Embed Size (px)
Citation preview


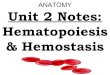
Antithrombin III
pro th rom bin * th rom b in
fib rinog en
F ibrin m onom er
F ib rin po lym erC L O T
*X a
X
X III X IIIa
*IX a
IX
*X Ia
X I
*X IIa
X IIW O U N D surface
*ka llik rein
k in inog en (H M W K )
prekallik re in
Va
V IIIa V III
V
Intrinsic p a thwa y
C o m m o np a thwa y
= C a lcium & P L com plex
* = ac tive serine p ro tease

Protein C system
pro th rom bin * th rom b in
fib rinog en
F ibrin m onom er
F ib rin po lym erC L O T
*X a
X
X III X IIIa
*IX a
IX
*X Ia
X I
*X IIa
X IIW O U N D surface
*ka llik rein
k in inog en (H M W K )
prekallik re in
Va
V IIIa V III
V
Intrinsic p a thwa y
C o m m o np a thwa y
= C a lcium & P L com plex
* = ac tive serine p ro tease
Thrombin + thrombomodulin
Protein CaProtein C + protein S
Cleaves Factor Va and VIIIa

Thrombin-activatable fibrinolysis inhibitor (TAFI)
Thrombin + thrombomodulin
Removes the terminal lysine on the fibrin molecule, renders the clot more susceptible to lysis by plasmin

Degradation of the Fibrin Clot Natural part of hemostasis Fibrin fibrils in the clot are dense,
dissolution occurs at “coiled coils” to form oligomers which are digested into smaller units
Highly regulated in terms of gene expression Plasmin
Tissue plasminogen activator (t-PA) urokinase streptokinase

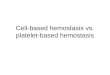
Plasminogenesis
C O O H
S
SArg
Va l
C O O H
S
S
Arg
Va l
p la sm inogen
t-PA(end o th e liu m )
p la sm in
NH 2NH 2
(k id n ey )u ro k in a se
(e x o g e n o u s)s tre p to k in a se
F ib rin c lo tF ib rin fragm en ts
2-an tip la sm in

Plasmin
Serine protease formed from plasminogen Plasminogen found in plasma and
extracellular space and has high affinity for fibrin
Inactive and requires activation to plasmin by urokinase and t-PA
Formation of plasmin is highly regulated Cleaves fibrin into degradation products. Circulating plasmin is inhibited by α2-
antiplasmin. Forms complex with plasmin and prevents it from
binding to fibrin

Tissue Plasminogen Activator Serine protease released from ECs in response
to injury (in response to thrombin and some vasoactive peptides)
Chiefly responsible for conversion of plasminogen to plasmin
Secretion highly regulated at transcriptional level
Major binding is to fibrin clots and extracellular matrix
Highly specific ( site of clot formation ) Inhibited by plasminogen activator inhibitor-1
(PAI-1) Recombinant protein used clinically to inhibit
thrombosis

Urokinase
Serine protease secreted as pro-urokinase Produced by endothelial cells, fibroblasts, and
monocytes/macrophages Potent plasminogen activator but non-specific secreted as one chain: fragments in urine
generated by plasmin Functions to degrade ECM, enabling cells to
migrate Half life of only 7 minutes Inhibited by plasminogen activator-2 (PAI-2) synthesis tightly regulated by cytokines and
inflammatory mediators Used clinically (e.g. Abbokinase)

Streptokinase
Protein isolated from certain types of streptococci bacteria
Potent plasminogen activator Less selective than t-PA Can result in circulating plasmin Can produce degradation of fibrinogen
as well as fibrin May result in formation of plasmin in
excess of that inhibited by α2-antiplasmin and result in bleeding

BECAUSE OF THE COMPLEX NATURE OF HEMOSTASIS, POTENTIAL
INTERFERENCE IN THE PROCESS CAN OCCUR AT MANY LEVELS.

HEMOSTATIC DEFECTS
CONGENITAL Coagulation Factor deficiency
Hemophilia von Willebrand’s disease Factor XI,II, V, X, XIII deficiency
Platelet function defects Glanzmann’s thrombastenia Bernard-Soulier syndrome Storage pool disease

HEMOSTATIC DEFECTS
Major surface protein abnormality Glanzmann’s thrombastenia
Glycoprotein IIb / IIIa Absence of platelet aggregation
Bernard-Soulier syndrome Glycoprotein Ib / IX / V Absence of platelet adhesion

HEMOSTATIC DEFECTS
ACQUIRED Platelet abnormalities quantitative defects
failure of production Bone marrow disorder
shortened survival ITP / DIC
Sequestration hypersplenism

Conditions of Excess Bleeding Hemophilia ( inherited sex-linked rec.
) Hemophilia A (classic)- deficiency of
Factor VIII (85%) Hemophilia B – deficiency of Factor IX
(15%) Spontaneous bleeding
Joints frequently, crippling arthropathies Retroperitoneal hematoma Gastrointestinal/ genitourinary
NORMAL PLATELET FUNCTION

Conditions of Excess Bleeding von Willebrand’s disease
Autosomal dominant Low level of vWF
CARRIER FOR FACTOR VIII NORMAL PLATELET ADHESION
ABNORMAL PLATELET FUNCTION Easy bruising and mucosal bleeding
Menorrhagia is common

Conditions of Excess Bleeding
Thrombocytopenia Most common abnormality of hemostasis in
surgical patients Platelets fall from normal 150-400,000 to <
100,000/µl Massive blood loss Heparin induced Impaired platelet function Vit b12 / folic acid def ITP hypersplenism

Conditions of Excess Bleeding
Coagulopathy of liver disease Vitamin K deficiency
Required by liver for formation of prothrombin and Factors VII, IX, X and protein C
Leads to serious bleeding tendencies

Conditions of Clotting Dysfunction Thromboembolic conditions
Can result when endothelial surface is compromised or BF is slow
Associated with atherosclerosis, infection, or trauma
Femoral venous thrombosis When BF is slow (bed ridden, prolonged sitting) Clot grows and large piece can break off Can pass through right side of heart to lodge in
pulmonary arteries (pulmonary embolism) If large enough can be fatal

COAGULANTS
Thrombosis Inappropriate activation of hemostatic
mechanism; Venous –associated with stasis of blood
with small platelet component Arterial – associated with artherosclerosis
with large platelet component

COAGULANTS
Vitamin K Essential for the formation of clotting
factors (II, VII, IX and X) Given orally or thru IV (Natural Vit K
requires Bile-acid while Menadiol Na Phosphate does not but takes longer to act)
USE – bleeding 2o to oral anticoagulants, babies, Vit. K deficiencies

COAGULANTS
Antifibrinolytic Agent Tranexamic acid (Inhibit plasminogen
activation),for conditions with bleeding or risk of bleeding,life-threatening bleeding following thrombolytic drug administration and hereditary angioedema.
Aprotinin-inhibits proteolytic enzymes, used for hyperplasminemia due to fibrinolytic overdose & during cardiac
surgery

Conditions of Clotting Dysfunction Disseminated intravascular coagulation
Clotting activated in widespread areas Often from severe trauma or shock
(endotoxin) Plugging of vessels limits oxygen delivery lethal in ~85% of the cases

ANTICOAGULATION AND
BLEEDING

Prevention of Blood Clotting Critical for clots to dissolve or not form
when not neededEndothelial cell surface-
Most important factor – integrity prevents contact activation of intrinsic clotting system by collagen
Charged EC glycocalyx repels platelets and clotting factors
Thrombomodulin-EC membrane protein, binds thrombin to slow clotting process. Thrombomodulin-thrombin complex activates a protein C which inactivates Factors V and VIII.

Removal of Thrombin (blocks common pathway) Fibrin – absorbs 85-90% of thrombin by
absorption into fibers Anti-thrombin III – binds remaining
thrombin
Prevention of Blood Clotting

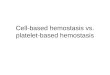
Vitamin K cycle (post-translational carboxylation)
NH
R
R
C H C H2 C H2
C = O
-C O 2
NH
R
R
C H C H2 C H
C = O
-C O 2
-C O 2
K (re d )
carboxylase
epoxidereductase
vitam in Kreductase
coum arin sK (e p o x )
K (o x )
C a
G L U res id u e
G L A res id u e
O + C O2 2 H O + H2+
D ie t Factors VII, IX, X and prothrombin


Anticoagulants for Clinical Use
Heparin Coumarins Aspirin
Cyclooxygenase inhibitor Prevents formation of thromboxane A2 and
activation of platelets Calcium-deionizing agents
Sodium, ammonium and potassium citrate combines with calcium in blood
Several factors require calcium for activation Used in test tubes to prevent clotting

Antithrombin III
pro th rom bin * th rom b in
fib rinog en
F ibrin m onom er
F ib rin po lym erC L O T
*X a
X
X III X IIIa
*IX a
IX
*X Ia
X I
*X IIa
X IIW O U N D surface
*ka llik rein
k in inog en (H M W K )
prekallik re in
Va
V IIIa V III
V
Intrinsic p a thwa y
C o m m o np a thwa y
= C a lcium & P L com plex
* = ac tive serine p ro tease

ANTICOAGULANT
Heparin -binds to antithrombin III Combines with anti-thrombin III and
increases activity 100-1000X Immediate effect ,half life of 60-
90min Monitor by aPTT

ANTICOAGULANT
Low molecular weight heparin- 4-6 kDa
Selective Xa inhibitor More favorable antithrombotic
effect,less bleeding,highly predictable bioavailability
Longer half life

ANTICOAGULANTS
Coumarin derivatives- warfarin,acenocoumarol,phenprocoumon
Block coagulation factors(2,7,9,10) Warfarin decreases formation of Factors VII,
IX and X by the liver Competes with vitamin K for reactive sites
Restoration after coumarin tx- 3-5 days Prothrombin time INR- corrects the differences of the
various thromboplastin activity. INR=1 no anticoagulation

ANTICOAGULATION
Antiplatelet Drugs Aspirin Dipyridamole Thienopyridine Derivatives Glycoprotein IIB/IIIA receptor antagonists Other antiplatelet drugs

ANTICOAGULATION
Antiplatelet Drugs Aspirin
Inhibits cyclooxygenase irreversibly Inhibits TXA2 Main drug – acute MI, High-risk for MI,
after coronary artery Bypass, after angioplasty, unstable coronary syndromes,TIA and AF if oral anticoagulant
is contraindicated

ANTICOAGULATION
Antiplatelet Drugs Dipyridamole
Phosphodiesterase inhibitor Additive effect to aspirin Less effective than aspirin Headache but no excess risk of bleeding

ANTICOAGULATION
Antiplatelet Drugs Thienopyridine Derivatives
Inhibits ADP-dependent aggregation Orally given, additive with aspirin Ticlopidine slow onset, unwanted effects-
blood dyscrasias (neutropenia) Clopidogrel – same as Ticlopidine except
for neutropenia

ANTICOAGULATION
Antiplatelet Drugs Glycoprotein IIB/IIIA Receptor Antagonists
Abciximab – for angioplasty patient as adjunct to heparin and aspirin, reduces restenosis, Tirofiban – an oligopeptide
Abciximab - Risk of bleeding & immunogenicity limits its use
They inhibit diverse agonists (e.g. ADP, TXA2 etc. )

ANTICOAGULATION
Thrombolytic agents- plasminogen activators.
Recombinant endogenous plasminogen activators(recombinant tPA)
Streptokinase- exogenous source bleeding

ANTICOAGULATION
Fibrinolytic Drugs Streptokinase
Protein extracted from cultures of streptococci
Activates plasminogen, given IV Additive with aspirin Action blocked by antistreptococcal
antibodies Allow 1 year before it can be used again

ANTICOAGULATION
Fibrinolytic Drugs Alteplase, Duteplase and Reteplase
Recombinant tPA (plasminogen activator) ‘Clot-selective’ – fibrin bound plasminogen Not antigenic-substitute for patients w/ ab
for streptokinase Reteplase –longer half-life, bolus
admn.simple

Tests of hemostasis
Primary deficiency/ defect in one component
Pharmacologic therapy Anticoagulant/ antiplatelet
Comorbid condition Thrombocytopenia Sepsis/ hepatic disease

Tests of hemostasis
Careful review of patient’s clinical history most important/ initial approach
Drug use Basic laboratory tests
Platelet count Prothrombin time ( PT ) or INR Activated partial thromboplastin time
( aPTT ) Bleeding time ( BT ) and clotting time
( CT )

Evaluation of surgical patient Patients history Questions to ask
Prolonged bleeding or swelling after biting the lip or tongue
Bruises without apparent injury Prolonged bleeding after dental extraction Excessive menstrual bleeding Bleeding problems associated with major and minor
operations Medical problems receiving a physician’s attention
within the past 5 years Medications including aspirin or remedies for
headache taken within the past 10 days Relative with a bleeding problem

Four levels of concern
Level I Hx(-); Sx (m) no test
Level II Hx(-); Sx (M) platelet ct
PTT
Level III Hx (suggestive) PT, PTT, BT, CT, pltelet ct
Level IV Hx(+)Hematologic consultation

Platelet dysfunction
Normal 150,000 to 400,000 /ul Clinical signs of thrombocytopenia
< 100,000 / ul Increased bleeding complications in major
surgical procedures < 50,00 / ul
Increased bleeding complications in minor surgical procedures
< 20,000 / ul SPONTANEOUS HEMORRHAGE

Platelet dysfunction
Bleeding time ( BT ) Evaluate platelet , vWD and vascular
dysfunction Several methods
Ivy test = 7mins
Clotting time ( CT ) … + Aspirin use

Clotting dysfunction
PT reagent contains thromboplastin and calcium + plasma =
clot PT measures
Factors I, II, V, X and VII Factor VII extrinsic pathway
Abnormal coagulation due to Vit K deficiency warfarin / coumadin therapy

Clotting dysfunction
Variations in thromboplastin activity from different sources PT value is adjusted = INR
ISI ( international sensitivity index ) Value for each batch of thromboplastin Optimal reagent has as ISI of 1.3 to 1.5
INR = ( PTpatient / PTnormal )ISI
INR- corrects the differences of the various thromboplastin activity. INR = 1.0 is NORMAL

Clotting dysfunction
aPTT reagent contains Phospholipid substitutes, activator and
calcium + plasma = clot aPTT measures
Factors I, II and V of the common pathway Factors VIII, IX, X and XII
intrinsic pathway Heparin therapy

HEMOSTASIS
RENE PSA MENDOZA, MD, MHSA
Associate Professor, Department of Surgery
FEU-NRMF Institute of Medicine