Embed Size (px)
Citation preview
BASIC SCIENCES
Assessment of Myocardial Oxidative MetabolicReserve with Positron Emission Tomographyand Carbon- 11 AcetateC. Gregory Henes, Steven R. Bergmann, Mary Norine Walsh, Burton E. Sobel, andEdward M. Geltman
Cardiovascular Division, Washington University School ofMedicine, St. Louis, Missouri
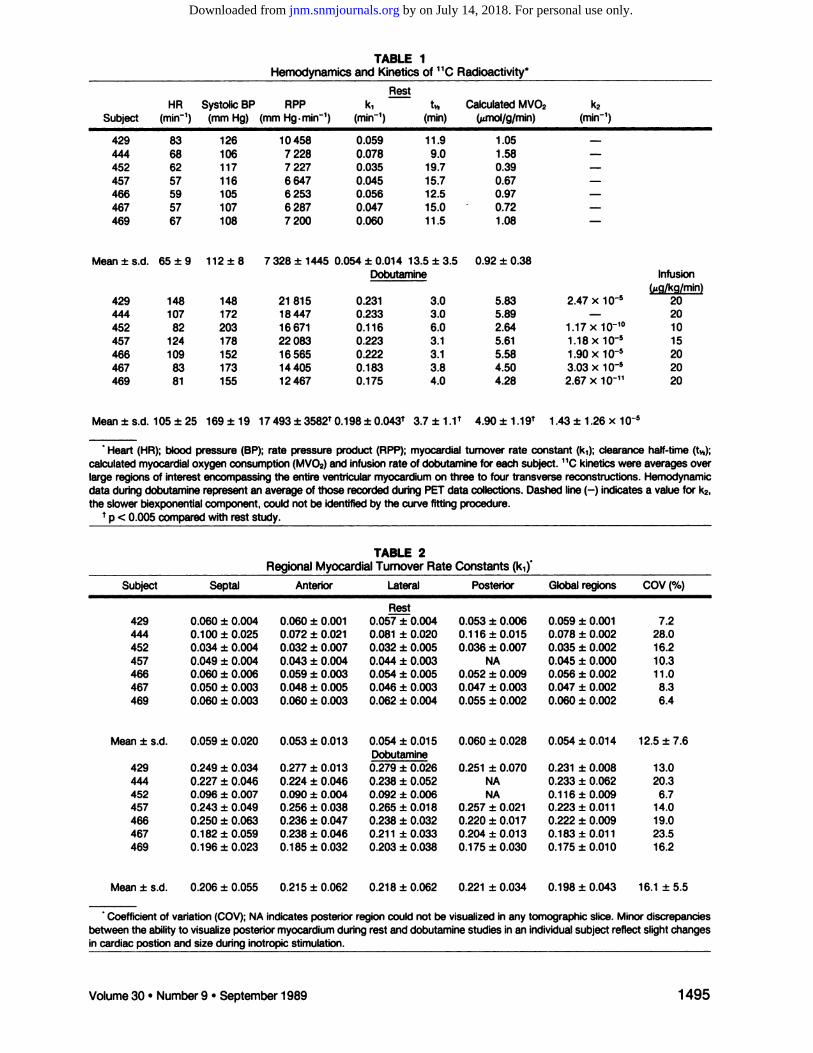
We have previously demonstrated that positron emission tomography (PET) with [@C]acetateallows noninvasive regional quantificationof myocardialoxidative metabolism. To assess themetabolic response of normal myocardium to increased work (oxidative metabolic reserve),clearance of myocardial @Cactivity after administration of [@C]acetate i.v. was measuredwith PET in seven normal subjects at rest and during dobutamine infusion. At rest, dearanceof 11Cwas monoexponential and homogeneous. The rate constant of the first phase of @Cclearance, k1, averaged 0.054 ±0.014 min@at a rate-pressure produce (APP)of 7329 ±1445 mmHg x bpm. Duringdobutamine infusion,APP increased by an average of 141% to17 493 ±3582 mm Hg x bpm. Clearance of 11Cbecame biexponential and remainedhomogeneous. k1 averaged 0.198 ±0.043 min@ with a mean coefficient of variation of 16%.k1and APP correlated closely (r = 0.91; p < 0.001), and the slope of the k1/APPrelationremained consistent in all subjects (1.48 ±0.42). These findings suggest that PET with [@C]acetate and dobutamine stress may provide a promising approach for evaluation of regionalmyocardialoxidative metabolic reserve in patients with cardiac diseases of diverse etiologiesand for assessment of the efficacyof interventions designed to enhance the recovery ofmetabolically comprised myocardium.
J Nuci Med 30: 1489—1499,1989
cute syndromes reflecting coronary artery disease(CAD) are characterized by an imbalance between regional myocardial oxygen supply and oxygen demandat rest or with stress, an imbalance that may be manifestclinically as stable angina, variant angina, unstable angina, or myocardial infarction. Unfortunately, however,diagnosis may be limited by difficulties in quantifyingregional myocardial oxygen consumption (MVO2).MVO2 can be measured directly at the time of cardiaccatheterization, but regional differences are difficult toquantify because of an admixture of coronary venousdrainage. Furthermore, widely applicable, noninvasiveprocedures have not been available. Coronary angiography provides descriptions of epicardial coronary vascular lesions, but does not measure the adequacy ofregional perfusion which is influenced not only by thegeometry of individual lesions but also by the numberof lesions in sequence and their length, the presence of
ReceivedJan. 17, 1989;revisionaccepted Apr. 12, 1989.For reprints contact: C. Gregory Henes, MD, Cardiovascular
Division, Box 8086, Washington University School of Medicine,660 S. Euclid Aye, St. Louis, MO 63110.
collateral flow, and myocardial compressive forces(among other factors). Measures of regional ventricularfunction extrapolated from radionuclide ventriculograms, contrast ventriculograms or echocardiogramsare affected not only by regional perfusion but also by
preload, afterload, autonomic tone, and circulating catecholamines.
Positron emission tomography (PET) is a promisingtool for characterizing regional myocardial perfusionand oxidative metabolism (1). Studies with tracers ofmetabolism of fatty acid [carbon-i 1- (‘‘C)labeled palmitate] (2,3) and glucose [fluorine-18- (‘8F)labeledfluorodeoxyglucose ([‘8F]FDG)](4) have delineatedstriking changes in patients with coronary artery diseaseand cardiomyopathy. However, quantification of overall regional myocardial oxidative metabolism based onanalysis of the behavior of these tracers is limited because their uptake and clearance depends upon arterialsubstrate content, sensitivity ofuptake to the hormonalenvironment, and competition among multiple metabolic pathways influencing the intracellular fates of each(5—10).Measures ofglycolytic flux have been useful indistinguishing viable from nonviable myocardium.
Volume30 •Number 9 •September1989 1489
by on July 14, 2018. For personal use only. jnm.snmjournals.org Downloaded from

However, they cannot differentiate aerobic from anaerobic glycolysis.
With ischemia, a backdiffusion of initially extractedbut unmetabolized tracers such as [‘‘Cjpalmitatemaylead to overestimates of beta oxidation (8, 9). As wehave recently shown, with ischemia and reperfusion thepattern of substrate use changes rapidly ( 7). Thus,estimates of overall regional oxidative metabolism witheither glucose or fatty acid as the sole tracer do notdelineate regional rates of myocardial oxidative metabolism or oxygen consumption.
Because metabolic flux through the tricarboxylic acid(TCA) cycle is tightly coupled to oxidative metabolismin the heart, we hypothesized that its delineation wouldprovide accurate estimates of regional myocardial oxygen consumption. Studies with experimental animalsin our laboratory demonstrated that tricarboxylic acidcycle flux could be traced with either [‘4Cjacetateor[‘‘C]acetateand that flux through the cycle correlatedclosely with myocardial oxygen consumption (11—13).In isolated perfused rabbit hearts, we found that thecorrelation between TCA cycle flux, measured by theoxidation oflabeled acetate to labeled C02, and oxygenconsumption was close over a wide range of physiologicand metabolic conditions (11). In closed-chest dogsstudied with PET, close associations between oxidationof extracted acetate to labeled C02, myocardial clearance of ‘‘Cactivity, and myocardial oxygen consumption over a wide range of cardiac work loads weredemonstrated (12). The correlation between [‘‘CJacetate clearance and MVO2 was unaffected by the patternofcarbohydrate and/or fatty acid substrate use (13).
In pilot studies in normal human subjects we delineated homogeneous extraction of[' ‘C]acetate throughout the myocardium with monoexponential clearancewhen the subjects were at rest (14). In patients withmyocardial infarction, uptake was reduced in ischemiczones and clearance ofextracted tracer was diminished,indicative of diminished regional myocardial oxygenconsumption (14). Because the capacity of myocardiumto augment oxidative metabolism in response to increased physiologic demand (metabolic reserve) is notnecessarily parallel to the capacity for augmentation ofregional perfusion (myocardial perfusion reserve) thepresent study was performed to determine whetherclearance of [‘‘C]acetatewas augmented in myocardium of normal subjects under conditions of increasedcardiac work, paralleling the known, homogeneous increase in regional myocardial oxygen consumption under these circumstances. Our objectives were: (a) todetermine the feasibility of measuring regional alterations in oxidative metabolism in human subjects; (b) todetermine whether the close relationship between [‘‘C]acetate clearance and myocardial oxygen consumptionobserved in animals was evident also in normal humansubjects; and (c) to define the extent of myocardial
metabolic reserve apparent in normal human subjectsin response to marked augmentation of cardiac contractility.
METhODS
The protocol used was approvedby the WashingtonUniversity Human Studies Committee. Informed written consentwas obtained from all subjects. The study population comprised seven healthy male volunteers aged 21 to 34 yr withoutprior history of cardiac disease, chest pain, hypertension, orcardiac arrhythmias, or ECG criteria of cardiac disease. Allsubjects were studied in the fasted state. A polyurethane moldof the subject'supper torso was formed to maximizepatientcomfort and minimize patient motion during the study. A 25-cm, 17-gauge polyethylene catheter was placed in an antecubital vein for injection oftracer and a short 18-gauge catheterplacedin the contralateralforearmforsamplingvenousblood.Subjects were positioned within the tomograph so that theheart wascenteredwithin the instrument's fieldof viewwiththe aid of positioning light beams and indelible markings toensureaccuraterepositioning.
Collectionof DataSubjectswerestudiedin SuperPETTI, a whole-body,time
of-flightpositronemission tomographypermittingacquisitionof list mode data sufficient for the reconstruction of seventransaxial slices with a slice thickness of 1.14 cm and a centerto-center slice separation of 1.5 cm (15). Operated in highresolution,time-of-ifightmode, the scanner has an effectivesensitivityof 170,000cps/@iCi/cc.Data were reconstructedwith an effectivefull width half maximum resolutionof 13.5mm. At the beginning of each study, to correct for photonattenuation, a 12-mmtransmission scan using a 68Oefl@Gasource was acquired. Proper positioning of the patient wasverifiedby review of transmission tomograms prior to theadministration of radiotracers.Subsequently, to permit visualizationofthe bloodpool,40 mCi to 50 mCi of oxygen-iSlabeledcarbon monoxide(C'5O)were administeredby inhalation. After 30 to 60 sec to allow equilibrationwith the bloodpool, data werecollectedfor 300 sec in list mode. Five to 10minutes thereafter, [‘‘C]acetate(0.4 mCi/kg) was administered as a bolus intravenously, and data acquired for 30 mmin list mode. The patient was removed from the scanner andpermitted to rest for @‘45mm, after which an incrementalinfusion ofdobutamine was initiated as described below. Aftera maximal steady-state infusion of dobutamine had beenestablished, C'5O and I' ‘C]acetatewere administered again.Imagingwas repeatedas in the baselinestudy.
Total reconstructedcounts perstudyaveraged15—30x 106.The approximateaveragects/slice/scanwas3.5±106.Radioactivitywas reconstructedinto “PET―counts which are linearly proportional to true count rate. At similar count ratesto those observed in human subjects after [‘‘Cjacetateadministration,phantom studiesyieldeda scalefactorof―—lOOPETcts/sec/@Ci.
Infusionof DobutamineInfusionofdobutamine wasemployedto increasemyocar
dial work. We utilized dobutamine rather than exercise to
1490 Henes,Bergmann,Walshetal The Journal of Nudear Medicine
by on July 14, 2018. For personal use only. jnm.snmjournals.org Downloaded from

The data acquired after the inhalation ofC'5O were reconstructed into a singlecompositereconstructionfor each tomographiclevel.Thesereconstructionswereusedfor placementof regions of interest in the left atrial blood pool so that theI ‘Cradioactivity in arterial blood could be determined.
The radioactivity within each region of interest was determined for each time point and corrected for physical decay ofthe tracer. Time-activity curves were obtained from eachregion of interest and analyzed with a multi-exponential leastsquares curve fitting algorithm. Data from the first 120 to 180sec were excluded because they are influenced by continuinguptake of tracer and spillover of radioactivity from the bloodpool. Curves were fit beginning with the time of onset of themost rapid decrease in counts after the initial peak, generallybetween 180 and 270 sec after injection of tracer. Timeactivity curves were fitted using a Marquardt nonlinear leastsquares fitting algorithm which weights data points inverselyproportional to the time of their occurrence. This accountsfor the decreasing reliability of count statistics due to tracerclearance and radioactive decay. Although all curves wereinitially intended to be fitted by a multi-exponential function,as detailed below, curves obtained under resting conditionsonly conformed to a monoexponential fit. Because clearancefrom the blood pool wasrapid with valuesdecliningby 85 to90% from peak values within 3 mm, correction of myocardialradioactivity for spillover from the blood pool was not required. The ‘‘Cturnover rate constant was defined as thecoefficient k, from the equation:
Q= A,e@t
for monoexponential curves and:
Q= A,e_@@t+ A2e@2t
for biexponentialcurveswhere,
Q= myocardial‘‘Cactivity,A, and A2= constants(y intercepts),k, and k2 = myocardial turnover rate constants, and t =time.
The half-time (t,12)of the rapid phase of clearance of ‘‘Cradioactivity was defined as ln 2/k,.
Resultsofprevious studies from our laboratoryhave shownthat the myocardialturnover rate constant k, assessedafterthe i.v. injection of [‘‘C]acetatecorrelates closely with myocardial oxygen consumption MVO2 measured directly by arterial and coronary sinus measurements in intact dogs (n =33) (12,13). Because normal ranges of MVO2 are availablefrom prior catheterizationstudiesin human subjects,we didnot feel that coronary sinus catheterizationwas necessaryorjustified in the present study. Accordingly, for purposes ofcomparison to determinants of myocardial oxygen requirements (rate pressureproduct) MVO2was estimated for eachdefined region of interest based on the relationshipbetweenMVO2and k, that had been delineated in studies of dogs.
Preparation of Tracers
C,5Oand [‘‘C]acetatewerepreparedaspreviouslydescribed(11,24,25). Purity of [‘‘C]acetatewas evaluated by HPLC forevery preparationand generallyexceeded 99.5% with specificradioactivityof [‘‘Cjacetate> 1Ci/mmol.
augment myocardial oxygen consumption because: (a) dobutamine has been shown to increase cardiac work safely inpatients with CAD (16—21);(b) dobutamine provides a continuous homogeneous stress over the 30 mm required for [‘‘C]acetate imaging, in contrast to exercise which may not besustainable at a constant, high workload for 30 mm; (c)exercise performed during acquisition of tomographic datamay lead to artifacts because of motion ofthe thorax.
Infusion ofdobutamine began with a dose of 5 @ig/kgJmin.Every 5 mm, the infusion rate was increased by 5 @@g/kg/minup to a maximum dose of 20 @g/kg/minor until one of thefollowing endpoints had been reached: heart rate >80% ofmaximum predictedheart rate for age;blood pressure>200/110 mmHg or <90/60; or an absolute decrease in bloodpressure @20mmHg; occurrence of chest pain; ST-segmentdepression @2mm or ST-segmentelevation@ 1 mm; occurrence of significant atrial or ventricular arrhythmias. If aclinical endpoint was reached at a given infusion rate, theinfusion was stopped for 5 mm and then restarted at thepreceding infusion rate. This procedure was continued untilan infusion rate could be maintained for at least 5 to 7 mmwithout eliciting a clinical endpoint. Once the maximumtolerable infusion rate had been established, the infusion wasmaintained at that level for the entire duration of the second[I ‘C]acetate scan. Heart rate and blood pressure were moni
tored every I5 mm at rest, every mm during incrementalinfusions of dobutamine, and at 3 mm intervals during thesteady state infusion ofdobutamine. The ECG was monitoredcontinuously oscilliscopically and recorded at baseline andevery 3 mm with infusions. Blood was sampled for measurement ofsubstrates (glucose, free fatty acids, acetate) at baselineand at the beginning, midpoint, and conclusion of tomographicdata collectionperformedduring infusionof dobutamine. Glucose was assayed using a commercially availableenzymatic kit (Behring Diagnostics, La Jolla, CA). Analysis offree fatty acids and acetate were performed as previouslydescribed (22,23).
In orderto measuretrue blood radioactivity,in one subjectstudied at rest, venous blood was withdrawn every minute forthe first 4 mm after administration oftracer, then every 2 mmfor 16additionalminutes,and then every4 mm until the endof the data acquisition. Total ‘‘Cradioactivity, ‘‘CO2,andnon-' ‘CO2radioactivity were measured in each sample aspreviously described (12).
Analysisof DataThe data collectedafteradministrationof[' ‘C]acetatewere
reconstructedin two ways. Each tomograph slice was represented as a 128 x 128 voxel array. Data acquired between 3mm and 8 mm after administration of tracer were reconstructed as composite images used solely for placement ofregions of interest (ROI). Data were reconstructed also into20 serial 90-sec frames commencing at the time of injectionof [“C]acetate.To assess the regional homogeneity of myocardial metabolic function, multiple contiguous regions ofinterest (each encompassing a volume of 1.3 cm3) were placedaround the circumference of two or more ventricular sliceswith the use of an interactivecomputer system. In additiøn,asingle large global region of interest encompassing the entiremyocardiumwasplacedon each tomographicreconstructionto determineaveragetracer kinetics.
1491Volume30 •Number9 •September1989
by on July 14, 2018. For personal use only. jnm.snmjournals.org Downloaded from
STATISTICS
Resultsare reported as means ±s.d. Differencesbetweenstudies performed at rest and during dobutamine infusionwere assessed with paired t-tests. Linear regression was calculated by the least-squares method; p < 0.05 was considered tobe significant.
RESULTS
HemodynamicsHemodynamics recorded at rest and in response to
infusion of dobutamine are indicated in Table 1. Theresults reported for dobutamine-stress reflect an averageofvalues obtained during the steady-state infusion whiletomographic data were being collected. The rate pressure product (RPP) [heart rate x systolic blood pressure], an index of global myocardial work, was calculated for all subjects. RPP increased by at least 73% inall subjects during infusion of dobutamine, with theincrease averaging 141 ±50% (p < 0.001 versus studiesat rest). The response to dobutamine varied substantially from subject to subject. Some demonstrated predominant increases in heart rate and others prominentincreasesin systolicbloodpressure.The dosesof dobutamine employed during steady state infusions during tomographic data collections are indicated in Table1. The maximal target dose of 20 @g/kg/min wasachieved in five of the seven subjects. In the remainingtwo subjects, the dose was limited by the blood pressureresponse. RPP remained constant during the steady
state infusion of dobutamine with a mean coefficientof variation of 4.5%.
All subjects tolerated the tomographic procedureswell. In no subject was there an adverse response toinfusion of dobutamine or administration of tracer.
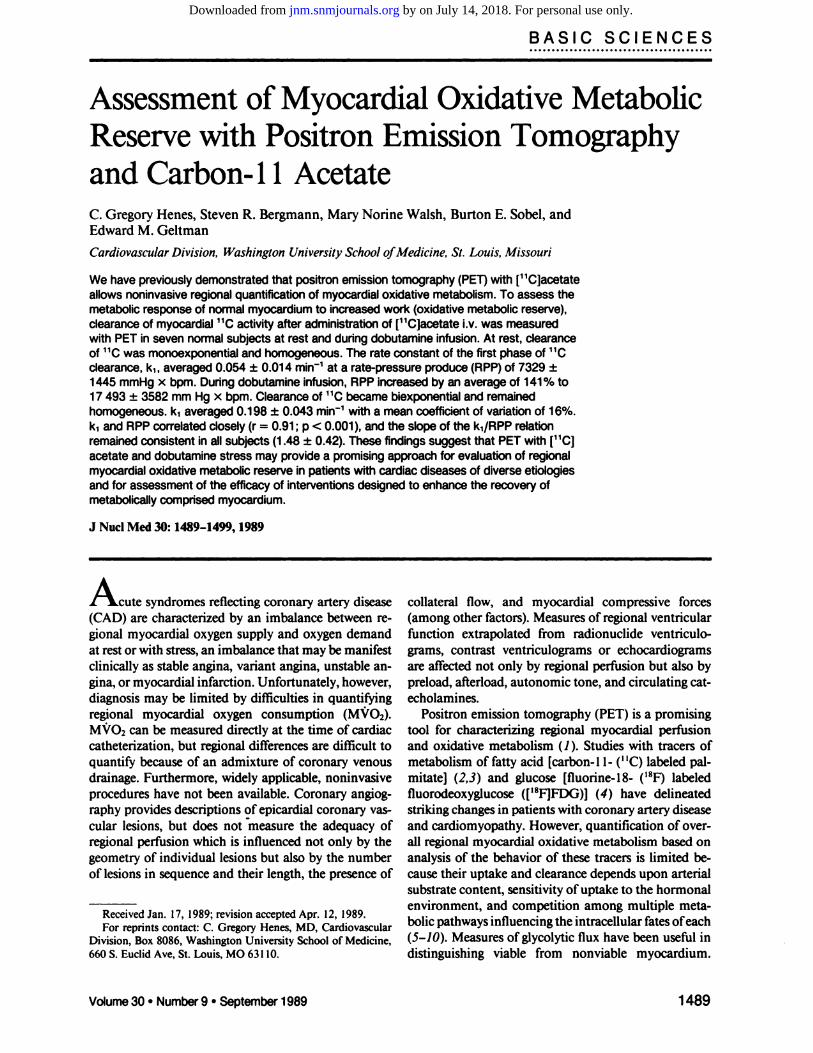
Tomographic ObservationsTypical images at four levels of the ventricle from a
normal subject acquired at rest are displayed in Figure1. The data incorporated in these reconstructions represent radioactivity recorded between 3 and 8 mm afterinjection of[' ‘C]acetate.These data were reconstructedwithout blood-pool subtraction or spillover correction.In all subjects accumulation of [‘‘C]acetateappearedhomogeneous at all tomographic levels of the heartrecorded at rest and after infusion of dobutamine.
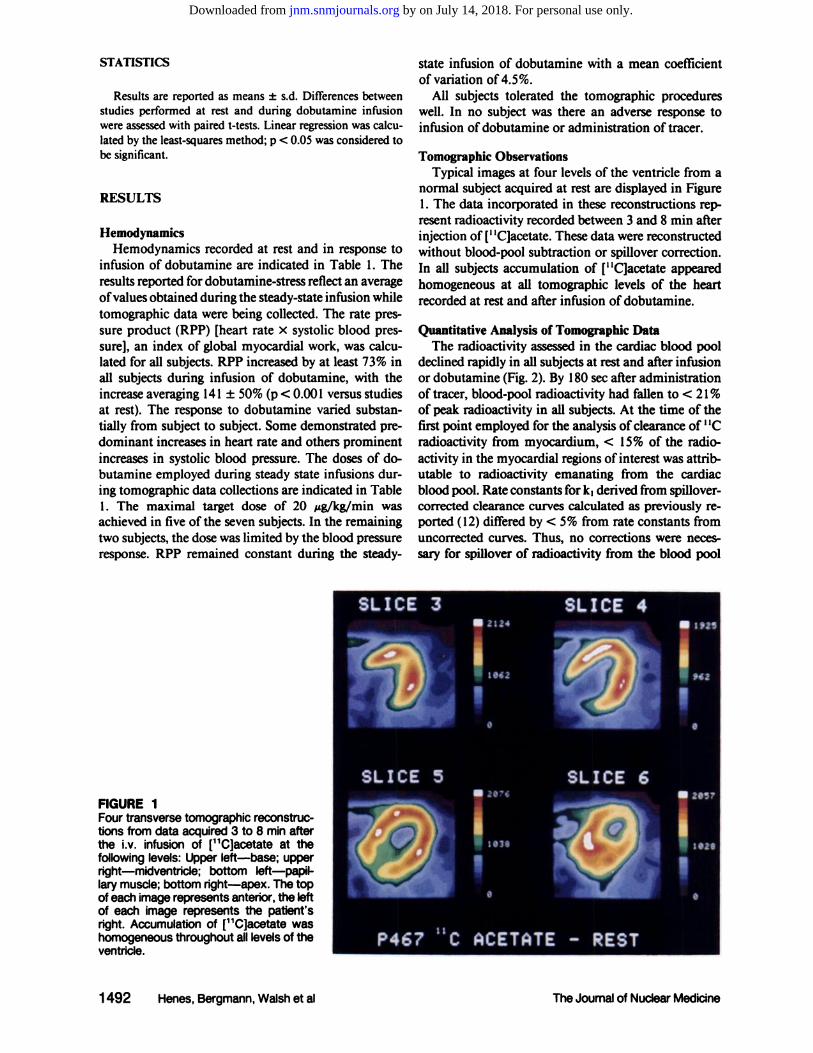
Quantitative Analysis of Tomographic DataThe radioactivity assessed in the cardiac blood pool
declined rapidly in all subjects at rest and after infusionor dobutamine (Fig. 2). By 180 sec after administrationof tracer, blood-pool radioactivity had fallen to < 21%of pea radioactivity in all subjects. At the time of thefirst point employed for the analysis ofclearance of' ‘Cradioactivity from myocardium, < 15% of the radioactivity in the myocardial regions ofinterest was attributable to radioactivity emanating from the cardiacblood pool. Rate constants for k, derived from spillovercorrected clearance curves calculated as previously reported (12) differed by < 5% from rate constants fromuncorrected curves. Thus, no corrections were necessary for spifiover of radioactivity from the blood pool
U 2124
! 1O@2
a
‘Ha
a I
U 2I'@
II
I 26S7
IllI
FIGURE 1Four transverse tomographic reconstructions from data acquired 3 to 8 mm afterthe i.v. infusion of [@C]acetate at thefollowing levels: Upper left—base; uppernght—midventride; bottom Ieft—pa@larymuscle; bottom right—apex.The topof each image represents anterior, the leftof each image represents the patient'sright. Accumulation of [@C]acetate washomogeneous throughout all levels of theventricle.
I
1492 Henes,Bergmann,Walshetal The Journal of Nuclear Medicine
SLICE 3 SLICE 4
SLICE 5 SLICE 6
P46? 11C ACETATE - REST
by on July 14, 2018. For personal use only. jnm.snmjournals.org Downloaded from
z
-Jw
0>
(I,I—z0UI-.Li
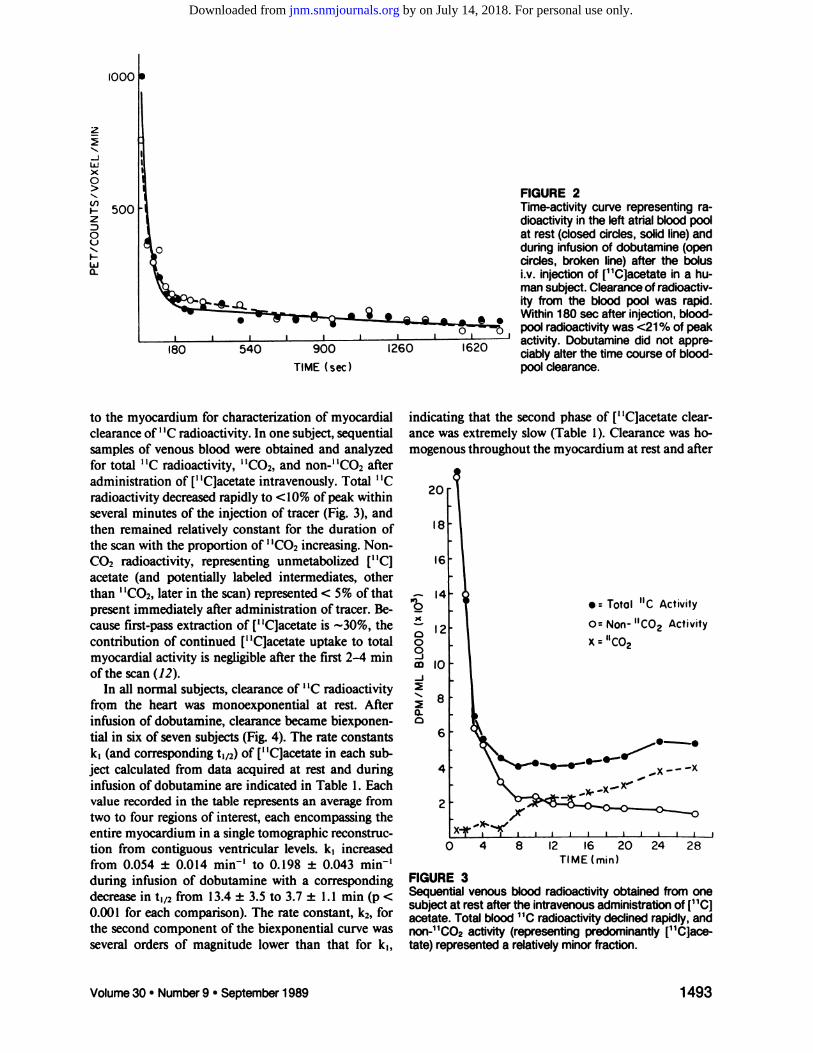
to the myocardium for characterization of myocardialclearance of ‘‘Cradioactivity. In one subject, sequentialsamples of venous blood were obtained and analyzedfor total ‘‘Cradioactivity, ‘‘CO2,and non-' ‘CO2afteradministration of [‘‘C]acetateintravenously. Total ‘‘Cradioactivity decreased rapidly to <10% ofpeak withinseveral minutes of the injection of tracer (Fig. 3), andthen remained relatively constant for the duration ofthe scan with the proportion of ‘‘CO2increasing. NonCO2 radioactivity, representing unmetabolized [“C]acetate (and potentially labeled intermediates, otherthan ‘‘C02,later in the scan) represented < 5% of thatpresent immediately after administration of tracer. Because first-pass extraction of [‘‘C]acetateis -@-30%,thecontribution of continued [“C]acetateuptake to totalmyocardial activity is negligible after the first 2—4mmofthe scan (12).
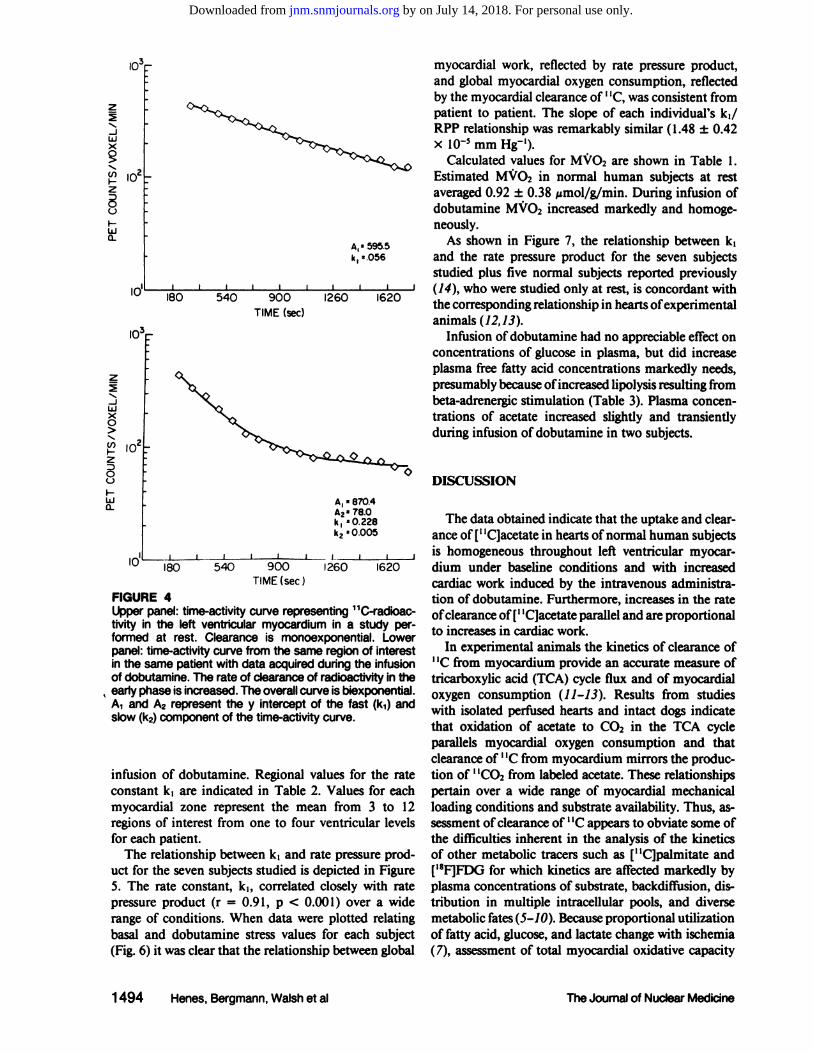
In all normal subjects, clearance of ‘‘Cradioactivityfrom the heart was monoexponential at rest. Afterinfusion of dobutamine, clearance became biexponential in six of seven subjects (Fig. 4). The rate constantsk, (and corresponding t,,2) of [‘‘C]acetatein each subject calculated from data acquired at rest and duringinfusion of dobutamine are indicated in Table 1. Eachvalue recorded in the table represents an average fromtwo to four regions of interest, each encompassing theentire myocardium in a single tomographic reconstruction from contiguous ventricular levels. k, increasedfrom 0.054 ±0.014 min' to 0. 198 ±0.043 min'during infusion of dobutamine with a correspondingdecrease in t,12from 13.4 ±3.5 to 3.7 ±1.1 mm (p <0.001 for each comparison). The rate constant, k2, forthe second component of the biexponential curve wasseveral orders of magnitude lower than that for k,,
FIGURE 2Time-activity curve representing radioactivityin the left atrial blood poolat rest (closed circles, solid line) andduring infusion of dobutamine (opencircles, broken line) after the bolusi.v. injection of [11C]acetate in a human subject. Clearance of radioactivity from the blood pool was rapid.Within180 sec after injection, bloodpool radioactivitywas <21 % of peakactivity. Dobutamine did not appreciablyalter the time course of bloodpool clearance.
260 620
TIME (sec)
indicating that the second phase of [‘‘C]acetateclearance was extremely slow (Table 1). Clearance was homogenous throughout the myocardium at rest and after
‘C
0
S-j
0-
20
•:Total “CActivity
0= Non- “CO2Activity
x =“CO2
10
8
6
0
FIGURE 3Sequential venous blood radioactivityobtained from onesubject at rest after the intravenous administrationof [11C]acetate. Total blood ‘1Cradioactivity declined rapidly, andnon-'1C02 activity (representing predominantly [11C]acetate) represented a relativelyminor fraction.
2
16 20
TIME (mm)
24 28
1493Volume 30 •Number 9 •September1989
by on July 14, 2018. For personal use only. jnm.snmjournals.org Downloaded from
@,_,,, I@@ @L@ @j I f@
900 260 620TIME (sec)
FIGURE 4Upper panel: time-activitycurve representing 11C-radioactivity in the left ventricular myocardium in a study performed at rest. Clearance is monoexponential. Lowerpanel: time-activitycurve from the same region of interestin the same patient with data acquired during the infusionof dobutamine. The rate of clearance of radioactivityin the
‘early phase is increased. The overallcurve is biexponential.
A1and A2 represent the y interceptof the fast (k1)andslow (k2)component of the time-activitycurve.
infusion of dobutamine. Regional values for the rateconstant k, are indicated in Table 2. Values for eachmyocardial zone represent the mean from 3 to 12regions of interest from one to four ventricular levelsfor each patient.
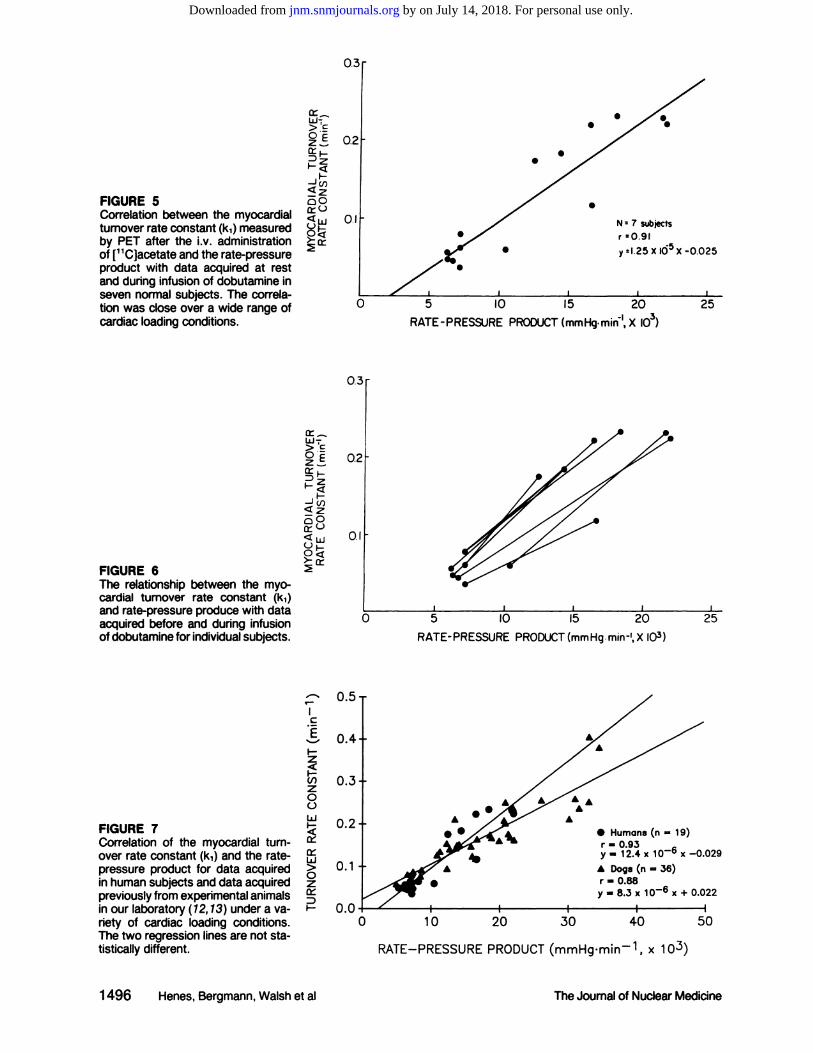
The relationship between k, and rate pressure product for the seven subjects studied is depicted in FigureS. The rate constant, k,, correlated closely with ratepressure product (r = 0.91, p < 0.001) over a widerange of conditions. When data were plotted relatingbasal and dobutamine stress values for each subject(Fig. 6) it was clear that the relationship between global
IL)
myocardial work, reflected by rate pressure product,and global myocardial oxygen consumption, reflectedby the myocardial clearance of ‘‘C,was consistent frompatient to patient. The slope of each individual's k,/RPP relationship was remarkablysimilar (1.48 ±0.42x 10-smm Hg').
Calculated values for MVO2 are shown in Table 1.Estimated MVO2 in normal human subjects at restaveraged 0.92 ±0.38 imol/g/min. During infusion ofdobutamine MVO2 increased markedly and homogeneously.
A@ 5955 As shown in Figure 7, the relationship between k,
k, .056 and the rate pressure product for the seven subjects
studied plus five normal subjects reported previouslyJ (14), who were studied only at rest, is concordant with
260 1620 the corresponding relationship in hearts of experimentalanimals (12,13).
Infusion ofdobutamine had no appreciable effect onconcentrations of glucose in plasma, but did increaseplasma free fatty acid concentrations markedly needs,presumably because ofincreased lipolysis resulting frombeta-adrenergic stimulation (Table 3). Plasma concentrations of acetate increased slightly and transientlyduring infusion of dobutamine in two subjects.
180 540
ILl 180 540 900
TIME (sec)
l0@
102.
10@
2
-ILi
(.1) ,,[email protected] ‘-‘2
U
Li
2
-JU
0>
U)I—z
0I-Ua-
DISCUSSION
The data obtained indicate that the uptake and clearance of[―C]acetatein hearts ofnormal human subjectsis homogeneous throughout left ventricular myocardium under baseline conditions and with increasedcardiac work induced by the intravenous administration of dobutamine. Furthermore, increases in the rateofclearance of[' ‘C]acetateparallel and are proportionalto increases in cardiac work.
In experimental animals the kinetics of clearance of, ‘Cfrom myocardium provide an accurate measure of
tricarboxylic acid (TCA) cycle flux and of myocardialoxygen consumption (11-13). Results from studieswith isolated perfused hearts and intact dogs indicatethat oxidation of acetate to CO2 in the TCA cycleparallels myocardial oxygen consumption and thatclearance of ‘‘Cfrom myocardium mirrors the production of ‘‘CO2from labeled acetate. These relationshipspertain over a wide range of myocardial mechanicalloading conditions and substrate availability. Thus, assessment ofclearance of ‘‘Cappears to obviate some ofthe difficulties inherent in the analysis of the kineticsof other metabolic tracers such as [“C]palmitateand[‘8fl@forwhichkineticsareaffectedmarkedlybyplasma concentrations of substrate, backdiffusion, distribution in multiple intracellular pools, and diversemetabolic fates(5-1O). Because proportional utilizationof fatty acid, glucose, and lactate change with ischemia(7), assessment of total myocardial oxidative capacity
A, [email protected], p0.228k2 @0.0O5
1494 Henes,Bergmann,Walshetal TheJournalof NuclearMedicine
by on July 14, 2018. For personal use only. jnm.snmjournals.org Downloaded from
HRSystolic BPRPPRest k1 t@CalculatedMVO2k2Subject(min1)(mm Hg)(mm Hg.min1)(min1)(mm)(@mol/g/min)(min')
. Heart (HR); blood pressure (BP); rate pressure product (RPP); myocardial turnover rate constant (ki); clearance half-time(t½);calculated
myocardialoxygen consumption (MVO2)and infusionrate of dobutamine for each subject. ‘1Ckineticswere averagesoverlargeregionsof Interestencompassingthe entireventricularmyocardiumon threeto fourtransversereconstructions.Hemodynamicdataduringdobutaminerepresentan averageof those recordedduringPETdatacollections.Dashed Ik@e(-) indicatesa valuefork2,the
slower biexponentialcomponent, could not be identifiedby the curve fittingprocedure.tp < 0.005 compared with rest study.TABLE
2RegionalMyocardialTurnover Rate Constants(k1)Subject
Septai Anterior Lateral Posterior Globalregions COy (%)
. Coefficient of variation (COV); NA indicates posterior region could not be visualized in any tomographic slice. Minor discrepancies
betweentheabilityto visualizeposteriormyocardiumduringrest anddobutaminestudiesinan individualsubjectreflectslightchangesin cardiac postion and size during inotropicstimulation.
TABLE 1Hemodynamics and Kineticsof 11CRadioactivity*
42983126104580.05911.91.054446810672280.0789.01.584526211772270.03519.70.394575711666470.04515.70.674665910562530.05612.50.974675710762870.04715.00.724696710872000.06011.51.08
Mean±s.d. 65±9 112±8 7 328 ±1445 0.054 ±0.014 13.5 ±3.5Dobutamine
0.92 ±0.38Infusion
(@g/kg/min)2042914814821 8150.2313.05.832.47 [email protected]—2045282203166710.1166.02.641.17x10'°10457124178220830.2233.15.611.18x10515466109152165650.2223.15.581.90x1052046783173144050.1833.84.503.03x1052046981155124670.1754.04.282.67x101'20
Mean ±s.d. 105 ±25 169 ±19 17 493 ±3582t 0.198 ±[email protected] ±1.1@ 4.90 ±1.19@ 1.43 ±1.26 x 1O@
Rest4290.060±0.0040.060 ±0.0010.057 ±0.0040.053 ±0.0060.059 ±0.0017.24440.100±0.0250.072 ±0.0210.081 ±0.0200.1 16 ±0.0150.078 ±0.00228.04520.034±0.0040.032 ±0.0070.032 ±0.0050.036 ±0.0070.035 ±0.00216.24570.049±0.0040.043 ±0.0040.044 ±0.003NA0.045 ±0.00010.34660.060±0.0060.059 ±0.0030.054 ±0.0050.052 ±0.0090.056 ±0.00211.04670.050±0.0030.048 ±0.0050.046 ±0.0030.047 ±0.0030.047 ±0.0028.34690.060±0.0030.060 ±0.0030.062 ±0.0040.055 ±0.0020.060 ±0.0026.4Mean
±s.d.0.059 ±0.0200.053 ±0.0130.054 ±0.015Dobutamine0.060
±0.0280.054 ±0.01412.5 ±7.64290.249
±0.0340.277 ±0.0130.279 ±0.0260.251 ±0.0700.231 ±0.00813.04440.227±0.0460.224 ±0.0460.238 ±0.052NA0.233 ±0.06220.34520.096±0.0070.090 ±0.0040.092 ±0.006NA0.116 ±0.0096.74570.243±0.0490.256 ±0.0380.265 ±0.0180.257 ±0.0210.223 ±0.01114.04660.250±0.0630.236 ±0.0470.238 ±0.0320.220 ±0.0170.222 ±0.00919.04670.182±0.0590.238 ±0.0460.21 1 ±0.0330.204 ±0.0130.183 ±0.01123.54690.196±0.0230.185 ±0.0320.203 ±0.0380.175 ±0.0300.175 ±0.01016.2
16.1 ±5.5Mean±s.d. 0.206±0.055 0.215 ±0.062 0.218 ±0.062 0.221 ±0.034 0.198 ±0.043
1495Volume 30 •Number 9 •September1989
by on July 14, 2018. For personal use only. jnm.snmjournals.org Downloaded from
I.>.c:
0E
@ci:
C
EI-z
C,)z00Li
ci::Li>0zci:::DI-
.
0.1 N =7 subjects
r :0.91
y:l.25X K55X -0.025
I
5 10 IS 20 25RATE-PRESSURE PRODUCT(mmHg.min@,X lOs)
0.3
0.2
0.I
0 5 10 IS 20 25
RATE-PRESSURE PRODUCT(mmHg.min-', X I0@)
0.5
0.4
0.3
A0.2
FIGURE 5Correlation between the myocardialturnover rate constant (k1)measuredby PET after the i.v. administrationof [11C]acetate and the rate-pressureproduct with data acquired at restand during infusion of dobutamine inseven normal subjects. The correlation was close over a wide range ofcardiac loading conditions.
FIGURE 6The relationship between the myocardial turnover rate constant (k1)and rate-pressure produce with dataacquired before and during infusionofdobutaminefor individualsubjects.
FIGURE 7Correlation of the myocardial turnover rate constant (k1)and the ratepressure product for data acquiredin human subjects and data acquiredpreviously from experimental animalsin our laboratory (12, 13) under a variety of cardiac loading conditions.The two regression lines are not statisticallydifferent.
. Humans(n —19)r —0.93y —12.4 x i06 x —0.029
0.1 A Dogs (n = 36)r —0.88y —8.3 x i06 x + 0.022
0@0 10 20 30 40 50
RATE—PRESSUREPRODUCT(mmHg.minl, x 103)
1496 Henes,Bergmann,Walshetal The Journal of Nudear Medicine
by on July 14, 2018. For personal use only. jnm.snmjournals.org Downloaded from

Rest acetate scan
MidpointAcetate
scan duringdobutamineStartMidpointConclusionGlucose
(mM)4.8 ±0.44.9 ±0.14.7 ±0.24.6 ±0.4Freefattyacids(pM)522±243906±370822±128829±103Acetate
(tiM)1 06 ±23121 ±16203 ±83145 ±16
TABLE3Plasma Substrate Levels
is not possible by analysis of metabolism of any one ofthem alone.
Both oxidative glucose metabolism and beta oxidation of fatty acids result in the production of acetylCoA which subsequently undergoes oxidative metabolism in the mitochondria through the tricarboxylic acidcycle. Thus, the tricarboxylic acid flux reflects overalloxidation of substrate regardless of origin in long-chainfatty acid or carbohydrate. The close relationship between MVO2 and acetate clearance is unaltered byconditions of ischemia, hypoxia, and altered substrateavailability (11—13).Thus, measurement of ‘‘Cclearance with PET after injection of [‘‘C]acetatepermitsnoninvasive, regional assessment of myocardial oxidative metabolism.
Dobutamine exerts potent positive inotropic effectsand can activate beta-i, beta-2, and alpha-i adrenoreceptors (26,27). It improves myocardial performancein patients with reduced cardiac output resulting fromacute coronary syndromes, cardiomyopathy, or valvular heart disease (27). It has been used for pharmacologic stress testing (16—21)because it increases myocardial oxygen demand by increasing both heart rate andblood pressure without unduly increasing the incidenceof cardiac arrhythmias. In experimental animals, dobutamine alters the distribution ofcoronary blood flowto zones distal to coronary stenoses and induces regionalabnormalities ofleft ventricular wall motion, wall thickening, and ventricular performance in animals withsignificant coronary stenoses (28—34).Regional alterations of left ventricular wall motion (16, 18—20)and ofthe distribution of 20'TI (17) occur with dobutaminestress in human subjects with coronary artery disease.
We used dobutamine to induce pharmacologic stressso that regional myocardial metabolic reserve could becharacterized in this study because it increases myocardial oxygen demand without the need for exercise. Thecontinuous stimulus required to provide a homogeneous metabolic stress over a 30-mm interval would notbe readily accomplished with exercise stress becausemost patients would not have sufficient endurance.Furthermore, exercise would be likely to give rise tosignificant image artifacts because of motion. Atrialpacing was not selected because of its invasive natureand because the extent of myocardial stress that can beinduced with atrial pacing is modest (35). Varyingdegrees of atrioventricular block are encountered often
before the RPP is increased maximally when pacing isemployed.
The uptake and clearance of [‘‘C]acetatewas foundto be homogeneous in normal subjects at rest and withpharmacologic stress. The early phase of clearance of‘‘Cincreased proportionally to increasing global cardiac
work as measured by the rate-pressureproduct. Theincrease in the rate of clearance of ‘‘Cfrom myocardium was spatially uniform. After dobutamine, thekinetics of clearance became biexponential. The rateconstant of the second component of the clearancecurve was extremely low. Late clearance represented avery small proportion of initially extracted tracer. Ifwhole myocardial regions ofinterest were used for timeactivity analysis, it was possible, under some circumstances, to define biexponential clearance of ‘‘Cradioactivity from the heart. However parameters estimatedin this manner had a standard error of@ 40—200%compared to an error of 1.5—3%using the monoexponential fit. When biexponential fits were possible insubjects at rest, A2averaged 4% of A,, and k2 averaged< 0. 1% of k,. Thus, it is probable that clearance is
biexponential at rest in humans but the second component is obscured by the relatively slow clearance ofthe first component at rest and is also obscured bystatistical noise. In several subjects studied previouslyfor up to 60 mm after administration of tracer, nobiexponential component of clearance could be seen(14). In addition, it should be noted that the clearanceof the second component even after dobutamine isessentially infinite. Thus, for clinical applications, fitting of the early portion of all time-activity curves to amonoexponential simplifies the computational analysisand is accurate and valid under most circumstances,especially for interrogation of small regions of interest.Carbon-i 1acetate entering the slowly turning over poolmost likely represents incorporation of[' ‘C]acetateintoamino acids (glutamate, glutamine, and aspartate) orinto lipid pools (11,36,37).
Because the RPP correlates closely with global myocardial oxygen consumption (determined invasively) inanimals (12,13) and patients (38—40)and because k,correlates closely with myocardial oxygen consumptionmeasured directly in animals, the present results suggestthat the rate of clearance of ‘‘Cfrom the myocardiumin man provides a noninvasive measure of regionalMVO2. Values of MVO2 estimated in patients ranged
1497Volume 30 •Number 9 •September1989
by on July 14, 2018. For personal use only. jnm.snmjournals.org Downloaded from
from 0.92 ±0.38 @imol/g/minat rest to 4.90 ±1.19@imol/g/min with infusion of dobutamine. These esti
mated values are somewhat lower than those that havebeen measured invasively in human subjects (38—40).The discrepancy may reflect interspecies differences inthe numerical relation of k, to MVO2 (11—13,41).
Clinical ImplicationsNoninvasive assessment of regional myocardial oxy
gen consumption has considerable potential utility forthe evaluation ofpatients with cardiac disease. It shouldpermit assessment of the physiologic significance ofcoronary stenoses by determination of the metabolicconsequences of physiologic stress in patients with obstructive coronary lesions of questionable physiologicsignificance. In addition, it should provide estimates oftissue viability and metabolic reserve in patients withcoronary artery disease, cardiomyopathy, valvular heartdisease, and other processes manifested by abnormalities of regional or global function. It should facilitateobjective noninvasive assessments ofthe potential benefit of therapeutic interventions and improve the selection ofpatients likely to benefit from diverse proceduresincluding coronary artery bypass grafting, valve replacement, and cardiac transplantation.
ACKNOWLEDGMENTS
The authors thank Theron Bairdand ColleenSchaab,RNfor technical assistance; Dave Marshall, Jim Bakke, and thestaff of the Washington University Medical Center Cyclotronfor tracer preparation; and Joyce Kalayeh and Becky Leonardfor secretarial assistance.
This work was supported in part by National Heart, Lungand Blood Institute, grant HL17646, Specialized Center ofResearchin IschemicHeart Disease.
REFERENCES
1. Bergmann SR, Fox KAA, Geitman EM, Sobel BE.Positron emission tomography ofthe heart. Prog CardiovascDis1985;28:165—194.
2. Sobel BE, Geltman EM, Tiefenbrunn AJ, et al. Improvement of regional myocardial metabolism aftercoronary thrombolysis induced with tissue-type plasminogen activator or streptokinase. Circulation 1984;69:983—990.
3. Geltman EM, Smith JL, Beecher D, Ludbrook PA,Ter-Pogossian MM, Sobel BE. Altered regional myocardial metabolism in congestive cardiomyopathy detected by positron tomography. Am J Med 1983;74:773—785.
4. Marshall RC, Tillisch JH, Phelps ME, et al. Identification and differentiation of resting myocardial ischemia and infarction in man with positron computedtomography, ‘8F-labeledfluorodeoxyglucose and N-13 ammonia. Circulation 1983; 67:766—778.
5. Schelbert HR, Henze E, Schon HR, et al. C-i 1 palmitate for the noninvasive evaluation ofregional myocardial fatty acid metabolism with positron computedtomography. III. In vivo demonstration of the effects
of substrate availability on myocardial metabolism.Am Heart J 1983; 105:492—504.
6. Schelbert HR, Henze E, Sochor H, et al. Effects ofsubstrate availability on myocardial C-i 1 palmitatekinetics by positron emission tomography in normalsubjects and patients with ventricular dysfunction. AmHeartJ 1986;111:1055—1064.
7. Myears DW, Sobel BE, Bergmann SR. Substrate usein ischemic and reperfused canine myocardium: quantitative considerations.Am JPhysiol: Heart CircPhysiol1987;253:Hl07—H114.
8. Fox KAA, Abendschein D, Ambos HD, Sobel BE,Bergmann SR. Efflux of metabolized and nonmetabolizedfatty acid from canine myocardium.Implications for quantifying myocardial metabolism tomographically. CircRes 1985; 57:232—243.
9. Rosamond TL, Abendschein DR, Sobel BE, Bergmann SR, Fox KAA. Metabolic fate of radiolabeledpalmitate in ischemic canine myocardium: Implications for positron emission tomography. J Nud Med1987;28:1322—1329.
10. Merhige ME, Ekas R, Mossberg K, Taegtmeyer H,Gould KL. Catecholamine stimulation, substratecompetition, and myocardial glucose uptake in conscious dogs assessed with positron emission tomography. Circ Res 1987; 61:11-124-11-129.
11. Brown MA, Marshall DR. Sobel BE, Bergmann SR.Delineation ofmyocardial oxygenutilization with carbon-1 1 labeled acetate. Circulation 1987; 76:687—696.
12. Brown MA, Myears DW, Bergmann SR. Noninvasiveassessment of canine myocardial oxidative metabolism with carbon-i 1 acetate and positron emissiontomography.J Am CoilCardiol1988;12:1054—1063.
13. Brown MA, Myears DW, Bergmann SR. Validity ofestimates of myocardial oxidative metabolism withcarbon-i 1-acetate and positron emission tomographydespite altered patterns ofsubstrate utilization. J NuciMed 1989;30:187—193.
14. Walsh MN, Brown MA, Henes CG, et al. Estimationof regional myocardial oxidative metabolism by positron emission tomography with carbon-i 1-acetate inpatients [Abstract]. Circulation 1988; 78(II):599.
15. Ter-Pogossian MM, Ficke DC, Yamamoto M, HoodJT. Super PElT I: a positron emission tomographutilizing photon time-of-ifight information. IEEETransMedlmag 1982;3:179—187.
16. Freeman ML, Palac R, Mason J, et al. A comparisonof dobutamine infusion and supine bicycle exercisefor radionuclide cardiac stress testing. Clin Nucl Med1984;19:251—255.
17. Mason JR, Palac RT, Freeman ML, et al. Thalliumscintigraphy during dobutamine infusion: nonexercisc-dependent screening test for coronary disease. AmHeartJ 1984; 107:481—485.
18. Meyer SL, Curry GC, Donsky MS, Twieg DB, ParkeyRW,WifiersonJT. Influenceofdobutamineon hemodynamics and coronary blood flow in patients withand without coronary artery disease. Am J Cardiol1976; 38:103—108.
19. David D, Lang RM, Borow KM. Clinical utility ofexercise, pacing, and pharmacologic stress testing forthe noninvasive determination ofmyocardial contractility and reserve. Am Heart J 1988; 116:235—247.
20. Berthe C, Pierard LA, Hiernaux M, et al. Predictingthe extent and location of coronary artery disease inacute myocardial infarction by echocardiography during dobutamine infusion. Am J Cardiol 1986; 58:1167—1172.
21. Mannering D, Cripps T, Leech G, et al. The dobuta
The Journal of Nuclear Medicine1498 Henes,Bergmann,Walshetal
by on July 14, 2018. For personal use only. jnm.snmjournals.org Downloaded from
mine stress test as an alternative to exercise testingafter acute myocardial infarction. Br Heart J 1988;59:521—526.
22. Bergmann SR, Carlson E, Dannen E, Sobel BE. Animproved assay with 4-(2-thiazlylaso)-resorcinol fornon-esterified fatty acids in biological fluids. C/micaChimica Acta 1980; 104:53—63.
23. Bergmeyer HU, Mollering H. Acetate. In: BergmeyerHU, ed. Methods of enzymic analysis. Weinheim:Verlag-Chemle, 1984;628—639.
24. Welch MJ, Ter-Pogossian MM. Preparation of shorthalf-lived radioactive gases for medical studies. RadRes 1968;36:580—587.
25. Pike VW, Eakins MN, Allan RM, Selwyn AP. Preparation of [1-―C]acetate—anagent for the study ofmyocardial metabolism by positron emission tomography. IntJApplRadiatlsot 1982; 33:505—512.
26. Tuttle RR and Mills J. Dobutamine: development ofa new catecholamine to selectively increase cardiaccontractility. CircRes 1975; 36:185—196.
27. Ruffolo RR. Review: the pharmacology of dobutamine. Am JMedSci 1987; 294:244—248.
28. Willerson JT, Hutton I, Watson JT, Platt MR, Templeton GH. Influence ofdobutamine on regional myocardial blood flowand ventricular performance duringacute and chronic myocardial ischemia in dogs. Circulation 1976; 53:828—833.
29. Tuttle RR, Pollock GD, Todd G, MacDonald B, TustR, DusenberggyW. The effect of dobutamine oncardiac oxygen balance, regional blood flow, and infarction severity after coronary artery narrowing indogs. Circ Res 1977; 4 1:357—364.
30. Warltier DC, Zyvoloski M, Gross GJ, Hardman HF,Brooks HL. Redistribution of myocardial blood flowdistal to a dynamic coronary arterial stenosis by sympathomimetic amines. Am J Cardiol 1981; 48:269—279.
3 1. Lanzer P, Garrett J, Lipton M, et al. Quantitation ofregional myocardial function by cine computed tomography: pharmacologic changes in wall thickness.JAm Coil Cardiol 1986;8:682—692.
32. Buda iU, Zotz Ri, Gallagher KP. The effect of motropic stimulation on normal and ischemic myocardium after coronary occlusion. Circulation 1987;76:163—172.
33. Fung AY, Gallagher KP, Buda Al. The physiologicbasis of dobutamine as compared with dipyridamolestress interventions in the assessment of critical coronary stenosis. Circulation 1987; 76:943—951.
34. McGillen MJ, DeBoe SF, Friedman HZ, ManciniGBJ. The effects of dopamine and dobutamine onregional function in the presence of rigid coronarystenoses and subcritical impairments of reactive hyperemia. Am Heart J 1988; 115:970—977.
35. Grover-McKay M, Schelbert HR, Schwaiger M, et al.Identification of impaired metabolic reserve by atrialpacing in patients with significant coronary arterystenosis. Circulation 1986; 74:281—292.
36. Neurohr KH, Barrett EJ, Shulman RS. In vivo carbon13 nuclear magnetic resonance studies ofheart metabolism.ProcNat!AcadSciUSA 1983;80:1603—1607.
37. Malloy CR, Sherry AD, Jeffrey FMH. Carbon fluxthrough citric acid cycle pathways in perfused heartby ‘3CNMR spectroscopy. FEBS Lett 1987; 212:58—62.
38. Kitamura K, Jorgensen CR, Gobel FL, Taylor HL,Wang Y. Hemodynamic correlates ofmyocardial oxygen consumption during upright exercise. JApplPhysiol 1972; 32:516—522.
39. Nelson RR, Gobel FL, Jorgensen CR, Wang K, WangY, Taylor HL. Hemodynamicpredictorsor myocardial oxygen consumption during static and dynamicexercise.Circulation1974;50:1179—1189.
40. Gobel FL, Nordstrom LA, Nelson RP, Jorgensen CR,Wang Y. The rate-pressureproduct as an index ofmyocardial oxygen consumption during exercise inpatients with angina pectoris. Circulation 1978;57:549—556.
41. Buxton DB, Schwaiger M, Nguyen A, Phelps ME,Schelbert HR. Radiolabeled acetate as a tracer ofmyocardial tricarboxylic acid cycle flux. Circ Res1988; 63:628—634.
1499Volume 30 •Number 9 •September1989
by on July 14, 2018. For personal use only. jnm.snmjournals.org Downloaded from
1989;30:1489-1499.J Nucl Med. C. Gregory Henes, Steven R. Bergmann, Mary Norine Walsh, Burton E. Sobel and Edward M. Geltman Tomography and Carbon-11 AcetateAssessment of Myocardial Oxidative Metabolic Reserve with Positron Emission
http://jnm.snmjournals.org/content/30/9/1489This article and updated information are available at:
http://jnm.snmjournals.org/site/subscriptions/online.xhtml
Information about subscriptions to JNM can be found at:
http://jnm.snmjournals.org/site/misc/permission.xhtmlInformation about reproducing figures, tables, or other portions of this article can be found online at:
(Print ISSN: 0161-5505, Online ISSN: 2159-662X)1850 Samuel Morse Drive, Reston, VA 20190.SNMMI | Society of Nuclear Medicine and Molecular Imaging
is published monthly.The Journal of Nuclear Medicine
© Copyright 1989 SNMMI; all rights reserved.
by on July 14, 2018. For personal use only. jnm.snmjournals.org Downloaded from





























