Embed Size (px)
Citation preview
Bedside Monitoring
Brian S. Rothman, MD Vanderbilt University Medical Center
November 13, 2014
1
© 2014 Association for the Advancement of Medical Instrumentation www.aami.org
1. CLINICAL NEED/RESULT: Why did you institute continuous monitoring of patients on opioids? What were the results you saw after implementing continuous monitoring? 2. SOLUTIONS/VENDORS: How did you implement continuous monitoring? Where did you start? How did you collection/analyze the data? 3. ALARM STRATEGY: How did your institution ensure continuous monitoring did not increase non-clinically actionable alarms? Was there a policy? Strategy? Clinical/Patient Education? 4.CHALLENGES/BARRIERS What are some challenges/barriers you experienced? How did you overcome these barriers? 5.ROI DATA What kind of data did you collect that demonstrates this was a sound investment? Please show in terms of dollars for decrease in ICU transfers/reduced LOS? How did you show improved patient outcomes? 6. INSTITUTIONAL STANCE Does your institution have a policy or stance on continuous monitoring of patients on opioids? Please insert stance or policy excerpt.
2
Acknowledgements
• Liza M Weavind, MBBCh., FCCM, MMHC
• Sharon Mullins, RN, BSN, MA
Clinical Need
Failure to Rescue • Healthcare systems safety target • Institute of Medicine • Anesthesia Patient Safety Foundation
• Definition(Silber, 1992) • Hospital death following an adverse occurrence..
• Retrospective reviews demonstrate adverse events are preceded by a period of physiologic instability 6- 8 hours prior to the event.
• Early recognition of such physiologic change prompts early intervention potentially minimizing the occurrence of escalation in care and adverse events. (Taenzer 2012).
Clinical Need
• No current continuous patient physiologic monitoring provision outside of the intensive care units
• General care floors • Continual monitoring, but • No continuous monitoring
Continual/Periodic Vital Signs
Like checking to see if the fridge light is on...
http://www.niemanlab.org/images/smart-refrigerator.jpg

Current State
http://4.bp.blogspot.com/_UD1TRPOssR0/RswK910GEUI/AAAAAAAAAIU/4CSLjP61NsE/s400/3+monkeys.jpg http://www.presspartners.org/wp-content/uploads/2013/05/monkeys_22027_lg.gif
Possible Ideal Future State
http://1.bp.blogspot.com/-rlT-Alch12M/T3S5ci84JdI/AAAAAAAAAUw/GtvGIv5lw3A/s1600/3monkeys.jpg
http://photos.merinews.com/upload/imageGallery/bigImage/1220001163553.jpg
Purpose & Objectives • Evaluate monitoring technology for its ability to
increase detection and intervention for patients showing early signs of decline • Impact on Patient Safety • Primary alerting of patients at the bedside • Transmission of data via Wi-Fi signal • Escalation of Alerts through paging system if not
resolved • Limitation of Alert fatigue by setting alarm
parameters and technology • Assess Nurse and Staff satisfaction
Implementation
Project • Implement a continuous physiologic
monitoring system and process for general care floor patients
• System facilitates early recognition of deterioration and cues rescue interventions
• Notifications to • Patient’s nurse via pager when limits
violated • Escalation if no nurse response
Operational Objectives • Pilot - Install continuous physiologic
monitoring system in selected units. • Parameters may include • Pulse oximetry • Heart rate • End tidal carbon dioxide (not included in
first phase) • Establish clinical alerting and escalation
model • Integration with nursing documentation
excluded
Technology • Covidien Vital Sync Monitoring Platform
with Nellcor pulseox probes • Measures patient vital signs • Delivers values to database • Algorithms to generate alerts
• Connexall Alert/Alarm System • Receives alerts from Covidien system • Delivers alerts and escalations
The Pilot - 2 General Care Floors • Design and configure hardware and software • Create and validate current and future business work flow
operational processes • Design and develop new incoming interfaces • Design and develop new outgoing interface • Create and execute a Testing Plan • Document and execute a Business Continuity Plan • Create and execute a Training Plan • Develop and implement a Go Live Plan • Transition the system to Support Teams post Go Live • Document Lessons Learned and create a Post Implementation
Review
Infrastructure and Maintenance
• Establish technical support model • Monitor data and alarms • Reporting (real-time, dashboard, etc.) • Retention
Institutional Support and Governance
• Project team and steering committee • Stay within scope

Alarm Strategy
Low Thresholds Wide Ranges
• Sufficient latencies offset artifacts
• Decreased false positives • Identify only those at risk regardless of
definition
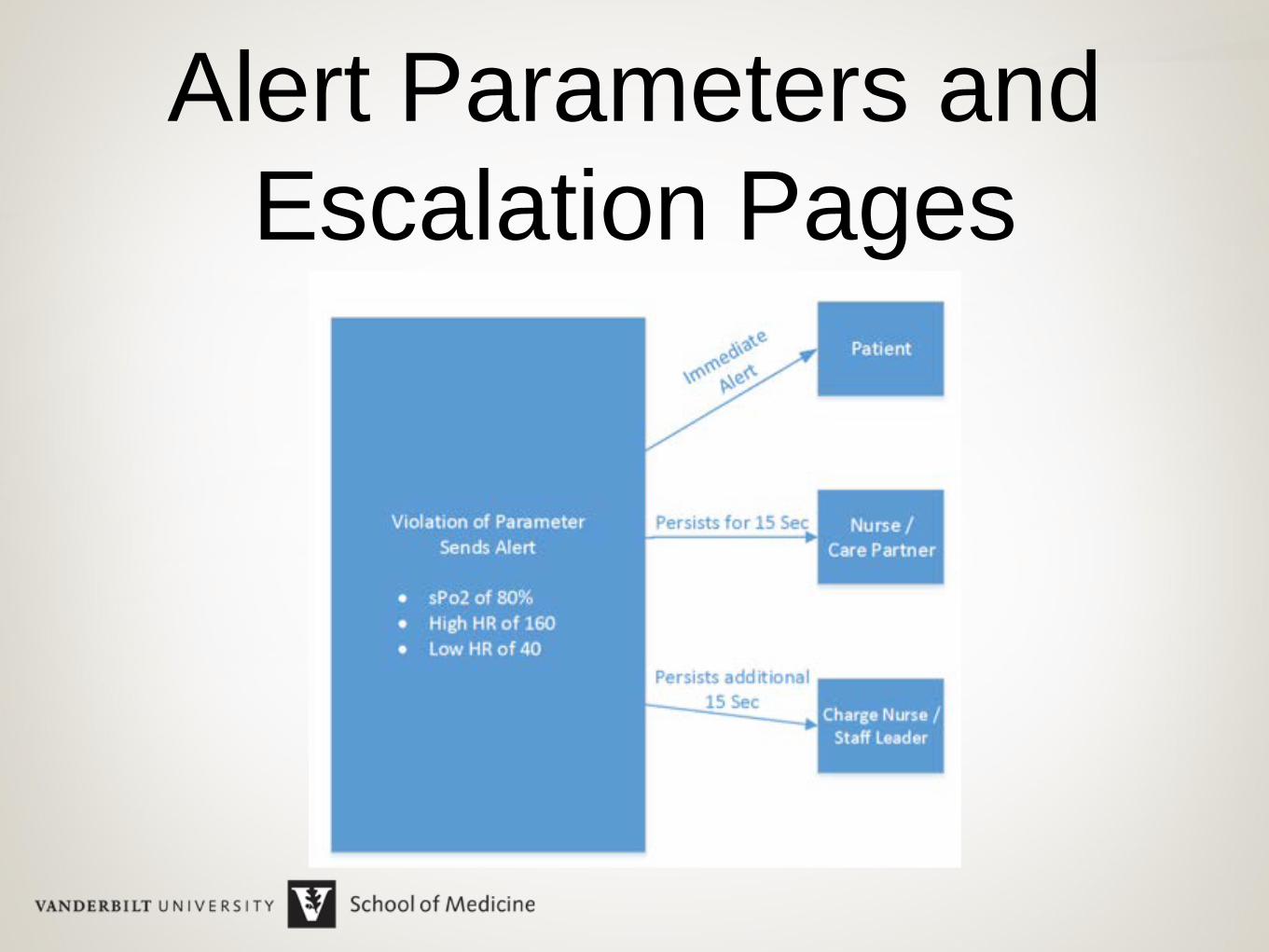
Alert Parameters and Escalation Pages
Challenges/Barriers
Data Retention Medicolegal Risk
• Benefits • Analysis • History and research
• Risks • Medicolegal discovery • PHI exposure (non-Medicolegal
discovery)
Data Retention • Policy creation • Retain what data • Identifiable data • Snapshot concept
• Multiple location data collection • One-size-fits-all? • Customized policy/case-by-case
exceptions
Assumptions
• WIFI can support • Increased use by new devices • Real-time data flow
• Sufficient storage available • Technology scalable from 2 floors to
over 300 beds
Don’t Assume
• WIFI connectivity issues • Thought to be vendor based
• Actually WIFI configuration issue -
improved WIFI performance house-wide
Technical Requirements Not Met • Connectivity was inconsistent • Monitors could not all be linked to
patients or staff • Escalation of alerts did not occur when
monitors not connected • Data collection ceased with Server
Failure • Reporting function was unavailable
Nursing acceptance
• Changing culture
• Support culture change
Nursing Identified Barriers
• Connectivity • Ergonomic Impact • Perceived unreliability • Usability of Software Programs • Lack of Support • Cleaning of Machines • Monitors were not available for all patients at
Risk • Negatively affected Patient Satisfaction

Nursing Identified Patient Satisfaction • Too many false positives when patient is using their hands
• Finger probe uncomfortable • Probe interferes with personal hygiene • Patients don’t see necessity- “I’m not
that sick” • Impedes ambulation and inhibits
mobility • Rooms are too crowded
Survey Bias • Negatively worded survey questions
predominant • Skewed values and comments - still
valuable • Used comments for final
implementation criteria • Met resistance when we tried to remove
monitors from pilot locations
Results
37 Year Old Male…
• HCV, GERD, chronic pain s/p MVA ‘97 (L4 paraplegia, loop ileostomy, sacral decub, osteomyelitis), multiple prior surgical procedures.
• POD 10 from gluteus maximus myocutaneous flap
• On pulse Ox with bedside pilot on 9S
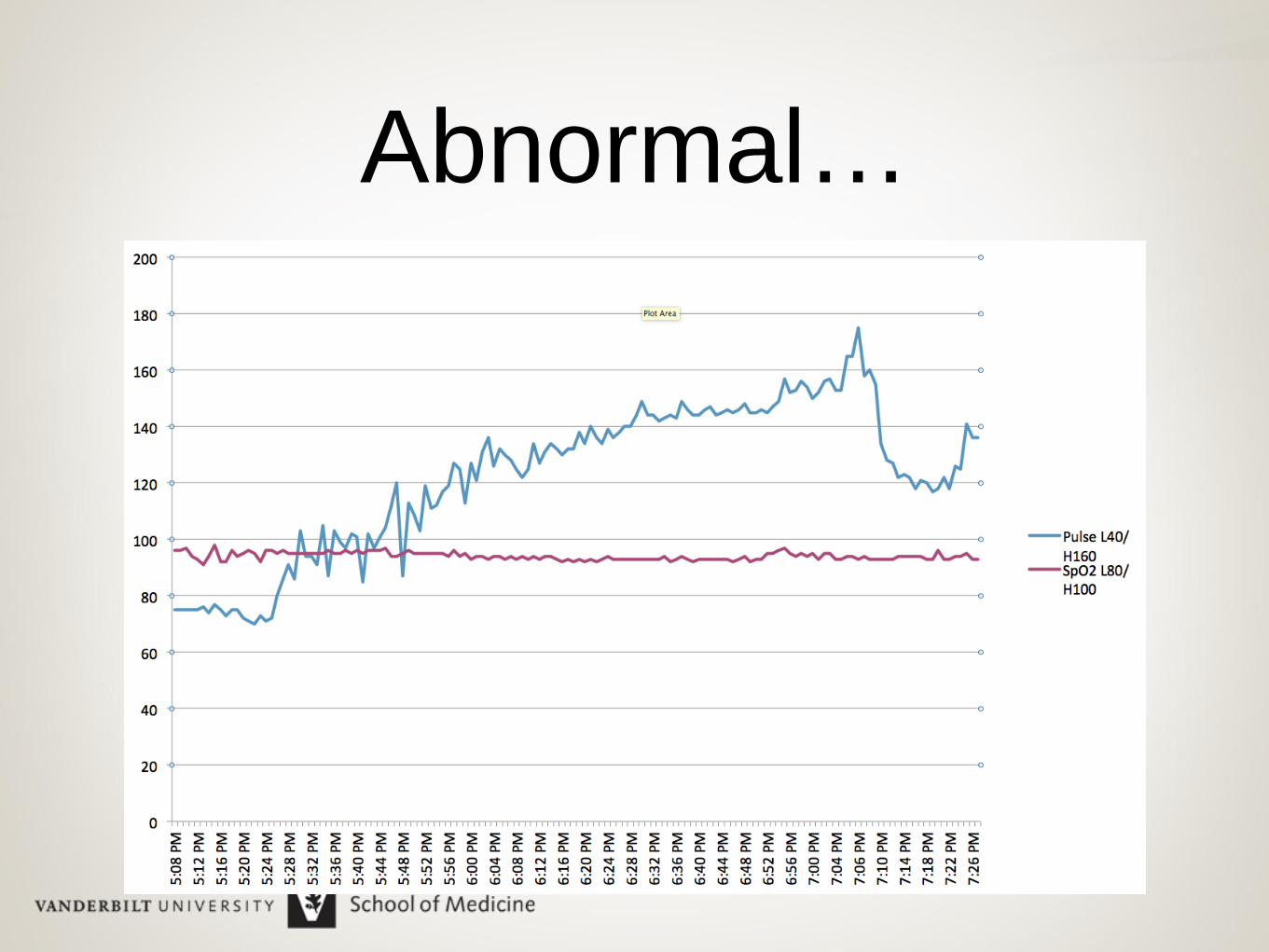
Abnormal…
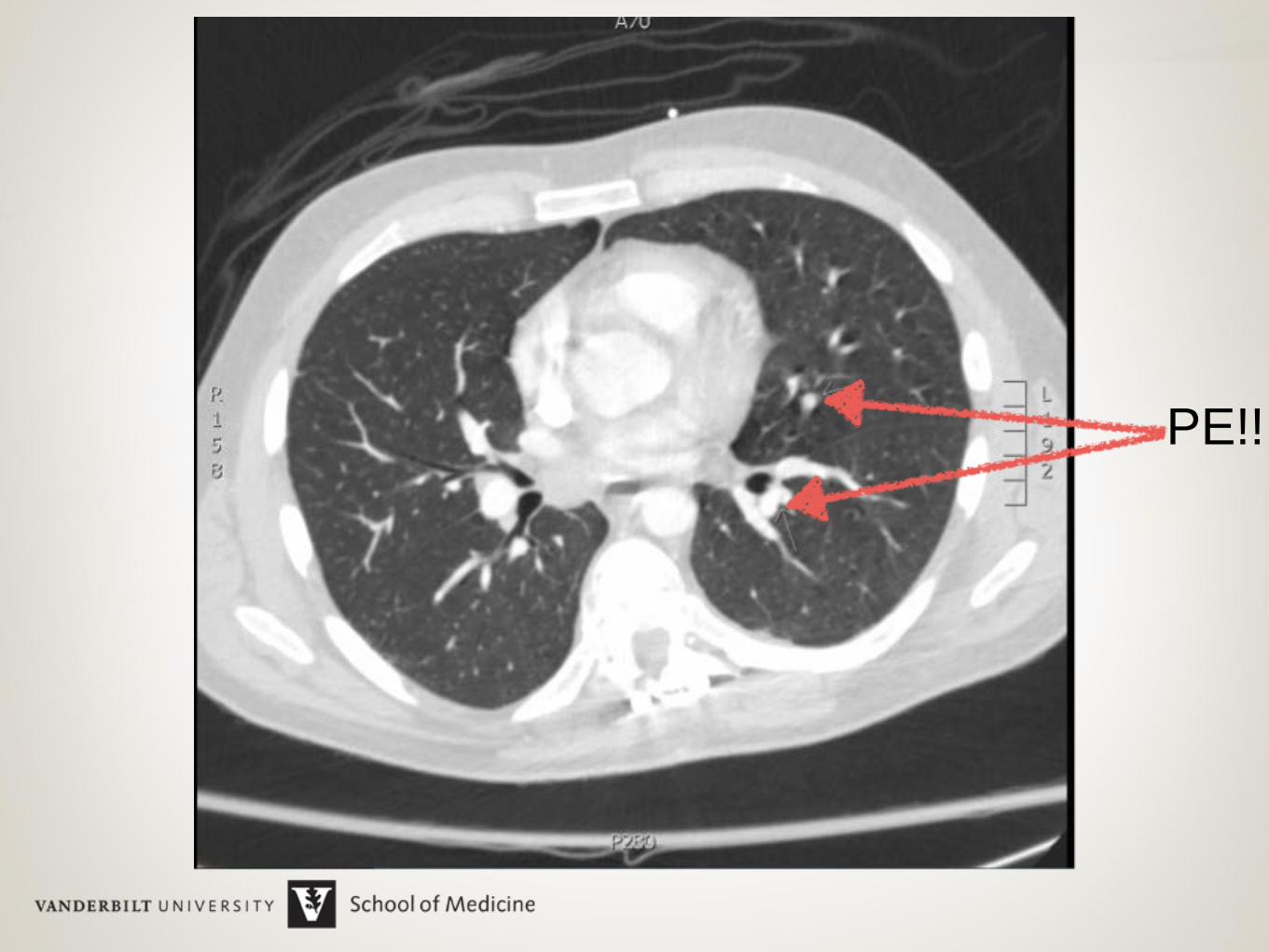
PE!!
Saves and Fewer RRT
• PE identified, treated, excellent outcome
• Hypoglycemia treated - no ICU transfer
• After pilot - new onset atrial fibrillation • Transfer and cardioversion
ROI
ROI Goals • Higher level of care transfer rate
reduction • Reduction in Rapid Response
Activations • ICU bed LOS decrease per 1000 pt
days • Decrease ED diversion from bed
availability
Value Trend
• 2 saves and decreased RRT calls • Fewer ICU admissions • Shorter LOS patients without care
escalation • Trend but insufficient power to show
significance
Non-Financial Quality Improvements • Improved Nursing Satisfaction • Decreased use of Narcan in units • Decreased code rate on surgical units • Identification of patients at risk for Obstructive
Sleep Apnea (OSA) • Earlier interventions and increased awareness • PCAs and epidurals
• Inconclusive
Institutional Position
No, But...
• Continual monitoring policy for patients • Upon initiation of PCAs • Basal rate addition, or • Continuous narcotic infusion
Implementation Planned January
2015