Embed Size (px)
Citation preview

Articles
Moderate Lead Poisoning: Trends in Blood Lead Levels in UnchelatedChildrenMorri E. Markowitz,1 Polly E. Bijur,1 Holly A. Ruff,1 Kenneth Balbi,2 and John F. Rosen11Department of Pediatrics, Albert Einstein College of Medicine, Bronx, NY 10467 USA; 2Montefiore Medical Center, Bronx, NY 10467 USA
The p clinical manage t of childre who,ae moderately wi lead (Pb) isunder actv investigation. To drne the ttern of cha in blood Pb (BPb) levds in theabsence ofelaton theray, w-folowed mode Plbpoison . ( u blood Pblevel 21266oiUl or-22-6
*~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.... ...:.".... . ."t~ 545 gll fr6mnhth repeaed BP leve eauemnstests tndscatis*g lmited response to t e ch n aet ci(CaNaEDTA. Eligiblechildreitid the foid inte n otiat of tie heathdepartento remediate leadh efforts about die tohucity sourcesand ntrnno£ Pb duing 10 ic ad 3 h i and iron therp oir children with fer-ritin leviIs less t i 16 WgL Tpo'qT atify he lead inth Ws,i h wcombine: a
te lea omi*oth panb 'Te su "& s th hmeniromna scoE'FS . Ddtiii "wiuild froi 79eild* BPb l F 27% on
average, over 6 mnts. HES w iorlated with BPb t _ t e inital norlater HSEmesreet pedictd BlPb at othertm points. The HES wshighest at enroli-ment and declined by 50% and75% a the eon.d .nd hi ..h.omerepei.. y Hoeer,only a minority of the children (20%) achieved an HES of 0~ imlic.tliig no lead paint h..a..s t .
home. Despte some ongoing Pb pose, a parallelM~fin Wib BeUre `s o hvin sgru
s etat id:nt account for thean n BPb lelh data tat our mnsure, theIs.r quantifbly rateso BPb level inldr; that his o tis sinitnonly prior so intreton; ad ha BPb level deln incilde hr moderatel poisonedwh PSb e t a ilena thive it , in ttheasenc
chelatio ther&a by,and ind:7%ttheseaesefonging ledpin rouseman PedelcenmK,, ;t'3. -: 1n *~~~~ ~ ~ ~ ~ ~~~~~~~~~~~~.'...........
werde chkin, children, enirnment, eroue Irn led ffnir ,:lt Pespc104:968-972 (1996) lt XX . . . . . . ............
The appropriate clinical management ofmoderately Pb-poisoned children (BPb level1.21-2.66 iimol/l or 25-55 pg/dl) is underactive investigation. Several types of interven-tions have been correlated with at least tran-sient declines in BPb. These include reduc-tion of environmental Pb availability andchelation therapy. Several other aspects oftreatment have theoretical advantages.Decreasing Pb ingestion through an alter-ation of behavior of both the child and theparents is a possibility that has been suggestedbut not formally tested. In addition, nutri-tional counseling to ensure dietary iron andcalcium sufficiency should reduce theenhanced Pb absorption and retention associ-ated with deficiency states in these minerals.
However, the relative weights of thesefactors in reducing BPb levels have not beendefined. Even the efficacy of environmentaland drug interventions in such children isnot established. For example, 6 weeks after acourse of chelation therapy was administeredto moderately Pb-poisoned children, thedecline in BPb levels was statistically indis-tinguishable from a nonchelated group withcomparable initial BPb levels (1). Even stud-ies correlating a fall in BPb levels to reduced
environmental Pb exposure have not quan-titated other possible explanations for theobservation, e.g., changed behavior orimproved metabolism (X4.
In this report, we have focused on twofactors that could explain change in BPbover time: exposure to leaded paint and Festatus. We selected and followed moderate-ly Pb-poisoned children (initial blood Pblevel 1.21-2.66 iimol/l or 25-55 .ig/dl) for6 months with repeated BPb level measure-ments. All the children underwent the leadmobilization test on at least one occasion;the results were negative, indicating limitedresponse to the chelating agent,CaNa2EDTA. Thus, none of these childrenqualified for or received chelation therapy.
We addressed the following questions:What is the magnitude of the correlationbetween home leaded paint exposure andBPb levels at the time moderately Pb-poi-soned children are initially identified andarrive for medical management? In theabsence of chelation therapy, is the subse-quent trend in BPb levels predicted byongoing exposure at home to leaded paint?Does Fe status or treatment of Fe deficien-cy affect the rate of BPb change?
MethodsChildren referred to the Montefiore MedicalCenter Lead Clinic during the years1986-1992 were potentially eligible for thisstudy. The main aim of this research was todetermine treatment outcomes in moderate-ly Pb-poisoned children, defined at the timeas those with blood lead (BPb) of 1.21-2.66pmol/l (25-55 pg/dl) and an erthrocyte pro-toporphyrin (EP) .0.66 iimol/l (35 pg/dl).The main outcome measure was globalintelligence, and those results have beenreported elsewhere (3). Exclusion criteriaincluded previous treatment and neurologi-cal or behavioral disorders from other caus-es. Informed consent was obtained from theparent or legal guardian.
All children received an 8-hour leadmobilization test (Pb-MT) at enrollmentafter undergoing a battery of tests thatincluded psychometric assessment and elec-trophysiological measurements. The Pb-MT protocol has been reported elsewhere(4). Briefly, the Pb-MT consists of theadministration of a single dose of calciumdisodium edetate, 500 mg/m2 given intra-muscularly followed by an 8-hr urine col-lection for lead determination. All the chil-dren in this report excreted less than 200pg/8 hr of Pb and had a ratio of urine Pb todrug dose less than 0.6, i.e., administrationof the drug did not induce a lead diuresis.
The dinical program consisted of inten-sive medical and environmental follow-up.A total of 10 visits over 6 months wasplanned for each child. Initially, visits to theclinic were more frequent and occurred atenrollment and at 1 week, 4 weeks, 6weeks, and 7 weeks later. Thereafter, visitfrequency was reduced to every 4 weeks-at12, 16, 20, and 24 weeks after enrollment.A final visit was scheduled for 25 weeks.The patient was seen at each visit by thepediatric nurse practitioners devoted to theproject and by a housing specialist.Potential sources of lead were discussedwith the parent as were routes of exposure,and information about nutrition and
Address correspondence to M. E. Markowitz,Department of Pediatrics, Montefiore MedicalCenter, 1 1 E. 2 1Oth Street, Bronx, New York10467.This work was completed at the affiliates of theAlbert Einstein College of Medicine and supportedby NIEHS grant ES04039 and W.T. GrantFoundation award 86109286.Received 30 October 1995; accepted 8 May 1996.
Volume 104, Number 9, September 1996 * Environmental Health Perspectives968

Articles - Trends in blood lead levels in unchelated children
hygiene was stressed. Blood was obtainedfor Pb determinations at each visit; ferritinwas measured on blood samples fromweeks 1, 7, and 24.
Three home visits were carried out by anX-ray fluorescence (XRF) specialist and anurse practitioner: at enrollment, at 6 weeks,and at 24-25 weeks. At the home visit, eachpainted surface was assessed visually for itscondition and scored on a 0-3 scale. A scoreof 0 was given to an intact surface; a score of3 was given to a peeling surface. If the sur-face had bubbling or cracks, then a score of1 or 2 was given, respectively. The lead con-tent of the surface was measured in triplicateby XRF using an XK-3 instrument(Princeton Gamma Tech). Each surface ofeach room was tested at one location persurface; three replicate measurements weremade at each site. No substrate correctionwas made since that was the standard at thetime the study was initiated. Surfaces testedincluded all walls, windows, doors, andbaseboards. Calibration procedures followedthe manufacturer's recommendations andwere performed hourly in triplicate usingthe standard block materials supplied by themanufacturer. The instrument was resetafter each reading. Readings with this instru-ment are reported on a scale of 0-10mg/cm2. The mean of the three XK-3 read-ings for each surface was then multiplied bythe visual rating. For example, an intact wallwith an XK-3 reading of 10 had a score of 0(10 x 0 = 0). At the other extreme, a peelingsurface with an XK-3 reading of 10 scored30 (10 x 3 = 30). The sum of all the prod-ucts for an individual home was termed thehome environmental score (HES). Thenumber of surfaces assessed varied betweenhomes. Because we did not quantify theamount of time a child spent in a particularroom, the ratings were not weighted for achild's potential access to any surface, e.g.,the child's bedroom did not have greatervalue than the living room.
After the homes were inspected, the fol-lowing intervention was performed for allthe subjects. The local Board of Health'sLead Bureau was notified. The LeadBureau is responsible for the initiation andfollow-up of the legal process needed tobring the home into compliance with exist-ing health and housing codes. No specificabatement protocol was enforced.Educational efforts aimed at the parent orguardian about the sources of lead, its toxi-city, and methods to reduce exposure werebegun at the first clinic visit. In particular,efforts were made to remove the child fromthe lead source either by placement inalternative lead-free housing such as a rela-tive's home, or by abatement of the prima-ry residence. Nutritional counseling
stressed the need for adequate calcium andFe intake as well. Parents or guardians ofchildren with ferritin levels <16 pg/l atenrollment were given sufficient Fe (Fer-in-sol) to provide the child with 5-6 mg/kg ofelemental Fe daily for 3 months. No for-mal behavior modification program wasused, and no quantitative assessment of anychanges in parental or child behavior overthe course of follow-up was made.
BPb was measured by graphite furnaceatomic absorption spectrometry using aVarian Techtron atomic absorption spec-trophotometer (4). The error of themethod is ± 0.05 pmol/l (1 pg/dl); (95%confidence limits) for the blood range ofthese patients. Ferritin was measured byradioimmunoassay in sera obtained at 1, 7,and 24 weeks (5).
Data analyses included calculation ofthe means and standard deviations for themeasures at each time point and determi-nation of the differences across time. Logtransformations of the HES scores wereperformed since the raw data were positive-ly skewed. The transformed data were usedfor regression analyses.
ResultsThere were 206 children originallyenrolled. Of these, 93 received at least onecourse of chelation. Of the remaining 1 13children, 79 children, 1-7 years of age withinitial BPb levels of 1.21-2.66 pmol/l(25-55 pg/dl) and negative Pb-MTs, com-pleted the study. None had received chela-tion treatment prior to or during the study.The mean age at enrollment was 31.5months. Approximately two-thirds of thechildren were of Hispanic origin and one-third were African American. They lived
mainly in pre-1960 housing.The HES scores are given in Table 1.
The median score at the time of enroll-ment, 37, was used as a reference point tocategorize the population into high- andlow-level lead exposure. By the secondhome visit at 6-7 weeks, the mean andmedian scores had declined appreciably.There were no differences between the twogroups on season of enrollment, age, or sex.Ten percent of the homes had an HES of 0at enrollment, 25% at 6 weeks, and 20% at6 months.
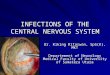
The mean BPb level was greater in thechildren with high HES scores at enroll-ment as compared to children with lowHES scores (Fig. 1). BPb declined overtime in a parallel manner in the two groupsas reflected by a correlation between meanBPb levels over time of 0.98. When plottedas percent dedine over time, the two curveswere superimposed. In these children, therate of decline was thus independent of ini-tial HES levels.
A significant association between BPband HES was noted at enrollment only(Table 2). Initial HES was not a predictorof BPb at 6 or 24 weeks or was HES relat-ed concurrently to BPb at the other twotime points.
To assess whether age or initial ferritinexplained the decline in BPb, multipleregression models were tested with age andferritin as explanatory variables. Neither
Table 1. Home environmental scores (HES)
HES Week 0 Week 6 Week 24
Minimum 0 0 0Maximum 830 766 294Mean±SE 88±16 44±11 27±5Median 37 14 17
35
30
X 25m=LU0SL 2
20
15 0 2 4 6 8 10 12 14 16 18 20 22 24
Time (weeks)
Figure 1. Average blood lead (BPb) levels over 6 months in children grouped above and below the initialmedian home environmental score (HES) of 37. r= 0.98.
Environmental Health Perspectives * Volume 104, Number 9, September 1996 969

Articles - Markowitz et al.
age nor initial ferritin levels contributedsignificantly to the regression models. Inaddition, change in BPb from enrollmentto completion at week 25 was unrelated tochange in HES over the same time interval.
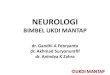
We further selected two subgroups ofchildren who remained either persistentlyabove or below the initial median HES of37 throughout the study (12.5% of theentire sample in each group). As before, thechildren with high HES scores had higherinitial BPb levels that declined over the sixmonths, despite ongoing exposure, at a ratecomparable to the low HES group (Fig. 2).
To test the hypothesis that change in Festatus as measured by ferritin levels couldaffect the rate of decline in BPb, we com-pared three subgroups: children who wereFe deficient throughout the 6 months, chil-dren with sufficient Fe throughout the 6months, and children who were initially Fedeficient but were Fe sufficient by the endof the 6 months. BPb levels appeared todecline in parallel in the three groups (Fig.3) with correlations of >0.9 between themean BPb levels over time.
The frequency distribution for the twoHES groups by BPb at the initial and finaltime points is given in Table 3. By 6months, the BPb levels had declined to lessthan 1.21 flmol/l (25 jig/dl) in two-thirds ofthe children, regardless of HES group. Thisis the BPb cutoff for Pb-MT eligibility.Only 7% reached a BPb level less than 0.72pmol/l (15 pg/dl); the lowest BPb achievedwas 0.43 limol/l (9 pg/dl) in one child.DiscussionThis study describes the trend in BPb levelsin moderately Pb-poisoned children whowere enrolled in a comprehensive Pb treat-ment program but were not eligible forchelation therapy. Our sample was drawnfrom a population at high risk for Pb poi-soning-poor, urban, minority children(6). In the absence of chelation but in thecontext of an intervention focused onsource abatement, education, nutritionalcounseling, remediation of Fe deficiency,and very close follow-up, average BPb lev-els declined over 6 months.
Conceptually, treatment of lead poison-ing can be divided into four areas of activeintervention: source abatement, behavior
Table 2. Correlation matrix between home envi-ronmental scores (HES) and blood lead (BPb)
R(N)BPb HES week 0 HES week 6 HES week 24
Week 0 0.243 (77)*Week 6 0.175 (78) 0.049 (75)Week 24 0.111(75) 0.048 (72) 0.136 (65)*P<0.05.
modification programs, metabolic manipu-lation by diet, and chelation. Of these,chelation and behavior modification werenot offered to these children. In theabsence of active interventions such aschelation or behavior modification therapy,others have reported that BPb levels mayfall over time in moderately Pb-poisonedchildren. Over 6 months of observation,the reported decline has ranged from 7%to 18% (7,8). The decrease in BPb level inour group of 79 children in which therewas intervention was somewhat larger at27%. Initially BPb levels in this group wererelated to HES. In an extensive investiga-tion of environmental Pb exposure in andaround the homes of Cincinnati children,Clark et al. (9l) found that an assessment ofleaded paint hazards in the home correlatedsignificantly with Pb washed from the chil-dren's hands and with children's BPb lev-
40
=L
25
20
150 2 4 6 8 10
els. The lead paint hazard was a measurethat combined XRF wall measurementswith an evaluation of the status of the sur-face. This measure appears comparablequalitatively to our HES. Similarly, wefound a significant correlation of compara-ble magnitude between HES and BPb atthe time of enrollment.
In our study, change in our environ-mental exposure measure, the HES, wasnot correlated to the change in BPb levels.In general, both BPb and HES declinedover the 6 months. However, once childrenwere enrolled in the study, average BPblevels declined even in the children withcontinuing, though decreased, lead expo-sure. At the extreme, the rate of fall in BPblevels of the subgroup of children withHES persistently greater than the initialmedian of 37 was the same as that of thechildren with minimal exposure through-
12 14 16 18 20 22 24
Time (weeks)
Figure 2. Average blood lead (BPb) levels over 6 months in two groups of children: those whose homeenvironmental score (HES) was either persistently above or below the initial median value of 37 at allthree home assessments. R between group at all time points = 0.89.
35
30-6cm
a-mX 25a0
20
1516 20 24
Time (weeks)
Figure 3. Average blood lead (BPb) levels over 6 months in children grouped by iron (ferritin) status aseither iron deficient throughout the study period, iron sufficient throughout the study period, or initiallyiron deficient but iron sufficient by the end of the study period.
Volume 104, Number 9, September 1996 * Environmental Health Perspectives970

Articles - Trends in blood lead levels in unchelated children
out the study period. Few of the homes ofour children reached an HES of 0.Nevertheless, the continuing presence ofsome lead paint exposure in the children'shomes did not preclude a decline in theirBPb levels.
Other studies have examined the rela-tionship between abatement and change inBPb levels but have not reported quantifiedmeasures of ongoing lead paint hazards(2,10,11). In these studies, abatement pro-cedures differed and BPb levels either fell,remained the same, or transiently increasedbefore falling (2,10,11). A more proximatemeasure of lead exposure, dust lead content,has been evaluated as a predictor of lead inblood and teeth (2,12,13). Testing differentabatement protocols, Farfel and Chisolm(12) found little difference in dust Pb orBPb improvement over 6 months. Othershave also failed to document a linear corre-lation between changes in leaded dust in thehome environment and changes in BPb,although both declined over time (2). Wedid not measure the Pb content of the dustin the homes of our subjects; however,given the ongoing presence of lead painthazards in the majority of homes even after6 months, it is reasonable to postulate thatPb-contaminated dust remained in thehome. Despite this likelihood, BPb levelsdeclined. The implication of our observa-tion is not that abatement procedures areunimportant, rather, that the presence ofsome environmental Pb does not precludeBPb concentration reductions. Arguably,our data support the notion that evenincomplete remediation of lead hazards maybenefit lead poisoned children.
Fe status did not account for theobserved decline in BPb. The rate ofchange in BPb appeared comparable in thesubgroups of Fe-deficient and -sufficientchildren and was not accelerated by correc-tion of Fe deficiency. This is somewhatsurprising because previous research hasshown increased Pb absorption, retention,and toxicity in the presence of Fe deficien-cy (5,14,15). The effect of Fe status onBPb is relatively small and may beobscured by the magnitude of the lead bur-den, particularly in bone. Perhaps Fe status
Table 3. Frequency distribution (%) of home envi-ronmental scores (HES) and blood lead (BPb)
HES <37 HES >37
BPb (pg/dl) Week 0 Week 25 Week 0 Week 25
<15 0 14 0 015-24 5 53 0 6725-34 90 31 80 3035-44 5 0 15 3>44 0 3 5 0
To convert pg/dl to pmol/l, divide by 20.7.
would show a greater effect in a less Pb-poisoned population.
Several other factors need to be consid-ered. There is the seasonal variation in BPblevels reported by some (2,7,8,16) but notby others (17). In general, BPb levels arehigher in the late summer and fall (8).Enrollment in our study occurred through-out the year and no effect of season couldbe discerned.
A second factor is age of the children.Pb levels tend to peak around 2 years of age(6,16,18). This age group has a greaterprevalence of Fe deficiency and hand-to-mouth behavior, both predisposing factors,than older children. The average age atenrollment of our population was 31.5months; thus, a decline based on the agingof our group was to be expected. However,the magnitude of the decline between 2and 3 years of age reported in several longi-tudinal studies is considerably less (7%)than in ours (27%) (16,18).
Our study has limitations. No attemptwas made to quantify the amount of timethe child spent in the primary residence,and potential secondary sources of Pbexposure (e.g., at relatives' homes) were notdetermined. We also did not and could notassess the duration of exposure prior toenrollment. Though we documented onemeasure of exposure, the HES, we did notmeasure the Pb content of the dust in therooms or on the hands of the child.
In the absence of chelation and in thepresence of ongoing Pb exposure, averageBPb levels still fell. Other aspects of ourintervention may have contributed to thisevent, such as the educational and nutri-tional information provided at the frequentclinic visits. Each clinic visit includedinformation about the sources and path-ways of lead exposure and accumulation.Perhaps this resulted in improved house-hold cleaning. Alternatively, the informa-tion provided to parents about the inges-tion of leaded dust may have led them towash the children's hands more often or tocurb the children's hand-to-mouth behav-ior. As a speculation, different amounts ofmouthing behavior may account, in part,for the observation that siblings with equalenvironmental lead exposure may have sig-nificantly different lead levels. Thesehypotheses remain to be tested. Staess et al.(11) made an indirect estimate of the effectof factors other than abatement and chela-tion that contribute to a change in BPbconcentrations over 10-14 months. BPblevels declined 12% (35.1-30.9 pg/dl) in agroup of unchelated children whose homeswere not abated (11).
BPb in moderately Pb-poisoned chil-dren reflects the aggregate of environmen-
tal exposure (usually leaded paint or itsdust), child behavior (pica, mouthing oftoys and fingers), absorption (affected byiron and calcium status), distribution toand from other tissues (bone and soft tis-sues), and excretion (mainly in urine). Inthis study we focused on two of these com-ponents, environmental exposure and ironstatus, and found that neither componentfully accounts for the observed decline inBPb levels in our unchelated children. Thespecific aspects of our comprehensive pro-gram that contribute to this decline havenot been identified. What has been identi-fied is a group of moderately Pb-poisonedchildren whose BPb levels decreased, evenin the presence of lead in their homes, Fedeficiency, and no chelation. We suggestthat future studies attempting to define fac-tors most likely to affect BPb levels in chil-dren include 1) more proximal measures ofenvironmental exposure such as hand dustPb; 2) measures of body stores of lead inthe child's skeleton, the major reservoir oflead in humans; and 3) quantitative mea-sures of child behavior (such as hand-to-mouth activity and pica) and parentalbehavior (such as attention to the child'sactivities, diet, environment, and frequencyof hand washing).
REFERENCES
1. Markowitz ME, Bijur PE, Ruff H, Rosen JF.Effects of calcium disodium versenate(CaNa2EDTA) chelation in moderate child-hood lead poisoning. Pediatrics 92:265-271(1993).
2. Charney E, Kessler B, Farfel M, Jackson D.Childhood lead poisoning: a controlled trial ofthe effect of dust-control measures on bloodlead levels. N Engl J Med 309:1089-1093(1983).
3. Ruff HA, Bijur PE, Markowitz ME, Ma YC,Rosen JF. Declining blood lead levels and cog-nitive changes in moderately lead-poisonedchildren. JAMA 269:1641-1646 (1993).
4. Markowitz ME, Rosen JF. Assessment of leadstores in children: validation of an 8-hourCaNa2EDTA provocative test. J Pediatr104:337-341 (1984).
5. Markowitz ME, Rosen JF, Bijur PE. Effects ofiron deficiency on lead excretion in childrenwith moderate lead intoxication. J Pediatr116:360-364 (1990).
6. Mahaffey KR, Annest JL, Roberts J, MurphyRS. National estimates of blood lead levels:United States, 1976-1980. Association withselected demographic and socioeconomic fac-tors. N Engl J Med 307:573-579 (1982).
7. Klein MC, Schlageter M. Non-treatment ofscreened children with intermediate blood leadlevels. Pediatrics 56:298-302 (1975).
8. McCusker J. Longitudinal changes in bloodlead level in children and their relationship toseason, age and exposure to paint or plaster.Am J Public Health 69:348-352 (1979).
9. Clark S, Bornschein R, Succop P, Roda S,Peace B. Urban lead exposures of children in
Environmental Health Perspectives * Volume 104, Number 9, September 1996 971
Articles e Markowitz et al.
Cincinnati, Ohio. Chem Speciation Bio-availability 3(314):163-171 (1991).
10. Amitai Y, Brown MJ, Graef JW, Cosgrove E.Residential deleading: effects on the blood leadlevels of lead-poisoned children. Pediatrics88:893-897 (1991).
11. Staes C, Matte T, Copley CG, Flanders D,Binder S. Retrospective study of the impact oflead based paint hazard remediation on chil-dren's blood lead levels in St. Louis, Missouri.AmJ Epidemiol 139:1016-1026 (1994).
12. Farfel MR, Chisolm JJ Jr. Health and environ-mental outcomes of traditional and modified
practices for abatement of residential lead-basedpaint. Am J Public Health 80:1240-1245(1990).
13. Alexander LM, Heaven A, Delves HT,Moreton J, Trenouth MJ. Relative exposure ofchildren to lead from dust and drinking water.Arch Environ Health 48:392-400 (1993).
14. Watson WS, Hume R, Moore MR. Oralabsorption of lead and iron. Lancet 2:236-237(1980).
15. Barton JC, Conrad MEC, Harrison L. Effectsof iron on the absorption and retention of lead.J Lab Clin Med 92:536-547 (1978).
16. McMichael AJ, Baghurst PA, Robertson EF,Vimpani GV, Wigg NR. The Port Pirie cohortstudy: blood lead concentrations in early child-hood. Med J Aust 143:499-503 (1985).
17. Reigart JR, Whitlock NH. Longitudinal obser-vation of the relationship between free erythro-cyte porphyrins and whole blood lead.Pediatrics 57:54-59 (1976).
18. Dietrich KN, Berger OG, Succop PA. Leadexposure and the motor developmental statusof urban six-year-old children in the Cincinnatiprospective study. Pediatrics 91:301-307(1993).
ENVIRONMENTAL SCIENCES FACULTY POSITION
The University of Texas-HoustonHealth Science CenterSchool of Public Health
t he Environmental Sciences Discipline of The service. The incumbent ideally will have research
University of Texas-Houston School of Public interest pertinent to the particular problems of pub-Health is seeking candidates for a tenure-track lic health in South Texas and the United States-
position at the Assistant or Associate Professor level to Mexico border region. An opportunity to assume adminis-
join the faculty of the Satellite MPH program in San trative responsibilities may be available for a candidate
Antonio. The satellite program, an integral part of the hired at the Associate level.
UT-Houston Health Science Center School of Public
Health, is located on the campus of The University of Greater detail about this position, The University of
Texas Health Science Center at San Antonio. Texas-Houston Health Science Center School of Public
Health, and the University of Texas Health Science
Candidates must have a doctoral degree in the environ- Center at San Antonio may be obtained through the
mental sciences or an M.D., M.P.H. with board certification Internet at the following address:
in preventive medicine; demonstrated competence and http://utsph.sph.uth.tmc.edu/
experience in teaching environmental and occupationalhealth at the graduate level; and evidence of scholarly The University of Texas is an Equal Opportunity
achievement as indicated by research projects and publica- Employer. Minorities and women are particularly encour-
tions. Experience in the development and administration of aged to apply. The start date is flexible; review of applica-environmental health programs at the community or state tions will begin immediately and continue until a suitable
level is preferred. Responsibilities will include teaching, candidate is selected.
research, supervision of graduate students and community
MPH Program at San Antonio
To apply: Send your curriculum vitae to:
George L. Delclos, M.D., M.P.H., Search Committee Chair, School of Public Health,
The University of Texas-Houston, Health Science Center, PO Box 20186, Houston, Texas 77225
972 Volume 104, Number 9, September 1996 * Environmental Health Perspectives


![Suffix Ordering in Bantu: A Morphocentric Approach1 Ordering in Bantu: A Morphocentric Approach1 ... (1993) to the ... V CAUS REC V REC CAUS [ [ [ mang ] its ]](https://img.pdfslide.us/doc/110x75/5b2598277f8b9a221d8b4689/suffix-ordering-in-bantu-a-morphocentric-approach1-ordering-in-bantu-a-morphocentric.jpg)