Embed Size (px)
Citation preview

Basal Bolus: The Strategy for Managing All Diabetes
Fall, 2003
Paul Davidson, MD, FACE
Atlanta Diabetes Associates
Atlanta, Georgia

ACE / AACE Targets for Glycemic Control
HbA1c < 6.5 %
Fasting/preprandial glucose < 110 mg/dL
Postprandial glucose < 140 mg/dL
ACE / AACE Consensus Conference, Washington DC August 2001

Step Therapy
Diet
Exercise
Sulfonylurea or Metformin
Add Alternate Agent
Add hs NPH
Switch to Mixed Insulin bid
Switch to Multiple Dose Insulin
Utilitarian, Common Sense, RecommendedProne to Failure fromMisscheduling and Mismanagement

Stumble Therapy
YAG Diet
Golf Cart Exercise
Sample of the Week Medication
– Interupted,
– Not Combined
Poor Understanding of Goals
Poor Monitoring
HbA1c >8% (If Seen)
Informed Patient Refers Self Elsewhere

PETS TherapyStep--Spelled Backwards
All at once, nothing first, Just like bubbles, when they burst.
Start with Fast to Glucose <126 mg/dL
– Glargine, Wt x 0.1 units qd Feed PSMF Diet Add SU, MF, TZD, Repaglanide + prn Lispro for
BG <150 “Normal” BG from Day 1 Monitor BG qid See Patient Monthly, HFP HbA1c Bimonthly GI Problems: Cut MF
Hypoglycemia: Cut SUHypoglycemia Again: Cut RepaglinideAllow 2 Month to See TZD Effect

MIMICKING NATURE WITH INSULIN THERAPY
All persons need
both basal and mealtime insulin
to controlcontrol glucose
6-19
(endogenous or exogenous)

Limitations of NPH, Lente,and Ultralente
Do not mimic basal insulin profile
– Variable absorption
– Pronounced peaks
– Less than 24-hour duration of action
Cause unpredictable hypoglycemia
– Major factor limiting insulin adjustments
– More weight gain

1 5 10 15 20 25 30
1 5 10 15 20Asp
Gly
ArgExtension
Substitution
Arg
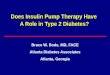
Insulin GlargineA New Long-Acting Insulin Analog
Modifications to human insulin chain
– Substitution of glycine at position A21
– Addition of 2 arginines at position B30
Gradual release from injection site
Peakless, long-lasting insulin profile

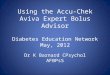
Glucose Infusion Raten = 20 T1DMMean ± SEM
SC insulin
4.0
3.0
2.0
1.0
0
24
20
16
12
8
4
0
0 4 8 12 16 20 24Time (hours)
mg
/kg
/min
µm
ol/k
g/m
in
Lepore M, et al. Diabetes. 2000;49:2142–2148.
NPH
Ultralente
Glargine
CSII

Lepore, et al. Diabetes. 1999;48(suppl 1):A97.
6
5
4
3
2
1
00 10
Time (h) after SC injection
End of observation period
20 30
GlargineNPH
Glu
cose
util
izat
ion
rate
(mg/
kg/h
)
Glargine vs NPH Insulin in Type 1 DiabetesAction Profiles by Glucose Clamp

Treat to Target Study: NPH vs Glargine in DM2 patients on OHA
Add 10 units Basal insulin at bedtime (NPH or Glargine)
Continue current oral agents Titrate insulin weekly to fasting BG < 100 mg/dL
• Based on average FBG of 6th and 7th day
- if 100-120 mg/dL, increase 2 units
- if 120-140 mg/dL, increase 4 units
- if 140-160 mg/dL, increase 6 units
- if 160-180 mg/dL, increase 8 units

The Treat-to-Target TrialRandomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patientsRiddle, Rosenstock, Gerich DIABETES CARE 2003 26;3080-2083

Percentage of Patients in Target (A1C < 7%)
2.5
32.3
48.8
66.2
58
0
10
20
30
40
50
60
70
Week 0 Week 8 Week 12 Week 18 Week 24
The Treat-to-Target TrialRandomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patientsRiddle, Rosenstock, Gerich DIABETES CARE 2003 26;3080-2083

GEMS--Glargine Evening Mealtime Secretagogue
Basal Dosing
– (Weight in #`s x 0.1)
• Glargine hs Prior to Meals
– Short Acting Secretagogue
• Rapaglinide 2 mg
• Nateglinide 120 mg
– Glimepiride 2 mg

The Treat-to-Target TrialRandomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patientsRiddle, Rosenstock, Gerich DIABETES CARE 2003 26;3080-2083

The Treat-to-Target TrialRandomized addition of glargine or human NPH insulin to oral therapy of type 2 diabetic patientsRiddle, Rosenstock, Gerich DIABETES CARE 2003 26;3080-2083

The Treat-to-Target Trial . Bedtime Glargine vs NPH
With Mealtime Regular
4
3
2
1
0
48
36
24
12
0Nocturnal
HypoglycemiaWeight Gain
*
**
Wei
ght (
kg)
NPH Glargine
Patients (%
)
*P < .0007**P < .02 (compared to NPH)
Rosenstock, et al. Diabetes. 1999;48(suppl 1):A100.
6-52

Treatment to Target Study: NPH vs Glargine in DM2 patients on OHA
57% had HbA1c <7%
Nocturnal Hypoglycemia reduced by 42% in the Glargine group
33% had HbA1c <7% without any nighttime hypoglycemia in glargine group
Results significantly better than with NPH

Body Weight in pounds x 0.1
Average am BG x 2 after five days
Add to Glargine (BG-100)/10
Repeat weekly
Example: 200#
20 units glargine q hs
AM BG averages 200 on 6th and 7th day
Add (BG-100)10 to glargine,
i.e. increase to 20 to 30 units q hs
2nd week--average 130
increase glargine from 30 to 33
Establishing Basal Requirement for Glargine

Overall Summary: Glargine
Insulin glargine has the following
clinical benefits
– Once-daily dosing because of its prolonged duration of
action and smooth, peakless time-action profile
– Comparable or better glycemic control (FBG)
– Lower risk of nocturnal hypoglycemic events
– Safety profile similar to that of human insulin












![[PPT]Steroid Induced Diabetes - Healing, Teaching & … Induced... · Web viewACE/ADA Task Force on Inpatient Diabetes. Diabetes Care. 2006;29(8):1955-1962. Bolus insulin to keep](https://img.pdfslide.us/doc/110x75/5ab7ace77f8b9a684c8bcb29/pptsteroid-induced-diabetes-healing-teaching-inducedweb-viewaceada.jpg)