Embed Size (px)
Citation preview

Best practice rail safety:
Lessons from safety investigations
Rail 2007
Kym Bills
Executive Director ATSB
3 April 2007

Overview
‘Best practice rail safety: lessons from safety investigations’
�Background regarding the ATSB’s role and operations
�Recent rail safety data and the inter-modal context
�Developments to enhance rail safety data and its use
�ATSB investigations and key safety lessons from reports
�Concluding remarks on safety and sustainability

Rail
Marine
Aviation
Road

http://www.atsb.gov.au

ATSB role and operations
�ATSB approximately 111 staff, mostly in Canberra and
mostly dealing with aviation (Commonwealth sole role)
�Aviation and marine investigation recognised as among
best in world (ICAO, ISASI, IMO, MAIIF, ITSA activities)
�Road safety - similar recognition based on a dozen staff
�Rail safety – seeking to build a top reputation with 9
investigators and professional staff (4 in Adelaide HQ).
Via MOUs with jurisdictions, our focus is on the DIRN.

Defined Interstate Rail Network (DIRN)

Transport Safety Investigation Act 2003
�ATSB investigations do not apportion blame or liability
�Investigation reports cannot be used as evidence in civil or
criminal proceedings
�All investigation reports must be publicly released
�The Act gives the ATSB considerable investigative powers
�Independence, but cooperation with other investigations
and minimise unnecessary disruption to industry

Recent Rail Safety Data
�ATSB-published national regulator data for 2005-06:
-45 non-suicide deaths and 479 serious injuries
-121 running line derailments
-206 running line collisions (112 with infrastructure, 54 with
persons, 16 with rollingstock, 14 other trains, 10 road vehicle)
- 78 level crossing collisions (71 of which with road vehicles)
-457 signals passed at danger
-519 loading irregularities
-1084 track/civil infrastructure irregularities.

Inter-modal context
�Annual rail deaths about the same as in aviation and marine
�Road deaths by comparison are now around 1600 annually
�Rail, bus and low capacity regular public transport air travel are about equally safe based on passenger kilometres travelled and about 5 times safer than car travel
�High capacity regular public transport air travel in Australia has zero fatal accidents in the jet age
�Motorcycle travel is 28 times less safe than car travel (ie about 140 times less safe than rail).

Enhancing Rail Safety Data
�Rail regulators in jurisdictions will provide the ATSB with rail
safety data for calendar 2001 to calendar 2006 for publication
before the end of June 2007
�Regulators are working with the ATSB and NTC on broader,
more strategic and useful data including with causal factors to
enable pro-active analysis
�After some false-starts, there appears to be goodwill to make
substantial progress as required by Ministers and COAG

Levels of analysis

Investigation report findings
�Contributing safety factors
�Other safety factors
–Other safety factors identified during investigation which are considered important
�Other key findings
–Resolve significant ambiguity or controversy
–Discuss potential scenarios
–Positive factors which ‘saved the day’

ATSB safety action activities
�Critical safety issue:
–Communicate concern immediately
– If safety action not prompt, issue recommendation
�Significant safety issue:
–Communicate concern as soon as reasonable
�Minor safety issue: communicate with operator via
regular liaison and if safety action taken, record results

ATSB Recommendations
� Not enforceable (we do not place ourselves in the
position of a quasi regulator)
� Close liaison with regulators and operators for periodic
updates of implementation progress
� Non-prescriptive - ie identify the safety issues and
recommend “review” so that the organisation which
carries the risk is selecting/implementing the “fix”
� Early communication of safety issues so that “good
news” may be included in final report – a win/win.

Pre – July 2003
�ATSB investigation by invitation from State governments
�Usually the more serious accidents and provides more independence
�Conducted under State Legislation provided ‘no blame’ (could only help Waterfall Commission obtain investigation experts)
�Phased out when TSI Act in place (DIRN focus) and NSW developing capacity

Beresfield (NSW) – 23 Oct 1997 Zanthus (WA) – 18 Aug 1999
Ararat (VIC) – 26 Nov 1999

Key safety findings: Beresfield
�coal train collision with rear of another
coal train after failed to comply with
caution & stop signals
�3 locos & ten coal wagons derailed
�3 serious injuries (2 crew; 1 @ station)
�fatigue, system intolerant of human
error, inadequate safety defences

Key safety findings: Zanthus
�Indian Pacific directed into standing
freight train at low speed
�crew member of freight train pushed
a button which moved the points
and couldn’t reverse the mistake
�systemic vulnerability & human error
�safety action: interlock system &
new procedures to prevent repeat

Key safety findings: Ararat
�In this case a Freight Victoria employee
moved points diverting grain train into yard to
collide with stationary ballast train
�unsafe & unauthorised: ‘trying to be helpful’
�system vulnerability & human error
�training, control, system design, hazard
identification and risk management needed

Wodonga (VIC) – 25 Apr 2001 Footscray (VIC) – 5 June 2001
Black Mountain (QLD) – 1 Jul 2001

Key safety findings: Wodonga
�Countrylink XPT derailment on sharpest curve on
Sydney-to-Melbourne main line in Wodonga
�condition of high rail fasteners resulted in gauge
widening of up to 49mm at point of derailment
�also bogie thin wheel flange & issues with yaw
friction pads
�the combination led to derailment

Key safety findings: Footscray
�empty suburban electric express train collided with back of a suburban passenger train when driver impaired by medical condition/asleep
�‘deadman’s handle’ could be bypassed
intentionally or by weight of lower leg
�health standards to assess driver health were deficient (chronic sleep problems, medication)
�also signal & train stop system issues and train system radio network reliability

Key safety findings: Black Mountain
� QR runaway coal train hauling 120 wagons
during steep descent of Connors Range
�At 93 km/h front of consist with 28 wagons
separated & 74 wagons, 2 remote locos & the
electric locomotive control unit derailed
�extra errant O-ring reduced braking by over half
�also issues re communications & dataloggers

Epping (VIC) – 18 Jun 2002
Benalla (VIC) – 13 Oct 2002
Salisbury (SA) – 24 Oct 2002

Key safety findings: Epping
�scheduled suburban electric passenger train 60 km/h
on up journey SPAD - collided with scheduled
suburban empty train 12 km/h on a down journey
�up driver unwell (migraine, stress) - no recall 1 minute
�signalling system couldn’t maintain minimum safety
margin to prevent the collision
�deadman’s handle (pilot valves) ineffective again

Key safety findings: Benalla
�passive level crossing accident involving a loaded B-double and a passenger steam train
�B-Double driver didn’t see train before crossing
�train driver, fireman, and a footplate visitor died, one serious injury
�Victoria’s TOR focus on rail not B-Double
�recommendations included reviewing level crossings on B-double routes, track sighting, and education program

Key safety findings: Salisbury
�passenger train collided with a car and Serco
bus in which 4 killed and 26 injured
�road vehicles had queued across an active
level crossing and could not exit tracks
�this was forseeable as it occurred regularly

Spencer Street (VIC) – 3 Feb 2003
Chiltern (VIC) – 16 Mar 2003
Aloomba (QLD) – 23 May 2003

Key safety findings: Spencer Street
�driverless empty suburban train rolled away
while driver using the amenities and travelled
about 17 kms at speeds of over 100 km/h
�after near miss with previous passenger train
and at many level and pedestrian crossings,
finally collided with stationary passenger train
at Spencer Street station at 75 km/h
�safety action included park brake and
procedures when changing ends

Key safety findings: Chiltern
�PN freight train carrying steel etc derailed as a result
of a ‘screwed journal’ on a wagon that had been in
storage for several years
�a V/Line passenger train on the broad gauge
collided with the wreckage
�maintenance schedules for the journal bearing on
the failed axle were based on distance travelled not
both distance and time
�deficiencies in comms between control centres

Key safety findings: Aloomba
�passive level crossing accident when a local woman
stopped her car ‘in automation’ mode and drove in
front of 80km/h Sunlander passenger train
�7 year old killed and 5 year old seriously injured
�safety recommendations included reassess level
crossing upgrade program

Post – July 2003
�Increasing number of DIRN-only investigations:
Budget resourced for about 10 new per annum
�Now do non-DIRN if Ministerial request & under TSI
Act; eg because no assured funding from
jurisdictions to enable training of extra staff
�OTSI followed best practice independent model
after Waterfall changes; & VIC subsequently
�legislation review likely by other jurisdictions/NTC

Bates (SA) – 9 Nov 2003
Ararat (VIC) – 28 Nov 2003
Sandgate (NSW) – 25 Feb 2004

Key safety findings: Bates
�PN derailment at 77 km/h after axle separated
and ‘screwed off’ due to heat plasticising roller
bearing
�probable water ingress via suboptimum storage
�radius of roller bearing unit at opposite end of
failed axle was out of specification and rusty

Key safety findings: Ararat
�PN freight train derailed 2 wagons after
traversing buckled rail which was made
progressively worse as train passed over it
�found probably tamping a week before altered
geometry of track and lowered stress free
temperature to below 38C

Key safety findings: Sandgate
�empty Endeavour passenger train stopped 75m
short of collision with stationary loaded coal train
after points placed in wrong position
�signaller distracted and did not apply blocking
facilities or check route thoroughly
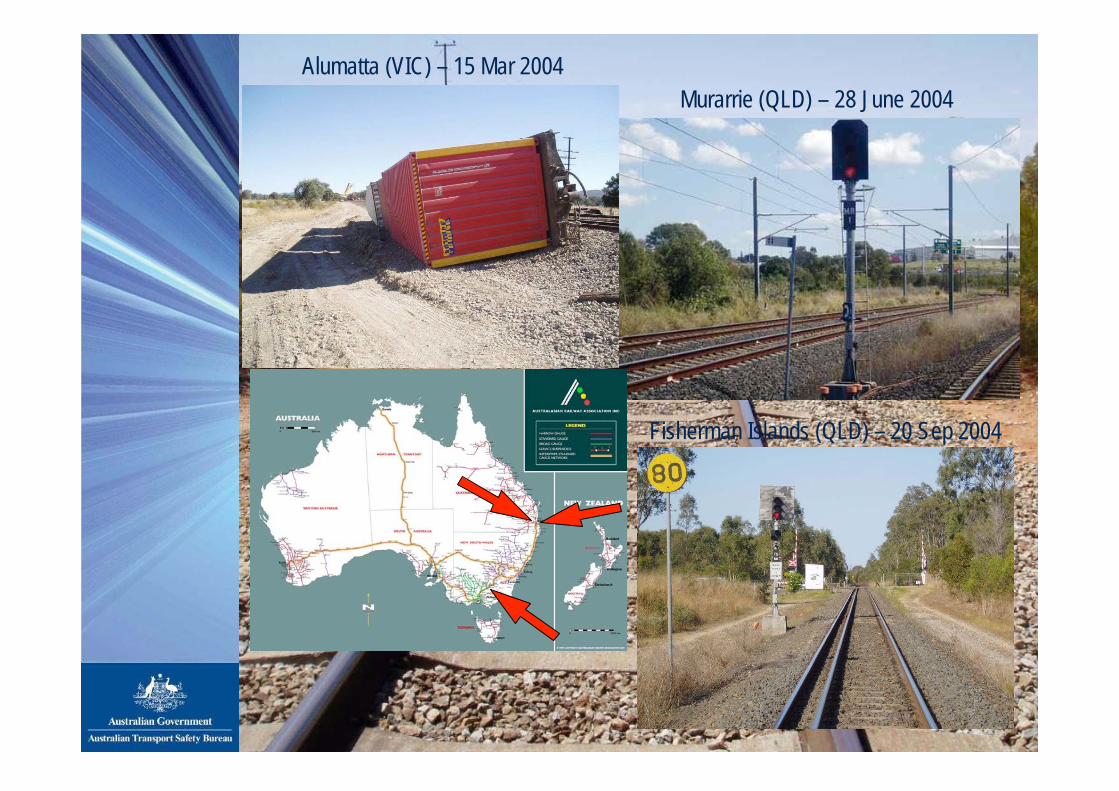
Alumatta (VIC) – 15 Mar 2004
Murarrie (QLD) – 28 June 2004
Fisherman Islands (QLD) – 20 Sep 2004

Key safety findings: Alumatta
�derailment of trailing bogie of 2nd to last wagon of
Freight Australia train departing crossing loop due
to combined track geometry and excessive speed
�travelled almost 5km in derailed state through 4
level crossings and a bridge at up to 69 km/h
�issue of broad gauge only metres from standard but
operated independently and poor communications

Key safety findings: Murarrie
�freight train SPAD when driver passed stop
while said retrieving a dropped radio hand-set
�train controller absent from workstation so 16
second delay while colleague dealt
�driver had a history of SPADs and died of
severe coronary 4 months after this one
�issue that not monitored or supervised after
previous SPADs, and QR medical standards

Key safety findings: Fisherman Islands
�freight train SPAD when driver fell asleep
and half woke and applied full power
�realised signal red and cars on level crossing but only stopped 74 metres beyond
�unclear if microsleep episodes based on
personal or task induced fatigue
�system vulnerable to such error in terms of
track and train secondary protection and
fatigue management standards and policy

Benalla (VIC) – 23 Sep 2004
Thornton (NSW) – 11 Oct 2004
Berajondo (QLD) – 15 Nov 2004

Key safety findings: Benalla
�4 of 15 Freight Australia wagons carrying dry
bulk cement derailed
�80km/h temporary speed restriction in place
due to weak track structure and geometry
was still too high given deteriorated track

Key safety findings: Thornton
�derailment of last 7 of 54 loaded coal wagons
due to combination with track
�gauge widening due to poor rail fastener
condition and asymmetric wheel wear

Key safety findings: Berajondo
�tilt train with 150 pax and 7 staff derailment at 112km/h on 60km/h curve
�lead car and 7 trailer cars derailed and only trailing power car remained upright
�driver distracted and lost position awareness while co-driver in adjacent vestibule
�QR was in process of reviewing advance speed boards to give drivers warning of speed reductions of over 40 km/h; and intended to expand use of Automatic Train Protection

Glenalta (SA) – 21 Nov 2004
South Dynon (VIC) – 19 Jan 2005
Koolyanobbing (WA) – 30 Jan 2005

Key safety findings: Glenalta
�PN freight train 10 wagons derailed in Adelaide
Hills with 5 obstructing broad gauge passenger
track and 4 down into residential properties
�likely triggered when wheel made contact with
check rail at entrance to Belair crossing loop
�4 factors combined including 3 empty wagons
behind locos; followed by 2900 tonnes; use only of
dynamic braking down descent; track geometry

Key safety findings: South Dynon
�two wagons of a PN freight train propelled at 9
km/h into the side of an XPT passenger train
running on the main line at about 13 km/h
�trainee marshalling freight wagons did not have
a clearly specified task or role or supervision
�also issue with performance of catch points

Key safety findings: Koolyanobbing/Booraan
�two PN freight train derailments (23 & 19
wagons) within an hour of each other 200 &
360km west of Kalgoorlie when track 18-21
degrees hotter than 40C design neutral temp
�both in vicinity of rural road level crossings
�track misalignment via buckle worsened by
passage of trains �for Koolyanobbing, track tamping on morning
probably contributed

Booraan (WA) – 30 Jan 2005
Regency Park (SA) – 2 Feb 2005
Horsham (VIC) – 11 Aug 2005

Key safety findings: Regency Park
�SCT employee directing shunting of a
locomotive and 9 wagons seriously injured
�either shunter fell from wagon end step or
slipped as trying to get on step
�procedures allowed this with no confirmation
by driver that shunter safe before starting

Key safety findings: Horsham
�active level crossing collision fatally injuring car
driver hit by PN locomotive which then derailed
�local driver probably did not expect train, and
possible personal distraction issues
�intersection after crossing may also have
distracted the driver
�recommendations included education and
awareness of level crossing safety and risk

Greenbank (QLD) – 25 Aug 2005
Eden Hills (SA) – 30 Sep 2005
Lismore (VIC) – 25 May 2006

Key safety findings: Greenbank
�freight train collided at 22km/h with a stationary
track vehicle at take-off point in station yard
�QR controller had not expected simultaneous
arrival because of trainee teaching distractions,
and ambiguous communication re departure
�track workers saw and heard train but thought
they would reach the take-off point and remove
the track vehicle before the train arrived

Key safety findings: Eden Hills
�out of gauge steel plate on PN freight train had
shifted from at least Murray Bridge before hitting
a TransAdelaide passenger train in Adelaide Hills
�ARTC track at Eden Hills station platform 140mm
closer to TransAdelaide track than design
�safety recommendations included steel tensile
strapping and improved load audit procedures

Key safety findings: Lismore
�passive level crossing accident between a rigid
tipper truck with quad axle trailer loaded with
citrus pulp and freight train travelling at 112km/h
�heavy fog, truck driver killed, and 41 of 64
wagons derailed
�truck not being driven according to conditions but
if it had stopped, longer time to cross so risk
remained unless active crossing greater warning

Inverleigh (VIC) – 25 Sep 2006
�26km/h impact by train
due to outer flag
position & late braking

Ongoing Investigations
� NT
– Elizabeth River
– Ban Ban Springs
� SA – Adelaide
– Tailem Bend
– Tarcoola
� VIC – Benalla
– North Geelong
– Seymour
– Wingeel
� NSW – Albury
– Harden
– Illabo
– Yerong Creek
– Back Creek

Yerong Creek (NSW) – 4 Jan 2006
Harden (NSW) – 9 Feb 2006
Adelaide (SA) – 28 Mar 2006

Ongoing investigations
�Yerong Creek – 9 wagons derailed,
track damage and closed 48 hours
�Harden – XPT derailment & power
car axle broken; 8 others cracked
�Adelaide – SPAD in yard damaging
54 points and potential collision with
Indian Pacific on DIRN

Benalla (VIC) – 2 Jun 2006
Albury (NSW) – 5 Jun 2006
Seymour (VIC) – 12 Sep 2006

Ongoing investigations
�Benalla – Interail freight train derailment
�Albury – car driver killed in active level
crossing accident involving XPT
�Seymour – derailment involving a Patrick
train

Tailem Bend (SA) – 4 Oct 2006
Elizabeth River (NT) – 20 Oct 2006
Ongoing investigations
�Tailem Bend – level crossing with stop
sign: train collision with prime mover/low
loader
�Elizabeth River – level crossing collision
between south bound freight train and
double-trailer road train

North Geelong (VIC) – 26 Oct 2006
Tarcoola (SA) – 1 Nov 2006
Illabo (NSW) – 2 Nov 2006

Ongoing investigations
�North Geelong – PN freight train collision with
‘bucket truck’ doing bridge works
�Tarcoola – Freightlink derailment after brake
pipe air lost
�Illabo – level crossing collision when train
collided with overturned semi trailer loaded
with wool bales

Wingeel (VIC) – 15 Nov 2006
Ban Ban Springs (NT) – 12 Dec 2006

Ongoing investigations
�Wingeel – level crossing collision: rigid tipper
truck and ‘dog’ trailer at passive crossing with
GSR Overland hauled by PN. Truck driver fatal.
�Ban Ban Springs – level crossing collision:
empty double-trailer road train drove into path of
Ghan derailing both locomotives & 10 wagons

Back Creek (NSW) – 10 Mar 2007

Ongoing investigations: Back Creek
�level crossing collision
�semi-trailer loaded with hay hit by
PN grain train at passive crossing
�truck driver fatality, one train driver
broken ribs, other minor injuries
�truck, 3 locomotives and ten span
bridge destroyed/burnt out

Conclusion re safety investigations
�I hope that this quick review has demonstrated a substantial
record of safety investigations and action, especially given
the dearth of other publicly reported investigations from 1999
�particularly proud of my team’s work on medical standards,
pilot valves, the need for better and standardised
communications, human error-tolerant systems, and level
crossing risk-based treatments and broader education

Rail Safety and Sustainability
�In conclusion, many lessons from best practice investigation
�Important these publicised to enable learning and change
�Good safety practices make good business sense
�A robust safety management system is key (safety culture)
�Australia’s rail safety record is good but can be improved
�One major accident can have disastrous consequences.

Further information
www.atsb.gov.au

Thank you for your attention
Rail 2007
Kym Bills Executive
Director ATSB
3 April 2007





























