDURES,
not
diagnoses. Services are assigned a group code:
Surgical
Significant procedures
Medical
Ancillary
Note: Modifiers are important to clarify multiple services!
Capitation/Percent of Revenue: Reimbursement to the hospital on
a per-member, per-
month basis regardless of hospitalization. Percent of Revenue is
a fixed rate of payment.
Case Rate: Averaging after a flat rate for a service has been
given to certain categoriesof procedures. Specialty procedures may
be given a case rate (e.g., graft surgery).
Bundled case rate is an all-inclusive rate for institutional and
professional
services connected with the procedure.
Breaking the Methodologies Down
-
8/13/2019 Best Practices for Complex Liability Claims
36/62
Fee schedule: list of charges based on procedure codes.
Fee-for-service basis.
Flat rate: A set amount per hospital admission regardless of
cost of actual services
Per diem: single charge for a day in the hospital, regardless of
actual charges or costs
Managed Care stop loss outliers:
Case-based stop loss: A mechanism of hospital and insurance
carrier sharing loss. It is
a payment of a percentage over a certain dollar threshold (e.g.,
65% of excess billing
over $100,000.)
Reinsurance stop loss: The hospital buys insurance to protect
against lost revenue
and receives less of a cap fee. The amount they dont receive
helps pay for the
reinsurance. Example: A case reaches $100,000. The plan may
allow 80% of expenses
in excess of that figure for the rest of the year.
Percentage stop loss: A percentage paid of charges when a
certain
threshold is met.
Breaking the Methodologies Down
-
8/13/2019 Best Practices for Complex Liability Claims
37/62
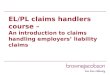
A percentile is defined as a value
on a scale of 100 that indicates
the percent of a distribution that is
equal to or below it. For example,
the 75th percentile means that 75
percent of all fees for CPT code
99203 fall at or below $136. It also
means that 25 percent of all fees
for CPT code 99203 fall at or
above $136. Data is analyzed
by ZIP code by the
insurer.
99203 = $136 by XYZ Insurer
Office or other outpatient visit for
the evaluation and management
of a new patient, which requires
these three key components: adetailed history; a detailed
examination; and medical decision
making of low complexity.
Physicians typically spend 30minutes face-to-face with the
patient and/or family.
37
Usual and Customary Explanation
-
8/13/2019 Best Practices for Complex Liability Claims
38/62
Workers Compensation DetailsAnalyzing the Process
38
2013AdvancedPatientAdvocacy
-
8/13/2019 Best Practices for Complex Liability Claims
39/62
Workers in the late 1800s had it tough. For injuries and deaths,
the legal processes were
uncertain. Negligence had to be proven by the employee, and very
often there was little
recourse.
In 1911, the first workers compensation laws were adopted by
several states. The laws allowed
injured workers to receive medical care without first taking
employers to court.
All states currently have workers compensation laws. They vary
from state to state.
This coverage is the most important coverage written to insure
workplace accidents.
A Very, Very Brief History
-
8/13/2019 Best Practices for Complex Liability Claims
40/62
Two types of coverage:
Federal compensation lawspaid by US Department of Labor
Applies to miners, maritime workers, postal workers, and
government workers
State compensation lawspaid by self-insured businesses,
insured
employers, or state insurance funds
State and private business employees
Types of Coverage
-
8/13/2019 Best Practices for Complex Liability Claims
41/62
Employers pay for medical expenses directly instead of insurance
premiums
Precertification is importantthe self-insured employer is very
mindful of treatment
costs
Self-insured employers are covered by ERISA (Employee Retirement
Income Security
Act.)
Mandates reporting
Not state regulatedis under federal jurisdiction
90-day payment timeline. Employers may violate thisthere are
no
penalties for violation. Courteous but aggressive pursuit is a
must.
Self-Insured Employers
-
8/13/2019 Best Practices for Complex Liability Claims
42/62
The Beginnings ofWorkers Compensation Reform
By 1994, dysfunction Work Comp systems were costing companies
more
than $65 billion annually in many US cities.
Insurers began denying coverage to businesses.
Some businesses began relocating to states allowing lower
premiums.
Widespread legal and medical corruption and abuse evolved
throughout
the system.
-
8/13/2019 Best Practices for Complex Liability Claims
43/62
Antifraud legislation and increased penalties for fraud.
Anti-referrals that restricted physicians referring patients for
diagnostic
studies to sites where the physician has financial interest.
Proof of medical necessity for treatments, as well as
appropriate medical
documentation arose. Payers may refuse to pay the entire bill
without
medical documentation.
What Workers Compensation Reform Did
-
8/13/2019 Best Practices for Complex Liability Claims
44/62
Preauthorization for major operations and expensive tests
Caps on vocational rehabilitation
Development of fee schedules
Medical bill reviewpayer examination of duplicate claims and
billing
errors
More Reform Measures
-
8/13/2019 Best Practices for Complex Liability Claims
45/62
Employee has an accident occurring within the course and scope
ofemployment. Accidents can result in physical or mental injuries,
but again, mustbe within the scope of employment.
Employee is treated at a healthcare provider.
The accident must be reported by the employers HR/administrator
to both the
state and insurance company. Failure to report may be against
state law.
The healthcare provider must supply comprehensive information,
and they alsomay have to report information to the state, depending
on the law. (For instance,New York has a very involved state
reporting process.)
The insurance company must receive accident reports,
medicalrecords, and bills in order to make judgment and pay the
claim.
The ProcessIn Brief
-
8/13/2019 Best Practices for Complex Liability Claims
46/62
Out-of-State Claims
Follow all regulations from the jurisdiction in which the
injured was hired, andnot the state where the injury occurred
Companies with employees that travel must have policies that
cover out ofstate injuries
If a patient seeks treatment out of state, referralrequirements
must be met
Unauthorized care holds the patient responsible inthese
states:
Note:Maritime employeesdo not fall under state
workers compensation
laws. Example: Cruise shipemployees injured at seaoften have
their medical
bills paid in full, ornegotiated with a maritimecompany that
works with
the cruise line.
.
Alabama Alaska Arkansas
New Jersey North Dakota Ohio Washington West Virginia
Wisconsin
-
8/13/2019 Best Practices for Complex Liability Claims
47/62
Billing ProblemsSolutions to Common Issues,
and Avoiding Underpayments and Denials
47
2013AdvancedPatientAdvocacy
-
8/13/2019 Best Practices for Complex Liability Claims
48/62
Billing Problems
Lack of medical records
Incorrect patient name
Duplicate statements
Illogical dates
Date of service prior to date
of accident
Birthdate in the future
Facility Name & Address incorrectly or
not linked to facility Tax ID
Send documentation
Investigate patients name as it is on
valid ID and insurance cards
Send corrected claims and appeals to thecorrect addresseeit can
get lost in the
shuffle at any point
Correct dates
Send W-9 to Insurance
-
8/13/2019 Best Practices for Complex Liability Claims
49/62
Gender error
Missing principal diagnosis code
Missing revenue codes on UB
Missing CPTs on 1500 or outpatient UB
Missing Physician name and ID
Type of bill third digit (billing sequence)
doesnt correspond to statement coverage
dates
Correct gender
Add diagnosis
Add revenue codes
Add CPTs
Add Physician name
Correct Type of Bill to correspond
with dates
Note: Resubmit corrected claims
with new Type of Bill
Billing Problems
-
8/13/2019 Best Practices for Complex Liability Claims
50/62
Number of hospital days for room
charges must match number of
inpatient days
Missing unitsmany times defaulted
to 1 at insurance company if missing
on claim!
Always match inpatient days
Add value codes wherever applicable
Always, always input units. Insurance
companies pay by units. Anesthesia is
paid by minutes. (Surgical time is
examined.)
Billing Problems
-
8/13/2019 Best Practices for Complex Liability Claims
51/62
Undocumented workers
Incarcerated individuals
Municipal workers
Burn liability claims
Discuss with employer how claim will be paid
Is a contract in place with local Department ofCorrections? Will
Medicaid pay?
Is the municipality self-insured, or insured bya carrier?
How did the burn occur? Source is importantto determine
payment!
Industrial Accident
Home
MVA
Crime Victims Compensation
Unique Situations
-
8/13/2019 Best Practices for Complex Liability Claims
52/62
Coordination of BenefitsWhos on First, Second, Third
52
2013Adv
ancedPatientAdvocacy
-
8/13/2019 Best Practices for Complex Liability Claims
53/62
All Workers Compensation plans are
inherently no-fault
The injured worker is not responsible for
payments
The workers compensation carrier that
insures the employer will absorb liability and
pay
If the employer is self-insured, they will pay
Workers Compensation COB
Note:ONLY if a claim
ultimately ends upNOT being a true
workers compensation
situation, then it willbe: A health planresponsibility, or
A self-pay claim, if nohealth plan is active
-
8/13/2019 Best Practices for Complex Liability Claims
54/62
Sometimes, a patient will opt out of the Workers
Compensation
plan entirely, and outright sue their employer for damages
Settlement money will be owed to the hospital
Conduct regular follow-up with the attorney representing the
patient
Workers Compensation Tort Cases
-
8/13/2019 Best Practices for Complex Liability Claims
55/62
Motor Vehicle COB
In a No-Fault state, COB looks likethis:
PIP (Personal Injury Protection)
pays first
Patients health plan payssecond
At-fault third party pays third
Co-pays and deductibles can
kick into patients MedPayif
funds are available
At-fault settlement reimburses
health plans; satisfies
outstanding provider residuals
In a Tort state, COB looks like this:
- Patients MedPay pays first OR
at-fault Bodily Injury plan can
also be pursued
- Patients health plan pays second- At-fault settlement
reimburses
health plans; satisfies
outstanding provider
residuals
55
Note: Governmental payers are the payersof last resort
Note: Double check your health contractsfor any specific COB
language with lien
filing and liability settlement pursuit
-
8/13/2019 Best Practices for Complex Liability Claims
56/62
Challenging InsurersMaximizing Reimbursement and Speeding up
Payments
56
2013Adv
ancedPatientAdvocacy
-
8/13/2019 Best Practices for Complex Liability Claims
57/62
Affirm with the carrier that a cleanclaim was sent
Precert/Preauth done
Documentation received
Follow up in a timely manner (every 28
days)
Send in written tracer forms that ask
where the claim is at in the
adjudication process
Track all denials to learn what servicesare being denied, and
which insurance
companies are doing the denying
Send all high-dollar claims by certified
mail
Open a grievance with the State
Insurance Department if you dont get
anywhere
Delinquent or Slow Pay Claims
-
8/13/2019 Best Practices for Complex Liability Claims
58/62
An Explanation of Benefits (EOB) is sent either electronically
or by mail to thehealthcare provider for each claim.
Payment is enclosed with the EOB.
The remarks on the EOB are the first indication of whether
follow-up procedures
are required for the claim.
In many underpaid/unpaid cases, the next action is to correct
the claim information
and either re-bill the claim, or file an appeal.
Payer Response
Example of Appeal Letter:
-
8/13/2019 Best Practices for Complex Liability Claims
59/62
Example of Appeal Letter:Contractual Reduction
Dear Director of Claims,
It is our understanding that your company has released a partial
payment on the referenced claim. It is ourposition that this claim
has still not been reimbursed correctly and that additional
benefits are due.
Please be advised, it is our position that contractual
provisions stipulate a higher level of payment for thistreatment.
As a participating provider, we feel the following contractual
language or fee schedule reference isapplicable to this claim and
justifies additional payment:
{Insert potentially applicable contractual language. Reference
the page number or attach copy from contractto add as an attachment
to appeal.}
Our review of the provider contract does not reveal any language
justifying the current level of payment. Inorder to assess the
accuracy of payment, we request your response regarding how the
payment wascalculated ,and what portion of the fee schedule was
utilized. It is our position that if terms of the contract arein
direct conflict, the higher reimbursement should be allowed. As you
are likely aware, many courts haveruled that managed care contracts
are contracts of adhesion and that the organization responsible for
draftingthe contract wording can be responsible for unclear and
ambiguous terms.
Based on this information, we ask that this claim be reviewed.
We appreciate your prompt attention to thismatter.
Sincerely,Appeals Specialist
-
8/13/2019 Best Practices for Complex Liability Claims
60/62
Summary & Training OpportunitiesWhat Weve Learned Today and
Steps for the Future
60
2013Adv
ancedPatientAdvocacy
-
8/13/2019 Best Practices for Complex Liability Claims
61/62
Always educate the patient and take the stance of
patient-friendliness
Have the patient fill out Assignment of Benefits
forms consistently
Basic coding training includes locale (industrial
premises; highway) of injuries, which will help
identify accidents
Keep a paperless paper trail by notating every
detail of the claim cycle. Every detail helps.
Terms to Remember:
Adjuster
Adjudication
Utilization Review
Silent PPO
Appeal
Training Opportunities
-
8/13/2019 Best Practices for Complex Liability Claims
62/62
FeedbackClaudine Nesheiwat
Director of Operations, Liability Services
Phone: 804-272-6001 x227
E-mail: [email protected]