-
oninvasive quantification of regional myocardialoxygen
consumption has been an elusive and longstanding objective
ofcardiovascular research. Its utilityis analogous to that of
delineation of ventricular function, now readily accomplished by
ventriculography orechocardiography among other methods; or of
assessment of myocardial blood flow. Its potential value
isunderscored by clinical issues such as optimization oftreatment
of patients with ischemic heart disease requiring titration of
myocardial oxygen requirementsand ventricularperformance,and by the
importance ofdelineating viable myocardium after interventions
suchas coronary thrombolysis, essential for identification
ofpatients who may benefit from subsequent additional
Received Feb. 20, 1989; revision accepted June 12, 1989.For
reprints contact: Mary Norine Walsh, MD, Cardiovascular
Division,Washington University School of Medicine, Box 8086,660
S. Euclid Ave., St. Louis, MO 63110.
measures such as angioplasty or coronary artery bypassgrafting.
In addition, elucidation ofthe pathophysiologyof syndromes such as
angina with angiographicallynormal coronary arteries (syndrome X)
or of cardiomyopathies ofdiverse etiologies requires
quantificationof regional myocardial oxygen consumption and
callmation of oxidative metabolic reserve.
Despite the quantitative power of positron emissiontomography
and its sensitivity for detection of labeled,physiologic
substrates, quantification of carbohydrateor fattyacid metabolism
alone does not provide a directmeasure of regional myocardial
oxygen consumption(1,2). We have shown that admixture of diverse
substrates obscures changes in myocardial oxygen consumption
estimated on the basis of metabolism ofindividual substrates such
as glucose or fatty acid (2).In addition, the myocardial handling
of either labeledpalmitate or glucose (or the glucose analogue,
fluorodeoxyglucose) is critically dependent upon the level of
The Journal of Nudear Medicine1798 Walsh,Geltman,Brownetal
Noninvasive Estimation of RegionalMyocardial Oxygen Consumption
by PositronEmission Tomography with Carbon-11 Acetatein Patients
with Myocardial InfarctionMary Norine Walsh, Edward M. Geltman,
Michael A. Brown, C. Gregory Henes,Carla J. Weinheimer, Burton E.
Sobel, and Steven R. Bergmann
Cardiovascular Division, Department oflnternal Medicine,
Washington University School ofMedicine, St. Louis, Missouri
Wepreviouslydemonstratedin experimentalstudiesthat
myocardialoxygenconsumption(MVO2)can be estimated noninvasively
with positron emission tomography (PET) fromanalysisof the
myocardialturnoverrateconstant(k)afteradministrationof carbon-I1
(11C)acetate.To determineregionalk in healthyhumansubjectsandto
estimatealterationsinMVO2accompanyingmyocardialischemia,we
administered[11C]acetateto five healthyhumanvolunteersand to six
patientswith myocardialinfarction.Extractionof [11Cjacetatebythe
myocardiumwas avidandclearancefromthe
blood-poolrapidyieldingmyocardialimagesof
excellentquality.Regionalk was homogeneousin myocardiumof
healthyvolunteers(coefficient variation = 11%). In patients, k in
regions remote from the area of infarction wasnot
differentfromvaluesin myocardiumof
healthyhumanvolunteers(0.061±0.025compared with 0.057 ±0.008
min1). In contrast, MVO2in the center of the infarct
regionwasonly6% of that in remoteregions(p < 0.01).In four
patientsstudiedwithin48 hr ofinfarction and again more than seven
days after the acute event, regional k and MVO2did
notchange.Theapproachdevelopedshouldfacilitateevaluationof the
efficacyof interventionsdesigned to enhance recovery of jeopardized
myocardium and permit estimation of
regionalMVO2andmetabolicreserveundetlyingcardiacdiseaseof
diverseetiologies.
J Nucl Med 30:1798—1808,1989
-
arterial substrate content as well as on the hormonalmilieu
(3—6).
We recently hypothesized that measurement of oxidation of
acetate would provide an indirect measure ofmyocardial oxygen
consumption (7-9). In contradistinction to the case with glucose or
fatty acid, metabolism of acetate is confined virtually exclusively
to mitochondrial oxidation. We have demonstrated in isolated
perfused hearts (7) and canine hearts in vivo (8)that the
extraction of carbon-i 1- (‘‘C)labeled acetateby myocardium is
avid and that the clearance from thetissue is very closely
correlated with both oxidation oflabeled acetate to ‘‘CO2and
with myocardial oxygenconsumption over a wide range of cardiac
workloads.Furthermore, we have demonstrated that the quantitative
relationshipbetween myocardial oxygen consumption and turnover of
[“Clacetateis persistent despitemarked changes in the proportion
of substrate presented to the heart in vivo (9).
The presentstudy was undertakento characterizetheturnover
rateconstant of [‘‘C]acetateby positron emission tomography in
normal human subjects and inpatients with acute myocardial
infarction and to usethe ‘‘Cmyocardial turnover rate constant
to estimateregional myocardial oxygen consumption.
METhODS
SubjectsThe protocol used was approved by the Washington Uni
versityInstitutionalReviewBoard(Human StudiesCommittee). After
the nature ofthe study had been explained to eachsubject, written
informed consent was obtained.
Five male volunteers with mean age of 28 yr (range 25 to36 yr)
comprised the control group. All had normal electrocardiograms,no
history of cardiac disease, and no knowncardiac risk factors. Six
patients (five male and one female)with
transmuralmyocardialinfarction(documented by analysis of plasma
creatine kinase activity and by Q waves on
theelectrocardiogram)werestudiedas well.None had been subjected to
acute interventions such as coronary thrombolysisor balloon
angioplasty.Their mean age was 48 yr (range= 38to 61 yr).One
patienthadsustainedinferiorinfarction,andfivehad sustainedanterior
infarctions.Four
(onewithinferiorandthreewithanteriorinfarction)studiedinitiallywithin48hr
ofinfarction were studied again at least 7 days after infarction to
define sequential changes in [‘‘Cjacetatemetabolismin normal
and infarct zones.
ProtocolEach subject was positioned in Super PElT I, a whole
bodypositronemissiontomographthat
providessimultaneousacquisitionofdata sufficientfor
reconstructionofseven transaxial slices with a
center-to-centerslice separationof 1.5 cm,anda slicethicknessof
1.14cm (10). A transmissionscanofthe chest was obtained with a ring
of germanium-68/gallium68 to correct for photon attenuation ofthe
emitted radiation.The transmission scan was viewed prior to the
collection of
emissiondata to verifyproper positioningof the patient sothat
four to six of the seven
cross-sectionaltransaxialimagingplanestransectedthe
heart.Correctpositioningwas maintamed throughout the study with the
use of a lightbeam andindelible marks on the subject's torso.
Polyurethane moldswere made individually for each subject prior to
each studyand used to stabilizethe head, neck, and upper torso
tominimize movement and maintain identical positions
formultipletomograms.Emissiondata werecollectedin the
highresolutionmode witha
reconstructedresolution(fullwidthathalfmaximum) of 13.5mm.
To characterizemyocardialperfusion,we usedthe diffusible
traceroxygen-15- (‘SO,t½= 2.1 mm) labeled water and amethod
previously developed in our laboratory and validatedin animals and
patients (11—14).After collection of attenuationdata,0.4 mCi/kgof
H2'5Owereinjectedas a bolusviaalarge bore catheter inserted into an
antecubital vein. Datawerecollectedbeginningat the time
ofadministration of tracerand continued for 150 sec in list mode
with time-of-flightcorrection. After a 5-mm interval for decay
ofactivity of tracerto baselinelevels,40 to 50 mCi of
oxygen-15-labeledcarbonmonoxide (C'5O)were administeredby
inhalation to label theblood pool. After a subsequent interval of
30 to 60 sec forclearanceof C'@Ofrom the lungs, data were collected
for 5mm. After an additional 5-mm interval for decay of
radioactivity to baseline levels, 0.4 mCi/kg of[' ‘C]acetate(t@=
20.3mm) were injected as a bolus. In general, ‘‘Cdata
werecollectedfor 30 mm. In some controls, collectionswerecontinued
for as long as 60 mm afteradministration of tracer.
Analysisof TomographicDataPerfusion. To display the distribution
of nutritional perfu
sion after administration of â€@̃Owater, radioactivity
emanatingfromthebloodpoolwascorrectedwiththeuseofC'5Oandamethodvalidatedpreviouslyin
our laboratory(11—14).Ineach pixel of the tomographic
reconstructionobtained afteradministration of
H2'5O,radioactivityemanating from theblood pool was subtracted to
provide an image of blood flowin the myocardium. Data
reconstructedinto cumulative 120-sec images were used to identify
regions of diminished perfusion in heartsof patients with
myocardial infarction.
Metabolism. To characterize qualitatively the distributionof
radiolabeled acetate in the heart and obtain a myocardialimage,
data were reconstructed into a single static 5-mmcomposite scan.
The reconstruction encompasseddata collected from 3 to 8 mm after
administration of tracer, anintervalwhen blood-poolradioactivityhad
declinedsubstantially. Images were used subsequently for placement
of regionsof interestbut not for quantitativeanalysis.
For quantitative analysis, a single midventricular tomographic
slice was selected from the reconstructed tomogramsin normal
control subjects. In patients, the reconstructioncontaining the
infarct region, as delineated from the H2150perfusionscan, was used
for analysis.In the case of
anteriorinfarction,midventriculartomogramswere used. In the caseof
inferior infarction a more apical tomographic plane wasused.
Regions of interest with a volume of 1 cm3 were
placedcircumferentiallyon each tomographic reconstruction.
Formidventriculartomograms,nine regionsof interestwereemployed. For
more apical tomograms, three posterior regionswere identified as
well. An additional region of interest was
Volume30 •Number11 •November1989 1799
-
assigned to the center of the left atrium or the left
ventricularcavityfordeterminationofactivityoftracer in the
bloodpool.
Regionsof interest in tomograms obtained after administration of
[‘‘C]acetateto patients were subdivided to encompass regions of
interest in normal, infarcted, and pen-infarcttissue.Normal
regionswereidentifiedas those fullycontainedwithin regions of
myocardium with normal perfusion (> 50%of maximum flow) judging
from the H2'5Otomograms. “Infarct―zoneswere identifiedas
regionsof hypoperfusionwith< 50% of maximum perfusion. In
addition, the 1 cm3 regionof interest in the center of this zone of
hypoperfusionwasidentified as being the most ischemic zone and
designated“centralinfarct―.Pen-infarct regions on either side
of theinfarct zone weredelineatedas the regionsof interest
immediately adjacent to the infarct but within a zone of
perfusionwith counts exceeding 50% of maximum activity of
H2'5O.
The [‘‘C]acetatemyocardialturnover rate constant
(k),wasobtained from the equation:
q = e@t
where,q = counts/voxel/minute corrected for physical decay,k =
myocardial turnover rate constant, andt = time
It wascalculatedfrom sequential90-120-secframes@A
multiexponential, least squares, curve fitting procedurewas usedto
fit myocardialtime-activitycurvesbeginningat the time ofoccurrence
of maximal myocardial ‘‘Cactivity. Data wereexpressed also as
the myocardial clearance half-time (t@1,=ln2/k).
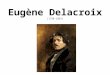
Myocardialoxygen consumption (MVO2)was estimatedfor each defined
region of interest based on the relationshipbetween the myocardial
turnover rate constant, k, and directlymeasuredMVO2in 33
individualstudies in intact dogs(Fig.1) (8,9). Although this
relationship has not been establisheddirectlyin humans, becauseof
ethicalconsiderations,we didnot
feelthatcoronarysinuscatheterizationwasjustifiableinnormal
subjects.Coronary sinus catheterization in
patientsanddeterminationofarterial-venousdifferencescouldprovideestimates
of myocardial oxygen consumption, but would provide global,
ratherthan regional, values.
Because clearance of radioactivity from the arterial bloodwasso
rapid(seeResults)spilloverfrombloodto myocardiumdid not
requirecorrection.Wehavepreviouslydemonstratedin experimental
animals that spillover correction of data obtamed after
administration of [‘‘Cjacetateis unnecessarybecauseofthe rapid
clearancefrom arterial blood (8).
Preparation of TracersOxygen-15 water, C'5O and
[‘‘Clacetatewere prepared as
previouslydescribedin detail (7,15,16).PUrityof['
‘C]acetatewas typicallygreater than 99.5%. Preparations of
200—300mCi,witha specificactivityofgreaterthan
1Ci/mmol,wereachievedroutinely.
StatisticsDataarereportedas
means±standarddeviations.Signifi
cance ofdifferences between groups were assessed with analysis
of varianceand post-hoc unpairedanalysis. Within
groupsdifferenceswerecomparedwith the useofpaired tests.Differences
with a p < 0.05 were considered to be significant.
EI-z
(I)z0C-)
L@J
U)>
a:I-
0S
0.
S
0.;
0. n â€3̃3r@ 0.88ys 0.036X + 0.021
0 I 2 3 4 5 6 7 8 9 0MYOCARDIAL OXYGEN CONSUMPTION
(pmol/g 1mm)FIGURE 1Correlation between the myocardial turnover
rate constantmeasurednoninvasivelywith PETafter i.v.
administrationof [11C]acetateand MVO2measuredby direct
arterialcoronary venous sampling Obtained from 33
individualmeasurements in 18 anesthetized, intact dogs studied
atrest or after myocardial work had been altered wfth sympathetic
stimulation or blockade, or after the pattern
ofmyocardialsubstrateuse had beenchangedby alteringarterial
substrate content after infusion of either glucoseor lipid. The
data presented here Is a summary of theresults from previously
published studies from our laborstory (8,9).Thisrelationshipwas
usedto estimateregionalMVO2in humansfrom the myocardialturnoverrate
conslant.
RESULTS
HemodynamicsNo adverse effects of administration of any
tracer
were observed. All subjects tolerated the tomographicprocedures
well. The rate-pressure product (heart ratex systolic blood
pressure), an index of global myocardial work, was calculated for
all subjects. The ratepressure product was lower in control
subjects undergoing tomography than it was in patients with
infarction(7051 ±1131 bpm x mmHg compared with9517 ±3023, p <
0.05), presumably because of differences inautonomic nervous system
activity. The rate-pressureproduct was also lower at the time of
follow-up 1 wkafter infarction in the four patients studied than it
wasin studies within 48 hr of onset of infarction (7082 ±2654 at
follow-up compared with 9879 ±3332 acutely,p < 0.05).
Assessment of Myocardial PerfusionNutritional perfusion,
assessed with H2'50, was ho
mogeneous in all subjects in the control group (Fig. 2).In
contrast, all patients with myocardial infarction displayed
diminished perfusion in a tomographic regionthat correspondedto the
locus ofthe region of infarction
TheJournalof NuclearMedicine1800 Walsh,Geitman,BrownetaI
-
•285
!14251756 1878
.@
, .@ :@@
@ @‘& ;@
8
FIGURE 2Mid-ventricular, transaxial, tomographic reconstructions
from a representative control subject (P360). On the left is
thereconstruction obtained after administration of 150 water,
corrected for vascular radioactivity. On the right is
thecorresponding tomogram obtained after administration of
[11C]acetate.In these mid-ventricular, transaxial
reconstructions,the septumis on the left, the lateralfreewallon the
right,the anteriormyocardiumtowardthe top, andthe
mitralvalveplane,devoldof
significanttraceruptake,towardthebottom.Concordanceof
distributionof tracerinthe perfusionand metabolicimagesis
evident.The slightdiscontinuityof tracer uptakeseen in the septumin
the H2150imageisrelated to statistical noise induced by correcting
the image for radioactivity emanating from the blood pool. Uptake
of[11C]acetatewas avid and resulted in myocardial images of high
quality in all subjects.
delineated electrocardiographically (Fig. 3). The regionof
diminished perfusion defined with H215O was usedto distinguish
infarct, normal, and pen-infarction regions.
Analysis of Data after Administration of t―CjAcetateAn example
of a midventriculartomographic recon
struction obtained after intravenous administration
of[“Clacetateon a normal subject is shown in Figure 2.The
homogeneity of myocardial ‘‘Cactivity observedand the quality
ofthe image are representativeof resultsin each control.
A reconstruction from a patient with anterior myocardial
infarction is displayed in Figure 3. Both theH215O and the
F'‘C]acetatetomograms show markedlydecreased tracer in the
anterior myocardium and relatively normal distribution ofperfusion
and metabolismin the septal and lateralwalls.
Quantitative AnalysisAs shown directly in studies in
experimental animals
(8,9), and confirmed in the human subjects studiedhere,
[‘‘Cjacetateradioactivityin the blood pool dimin
ished by 90% to 95% from peak radioactivity, usuallywithin 2 mm
(Fig. 4).
For each of the 9—12regions of interest placed
ontomographicreconstructions,a multi-exponential curvefit was used
to characterizedecay-correctedmyocardialtime-activity curves from
the time of occurrence ofmaximal myocardial ‘‘Cradioactivity.
In contrast tothe biexponential clearance of ‘‘Cradioactivity
observed in isolated rabbit hearts (7) and in hearts of dogsin vivo
(8,9), clearance of ‘‘Cwas monoexponential inboth controls and
patients (Fig. 5). This observation isconsistent with the lower
workload seen at rest innonanesthetized, noninstrumented human
subjectscompared with that in anesthetized dogs and with
preliminary observations in humans reportedby Pike et al(17) and by
Henes et al. (18). No second exponentialcomponent could be
identified even in two subjectsstudied for as long as 1 hr
afteradministration of tracer.
Clearance ‘‘Cradioactivity from the myocardiumwas
homogeneous in control subjects (Table 1, Fig. 5).The variation
ofthe turnover rate constant within eachtomogram, reflectedby the
coefficient of variation, was
FIGURE 3Mid-ventriculartomographicreconstructionsof
perfusion(left)andoxidativemetabolism(right)in a patientwith acute,
anterior, myocardial infarction (P354). A large anterior
flowdeficit is evidentin the perfusiontomogram and a concordant
decreasein myocardial oxygen consumptionreflected by decreased
[11C]acetateuptake is evident in the tomogramobtained after
administration of [11C]acetate.
1801Volume30@ Number11@ November1989
-
from k (Fig. 1), in normal human subjects,
calculatedMVO2averaged0.97 ±0.23 @imol/g/min(Table 1).
In contrast to the homogeneous clearance observedin hearts of
control subjects, clearance of radioactivityfrom the myocardium of
patients with infarction washeterogeneous (Table 2, Fig. 5). Uptake
oftracer in thezones ofinfarction was decreasedand the turnover
rateconstant within the infarct zone was markedly diminished,
indicative of a profound diminution of regionalMVO2 (Fig. 6).
Regions immediately adjacent to theinfarct zone also had diminished
MVO2 in comparisonto those regions more remote from the infarct
(Fig. 6).
To define changes in oxidative metabolism over timein infarct
and pen-infarct zones, four patients studiedinitially within 48 hr
of the onset of symptoms werestudied again at least 7 days after
the infarction. In eachofthese patients, uptakeof['
‘C]acetateremained markedly diminished in the infarct zone. The
turnover rateconstant, clearance half-time, and estimated
myocardialoxygen consumption did not change with time (Table3, Fig.
7).
DISCUSSION
Myocardial Imaging with t―CiAcetateIn this study, uptake of
[‘‘C]acetatewas found to be
avid in normal myocardium permitting acquisition ofmyocardial
tomographic images of high quality. Therapid clearance of tracer
from the blood pool results ingood contrast between blood and
myocardium and
0 Remote£ Pen-infarct0 Infarct
2 6 20 24 28TIME(minutes)
N0‘C
-JLU><
FIGURE 4Clearance of 11Cradioactivity from the blood was
rapid.Radioactivity cleared to < 10% of maximum within 2
mmafteradministrationof tracer.
11 ±3% in control subjects. Mean values ofk, clearancehalf-time
and estimates of MVO2 averaged from allregions, were similar to
values obtained from a regionof interest drawn to encompass the
entire left ventricle(Table 1). On the basis of extrapolation from
analysesin experimental animals in which the myocardial turnover
rateconstant was compared with MVO2measureddirectly to yield a
regression equation to estimate MVO2
4
l0@8
6
4
2
86
4
2
02
0 Septum0 AnteriorA Lateral
-JU)x0.C/,I—z3C.)I—U)0@
-JLU
0.
C/)I-
0
—-.-.-- 0a@ 0
0
86
4
2
86
4,
2
0' 5 10 5 20 5 @@iö 15 20TIME(min) TIME (mm)
FIGURE 5Representative myocardial time-activity curves obtained
from one control subject(P336, A) and one patient with
anteriormyocardial infarction (P362, B). Three of the 9—12
regions of interest comprising 1 cm@each are displayed. In hearts
ofindividuals without cardiac disease, clearance of tracer is
uniform, monoexponential, and homogeneous. In contrast, inpatients
with myocardial infarction, initial uptake of [11Cjacetate in the
infarct zone is diminished, and clearance isprolonged, consistent
with a decrease in myocardial oxygen consumption. These examples
from a control subject andfrom a patient with acute myocardial
infarction are typiCalof those seen in all subjects studied.
1802 Walsh,Geltman,BrownetaI TheJournalofNuclearMedicine
-
0
;; .@Q0u—ç@CO' .@
a:COIor...F.@r@.,_@
0
I
I.I@II@ U
I@II@ .i.@
I@II;0 0 ‘j.
‘-0000.26:@
a.Cv)Cs1i-Cs4CsJ@
1-00,-0 @0
?U@@fl@@-do@@ II
2..@ :@
r
U;
@ @1
[email protected]
01
0>
C0.@.
E
.@
@1
.@
I
I
0) CD CsJ0)
,- 0 0 i- 0
10@00,@@CD
I....10 11)0 11),- I- I- C@JC')CO0CsJ
c@.@-:@-c44Cv)c@J0000004141414141411@ C%J 0 I@) CD F@C') CD
00)0),- 0 0 @-00
I
.@
.@
.@
I
>S
Il)
IC')
cs1
C')
c'J
C')
c@J
C')
c@J
C4J'-IDO)CD
I.- 0 0 0 ‘-
.c
I
II
CD ‘-0) CD F'-0 CD CD C's)0),- 0 0 ‘-0
§
0000ar;;00
“1W
0) CD CO ‘-Co
0
000000414141414141
000000000000
I@II@
I@II@
l@II@
00000
CDI@@.01O@-CD F'-
0000000000
It)CsJCO F-.
00000
C@J0COC')P-.
00000
00000
@—00000.: 00000
0C'J0@-1t)t'-.
000000
@ 0 It)0) CD CsJ
@ 00000
:@V Cl)
F-.C@Ji- CD@,-C'-.CO0C')1@ 0 0 ‘-@
,-000@
@00@@
CD F'-CD LI)C@)[email protected]'@1@ 0 0 0@
1803Volume30 5Number11@ November1989
0)
tuc,Ju@0)@.+1I-@ I-@
ciLqcsJc%J,-@@
CsJ
Cs1COC') CD 0 0)1@ @- I-@ C@J i
+1+111+1+1+1C')CO i- 0 CO CO0@c%J'-c@J
I@I@ It) It)
ICSJI@CD@
CDI IC')It) cvi
CqCqc')[email protected])C')F-.C')C@J
@-C@0@F-@CD
0)@ C')00)
C@@C')IO@0 It) C') 00
0) C')@ C')0
CO 0) i- ‘@‘- C') C') 0 CsJ
0 CDC) COCs1
CO CDCD C')Cs4C@J0
‘@.c@J 0) CO F-.@
@ Cvicvici o
j
@iti@oi
-
g:@ [email protected],)
a:@
0) 00
Cd L V
Cl)@ @?8@8@I; a.C@ ociooacil.H II4.'.@ F'.
0@ 01
)( lCDaj @C,)@@‘5 j @:@@iI;.C lcD
w.@ ii
-@ @co8cv8ol3 .@
0 @o8o@lo> 00000aI+I
@, @cv) E
C@ 82 0 It)@E. 0E 01@ @Z8@(I)@ c:@c@@ddIo VC@ 41410414141141
a.0@ coF-.tt)1p@ IIC.) 0) F-.i-C@C@ c@c@od0@0) CS) CSICSJ @0
C.)>-@ c@i @cóCl)Ic,I
0..@ 41+I•@x0 (‘I,-. @“@i@―
C) r-.,.@ ‘@CDIO@0@ Itic;@ :@:@ i-CS)O)It)C@J@
C')
@ c'Jo (Oh) I@'
@51>-@E@@ .@ dd@doI0@ 4141d4141'HI@H
—1C>@ LO@ @-o)II)I0) II@@ C'I'-C')1C'J4 o,_, 000,0@@ 0000
a.
:t:,@ g@ “- 0I@ a:Eci@ d@@;IaWE
@@ +104100+1141
@@@@ >
=.cu)@ d olo@
n@
@ t@
Cl).c@?‘@C
to
.2 .@ C) CO CD@C')C 0 C@ F@I'@0 .,. ,-@
- .C
@:@ @±§@
4.' “@ 10@
@ .@ 0o0o@0I0
Cl) @1@@1I41
C @2 °@@@ 0@@ !@
(3 0 0 010@0 c-I @[email protected]
.@ Cl C') @@i-@'-1tO
a: 0 dcslddääld .@@L@ > 41@:4141@141I41@
@@ C') c',oc@i'-I@ >EE0)@
E 2 ‘@@-ddd@0
I—@ ,.:,.:cvi,@cSJ,.:IIti28c;@ 0 ,- CDCS)0) CD@ 0) c@ 0
@ 4141.H.H4I4IFH.@@ @Ll)'@@c')It)c')ICO.@ 0@ @a.
E Cs) (Dollg@ Cs)(Or•-C0@C')II)
>5 sG8Go8I@ o@i
@ @@I0@
41414141•H'H141 D@C@ @‘•-?@ o@_
äooociälo @@(De
@ @“
4.' V
@ U). +1 >@ca
@a_Q.a.Q.Q.@I
1804 Walsh,Geltman,Brownetal TheJournalofNuclearMedicine
-
C
E
I-z4I-U)z0C-)
wI-4
w>9
20
ii -I-
E
I0
0wI-4-J
U-J4U
-I-
@-@bi*InfarctInfarct--i.::
‘-‘-I . -.
Subjects r@ -I Subjects ________________________I I
PATIENTS PATIENTS
FIGURE 6(A)Histogramdepictingthe
regionalmyocardialturnoverrateconstantfromall regionsin
normalsubjectsandin infarct,central infarct, pen-infarct, and
remote regions in patients with myocardial infarction. (B)
Estimates of regional myocardialoxygenconsumptionin all regionsfrom
normalvolunteersand from infarct,central infarct, pen-infarct,and
remoteregions in patients with myocardial infarction. There was no
statistically significant difference between regions remotefrom
infarction in patients and regions from normal human volunteers.
Regional myocardial oxygen consumptiondiminishedin
pen-infarctregionsin patients,andwas severelydepressedin the zoneof
infarction(p < 0.05 comparedwith remoteregions).
facilitates quantitative analysis of myocardial turnoverrate
without the necessity for correctingfor myocardialspillover from
blood into myocardium (8,18).
In normal subjects, uptake and clearance of
‘‘Cwashomogeneous and monoexponential. Use of the relationship
between k and MVO2 established previouslyin canine hearts in vivo
and the data obtained in thepresent study in human subjects yielded
a calculatedhuman myocardial oxygen consumption value of 0.97
@mol/g/min,somewhat lower but close to that preyously obtained
by direct analysis with invasive procedures (19—21).
In patients with infarction, uptake of [‘‘C]acetateinthe
center of the infarct zone, delineated by perfusionimaging with
H2'5O, was markedly depressed and clearance was prolonged. Both are
a result of diminishedperfusion to the region. The diminished
clearance directly reflects the reduction of myocardial
oxidativemetabolism. Overall oxygen consumption within zonesof
hypoperfusion delineated by H2'5Oin humans was—30%of that in
normal zones, a finding consistentwith the recognized magnitude of
myocardial collateralperfusion in zones ofinfarction (22).
Estimated oxygenconsumption in the center of the hypoperfused
zonewas @—6%of normal. Regions remote from the centerof the
infarction exhibited normal myocardial uptakeand turnover of
tracerindicative of normal myocardialoxidative metabolism.
Pen-infarction zones manifestedprolongation of clearance indicative
of diminished oxidative metabolism. These regionsmay be
metabolically“stunned―.Thus, the diminution ofblood flow to
myocardium within these regions, although not sufficient toinduce
infarction, is sufficient to diminish regionalwork and regional
MVO2.Alternatively,pen-infarctionzones may contain a mixture of
viable and infarcted
cells constituting a heterogeneous population manifesting
phenomena integrated in the tomograms withinselected regions
ofinterest because ofthe limited spatialresolution of PET. This
latter interpretation is supported by the finding that MVO2 in
peri-infarct regionsin patients with infarction studied acutely and
again atleast 7 days after the acute event, at a time by
whichfunction and metabolism in myocardium not destinedto undergo
infarction have recovered, did not change.
Studies in experimental animals have demonstratedthat with
reperfusion, oxidative metabolism assessedwith
[‘‘C]acetaterecovers within 1wk in zones destinedto recover and
is predictive of recovery of ventricularfunction (23). Studies by
others have shown that restoration of ventricularfunction is
predicated on recovery of myocardial oxidative metabolism (24,25).
Although enhanced glycolytic flux is seen in reperfusedmyocardium
(2) and can be demonstrated with fluorine-l8
(‘8f@)fluorodeoxyglucose (25), the prolongedimaging intervals
requiredwith deoxyglucose as well asthe dependency of myocardial
uptake of this tracer onplasma substrate and hormonal
concentrations precludes its use to quantify regional myocardial
oxidativemetabolism.
Technical ConsiderationsResults of this study indicate that the
turnover rate
constant after i.v. administration of [‘‘Cjacetatecan
bequantified by PET. We developed [“Cjacetateas atracer suitable
for assessment of regional myocardialoxygen consumption because it
is metabolized virtuallyexclusively via mitochondrial oxidation
(7—9).Oxidalion ofacetate to CO2in mitochondria is coupled
tightlyto oxidative phosphorylation. We have shown preyously that
the turnover rate in isolated perfused hearts
1805Volume30@ Number11@ November1989
IIfi1r@L1rt1r@—1r@i
-
-a:?E@
-@C@ WV
XC0 @Q
V to
EV
j0E
.@
4-,
Cto
4.'
IE
4-,
I
a.
I
I
CD
3§F-.C000
8@41odo@
00
1@ C')LI)C')
3 88C,J0ooooc;418414141CO 0 ‘-C')It)‘0- ‘-0-CS)0 0000
@00
CDCsJw-CDCO
83883ctc@dod
414141414100COCDF'-It)C')―-0-C')ooc:@c@o00000,-
;;r..ci@: CoF'@41
@CS)1-,t
to‘0-
0) 0CD@@C- Cs)@-C')
+i: 1111110) F'-Cs)0)
@ oiCthC'i, CO'-C')
CSJCD'0COcsjcs@-
4141414141CsJ―-C')CDO)‘0C'@'0'0C'@‘- CS) ‘0 ‘-
Cs)‘0-
LI)
a.ICD'*CD*41a:l1—F-.Ln@o@
I'.-
LI)CS)
aooc,F—‘@
0
i ‘0@C')0 0011@@41410 0 0 Cs) C')F'- CDI')0 00
‘@‘)@C'@1C') CsJC')do cc4141@4141g@qo@0 0 0 0I
E
.@
.@
‘5
u15
§
.@
0
.V?1E
.Cl)
?.@F'-CsJCDc')O
8s8@a00004141414141C')CSJCDOi
dddoo
‘0@
G
@@o+lCOC')0@0
@doo@0
0IO@0)'-
ci
CS)C'Ji-Oe00000c@ctoctct41-H-H-H-H
00000ddc:@c@o
‘0-C')
CD@@°0
@c@c@-H;t!000k
@:@
@IOCO@@
E@ ocdodctc,84141414141
@C')COC')C')0)toCDF'@C')@10@-00000
@ddddd
@0
VCS)10CDIOCCDCDCSJF'-.'0
OCthCthOF-.
4141414141COCSJ0)F'-'00iu@Lti,.:Có,-C@)‘-@-
F—
C'@:C'i-H@; CS)@5@Cs) @;
0)
C@JCs)CsJ It)ItiCó,-1t@cvii-0)0'0C')
41-H-H-H-HF'-.@@@CqIt@0@-00LOCSJ0)10CSJ@
COi,-F'@
CO@-0)+l+l‘@C'iCDCOCO
I-'-
CO0)CO0C'4@@sj,@cö
4141414141LI)C')LI)C')O)
:@c;,@:cocvi‘@ Cs)'-,-.
@D .@ V
2 :@@CSJ10CO10@
C)c@
>@,
.@
a.
Cl)C8
@I
.@@E
@‘0@000
4141414141C')F'-ON-CSJ
@@It)CsJc,ut,-00‘-0Cs)
a.I@CD@ CD-Ha:[email protected].@o@,,,- F—
CD0)
@2
0
01-000IqC4JCS)qC')0'@-000
-H-H-H-H-HCOCOF—LOF'-
@F'@@C―4'0-00000
@3II)0)CD0°F@..@;ti-H000 CO
11)11)oo
0COv-0COi-C')'-'-COcc@OdO4141-H-H-HC')@-CSJi-CsJt-.0C')COO‘@0@'
V
CSJLI)CDLI)@C
@...@
,,,
.@@ :@@
‘E°-
:@@i
C@C‘@
€!.@@(D
W@v@
E•@0a.C@ @C9@‘)E@
§‘5to•.1
ç@a
@:
TheJournalof NuclearMedicine1806 Walsh,Geltman,Brownetal
-
1@
I
::- ‘2 20
‘C DAcute
:- 010 0 Follow-up
@ I.5L-@ 0 Acute@ 008 0 Follow-upI- N
U) 0
@006@ .0U
[1rLthrI.@i ____0
@004w
c@@ 0.5@ 002 U-J> 4
0 Uzc@ @_ _______________________ _______________________
@ I@/ Remote Pen-Infarct Infc@ct Central 0 Remote Pen-Infarct
Infarct Central
A Infarct B InfarctFIGURE 7Histogram displaying the myocardial
turnover rate constant, k (A), and estimated myocardial oxygen
consumption (B)from four patients studied acutely and again at
least 7 days after the acute event. There was no change in regional
kor MVO2with time in any region.
parallels regional myocardial oxygen consumption overa wide
range of physiologic and pathophysiologic conditions including
ischemia and reperfusion (7). Comparisons of the myocardial
turnover after intravenousadministration of [“Cjacetate with
direct measurements of myocardial oxygen consumption have
demonstrated the relationship between the myocardial turnover rate
constant (k) detected externally with PET,and MVO2 over a wide
range (Fig. 1) (8,9). This relationship is not altered by changes
in myocardial workor by the pattern of substrate utilization (9).
Despitethe fact that acetate is avidly extracted by the myocardium
with an extraction fraction of 30—50%,its oxidation does not
account for a largefraction of myocardialenergy supply because it
circulates in such low concentrations in normal human
subjects(80—100Mmol)(26).Nonetheless, the relationship between
the myocardialturnover rate constant and MVO2 has not been
established directly in human beings. Values of MVO2 inhumans
estimated by extrapolation of the relationshipobtained directly in
dogs yield values that are somewhatlower than those that have been
measured in humansubjects (19—21).We recently reported that the
relationship between k and the rate-pressureproduct (anindex of
myocardial work and therefore of myocardialoxygen consumption)
obtained in healthy human volunteers was indistinguishable from the
relationship obtamed in experimental animals (18). Nonetheless,
thediscrepancy in values of MVO2 obtained nomnvasivelyin the
present study with values obtained by otherinvestigatorsusing
invasive techniques may reflect atrue interspecies difference in
the relationship betweenk and MVO2. Although the
rate-pressureproduct canbe used to estimate MVO2in normal subjects,
it reflectsglobal, rather than regional, MVO2. In contrast, thePET
approach developed permits sequential assessments of regional
MVO2.
In the present study, areas of normal and hypoper
fusion were estimated using H2'5O and a techniquedeveloped
previously in our laboratory to correct
dataforintravascularradioactivity.Regional perfusion usingthis
approach correlates very closely with regional bloodflow estimated
with radiolabeledmicrospheres(11-13).In addition, we have
demonstrated the utility of thistechnique in patients with coronary
artery disease (14).Although tomography with H2150 permitted
independent delineation of normal from ischemic
myocardium,correction ofmyocardial H2'5O for vascular radioactivity
(which requires an independent measure of theblood pool with C'50)
results in images of relativelylow signal-to-noise ratios. Although
we recently vaildated a mathematical approach to quantitate
myocardial perfusion in absolute terms (i.e., ml/g/min)
usingH2'5Oand PET which does not requirean independentmeasurement
of the blood pool, we chose not to usethe quantitative approach in
the current study becauseit is less sensitive to estimates of flow
in infarctedmyocardium (27).
Clinical ImplicationsThe resultsofthe present study indicate
that positron
emission tomography with [‘‘C]acetate,a tracer of myocardial
oxidative metabolism, provides myocardial images of high quality
and permits estimation of regionalmyocardial oxygen consumption
with results consistentwith those obtained previously by invasive
measurements. Oxidative metabolism in the center of zones
ofinfarction is markedlydepressed and, in the absence ofacute
interventions, does not change with time. Acuteinterventions are
likely to restore oxidative metabolismin jeopardized myocardium and
can therefore be evaluated with the approach developed here.
Accordingly,quantification of myocardial oxygen consumption
with[‘‘C]acetateand positron tomography offers promisefor
objective, noninvasive characterization of the relative benefits
ofdiverse interventions designed to salvage
1807Volume 30 SNumber 11@ November1989
-
H2'5O.Circulation 1984;70:724—733.12. Knabb RM, Fox KAA, Sobel
BE, Bergmann SR.
Characterization ofthe functional significance of subcritical
coronary stenoses with H215O and positronemission tomography.
Circulation 1985; 71:1271—1278.
13. Knabb RM, Rosamond TL, Fox KAA, Sobel BE,Bergmann SR.
Enhancement of salvageof reperfusedischemicmyocardium by diltiazem.
JAm Coil Cardiol1986;8:861—871.
14. Walsh MN, Bergmann SR, Steele RL, et al. Deineation of
impaired regional myocardial perfusion bypositron emission
tomography with H2'50. Circulation1988;78:612—620.
15. Welch MJ, Ter-Pogossian MM. Preparation of shorthalf-lived
radioactive gases for medical studies. RadRes
1968;36:580—587.
16. Welch MJ, Kilbourn MR. A remote system for theroutine
production of oxygen-iS radiopharmaceuticals. J Label Comp
Radiopharmaceuticals 1985; 22:1193—1200.
17. Pike VW, Eakins MN, Allan RM, Selwyn AP. Preparation of
[1-―C]acetate—anagent for the study ofmyocardial metabolism by
positron emission
tomography.IntJApplRadiatlsot1982;33:505—512.
18. Henes GC, Bergmann SR, Walsh MN, Sobel BE,Geltman EM.
Assessment of myocardial oxidativemetabolic reserve with positron
emission tomographyand carbon-i 1-acetate. J Nuci Med 1989;
30:1489—1499.
19. Kitamura K, Jorgensen CR, Gobel FL, Taylor HL,Wang Y.
Hemodynamic correlates ofmyocardial oxygen consumption during
upright exercise.JApplPhysiol1972;32:516—522.
20. Nelson RR, Gobel FL, Jorgensen CR, Wang K, WangY, Taylor HL.
Hemodynamic predictors or myocardial oxygen consumption during
static and dynamicexercise.Circulation1974;50:1179—1189.
21. Gobel FL, Nordstrom LA, Nelson RP, Jorgensen CR,Wang Y. The
rate-pressure product as an index ofmyocardial oxygen consumption
during exercise inpatients with angina pectoris. Circulation
1978;57:549—556.
22. Knabb RM, Bergmann SR. Fox KAA, Sobel BE. Thetemporal
pattern of recovery of myocardial perfusionand metabolism
delineated by positron emission tomography after coronary
thrombolysis. J Nucl Med1987;28:1563—1570.
23. Brown MA, Nohara R, Vered Z, Perez JE, BergmannSR. The
dependence of recovery of stunned myocardium on restoration of
oxidative metabolism [Abstract].Circulation1988;78:11—467.
24. Taegtmeyer H, Roberts AFC, Raine AEG. Energymetabolism in
reperfused heart muscle: metabolic correlates to return of
function. JAm Coil Cardiol 1985;6:864—870.
25. SchwaigerM, SchelbertHR, Ellison D, et al. Sustainedregional
abnormalities in cardiac metabolism aftertransient ischemia in the
chronic dog model. J AmCoilCardiol1985;6:336—347.
26. In: Lentner C, ed. Geigy Scientific tables. Basle:
CibaGeigy, 1984;3:107.
27. Bergmann SR. Herrero P, Markham J, WeinheimerCI, Walsh MN.
Noninvasive quantitation of myocardial blood flow in human subjects
with oxygen-iSlabeled water and positron emission tomography. JAm
Coil Cardiol: in press.
jeopardized, ischemic myocardium. In addition, theapproach
developed should be useful for evaluatingregional MVO2 and
metabolic oxidative reserve in thehearts of patients with cardiac
disease of diverse etiologles and their response to therapy.
ACKNOWLEDGMENTS
The authors thank Theron Bairdand ColleenSchaab,RNfor technical
assistance, David Marshall, BS, James Bakke,MS, and the staff of
the Washington University MedicalCyclotron for preparationof
tracers;and Becky Leonard forpreparationof the typescript.
This work was supported in part by National Heart, Lungand Blood
Institute, Grant HL17646, SpecializedCenter ofResearchin
IschemicHeart Disease.
REFERENCES
1. Bergmann SR, Fox KAA, Geitman EM, Sobel BE.Positron emission
tomography ofthe heart. Prog CardiovascDis1985;28:165—194.
2. Myears DW, Sobel BE, Bergmann SR. Substrate usein ischemic
and reperfused canine myocardium: quantitative considerations. Am
JPhysiol(Heart CircPhysiol)1987;253:H107—H114.
3. Schelbert HR, Henze E, Schon HR, et al. C-i 1 palmitate for
the noninvasive evaluation ofregional myocardial fatty acid
metabolism with positron computedtomography. III. In vivo
demonstration of the effectsof substrate availability on myocardial
metabolism.Am HeartJ 1983;105:492—504.
4. Schelbert HR, Henze E, Sochor H, et a!. Effects
ofsubstrateavailabilityon myocardialC-i 1 palmitatekinetics by
positron emission tomography in normalsubjectsand patients with
ventricular dysfunction. AmHeartf 1986;111:1055—1064.
5. Phelps ME, Hoffman El, Scm C, et al. Investigationof
[‘8F]2-fluoro-2-deoxyglucose for the measure ofmyocardial glucose
metabolism. J Nuci Med 1978;19:1311—1319.
6. Merhige ME, Ekas R, Mossberg K, Taegtmeyer H,Gould KL.
Catecholamine stimulation, substratecompetition, and myocardial
glucose uptake in conscious dogs assessed with positron emission
tomography. Circ Res 1987; 61:II-l24—II-129.
7. Brown MA, Marshall DR, Sobel BE, Bergmann SR.Delineation
ofmyocardial oxygen utilization with carbon- 11labeled acetate.
Circulation 1987;76:687—696.
8. Brown MA, Myears DW, Bergmann SR. Noninvasiveassessment of
canine myocardial oxidative metabolism with carbon-i 1 acetate and
positron emissiontomography. JAm CoilCardiol 1988;
12:1054—1063.
9. Brown MA, Myears DW, Bergmann SR. Validity ofestimates of
myocardial oxidative metabolism withcarbon-i 1-acetate and positron
emission tomographydespite altered patterns ofsubstrate
utilization. J NuciMed 1989;30:187—193.
10. Ter-Pogossian MM, Ficke DC, Yamamoto M, HoodJT. Super PElT
I: A positron emission tomographutilizing photon time-of-flight
information. IEEETransMedlmagi 1982;3:179—187.
11. Bergmann SR, Fox KAA, Rand AL, et al. Quantification of
regional myocardial blood flow in vivo with
1808 Walsh,Geltman,Brownet al TheJournalof NudearMedicine