Embed Size (px)
DESCRIPTION
The impact of a limited subsidy on access to antiretroviral therapy (ART) and patient outcomes in Singapore. Barnaby Young Infectious Diseases registrar Communicable Diseases Centre, Institute of Infectious Diseases and Epidemiology, Tan Tock Seng Hospital, Singapore. Overview. - PowerPoint PPT Presentation
Citation preview

The impact of a limited subsidy on access to antiretroviral therapy (ART) and patient outcomes in Singapore
Barnaby Young
Infectious Diseases registrarCommunicable Diseases Centre,
Institute of Infectious Diseases and Epidemiology, Tan Tock Seng Hospital, Singapore

Overview
• Financing of public healthcare in Singapore – and how HIV funding changed in early 2010
• ‘Before-and-after’ analysis– Examine the hypothesis that funding changes
improved ART practice and patient outcomes
• Some considerations for long-term affordability

GDP PPP, 60,410 Int$ per capita, ranked third 4
GINI co-efficient 0.459, second highest 5,6
HIV prevalence in general pop 0.1-0.3%1
HIV prevalence in MSM 3-4%2
Healthcare performance ranked sixth globally3
1Chua 2012, 2Griensven 2010, 3WHO 2000, 4IMF 2013, 5DSS 2012, 6OECD 2012,
Singapore

M & M & M
Medisave(1984)
• National savings scheme – employer/employee• Inpatient and outpatient bills within limits
Medishield(1990)
• Basic medical insurance scheme• Co-payment for critical illness
Medifund(1993)
• Endowment fund established to cover medical bills which ‘the patient could not afford after exhausting all other means of payment’
cpf.gov.sg, accessed 18/6/13

Limits of the 3 MsMedisave Medishield Medifund Drug subsidy
Prior to 2009 Withdrawal for ART capped at $250 per month
Excluded Antiretroviral therapy and HIV viral load excluded
Nil
2010 Increased to $550 per month
Excluded Included Nil
cpf.gov.sg, accessed 18/6/13

Methods
• CDC primary HIV treatment site in Singapore
• HIV sentinel cohort database– Cohort of 50% of patients newly presenting for care at CDC
from 2005 (randomly selected)
• Extracted data for 1st year of care, divided into two cohortsi. 2005-2008 ii. 2010-2011

2005-8 2010-11 P-value
Subjects 389 256
Age 42 (IQR 32-51) 42 (IQR 31-50) NS
Male 94% 94% NS
Race- Chinese- Malay- Indian
80%15%2%
77%14%7%
MSM 41% 56% <0.001
IVDU 4% 3% NS
Primary education 45% 42% NS
No income at dx 31% 33% NS
Median CD4+ at dx 181 (13%) 241 (15%) <0.05
CD4+ <200 53% 46% NS

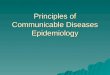
Proportion starting ART in 1st year
<200 200-350 350-500 >5000
0.2
0.4
0.6
0.8
12005-82010-11p<0.01
p<0.01
p<0.05NS
CD4+ Count

Time to ART after a diagnosis of AIDS (CD4+ <200)

Initial ART prescribed (for 2NRTI + NNRTI/PI combinations)

Outcomes at 1 year2005-8 2010-11 P-value
Deaths 18 (4.6% ) 1 (0.4%) <0.01
Hospital admission (Number - mean)
1.05 0.72 <0.01
Retention in care 90% 97% <0.01
Started ART 60% 71% <0.01
Time from diagnosis of AIDS to ART (days - median)
39 15 <0.01
Viral load in 1st year of therapy
28% 93% <0.001
Virologically suppressed (<1000 copies/ml)
94% 96% NS

Analysis of outcomes by year
2006 2007 2008 2009 2010 20110
2
4
6
8
10
12
14
Death
Loss to follow up
AIDS no ART in 1st year
Year
Perc
ent

IncomeNo income Income
Subjects 192 407
Cohort:- 2005-8- 2010-11
11478
250157
Age 45 (IQR 32-58) 39 (IQR 31-48) <0.05
Primary education 65% 36% <0.001
Baseline CD4+<200
62% 46% P<0.001
Hospital Admissions
1.38 0.75 <0.001
Deaths 12 (6.3%) 5 (1.2%) <0.001
Lost to follow up 13 (6.8%) 22 (5.4%) NS

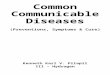
Proportion with AIDS who start ART
0 50 100 150 200 250 300 3500
0.2
0.4
0.6
0.8
1
2005-8 Income*2010-11 Income2005-8 No income*2010-11 No income
Days to ART
Prop
ortio
n st
artin
g AR
T
*p<0.05

Conclusion
• Outcomes markedly improved between the two cohorts
• This correlated with improved access to ART– Earlier initiation after AIDS diagnosis, and at higher
CD4 counts
– Timing and rapidity of changes suggests this was due to the increased funding available

Conclusion
• Improvements seen in both income groups – but greater magnitude in lower income due to late diagnosis
• Patient data regarding Medifund, Medisave utilisation and other financial sources in each cohort would be helpful– ?ART purchased locally or overseas

Limitations
• Retrospective study
• Financial data based on a spot estimates of salary only (no income group heterogeneous)– Loss of income due to illness
• Not known why some with low CD4+ counts did not start ART standard practice (pre-Zolopa 2009), ?too ill, psychosocial or financial

Future studies
• Means testing thresholds for Medifund eligibility has not been made public
• ART expensive, particularly for second-line therapies
• Concern over a ‘sandwiched group’ who do not qualify for Medifund assistance, and need to pay a significant proportion of household income for medical bills

Acknowledgments
• Co-investigators: Dr Arlene Chua, Dr Ng Oon Tek, Ms Ho Lai Peng, Dr Lee Cheng Chuan, A/Prof Leo Yee Sin
• Madeline Chua, Adriana, Chin Mei for data extraction
• The medical social workers at CDC