Benign biliary disease Dr. Gili Halfteck Department of General
Surgury Shaare Zedek Medical Center January 2014
Slide 2
Anatomy
Slide 3
Slide 4
Slide 5
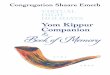
Calots triangle
Slide 6
Physiology Roles of bile secretion: 1.Excretion of toxins and
cellular metabolites (bilirubin) 2.Lipids absorption Components of
bile: 1.Bile salts 2.Lipids (phospholipids and cholesterol)
3.proteins 4.pigments
Slide 7
Bile flow
Slide 8
Stimuli of bile secretion 1.Vagal activity 2.Secretin 3.CCK
(bile secretion and gallbladder wall contraction)
Slide 9
Slide 10
Fasting state: -entero-hepatic circulation -Accumulation of
bile in the gallbladder -Retrograde filling of the gallbladder -
tonic activity of the sphincter of Oddi Fed state: -CCK (acid, fat
and protein in duodenum) -Vagal activity
Slide 11
Symptoms of biliary tree disease Pain Fever Juandice
Slide 12
Pain Biliary colic Usually constant pain Location:
RUQ/epigatrium Can be associated with meals (1 hour or more after a
meal) Caused by contraction of the gallbladder against an
obstructed neck Stasis + pressure + bacterial inoculum infection
and inflammation (RUQ tenderness on palpation) Murphys sign
Slide 13
Fever Accompanies infection and inflammation of the gallbladder
or biliary tree Not present in biliary colic
Slide 14
Juandice Elevation of serum bilirubin Surgical (obstruction) /
medical (hepatocellular) >2.5 mg/dl scleral icterus >5 mg/dl
cutaneous juandice Pathogenesis: failure to excrete bile from the
liver to the intestine Charcots triade: fever, RUQ pain, juandice
Reynolds pentad: + hypotension and altered mental status
Imaging 1. US study of choice for initial evaluation of
jaundice and gallbladder or biliary disease Surgical/medical
jaundice High sensitivity and specificity for gallstones
Slide 17
2. HIDA (hepatic iminodiacetic acid) scan Nuclear medicine test
demonstrated physiologic bile flow but does not provide anatomic
delineation Failure to fill the gallbladder 2 hours after injection
cystic duct obstruction (cholecystitis) Obstruction of the biliary
tree, bile leaks
Slide 18
3. CT scan Superior anatomic information Most gallstones are
isodense to bile Identifies cause and site of biliary obstruction
Preoperative planning in pancreatic/hepatic neoplastic processes 4.
MRI/MRCP Superior anatomic definition of intra- and extrahepatic
biliary tree and pancreas Non-invasive No radiation exposure
Slide 19
Slide 20
5. ERCP (endoscopic retrograde cholangiopancreatography)
Invasive test using endoscopy and fluoroscopy Contrast injection
through the ampulla and imaging of the biliary tree Able to
diagnose and treat many biliary tree diseases (choledocholithiasis,
tissue sampleing, CBD stenting) Complication rate - 10%
Slide 21
Bacteriology Without previous biliary intervention bile is
considered sterile The presence of gallstones or obstruction and
stasis increases the likelihood of bacterial contamination Mostly
gram-negative aerobes passage of bacteria upward from the duodenum
into the biliary tree E. Coli, Klebsiella, Enterobacter,
Enterococcus spp.
Slide 22
Gallstones Types: 1.Mixed stones (70%) cholesterol and calcium
2.Pure cholesterol stones (10%) 3.Pigment stones brown/black (10%)
Gallstones formation: -Supersaturation of bile -Concentration of
bile in the gallbladder -Crystal nucleation -Gallbladder
dysmotility
Slide 23
Natural history of gallstones Vast majority are asymptomatic
incidentale finding Biliary colic temporary obstruction of the
cystic duct or gallbladder neck 1% of patients with asymptomatic
stones develop complications before onset of symptoms -
prophylactic cholecystectomy is not warranted High risk patients:
-Hemolytic anemias -Porcelain gallbladder -Large (>2.5 cm)
stones -Long common channels of bile and pancreatic duct -Bariatric
surgery (sleeve, bypass) -Immunocompromised patients
Slide 24
Non-operative treatment of cholelitiasis Generally
unsuccessfull and rarely used!!! -Oral dissolution -Contact
dissolution -Shock-wave lithotripsy Up to 50% recurrence rate
Slide 25
Acute calculus cholecystitis Pathogenesis: unresolved cystic
duct obstruction Inflammation, edema, subserosal hemmorhage
Infection of stagnant bile pool Can progress to ischemia and
necrosis (gangrenous cholecystitis) Presentation: -Fever -RUQ pain
-Tenderness to palpation Laboratory finding: leukocytosis, mild
elevation of bilirubin, transaminases, alk-phos.
Slide 26
diagnosis 1. Transabdominal US -sensitive, inexpensive and
reliable -Sensitivity 85%, specificity 95% -Gallstones, gallbladder
wall thickening, pericholic fluid, sonographic murphys sign 2. Hida
scan -Atypical cases -Cystic duct obstruction 3. CT scan - Less
sensitive then US
Slide 27
Treatment NPO IV fluids IV antibiotics (broad-spectrum) Pain
control Cholecystectomy (open/lap.) Percutaneous
cholecystostomy
Slide 28
Chronic cholecystitis Inflammation and scarring of the
gallbladder neck and cystic duct Pathogenesis: recurrent biliary
colic which cause temporary cystic obstruction and do not cause
acute cholecystitis Presentation: recurrent biliary colic (usually
after fatty meals), nausea, vomiting RUQ/epigatric pain radiating
to the scapula, usually resolves within few hours Symptomatic
cholelithiasis indication for chlecystectomy
Slide 29
Diagnosis History Transabdominal US stones, sludge Treatment
Elective cholecystectomy Curative in > 90% of patients
Slide 30
choledocholithiasis 1.Primary common duct stones -De novo in
the bile duct -Usually brown pigment stones -More common in Asian
population -Associated with bacterial bile duct infection 2.
Secondary common duct stones -Arising from the gallbladder -Most
common bile duct stones in the USA Retained common duct stones
found within 2 years of cholecystectomy
Slide 31
Presentation 80-90% of common duct stones remain clinically
silent Routine cholangiography 10% choledocholithiasis Selective
cholangiography (pain, abnormal liver function test) 1-2% of
patients will present with retained stones Symptoms: -Biliary colic
-Obstructive juandice -Ascending cholangitis (fever, pain,
juandice)
Slide 32
Diagnosis Hepatic function panel abnormalities Leukocytosis US
choledocholithiasis, biliary ductal dilatation, gallstones Bile
duct dilatation (>8 mm) in the presence of biliary colic,
juandice or gall stones is suggestve of choledocholithiasis ERCP
-highly sensitive and specific -Usually therapeutic
-Sphincterotomy, balloon stone extraction -Complication rate 5-8%
MRCP - highly sensitive and specific - Does not provide therapeutic
solution
Slide 33
treatment 1.ERCP -Sphincterotomy and stone extraction -Reasons
for endoscopic failure: large stones, multiple stones, intrahepatic
stones, altered anatomy, duodenal diverticula, impacted stones
-Does not eliminate the risk of recurrent biliary stone disease (up
to 50% recurrence) 2.Common bile duct exploration (lap./open)
-Intraoperative cholangiogram -Trans-cystic/common duct
incision
Slide 34
Ascending cholangitis Acute ascending bacterial infection of
the biliary tree cause by obstruction Obstruction: stones,
malignancy Presentation: Charcots triad (fever, RUQ pain,
jaundice), Reynolds pentad (+hypotension, altered mental
status)
Slide 35
Diagnosis Tachycardia, shock symptoms Laboratory test:
leukocytosis, abnormal liver panel US dilatation of the biliary
tree CT site of obstruction ERCP/PTC diagnostic as well as
therapeutic
Slide 36
Treatment NPO IV fluids IV antibiotics Most patients respond to
medical therapy Emergent decompression of the biliary tree
(ERCP/PTC)