Embed Size (px)
Citation preview

Veteran Centered CareVeteran Centered CareNew Models of Care and Emerging Nursing Roles
Alan Bernstein MS, RNOffice of Nursing g
Services
1

Veterans Health Administration (VHA)VISION STATEMENTVISION STATEMENT
VHA ill ti t b th b h k f llVHA will continue to be the benchmark of excellence and value in health care and benefits by providing exemplary services that are both patient centered p y pand evidence based.
This care will be delivered by engaged, collaborative teams in an integrated environment that supportsteams in an integrated environment that supports learning, discovery and continuous improvement.
It will emphasize prevention and population health p p p pand contribute to the nation’s well-being through education, research and service in national emergenciesemergencies.
2
Vision of VHA Preventive Care Program
The Veteran will experience health promotion and disease prevention (HPDP) clinical interventions that are seamlessly integrated across the continuumthat are seamlessly integrated across the continuum of their health care and are delivered in a variety of modalities matched to the Veteran’s needs and preferences VHA clinicians and clinical supportpreferences. VHA clinicians and clinical support staff will value and participate in the delivery of HPDP interventions for patients tailored to each Veteran’s priorities and overall plan of care.
3

VHA Facilities Statistics (as of 5/11/11)
• Medical Centers: 152• Medical Centers: 152
• Community Living Centers 330
• Community-Based Outpatient Clinics: 798
• Veteran Readjustment Centers: 278
4

2010 VA Population Statistics (as of 9/30/10)(as of 9/30/10)
• U.S. Veteran Population: 22.7 millionU.S. Veteran Population: 22.7 million91.9% males8 1% females (projected to reach 15% by8.1% females (projected to reach 15% by
2035)
• VHA Statistics:Enrolled Population: 8 3 millionEnrolled Population: 8.3 million Outpatient Visits: 76 million Inpatient Admissions: 680 millionInpatient Admissions: 680 million
5

Veteran Period of Service Statistics (as of 9/30/10)9/30/10)
• Vietnam Era: 7.5 million• Peacetime only: 5.8 million• Gulf War: 5.7 million• Korean Conflict: 2.4 million• WWII: 2 million• Post 9/11 [Operation Enduring Freedom
(OEF) / Operation Iraqi Freedom (OIF) / Operation New Dawn (OND)]: 1.3 million
[Note: Categories are not mutually exclusive[Note: Categories are not mutually exclusive. Veterans may serve in multiple periods.] 6

VA Health Care Utilization: Post 9/11
OEF / OIF / OND Veterans:• Approximately 2.2 million have deployed since
2002• 1,250,663 have separated from service and
are eligible for care• 50% (625,385) of these have obtained VA
health care since FY 2002 (cumulative total)
7

What are the health care needs of our returning combat Veterans?returning combat Veterans?
8

What are the health concerns of OEF/OIF/OND veterans seen in the VA?of OEF/OIF/OND veterans seen in the VA?
1 250 663 f th 2 2 illi d l d t d d li ibl f VA1,250,663 of the 2.2 million deployed, are separated and eligible for VA50 % have been seen in VA between FY02 and December 2010
• Musculoskeletal 54.3%• Mental disorders 50.2%• Symptoms/signs 48.7%
N t (h i ) 42 0%• Nervous system (hearing) 42.0%• GI (dental) 35.1%• Endocrine/Nutrition 29.1%• Injury/Poisoning 27 3%Injury/Poisoning 27.3%• Respiratory 24.5%
VHA Office of Public Health and Environmental Hazards December 2010
9

Co-morbid Concerns in Combat Veterans
Lew, Otis, Tun, Kerns, Clark, & Cifu, in reviewSample = 340 OEF/OIF outpatients at Boston VA
TBI/Pain12.6%
P3 Multi‐symptom
5.3%10.3%
symptomDisorder42.1% 16.5%6.8%
Overall prevalence:Pain 81.5%TBI 68 %
PTSDTBI 68.2%PTSD 66.8%
2. %
10

Integrated Post-Combat CarePDICI (Post Deployment Integrated Care Initiative 2008)PDICI (Post-Deployment Integrated Care Initiative 2008)
PhysicalPhysical Psychological Psychological
Veteran
Psychosocial Psychosocial
11
Integrated Post-Combat CarePDICI (Post-Deployment Integrated Care Initiative 2008)PDICI (Post Deployment Integrated Care Initiative 2008)
Primary CarePrimary CarePrimary Care Primary Care ProviderProvider
Mental HealthMental HealthProvider Provider
Veteran
Social WorkerSocial Worker
12

Health Care Reform and
N iNursing
13

National Discussion
Healthcare Reform• Lower Healthcare Costs• Provide Affordable and Accessible Health
Insurance Coverage• Promote Prevention and Stress Public Health
14

National Discussion on the Future of NursingNursing
Nursing Shortage AgendaNursing Shortage
• Nursing Faculty• Nursing Workforce
g
• Lower Costs• Population Management• Nursing Workforce
Nursing Practice
Population Management• EBP• OutcomesNursing Practice
• DNP• CNL
• Quality and Safety• Access
• Informaticist• Certification
• Prevention• Primary Care
15

VA Nursing:VA Nursing: Influencing national
i inursing practice
16

Institute of Medicine (IOM)The Future of NursingThe Future of Nursing
• Affordable Care Act (ACA)• Accessible Quality Care• Wellness• Disease Prevention• Interprofessional Collaboration• Value of Service• Responsive to needs• Patient Centered
17

Institute of Medicine (IOM)The Future of Nursing – Key MessagesThe Future of Nursing Key Messages
• Practice to the full extent of education • Achieve higher levels of education• Full partners in redesigning healthcare• Improved data collection and information
infrastructure
18
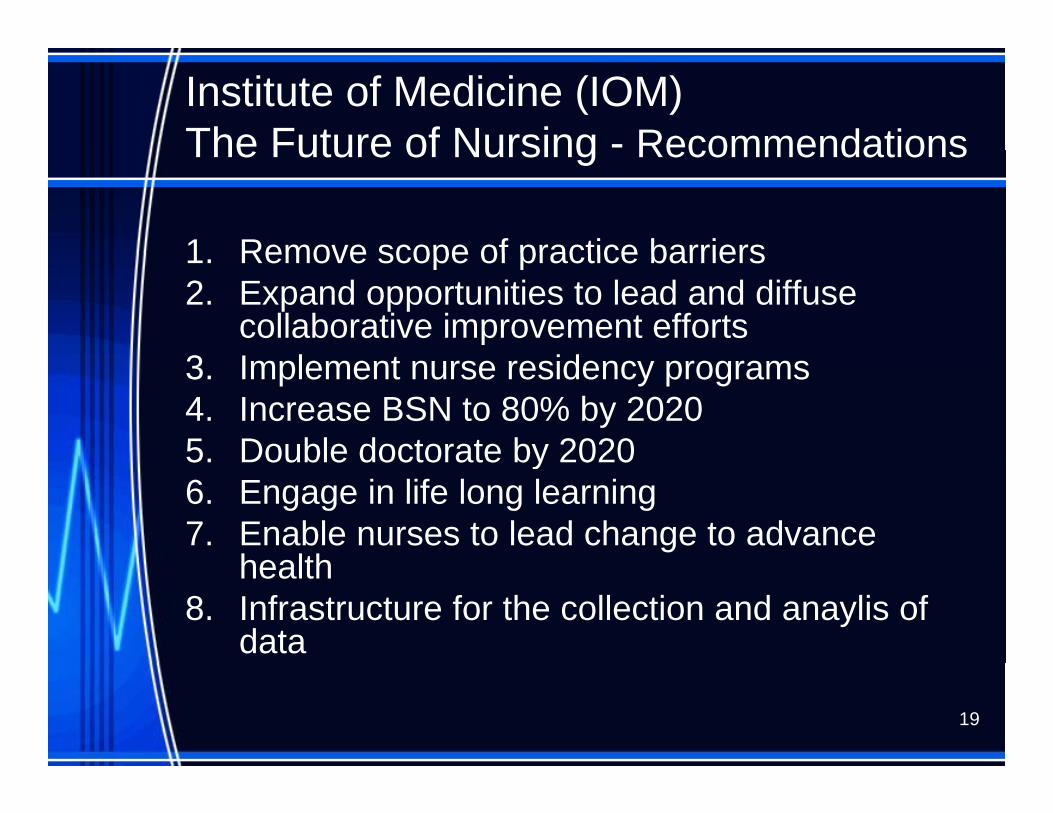
Institute of Medicine (IOM)The Future of Nursing - RecommendationsThe Future of Nursing Recommendations
1 Remove scope of practice barriers1. Remove scope of practice barriers2. Expand opportunities to lead and diffuse
collaborative improvement efforts3 I l t id3. Implement nurse residency programs4. Increase BSN to 80% by 20205 Double doctorate by 20205. Double doctorate by 20206. Engage in life long learning7. Enable nurses to lead change to advance
healthhealth8. Infrastructure for the collection and anaylis of
data
19

VA Advanced Practice Registered Nurses (APRN):Registered Nurses (APRN):
Nurse Practitioners (NP), Clinical N S i li (CNS) dNurse Specialists (CNS), and
Certified Registered Nurse gAnesthetists (CRNA)
20
APRN Practice
• All VA APRNs will function as• All VA APRNs will function as independent professionals
dl f th St t i hi h thregardless of the State in which they are licensed. The intent is to reduce variability in
practice across the entire VA healthpractice across the entire VA health care system.

APRN Practice
• Core privileges are based on education and tifi ti d i l dcertification and include:
Admitting and discharging privilegesBasic primary and emergency careOrdering/interpreting diagnostic studies
( di l d l b t di )(radiology and lab studies)Referrals and consultations
• Additional privileges are based on request and demonstration of competencyand demonstration of competency
22

VA Registered Nurses (RN):VA Registered Nurses (RN):Clinical Nurse Leaders, Primary Care RN, Care Managers, Nurse
Informaticists and Tele-Health RNsInformaticists and Tele Health RNs
23

Th Cli i l N L dThe Clinical Nurse Leader: Clinical leadership across the p
continuum of care
24

Clinical Nurse LeaderClinical Nurse Leader
Fi t t ’ d i lFirst new master’s prepared nursing role introduced in 35 years.
• A direct care provider prepared to deliver clinical leadership in all health care settings.
• The goal :Reduce fragmented careReduce fragmented care, Improve patient outcomes, and Increase patient safety/satisfaction at theIncrease patient safety/satisfaction at the
Microsystems level25

The CNL Role Is:
Unit-based (the Microsystems level)level)
A staff nurse
A generalist--not a specialistA generalist--not a specialist26

The CNL is not: A Nurse Manager
• No administrative function
• Provides clinical leadership and direct care for the most complex patientsp
27

The CNL is not: A Shift Charge NurseNurse • The shift charge nurse is
concerned with:The completion of tasks for patients duringThe completion of tasks for patients during
the shiftEnsuring that staff have the resources they g y
need to complete all patient care on the shift
• The CNL observes patient care practices and utilizes evidence-practices and utilizes evidencebased care to improve care 28

The CNL is not: A Clinical Nurse SpecialistSpecialist
• The CNS is a population specialist
• A CNS’ impact is greatest working at the Macrosystems level (across the entire facility) y)
29

The CNL is not: A Nurse EducatorEducator
A N Ed t ’ i• A Nurse Educator’s primary function is staff education
• A Nurse Educator works with the• A Nurse Educator works with the CNL to design/provide staff
d ti t h ti teducation to enhance patient care outcomes
30

The CNL is not: A Case ManagerManager
• A Case Manager’s emphasis is on• A Case Manager s emphasis is on the medical plan of care to ensure
ti it fcontinuity of care: Post-discharge Among multiple providers and care
settings, andg ,Ensure the patient’s care is
uninterrupteduninterrupted31

The CNL is not: A Discharge PlannerPlanner• The Discharge Planner works with
the CNL and Case Manager to ensure the patient:ensure the patient:Is transferred to the appropriate care
setting upon dischargesetting upon dischargeHas the necessary supplies and equipment
for home care
• The CNL participates and may lead discharge planning for selectdischarge planning for select patients 32

GI Protocol
• CNS • CNL– Developed protocol
• Approval by hospital administration
– Identified need for a protocolC di t d t ffadministration
– Conducted staff education
– Coordinated staff education
– Implemented protocol– Developed criteria for
quality monitoring– Revised protocol
– Conducted quality monitoring
– Evaluated resultsRevised protocol based on evaluation
– Evaluated results
33

Staff Education: Insulin
• CNS • CNL– Identified problem– Conducted staff
d ti i
– Coordinated staff educationC d t d liteducation sessions
– Developed criteria for quality monitoring
– Conducted quality monitoring
– Evaluated QM results– Evaluated QM results – Conduct ongoing staff
education sessionseducation sessions
34

Potential CNL Outcomes:
Reduce Falls Monitor care ofand Pressure Ulcers
Monitor care of complex patients
Teach /mentor novice nurses in
Evaluate pain management innovice nurses in
all specialty caremanagement in elderly post-ops
Successful diabetic self-
t
Coordination of care between
ttimanagement care settings35

D t t d CNL O tDemonstrated CNL Outcomes: Quality, Financial, and InnovationQ y, ,
36

CNL Outcomes
Domain Indicator Outcome
Financial Nursing Hours Per Patient Day (NHPPD)
Increased by 8.63% within 1yr
Q lit 1 Pressure Ulcers Decreased from 12 5% toQuality Processes
1. Pressure Ulcers
2. Patient Falls
Decreased from 12.5% to 4.2% Decreased from 1.93 to 1.37 in 3 months
3. Discharge Teaching
4. Ventilator Associated Pneumonia
Increased compliance from 13% to 100%
Decreased from 21.7% to 8 7%Pneumonia
5. CLC Restorative Care Factors
8.7% Increased by 8% in the 1st
month
Innovations Journalized CNL entries in innovative practices
Revealed team collaboration to reducein innovative practices collaboration to reduce care fragmentation, customize care, & engage MDs
37

Colonoscopy Screening CancellationsCancellations
• CNL assessed high rate of no-shows and cancellationsCNL t t d ti t t fi t t d• CNL contacted patients to confirm tests and review pre-procedure instructions
Results:N h t d d fNo-show rate decreased from
30% to 14%
38

Ambulatory Surgical Procedure CancellationsProcedure Cancellations
• Assessment of cancellations revealed patient-related reasons (not NPO; need topatient related reasons (not NPO; need to reschedule)
• CNL confirmed pre-op date/instructions prior to posting surgery scheduleprior to posting surgery schedule
Results:14 4% cancellation rate in 2006 dropped14.4% cancellation rate in 2006 dropped
to 11.4% in 2007 at an estimated cost-avoidance of $462KCancellation rate in 2008 dropped toCancellation rate in 2008 dropped to
9.4%CNL continued to improve surgical
efficiencies in collaboration with anefficiencies in collaboration with an interdisciplinary group
39

Innovations
• New Initiatives• Evidence-Based Practice Activity• Staffing Changes• Role Conversions• Changes in Staff Skills• Education Mix• Academic Affiliations
40

Th RN C M R lThe RN Care Manager Role in the Primary Care Patient Aligned y g
Care Team (PACT) Model
41

PCMHFour Major Operational ComponentsFour Major Operational Components
CareTeam Function
and Culture
Care Coordination &
Care Management
PatientPatient CenterednessCenteredness
g
EnhanceEnhance Access Enhance
Coordination Enhance EfficiencyEnhance
Comprehensive Care 42

Primary Care Team Functions
•Comprehensive Care Delivery
Professional Development
Care Coordination
AdministrativeSupport
Organizational Management
Face -to-Face Encounters
Program Management
Non Face- to Face-Encounters
Encounters g
Team Management
TASKSa age e t
•RN Care ManagerS i l W k
•Facility L d hi
•Clerk •LPN
•The Team•Teamlet
•Social Work•Specialists•Providers
Leadership•PC Management
•LPN•Health Tech/ NA
•The Team•Teamlet 43

PatientPatient Aligned Care TeamAligned Care Team
RN Care ManagerRN Care ManagerCNLCNL VeteranVeteran NPNP CNS
Direct Patient Care•Provides specialty
Direct Patient Care•Scheduled, walk in or urgent Visits
Schedule appointments
Direct Patient Care•Scheduled visits•Telephone Visits
Direct Patient Care•Scheduled Clinic Visits•Walk in /Urgent Visits
assessment and care.
Secure Messaging•Triage messages from patients•Email with/from other
urgent Visits•Group/telephone Visits•Triage/protocol orders•Pt Education
Secure Messaging•Triaged messages from
appointmentsAs needed or requested by primary care team
Appt check inUtilizes kiosk to
•Telephone Visits•Assess educational level of pts/families to create self‐mgmt strategies•Inpt/home visitsW k ith PCMH
Walk in /Urgent Visits•Group / Telephone Visits•Clinical Reminders
Secure Messaging•Triaged pt messages •E‐mail with consultants
•Email with/from other consultants
Care Management•Consulted by RN Care Manager or CNL for
•Triaged messages from patients•E‐mail with consultants
Care Management•Virtual/F2F in‐depth and ongoing pt review
•Utilizes kiosk to check in •Updates insurance & demographic info
Face to Face VisitsBring medications
•Work with PCMH vulnerable populations
Secure Messaging•Triaged pt messages•E‐mail w/consultants
Care Management•Virtual review of pts including inpatients •Identify high risk for hosp.•For CCHT, OEF/OIF, HBPC•Preventive care needs g
specialty assessment •Provide assistance with plan of care development•Coordinate/Conduct group visits with specialty
ongoing pt review including inpatients •Identify high risk for hospitalization.•Initiate consults for CM, home care, hospice, specialty nursing care
•Bring medications•Health risk assessment completion w/ RN•Complete Lab work
P f Vi it
Care Management•Needs assessment of the PCMH organization•Revise protocols•Track/trend disease data to improve pt
•Non VA records•View alerts•Diagnostic result•Discuss care with/refer to specialty consultants•Traveling veterans•Medication Reconciliation
populations•Identify additional services needed by Veteran/Family
TeamWork
specialty nursing care•Preventive/DM care •F/U VA & non‐VA care
Team Work•Daily huddle•Team Meeting
Prepare for Visit•Discuss concerns and plan of care•Contact team w/concerns
P ti i t
p poutcomes•Identify strategies to improve RN practice•Applies EBP to RN care
Team Worki
Medication Reconciliation•Refer as appropriate
Team Work•Daily huddle•Team Meeting•Physician collaboration
Team Work•Team meetings
Education•Augment pt teaching
•Team Meeting
Education•Mentor/precept nurse trainees
Participate•Committees & pt
•Team Meetings
Education•Mentor RN Care Mgr•Precept nurse trainees
Education•New patient orientation•Provider CME , Grand Rounds•Teaching trainees
44

Patient Complexity Health Status NeedsPatient Complexity Health Status NeedsPatient Complexity, Health Status, NeedsPatient Complexity, Health Status, Needs
Medical Home Team Specialty Care
Clinical Nurse Clinical Nurse Leader,Leader,
Case Managers, Case Managers, Clinical Clinical
PharmacistsPharmacistsCoordination
of Careof Care
Management of CareManagement of Care
Disease/Cohort ManagementDisease/Cohort Management
Management of CareManagement of Care
45

Provider/RN Care ManagerClinical TasksClinical Tasks
Direct Patient Care C M tDirect Patient Care
• Scheduled Clinic Visits• Group Visits
Care Management
• Virtual review of patients• Identify high risk for p
• Telephone Visits• Incoming calls• Walk in or Urgent Visits
y ghospitalization
• Determine appropriateness for CCHT, OEF/OIF, HBPC Pre enti e care needs• Pertinent Clinical Reminders
• Ordering diagnostic tests• Ordering consults
O d i di ti
• Preventive care needs • Non VA records • View alerts • Diagnostic result• Ordering medication • Diagnostic result • Discuss care with/refer to
specialty consultants • Traveling veterans g• Medication Reconciliation
46
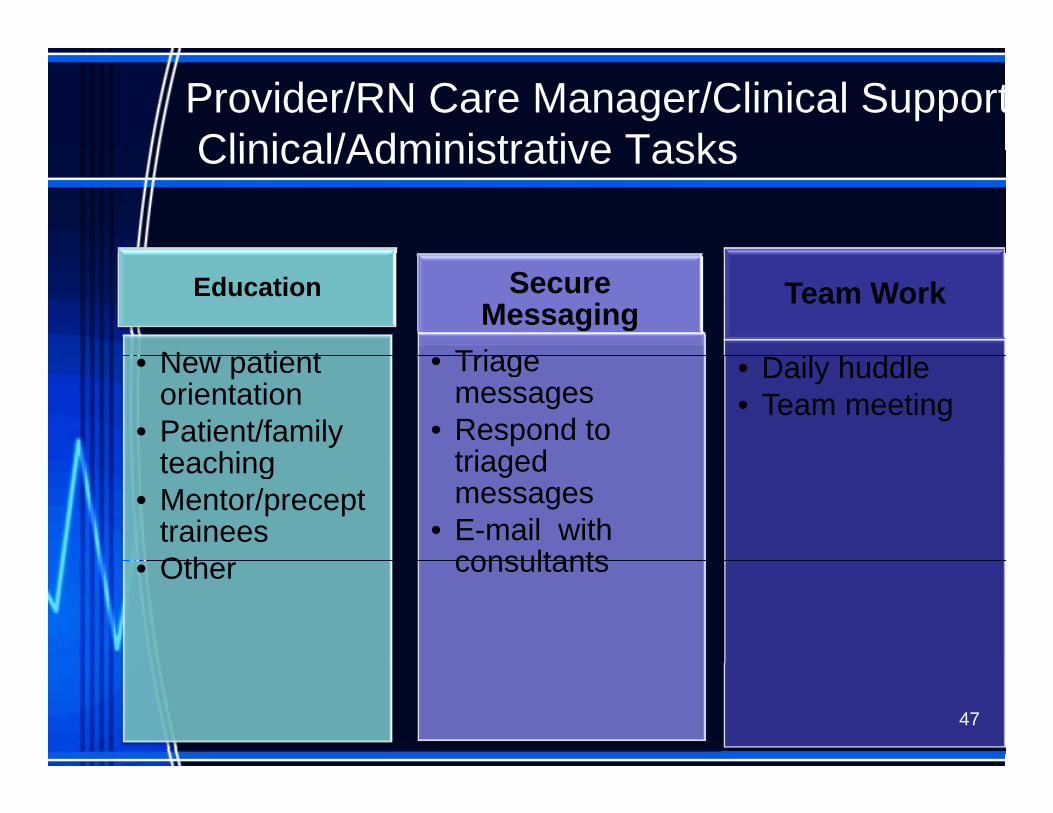
Provider/RN Care Manager/Clinical SupportClinical/Administrative TasksClinical/Administrative Tasks
Education
N ti t
Secure Messaging
Triage
Team Work
• New patient orientation
• Patient/family teaching
• Triage messages
• Respond to triaged
• Daily huddle • Team meeting
teaching • Mentor/precept
traineesOth
triaged messages
• E-mail with consultants• Other consultants
47

RN Care Manager Role and RN Care Manager Role and ResponsibilitiesResponsibilitiesResponsibilitiesResponsibilities
• “Gatekeeper” for all care needsGatekeeper for all care needs• Knows the role of the teamlet and team members• Applies critical thinking skills to identify barriers to
care• Promotes patient and staff safety• Collaborates with the pt/family, teamlet andCollaborates with the pt/family, teamlet and
expanded team to develop the patient-driven holistic care plan
• Smooth transitions by collaborating with• Smooth transitions by collaborating with multidisciplinary services, internal and external
• Education/Coaching to support self-management, ti d ll b d ti t lprevention, and wellness, based on patients goals
48
PACT RN Care Manager
Providing the right care at the right time by th i ht t th i ht lthe right person at the right place
• Puts Veteran and family at the center and they are engaged and share in decisionthey are engaged and share in decision making and goal setting
• Coordinates care and facilitates care plan• Coordinates care and facilitates care plan • Assure that all Veterans have info and
access to VA system/PACT and theaccess to VA system/PACT and the OEF/OIF/OND program
• Keeps all members of the Veteran’s teamKeeps all members of the Veteran s team on the same page
49

PACT RN Care Manager
Providing the right care at the right time by the right person at the right place
• Partners with OEF/OIF/OND team to assure d t d di t dneeds are met and care coordinated
• Understands resources and how to accessF ili l h d ff• Facilitates seamless handoffs
• Facilitates shared decision making• Assures that Veteran knows who is on the
team• Promotes health and well being reaching out
to nurture relationships 50

Patient Aligned Care TeamPatient Aligned Care Teamfor Returning Combat Veteransfor Returning Combat Veteransfor Returning Combat Veteransfor Returning Combat Veterans
Patient centered, team based, integrated careEvidence based continuously improving careEvidence based, continuously improving care
CommunicationCommunication
Combat Veteran Care/Case Manager
Collaboration Coordination
P t C b t C PACT f dPost-Combat Care moves our PACTs forwardThe PACTs move our Post-Combat Care forward 51

Implications for RN Care Managers
• Coordinate HPDP services for patient panel
• Offer and provide other clinically appropriate preventive services (screening tests, other health behavior counseling, immunizations and preventive medications)and preventive medications)
E d h lth li i d• Endorse healthy living messages and respond to questions from patients
52

Support for RN Care Managers
• Training Programs and Support in• Training Programs and Support in Patient-Centered Communication– Patient Education: TEACH for Success– Motivational Interviewing
• Tools and Resources– Websites (www.prevention.va.gov)– Clinical staff reference tools– Patient tools– Patient tools– Documentation tools– MOVE! Weight Mgmt. Program – Facility HPDP Program Committee
53
Clinical Staff Guide to Healthy Living MessagesMessages
54

Clinical Staff Guide to Health Coaching
55

Coming Attractions: Healthy Living MaterialsLiving Materials
56

Nurse Informaticists:
ADPAC – Automated Data Processing Applications Coordinatorpp
CAC – Clinical Applications CoordinatorPI/IS Coordinator PerformancePI/IS Coordinator – Performance
Improvement/Information Systems CoordinatorCoordinator
BCMA Coordinator – Bar Code Ad i i t ti C di tAdministration Coordinator
57

Nursing Informaticists
• Nursing Informatics integrates nursing science, computer andnursing science, computer and information science and cognitive science to manage communicatescience to manage, communicate and expand the data, information, k l d d i d f iknowledge and wisdom of nursing practice.
• ( ANA 2008) 58
Nurse Informaticists
“Computers are incredibly fast, accurate
and stupid. Human beings are incredibly p g yslow, inaccurate and brilliant. Together they are powerful beyond imagination.”y p y g
Albert Einstein
59

Telehealth Nursing
• The use of information and communication technology to deliver health services, expertise and information over distance
• Constant with the principles of primary healthcarehealthcare
Di ti di i d• Disease prevention, diagnosis and treatment 60

Telehealth Nursing
• Assessment and triage• Provision of health information• Provision of health information• Health counseling and teaching• Elicit patient concerns• Listening and providing support• Listening and providing support
61

Other Roles to Consider
• Travel Nurse– OR– Pediatrics
Critical Care– Critical Care• Nurse Educator
MSN– MSN– PhD, DNP
• Nurse Administrator• Nurse Administrator– Nurse Manager– CNO
62