Embed Size (px)
Citation preview

SCIENTIFIC PAPER
Assessment of concomitant testicular dose with radiochromic film
Katherine Fricker • Christine Thompson •
Juergen Meyer
Received: 3 April 2013 / Accepted: 17 June 2013
� Australasian College of Physical Scientists and Engineers in Medicine 2013
Abstract To assess the suitability of EBT2 and XRQA2
Gafchromic film for measuring low doses in the periphery
of treatment fields, and to measure the accumulative con-
comitant dose to the contralateral testis resulting from CT
imaging, pre-treatment imaging (CBCT) and seminoma
radiotherapy with and without gonadal shielding. Superfi-
cial peripheral dose measurements made using EBT2
Gafchromic film on the surface of water equivalent mate-
rial were compared to measurements made with an ioni-
sation chamber in a water phantom to evaluate the
suitability and accuracy of the film dosimeter for such
measurements. Similarly, XRQA2 was used to measure
surface doses within a kilovoltage beam and compared
with ionisation chamber measurements. Gafchromic film
was used to measure CT, CBCT and seminoma treatment
related testicular doses on an anthropomorphic phantom.
Doses were assessed for two clinical plans, both with and
without gonadal shielding. Testicular doses resulting from
the treatment of up to 0.83 ± 0.17 Gy were measured per
treatment. Additional doses of up to 0.49 ± 0.01 and
2.35 ± 0.05 cGy were measured per CBCT and CT image,
respectively. Reductions in the testicular dose in the order
of 10, 36 and 78 % were observed when gonadal shielding
was fitted for treatment, CT and CBCT imaging, respec-
tively. Gafchromic film was found to be suitable for
measuring dose in the periphery of treatment fields. The
dose to the testis should be limited to minimise the risk of
radiation related side effects. This can be achieved by using
appropriate gonadal shielding, irrespective of the treatment
fields employed.
Keywords Seminoma � Imaging dose � Peripheral dose �Gafchromic film
Introduction
Testicular cancer is rare, having a global prevalence of
0.8 % of male cancers, with a slightly increased incidence
in westernised countries (1.2 % in New Zealand) [1]. It is
the most common cancer in males of age 15–39 years in
New Zealand [1] but remains one on the most curable
cancers if treated in the early stages (5-year relapse-free
rate of 95–97 %) [2, 3].
Testicular seminoma has a predictable disease progres-
sion typically metastasising to the paraaortic (PA) lymph
nodes. For patients with a history of un-descended testes
and/or abnormal nodal drainage, there is also an increased
risk of disease spread to the pelvic and ipsilateral common
iliac lymph nodes [4]. Stage I seminoma is treated by
orchidectomy followed by one of the following: surveil-
lance, chemotherapy or radiotherapy to the PA lymph
nodes, including pelvic and iliac lymph nodes where
appropriate [4]. Lead shielding is routinely used to protect
This work was presented in part at Engineering and Physical Sciences
in Medicine (EPSM) Conference in the Gold Coast, Australia,
December 2012.
K. Fricker � J. Meyer
Department of Physics and Astronomy, University
of Canterbury, Private Bag 4800, Christchurch 8140,
New Zealand
K. Fricker (&) � C. Thompson
Cancer and Blood Services, Auckland City Hospital,
2 Park Road, Grafton, Auckland 1023, New Zealand
e-mail: [email protected]
J. Meyer
Department of Radiation Oncology, University of Washington,
1959 NE Pacific Street, Box 356043, Seattle, WA 98195, USA
123
Australas Phys Eng Sci Med
DOI 10.1007/s13246-013-0208-y

the remaining testis from radiation for patients undergoing
radiotherapy inclusive of the pelvic and ipsilateral common
iliac lymph nodes. Even though the testis is well removed
from the PA irradiation fields, scattered dose in the order of
1–6 % of the prescribed dose has been measured using
thermoluminescent detectors (TLDs) [5, 6]. The testicular
dose had been reported to be reduced to 0.4–3 % when
some form of gonadal shielding was fitted [5, 6].
Radiation induced cancer to the contralateral testis and the
late side effects of infertility are potential risks for survivors of
testicular seminoma due to their long life expectancy [7–9].
A retrospective study assessing patients at least 3 years
after treatment for testicular cancer, which included
orchidectomy followed by surveillance, radiotherapy and/
or chemotherapy, found a 30 % decrease in fertility [9].
Radiotherapy was found to have the greatest detrimental
effect [9]. Additionally, following radiotherapy for testic-
ular seminoma, patients are more likely to develop (a
second) testicular cancer compared with the general pop-
ulation [10, 11].
Radiotherapy is not the only contributor to dose in the
periphery of the treatment field. Healthy tissue will receive
dose contributions from planning CT and pre-treatment
imaging in the order of mGy [12, 13]. Brenner et al. [14]
suggested that approximately 1.5–2.0 % of all cancers in
the United States may be related to the radiation dose from
CT studies. Similarly, Berrington de Gonzalez et al. [15]
estimated that approximately 2 % of the cancers diagnosed
every year in the United States could be CT related.
Contrary to this, Van Walraven et al. [16] concluded that
the excess risk of second cancers among testicular cancer
survivors is not associated with diagnostic imaging.
Despite the conflicting reports on the role of diagnostic
imaging in cancer induction, it is important to quantify and
interpret the peripheral doses delivered during seminoma
radiotherapy.
In this work the usefulness of clinically available EBT2
and XRQA2 Gafchromic film for measuring low peripheral
dose was assessed. Subsequently, the accumulative dose a
patient receives while undergoing radiation treatment for
testicular seminoma was measured. Dose contributions from
CT, CBCT and treatment scatter were considered. Both PA
lymph node and extended field treatments were assessed
with and without gonadal shielding fitted. Although treat-
ment and imaging related dose has been studied indepen-
dently [5, 6, 17, 18], the total concomitant treatment related
dose has yet to be investigated using Gafchromic film.
Methods and materials
In Gafchromic film calibration, the process of calibrating
Gafchromic film for measuring dose in the periphery of
18 MV seminoma treatment fields and related imaging
fields is presented. In Dosimeter comparison, the suitability
of Gafchromic film for measuring low doses in the
periphery of treatment fields was assessed. This is followed
by the measurements of seminoma treatment related dose
in Measurements.
Gafchromic film calibration
Gafchromic film (International Speciality Products (ISP),
Wayne, NJ) is a type of self-developing radiochromic film,
which since its introduction in 2004 is gaining popularity as a
suitable dosimeter in radiology [19–21] and radiation oncol-
ogy [22–24] applications. Two types of Gafchromic film were
used; EBT2 for measurements in a megavoltage (MV) beam
and XR-QA2 for measurement in kilovoltage (kV) beams.
EBT2 film calibration
EBT2 Gafchromic film was calibrated in a 6 and 18 MV
beam using a Varian iX linear accelerator (Varian Medical
Systems, Palo Alto, CA). The majority of calibration
measurements were made for doses less than 50 cGy to
ensure accuracy in the film calibration at low doses. Gaf-
chromic film was cut into 4 9 4 cm2 pieces and marked to
keep the orientation of the film consistent. A film piece was
placed in a 30 9 30 9 20 cm3 stack of Solid Water�
(Gammex RMI, Middleton, WI, USA) at a depth of 5 cm.
The centre of the film was aligned with the central axis of
the beam along the crosswires. The linear accelerator dose
delivery is linear down to 3 Monitor Units (MU), where 1
MU is defined as 1 cGy to Dmax at a source to axis distance
(SAD) of 100 cm, in a 10 9 10 cm2 field. In order to
ensure linearity of the beam at low doses, the solid water
was placed at an extended SSD. The ratio of dose delivered
at isocentre in a water phantom (10 9 10 cm2 field, 95 cm
SSD) to that at the extended SSD in solid water (5 cm
depth, 5 9 5 cm2, 200 cm SSD) was used to correct for the
extended SSD setup. The correction factor, Cext, accounts
for the change in field size, SSD and any discrepancies
between measurements made in the water and solid water
phantoms. 12 pieces of film were irradiated with increasing
dose over the range 0–150 cGy. This was repeated three
times. The dose, D, to the films was calculated from the
delivered MU, with adjustments made for the deviation of
the machine output from calibration, Oc, which is the ratio
between the current machine output and that at calibration,
the placement of the film at depth and the extended SSD
setup and is given by
D ¼ MU � Oc � TMR� Cext ð1Þ
The tissue maximum ratio at a depth of 5 cm was 0.918
and 0.990 for 6 and 18 MV, respectively.
Australas Phys Eng Sci Med
123

The film pieces were digitised one at a time using an
Epson Expression 10000XL scanner (Seiko Epson Corpo-
ration, Nagana, Japan) 24 ± 1 h post irradiation. Films
were placed at the centre of the scanner bed, in a consistent
landscape orientation, with the short edge of the original
film parallel to the scanning direction and the polyester
substrate layer facing the glass. The scanner was used in
professional mode, with software selections transmission
and positive film and with all filters and colour corrections
turned off. Images were acquired in 48-bit colour, using a
resolution of 72 dpi and saved in tagged image file format
(TIFF). The scanner was switched on 30 min prior to use
and a preview, followed by three scans to warm up the
scanner before film digitisation commenced [25, 26].
Additionally, a preview scan was performed prior to each
scan [26]. Gloves were worn at all times when handling the
film. The image files were imported into MATLAB�
(MATLAB R2011a, The MathWorks Inc., Natick, MA)
and the central 58 9 58 pixels (2 cm2) were extracted and
separated into red, blue and green channels. Care was taken
to exclude any film area within 0.5 cm from a cut film
edge. A correction recommended by the manufacturers was
applied to the red channel data to smooth out possible
inconsistencies in the thickness of the active layer [27].
The pixel values were converted to optical density as
follows:
OD ¼ � logðpixel value=65535Þ ð2Þ
For each film piece, the mean optical density of the cor-
rected red channel data was plotted against the applied dose
to establish the calibration curve. The mean of the three
calibration curves was used for film analysis. For all EBT2
dosimetry measurements, the above scanning protocol was
used and unless stated otherwise, the central 0.5 9 0.5 cm2
(14 9 14 pixels) was extracted for film analysis.
EBT2 Gafchromic film is designed for use in the energy
range 50 kiloelectron volt (keV) into MV and with sensi-
tivity down to 1 cGy. Although the treatment, CBCT and
CT beam energies were within the suitable range, the
expected dose from CBCT and CT was B1 cGy and
therefore the use of EBT2 was limited to MV photon
irradiations.
XR-QA2 film calibration
XR-QA2 Gafchromic film is radiochromic film designed
for dosimetric use in the energy range 20–200 kVp and
within the recommended dose range 0.1–20 cGy, making it
suitable for CBCT and CT applications.
XR-QA2 Gafchromic film was calibrated for mea-
suring surface dose from cone-beam CT and CT image
acquisition. Because of the strong energy dependence of
the film in the kV energy range, the beam qualities of
the X-ray sources were determined prior to calibration.
The X-ray beam qualities of an On-Board Imager�
(OBI) and cone-beam CT capable Varian Linear
Accelerator were measured for the default CBCT pro-
tocols (100, 110 and 125 kVp), which are used clini-
cally in the department. To assess the greatest range of
half value layers (HVLs) the full bowtie filter was fit-
ted. A Piranha multimeter (RTI, Sweden) was used to
evaluate the effects of the bowtie filter by measuring
HVLs on the central axis and at longitudinal displace-
ments up to 10 cm. The HVLs ranged 4.9–7.6 mm Al
(mean HVL = 6.3 mm Al) over all assessed positions.
The mean beam quality on the central axis from the 3
protocols was 5.5 mm Al. The HVL increased off axis
due to beam hardening.
According to manufacturer’s specifications, the Siemens
Somatom Sensation Open helical scanner (Siemens Medi-
cal Solutions, Erlangen, Germany) HVL was 9.1 mm Al
for a 120 kVp imaging protocol.
The XR-QA2 Gafchromic film was calibrated on an
XStrahl 300 X-ray Therapy Unit (XStrahl Ltd., Surrey,
UK) using a 150 kVp beam with beam quality
HVL = 6.0 mm Al, similar to those expected during
CBCT acquisition. A 180 kVp beam with beam quality
HVL = 9.5 mm Al was used to calibrate the film for
measurements on CT.
Gafchromic XR-QA2 film was cut into 4 9 4 cm2 pie-
ces and marked with reference to the initial film orienta-
tion. The film was placed on the surface of a
30 9 30 9 13 cm3 Solid Water� phantom and a graphite
ionisation chamber was placed at a depth of 2 cm in the
solid water to record the dose at depth. The film was cal-
ibrated under the beam reference conditions (30 cm SSD,
8 cm circle applicator for 150 kVp and 50 cm SSD,
10 9 10 cm2 applicator for 180 kVp). 10 pieces of film
were irradiated with increasing dose over the range
0–20 cGy. This was repeated three times for each energy.
The delivered dose, D, to the film pieces was calculated
from the recorded ionisation chamber dose, Dion, with
corrections made for measuring at depth, percentage depth
dose (PDD), and in a Solid Water� phantom, Cp, and is
given by:
D ¼ Dion � Cp
PDDð3Þ
The PDD at 2 cm for the given beams was PDD150 kVp =
76.1 % and PDD180 kVp = 84.7 %. The difference between
ion chamber measurements made in water and Solid
Water� was 4.1 % (Cp = 1.041) and 3.7 % (Cp = 1.037)
for 150 and 180 kVp, respectively.
The same film digitisation and analysis process was
followed as with EBT2 except the films were digitised in
reflection mode with software selection photo.
Australas Phys Eng Sci Med
123

Dosimeter comparison
The dose response of Gafchromic film was investigated to
determine the suitability of using this dosimeter in primary
kV and peripheral region of MV beams. Dose in the
peripheral regions of the MV treatment field is complex;
with dose contributions from scatter within the patient
(internal scatter), leakage from the head of the treatment
machine (head leakage) and collimator scatter. Internal
scatter is the major contributor of dose in the near
periphery of the treatment field, having spectra peaks near
500 keV, while head leakage dominates further a field [28].
The out-of-field dose is largely dependent on beam energy,
field size and distance from the field edge [28–30]. The
photon contribution decreases exponentially with distance
from the field and the neutron contribution, which is non-
negligible for beam energies [15 MV, is independent of
distance from the field but decreases with depth in tissue
[31]. All these factors influence the choice of appropriate
dosimeter to quantify peripheral dose.
MV beam
EBT2 Gafchromic film measurements were compared to
those made with an IBA CC13 Ionisation Chamber (SN
6690) which, due to low angular dependence and weak
energy dependence across a broad spectrum (100 kVp to 50
MV), is a suitable reference dosimeter for out of field
measurements [32]. The dosimeter comparison was per-
formed using a Varian iX 6 MV beam. The response to
higher energies was assumed to be similar since the energy
dependence of EBT2 is small in the MV energy range [33].
The response of the ionisation chamber and UNIDOS
electrometer system (PTW, Freiburg, Germany) was
established for the delivery of a range of doses
(1.9–186.2 cGy). A Scanditronix-Wellhofer water phantom
system (Scanditronix-Wellhofer, Uppsala, Sweden) was set
up with the ionisation chamber positioned at a depth of
5 cm in a 10 9 10 cm2 field, at 95 cm SSD. The mean of
two readings were recorded for each dose delivery.
Peripheral dose measurements were made at increasing
distances from the edge of a 10 9 10 cm2 irradiated field
using an ionisation chamber with the effective point posi-
tioned on the surface of the water, 1 cm from the edge of the
field. Two peripheral dose measurements were made for the
dose delivery on the central axis of 101.4 cGy to dmax.
Measurements were repeated at 2, 3, 4, 5, 6, 8 and 10 cm
from the field edge and again at 3, 4, 5, 6, 8 and 10 cm for the
delivery on the central axis of 202.9 cGy to dmax.
3 9 3 cm2 pieces of EBT2 film were positioned on the
surface of a 30 9 30 9 20 cm3 stack of Solid Water�
(95 cm SSD), at distances 1, 2, 3, 4, 5, 6, 8 and 10 cm from
the edge of a 10 9 10 cm2 field. Individual sets of film
pieces were exposed to peripheral dose from dose deliv-
eries on the central axis to dmax of 101.6 and 203.3 cGy,
respectively. These measurements were repeated three
times and the film was digitised 24 h later. The uncertainty
in the ion chamber measurements was 1 % as specified by
the manufacturers.
kV beam
In order to accurately measure dose within CBCT and CT
fields, the suitability of XR-QA2 Gafchromic film for
measuring dose within kV beams was determined. All
measurements were performed using the XStrahl 300 X-ray
Therapy Unit.
3 9 3 cm2 pieces of XR-QA2 Gafchromic film were
fixed centrally using tape on a stack of solid water, at least
10 cm high to ensure sufficient backscatter. A NE2571
graphite cylindrical ionisation chamber was placed at a
depth of 2 cm on the central axis. Measurements were
made under reference conditions for deliveries of 1.1, 3.2,
5.2 and 10.3 cGy. The film was digitised 46 h after
irradiation.
Measurements
Treatment planning
A Rando Phantom (Alderson Research Laboratories, Long
Island City, New York), fitted with a wax scrotum (den-
sity = 0.9 g/cm3) which was moulded in the department
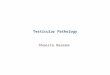
workshop, was positioned on the CT couch. Three surface
measurement points were identified and marked with tape;
one on the anterior scrotal surface, one on the posterior
scrotal surface and one on the abdomen, 5 cm superior to
the superior edge of the wax mould. These can be seen in
Fig. 1. In addition to identifying the measurement points,
the tape markings protected the Gafchromic film from wax
residue. Lead gonadal clam-like shielding is used at treat-
ment to protect the remaining testis, however, this results in
image artefacts if fitted at CT imaging. To accommodate
this, a replicate constructed from PVC, which is used
clinically, was fitted. Both the pseudo and lead clam
gonadal shielding were crafted in the department work-
shop. The phantom was scanned on a Siemens Somatom
Sensation Open helical scanner (Siemens Medical Solu-
tions, Erlangen, Germany) following departmental protocol
for pelvis CT scans (120 kV, 148 mA, 3 mm slice thick-
ness). The scan extended from the T7/T8 joint to mid
femur.
Two treatment plans consisting of anterior/posterior
parallel opposed beams were created using 18 MV pho-
tons in Pinnacle3 (Philips Medical Systems, Milpitas
Australas Phys Eng Sci Med
123

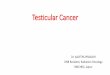
CA). The PA plan consisted of a rectangular field 20 cm
long and 8 cm wide in the abdominal region to include
the PA lymph nodes with a prescribed dose of 20 Gy in
10 fractions. The kidneys were shielded by multileaf
collimators (MLCs). This treatment was prescribed to
100 % of the dose at the isocentre, which corresponds
to the zero slice in the data set. The posterior beam
(Gantry = 180�) was a mirror of the anterior beam
(Gantry = 0�). The anterior beam digitally reconstructed
radiograph (DRR) in Fig. 2 shows the treatment field and
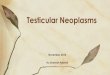
kidney shielding. The second treatment plan, commonly
referred to as a dogleg (DL), was an extension of the PA
to include the ipsilateral pelvic and common iliac lymph
nodes while avoiding the remaining testis, with a pre-
scribed dose of 30 Gy in 18 fractions. The prescription
isocentre was positioned more inferiorly than in the PA
treatment plan and MLCs were used to shield the kidneys
and the remaining testis (Fig. 3). Again, the posterior
beam was a mirror of the anterior treatment beam. The
isodose distributions from the respective plans are shown
in Figs. 2 and 3.
CT
The Rando anthropomorphic phantom was positioned on
the CT scanner bed and aligned with the lasers.
1.5 9 3 cm2 XR-QA2 Gafchromic film strips were secured
with tape at the anterior and posterior scrotal positions and
a 3 9 3 cm2 piece of film was placed at the abdominal
position, ensuring the tape extended no further than 0.5 cm
over the film edge. These film piece dimensions were used
for all measurements unless stated otherwise. The scan was
carried out as per departmental protocol (see ‘‘Treatment
planning’’). The measurements were repeated three times
with and three times without the clam shielding fitted. An
unexposed film piece was used for each scan. In keeping
with calibration, the film was digitised 46 h post irradiation
and analysed as previously described.
CBCT
Rando was positioned on the treatment couch with the XR-
QA2 film and lead shielding in place and aligned with the
.tnemecalpmlifcimorhcfaG(b).dettifgnidleihsdaellluF(a)
Fig. 1 a Rando set up on the
treatment couch with XR-QA2
film positioned at the
measurement points. The
treatment gantry angle is not
shown. b Half the clam
shielding is removed showing
the placement of the film
dosimeter. (The posterior scrotal
measurement point is not seen.)
(a) A digitally reconstructed radiograph of the (b) A coronal view of the isodose distribution at the.tniopecnereferTC.maebtnemtaertroiretna
Fig. 2 The paraaortic treatment
plan. a The centre of the beam is
aligned with the isocentre (red
wireframe sphere). b The pink
and red isodose lines represent
the 95 and 100 % dose
coverage, respectively
Australas Phys Eng Sci Med
123

lasers to the CT reference point. The half bow tie was fitted
and a pelvis CBCT image, using the standard imaging
protocol (125 kVp, 706 mA s, 360�), was taken for pre-
treatment image matching. The CBCT field was 16 cm
wide, inclusive of the abdominal measurement point;
however, the scrotum lay out of the imaging field. Three
CBCT images were performed with and three without the
shielding fitted.
Treatment
EBT2 Gafchromic film was cut to size and secured in place
using tape. Rando was set up on the treatment couch, with
the gonadal shielding fitted, using localisation lasers to
match the position at CT. One fraction of the PA treatment
was delivered. A total of three measurements with shield-
ing and three without shielding were performed. Mea-
surements were carried out in the same manner for the DL
treatment plan delivery.
Results
A. Dosimeter comparison
MV beam
The mean (95 % CI) of the measurements was normalised
to the ionisation chamber water surface dose measurements
at the respective distances. These values are compared in
Fig. 4.
Overall, EBT2 tended to overestimate the dose. In one
instance, the EBT2 measurement was 40 % greater than the
ionisation chamber. This translates to an overestimation
of 0.69 cGy. The maximum variation from the CC13
ionisation chamber measurements across the range of dose
deliveries was 1.3 cGy.
kV beam
The mean (95 % CI) of the measurements was calculated
and the numerical values were normalised to the applied
dose. The ratios are represented graphically in Fig. 5.
XR-QA2 measures within 5 % of the ionisation cham-
ber measurements for doses above 3 cGy but overestimates
the dose by approximately 25 % for a dose delivery of
1.1 cGy. This dose is approaching the limit of the recom-
mended dose range 0.1–20 cGy. XR-QA2 film has excel-
lent precision across the delivered dose range. Overall, XR-
QA2 is in good agreement with the ionisation chamber for
doses above 3 cGy.
(a) A digitally reconstructed radiograph of the (b) A coronal view of the isodose distribution.tniopecnereferTCehtta.maebtnemtaertroiretna
Fig. 3 The Dogleg treatment
plan. a The MLCs shielding the
kidneys and testis can be seen in
the DRR. b The turquoise, red
and pink isodose lines represent
the 102, 100 and 95 % dose
coverage, respectively
Fig. 4 EBT2 Gafchromic film measurements made in the periphery
of a 10 9 10 cm2 6 MV beam, for a delivery of 101 and 203 cGy to
dmax on the central axis, were normalised to those measured with a
CC13 ionisation chamber
Australas Phys Eng Sci Med
123

B. Measurements
CT and CBCT imaging
The mean (95 % CI) of the measurements recorded while
acquiring images is given in Table 1. For CBCT imaging
using XR-QA2, a dose reduction to the testis of more than
60 % is seen when the lead shielding is fitted. With the
pseudo shielding fitted, the dose to the testis from CT
acquisition is reduced by approximately 36 %.
Treatment delivery
The mean (95 % CI) of the doses measured for DL and PA
treatment deliveries, averaged over the duration of treat-
ment, are given in Table 2. For a total prescription of
20.0 Gy to the PA region, the mean measured dose to the
contralateral testis was 0.30 ± 0.08 and 0.31 ± 0.04 Gy
with and without lead shielding, respectively. For the PA
region, including the pelvic and ipsilateral common iliac
lymph nodes, and with a prescribed dose of 30.0 Gy, the
mean testicular dose was 0.61 ± 0.11 and 0.68 ± 0.39 Gy
with and without shielding, respectively. In general, less
dose was recorded for the PA treatment. This was expected
as the DL fields were closer to the measurement points. At
the anterior scrotum, a dose reduction of approximately 1/4
was seen with the gonadal shielding fitted. Contrary to this,
marginal change was recorded at the posterior scrotal
position when the shielding was fitted.
Discussion
The use of clinically available XR-QA2 and EBT2 Gaf-
chromic film was assessed for measuring dose in imaging
fields and the periphery of treatment fields, respectively.
XR-QA2 was found to agree within 5 % for applied doses
greater than 3 cGy. For an applied dose of 1.1 cGy, the
measured dose was overestimated by approximately 25 %.
This dose is approaching the minimal usable range of the
film.
For distances up to 5 cm from the edge of the field,
EBT2 overestimated the peripheral dose by as much as
25 % relative to the ionisation chamber. At a distance of
10 cm, the dose was overestimated by approximately
40 %. This equates to a dose overestimation of 0.69 cGy,
which in absolute terms is relatively small.
There are limitations in the current approach. The ion
chamber produces an over response in signal at the surface
due to the large chamber volume [34] and although the
dose at the surface was determined relative to the signal
response at depth, perturbation errors are introduced by the
placement of the chamber proud of the water surface. On
the other hand, surface dose measurements comparing
EBT2 with an Attix parallel plate chamber [35] and Monte
Carlo simulations [36] are in good agreement. A more
detailed analysis is beyond the scope of the paper but
further work is required to fully understand the use of ion
chambers and EBT2 for out of field surface dose
measurements.
Fig. 5 XR-QA2 Gafchromic film surface dose measurements within
150 and 180 kVp orthovoltage beams. The measured doses were
normalised to the applied doses, which were measured using a
NE2571 graphite cylindrical ionisation chamber
Table 1 Dose measured using XR-QA2 film for a single scan of each
imaging technique
Imaging dose (cGy)
Technique Shielding Regions of interest
Abdomen ANT POST
CBCT Y 3.25 ± 0.03 0.19 ± 0.01 0.02 ± 0.01
N* 3.26 ± 0.02 0.49 ± 0.01 0.46 ± \ 0.01
CT Y 2.63 ± 0.12 1.70 ± 0.04 1.26 ± 0.05
N 2.56 ± 0.18 2.28 ± 0.17 2.35 ± 0.05
Measurements were made with and without gonadal shielding present
* The mean of two measurement sets. The third set was discarded due
to visible anomalies
Table 2 Dose recorded using EBT2 film, with and without lead
shielding fitted, for paraaortic and dogleg treatment techniques
Seminoma treatment dose (Gy)
Technique Shielding Regions of interest
Abdomen ANT POST
Dogleg Y 1.72 ± 0.06 0.63 ± 0.02 0.59 ± 0.10
N 1.77 ± 0.02 0.83 ± 0.17 0.53 ± 0.28
PA Y 0.70 ± 0.07 0.32 ± 0.04 0.27 ± 0.06
N 0.68 ± 0.11 0.43 ± 0.02 0.19 ± 0.02
Australas Phys Eng Sci Med
123

Overall, Gafchromic film was found to be suitable for
measuring imaging dose and dose in the periphery of
treatment fields, but is subject to the above findings.
For a total prescription of 20.0 Gy to the PA region, the
mean measured dose to the contralateral testis was
0.30 ± 0.08 and 0.31 ± 0.04 Gy with and without lead
shielding, respectively. The DL field treatment, with a
prescribed dose of 30.0 Gy, resulted in a mean testicular
dose of 0.61 ± 0.11 and 0.68 ± 0.39 Gy with and without
shielding, respectively. For the Seminoma treatment, dose
reductions up to 10 % were observed with shielding fitted.
This increased to approximately 25 % when considering
the anterior scrotal dose alone.
The testicular doses measured were approximately two
times the doses previously reported. Bieri et al. [5] mea-
sured mean doses, using TLDs, of 0.09 Gy (±0.05 SD) and
0.26 Gy (±0.12 SD) with and without gonadal shielding,
respectively, for a prescribed dose of 25.2 Gy to the PA
region. For the same dose prescribed, only with DL treat-
ment fields, mean doses of 0.55 Gy (±0.20 SD) and
0.21 Gy (±0.07 SD) were measured, without and with
shielding, respectively. Similarly, Jacobsen et al. [37]
reported a mean dose of 0.32 Gy (±0.08 SD) to the
shielded testis for a delivered dose of 30.0 Gy with DL
fields. The contralateral testicle was shielded using a 5 mm
lead belt and a 5 cm thick lead block. The disparity
between the doses in this work and those reported may be
due to differences in shielding techniques used and varia-
tions in the type and placement of dosimeters.
Kinsella et al. [38] reported a temporary reduction in
sperm count for testicular doses of 0.2–0.7 Gy, returning to
normal within 12–24 months, while Centola et al. [39]
reported doses above 1.2 Gy indicate permanent testicular
damage. Following this, the doses recorded in this work are
within a range in which no permanent testicular damage
should occur.
A mean testicular dose of 2.32 cGy was measured per
CT scan without the use of gonadal shielding. This was
0.48 cGy per CBCT image. Dose reductions to the
remaining testis of up to 36 and 78 % were recorded with
gonadal shielding fitted at CT and CBCT acquisition,
respectively.
The reported role of diagnostic imaging in cancer
induction is conflicted in the literature. A population-based
study observed the incidence of second malignancies in
2,569 men who were either monitored via active surveil-
lance or treated with chemotherapy for testicular cancer
and received 10 CT scans in 5 years after diagnosis. With a
median follow-up was 11.2 years, Van Walraven et al. [16]
concluded that the excess risk of second cancers among
testicular cancer survivors is not associated with diagnostic
imaging. In contrast, a model based study report a lifetime
cancer risk ranging from 1 in 39 to 1 in 85 for a similar
surveillance protocol [40]. Nevertheless, the majority of
diagnostic imaging in this work was CBCT imaging, which
based on this work delivered doses approximately 1/5 of
those reported at CT acquisition.
In summary, the concomitant dose to the remaining
testis while undergoing radiotherapy for seminoma cancer
is small. Still, gonadal shielding should be fitted to ensure
the dose to the testis is as low as reasonably achievable
(ALARA) [41] regardless of the treatment fields.
Conclusions
Mean testicular doses of 0.30 ± 0.08 and 0.31 ± 0.04 Gy
with and without lead shielding, respectively, were mea-
sured with film for a prescription of 20 Gy to the PA
region. Seminoma radiotherapy via DL fields resulted in
respective mean doses of 0.61 ± 0.11 and 0.68 ± 0.39 Gy,
with and without shielding. Additional doses of up to
0.49 ± 0.01 and 2.35 ± 0.05 cGy were measured per
CBCT and CT image, respectively. The dose to the
remaining testis was reduced when shielding was employed
at treatment (10 %), planning CT imaging (36 %) and pre-
treatment CBCT imaging (78 %).
The dose to the testis should be limited to minimise the
risk of radiation related side effects. This can be achieved
by using appropriate gonadal shielding, irrespective of the
treatment fields employed.
References
1. Ferlay J, Shin HR, Bray F, Forman D, et al (2010) GLOBOCAN
2008 v 1.2, cancer incidence and mortality worldwide: IARC
CancerBase No.10
2. Livsey JE, Taylor B, Mobarek N, Cooper RA et al (2001) Pat-
terns of relapse following radiotherapy for stage I seminoma of
the testis: implications for follow-up. Clin Oncol 13(4):296–300
3. Warde P, Gospodarowicz MK, Panzarella T, Catton CN et al
(1995) Stage I testicular seminoma: results of adjuvant irradiation
and surveillance. J Clin Oncol 13(9):2255–2262
4. Boujelbene N, Cosinschi A, Boujelbene N, Khanfir K et al (2011)
Pure seminoma: a review and update. Radiat Oncol 6(1):90
5. Bieri S, Rouzaud M, Miralbell R (1999) Seminoma of the testis:
is scrotal shielding necessary when radiotherapy is limited to the
para-aortic nodes? Radiother Oncol 50(3):349–353
6. Serge M, Costa A, Lagrange JL (1995) Protection of testes during
radiation treatment by irregular and focused fields of 25 MV
X-rays: in vivo evaluation of the absorbed dose. Med Dosim
20(4):269–273
7. Travis LB, Fossa SD, Schonfeld SJ et al (2005) Second cancers
among 40576 testicular cancer patients. Focus on long-term
survivors. J Natl Cancer Inst 97(18):1354–1365
8. Robinson D, Møller H, Horwich A (2007) Mortality and inci-
dence of second cancers following treatment for testicular cancer.
Br J Cancer 96:529–533
9. Huyghe E, Matsuda T, Daudin M, Chevreau C et al (2004) Fertility
after testicular cancer treatments. Cancer 100(4):732–737
Australas Phys Eng Sci Med
123

10. Ruther U, Dieckmann KP, Bussar-Maatz R, Eisenberger F (2000)
Second malignancies following pure seminoma. Oncology 58(1):
75–82
11. Hellbardt A, Mirimanoff RO, Obradovic M, Mermillod B, Pau-
nier JP (1990) The risk of second cancer (SC) in patients treated
for testicular seminoma. Int J Radiat Oncol Biol Phys 18(6):
1327–1331
12. Mayo JR, Aldrich J, Muller NL (2003) Radiation exposure at chest
CT: a statement of the Fleischner Society. Radiology 228(1):15–21
13. Prabhakar R, Haresh K, Julka P, Ganesh T et al (2007) A study on
contralateral breast surface dose for various tangential field
techniques and the impact of set-up error on this dose. Australas
Phys Eng Sci Med 30:42–45
14. Brenner DJ, Hall EJ (2007) Computed tomography: an increasing
source of radiation exposure. N Engl J Med 357(22):2277–2284
15. Berrington de Gonzalez A, Mahesh M, Kim K, Bhargavan M et al
(2007) Projected cancer risks from computed tomographic scans per-
formed in the United States in. Arch Intern Med 169(22):2071–2077
16. van Walraven C, Fergusson D, Earle C, Baxter N et al (2011)
Association of diagnostic radiation exposure and second
abdominal-pelvic malignancies after testicular cancer. J Clin
Oncol 29(21):2883–2888
17. Deng J, Chen Z, Yu JB, Roberts KB et al (2012) Testicular doses
in image-guided radiotherapy of prostate cancer. Int J Radiat
Oncol Biol Phys 82(1):e39–e47
18. Deng J, Chen Z, Roberts KB, Nath R (2012) Kilovoltage imaging
doses in the radiotherapy of pediatric cancer patients. Int J Radiat
Oncol Biol Phys 82(5):1680–1688
19. Tomic N, Devic S, DeBlois F, Seuntjens J (2010) Reference
radiochromic film dosimetry in kilovoltage photon beams during
CBCT image acquisition. Med Phys 37(3):1083–1092
20. Boivin J, Tomic N, Fadlallah B, DeBlois F, Devic S (2011)
Reference dosimetry during diagnostic CT examination using
XR-QA radiochromic film model. Med Phys 38(9):5119–5129
21. Rampado O, Garelli E, Ropolo R (2010) Computed tomography
dose measurements with radiochromic films and a flatbed scan-
ner. Med Phys 37(1):189–196
22. Kairn T, Hardcastle N, Kenny J, Meldrum R et al (2011) EBT2
radiochromic film for quality assurance of complex IMRT
treatments of the prostate: micro-collimated IMRT, RapidArc,
and TomoTherapy. Australas Phys Eng Sci Med 34:333–343
23. He C, Geso M, Ackerly T, Wong C (2008) Stereotactic dose
perturbation from an aneurysm clip measured by Gafchromic�
EBT film. Australas Phys Eng Sci Med 31:18–23
24. Gotanda R, Katsuda T, Gotanda T, Tabuchi A, Yatake H, Takeda
Y (2008) Dose distribution in pediatric CT head examination
using a new phantom with radiochromic film. Australas Phys Eng
Sci Med 31:339–344
25. Devic S, Seuntjens J, Sham E, Podgorsak EB et al (2005) Precise
radiochromic film dosimetry using a flat-bed document scanner.
Med Phys 32(7):2245–2253
26. Paelinck L, De Neve W, De Wagter C (2007) Precautions and
strategies in using a commercial flatbed scanner for radiochromic
film dosimetry. Phys Med Biol 52(1):231–242
27. International Specialty Products (ISP) (2009) Correction protocol
for Gafchromic EBT2 dosimetry film
28. Chofor N, Harder D, Willborn KC, Poppe B (2012) Internal
scatter, the unavoidable major component of the peripheral dose
in photon-beam radiotherapy. Phys Med Biol 57(6):1733
29. Taylor ML, Kron T, Franich RD (2011) Assessment of out-of-
field doses in radiotherapy of brain lesions in children. Int J
Radiat Oncol Biol Phys 79(3):927–933
30. Taylor M, Kron T (2011) Consideration of the radiation dose
delivered away from the treatment field to patients in radiother-
apy. J Med Phys 6(2):59–71
31. Kry S, Salehpour M, Followill DS, Stovall M et al (2005) Out-of-
field photon and neutron dose equivalents from step-and-shoot
intensity-modulated radiation therapy. Int J Radiat Oncol Biol
Phys 62(4):1204–1216
32. IBA Dosimetry GmbH (2008) CC13 User’s guide. IBA Dosim-
etry GmbH, Schwarzenbruck
33. Arjomandy B, Tailor R, Anand A, Sahoo N et al (2010) Energy
dependence and dose response of Gafchromic EBT2 film over a
wide range of photon, electron, and proton beam energies. Med
Phys 37(5):1942–1947
34. Apipunyasopon L, Srisatit S, Phaisangittisakul N (2013) An
investigation of the depth dose in the build-up region, and surface
dose for a 6-MV therapeutic photon beam: Monte Carlo simu-
lation and measurements. J Radiat Res 54(2):374–382
35. Nakano M, Hill R, Whitaker M, Kim J, Kuncic Z (2012) A study
of surface dosimetry for breast cancer radiotherapy treatments
using Gafchromic EBT2 film. J Appl Med Phys 13(3):83–97
36. Kim J, Hill R, Kuncic Z (2012) Practical considerations for
reporting surface dose in external beam radiotherapy: a 6 MV
X-ray beam study. Australas Phys Eng Sci Med 35(3):271–282
37. Jacobsen KD, Olsen DR, Fossa K, Fossa SD (1997) External
beam abdominal radiotherapy in patients with seminoma stage I:
field type, testicular dose, and spermatogenesis. Int J Radiat
Oncol Biol Phys 38(1):95–102
38. Kinsella TJ, Trivette G, Rowland J, Sorace R et al (1989) Long-
term follow-up of testicular function following radiation therapy
for early-stage Hodgkin’s Disease. J Clin Oncol 7(6):718–724
39. Centola GM, Keller JW, Henzler M, Rubin P (1994) Effect of
low-dose testicular irradiation on sperm count and fertility in
patients with testicular seminoma. J Androl 15(6):608–613
40. Tarin TV, Sonn G, Shinghal R (2009) Estimating the risk of
cancer associated with imaging related radiation during surveil-
lance for stage I testicular cancer using computerized tomogra-
phy. J Urol 181(2):627–633
41. ICRP (2007) The 2007 recommendations of the International
Commission on Radiological Protection. ICRP Publication 103,
Ann. ICRP 37(2–4)
Australas Phys Eng Sci Med
123

![Perinatal Testicular · PDF filePerinatal Testicular TorsionTorsion Audrey C. Durrant, ... departments with acute scrotum. ... Neonatal Testicular Torsion.ppt [Compatibility Mode]](https://img.pdfslide.us/doc/110x75/5a9f7f227f8b9a62178cccbd/perinatal-testicular-testicular-torsiontorsion-audrey-c-durrant-departments.jpg)

![CONCOMITANT SYMPTOMS & REMEDIEShomoeopathybooks.com/Repertory of Concomitant Symptoms-1/Repe… · CONCOMITANT SYMPTOMS & REMEDIES :- GRAPH., KALI FACE :[ABDOMEN] : ... aconite if](https://img.pdfslide.us/doc/110x75/5aac6f627f8b9a8f498d0756/concomitant-symptoms-reme-of-concomitant-symptoms-1repeconcomitant-symptoms.jpg)
![Principal Component Analysis of EBT2 Radiochromic Film for ... · A radiochromic film that incorporates a yellow dye in its sensitive layer [Gafchromic EBT2, Ashland, Inc.] is commercially](https://img.pdfslide.us/doc/110x75/5fd0e39e66d6d301e55dcd76/principal-component-analysis-of-ebt2-radiochromic-film-for-a-radiochromic-film.jpg)

![Isolated Testicular Tuberculosis Mimicking Testicular ... involvement, but testicular involvement is an unusual clinical condition [3]. In this report, a case with isolated testicular](https://img.pdfslide.us/doc/110x75/5f3d57bf74280d66ef795ba2/isolated-testicular-tuberculosis-mimicking-testicular-involvement-but-testicular.jpg)