Embed Size (px)
Citation preview

Arno Zaritsky, M.D. Arno Zaritsky, M.D. University of Florida College of MedicineUniversity of Florida College of MedicineSSome slides from ome slides from www.www.dicsepsisdicsepsis.org.org and and
www.www.coumadincoumadin.com.com
Disseminated Intravascular Coagulation (DIC) and related disorders in critically ill patients

Normal haemostasis is dependent on:
PlateletsPlatelets The coagulation systemThe coagulation system The fibrinolytic systemThe fibrinolytic system Endothelial/subendothelial cellsEndothelial/subendothelial cells Blood viscosityBlood viscosity Blood flowBlood flow
CoagulationInflammation
AnticoagulantsAntiinflammatoryFibrinolysis
Case A 10-year-old 30 kg boy is involved in an ATV A 10-year-old 30 kg boy is involved in an ATV
accident. He is hypotensive with a distended accident. He is hypotensive with a distended abdomen and severe laceration to his thigh.abdomen and severe laceration to his thigh.
Taken to OR and requires 6 units of pRBC, 2 Taken to OR and requires 6 units of pRBC, 2 units of FFP and 7 liters of Ringers lactate to units of FFP and 7 liters of Ringers lactate to manage severe bleeding from a laceration to manage severe bleeding from a laceration to his femoral artery, splintered spleen and his femoral artery, splintered spleen and fractured liver.fractured liver.
Arrives in the PICU with oozing from wound. Arrives in the PICU with oozing from wound. He is hemodynamically stable: HR = 110; BP He is hemodynamically stable: HR = 110; BP 105/70 and breathing spontaneously105/70 and breathing spontaneously

Case
H/H = 9.5/28.5; platelets = 43,000; H/H = 9.5/28.5; platelets = 43,000; PT = 18.6 seconds/ PTT = 48 secs; PT = 18.6 seconds/ PTT = 48 secs; FDP = 1.4; Fibrinogen = 124 mg%FDP = 1.4; Fibrinogen = 124 mg%
Does he have DIC?Does he have DIC? What is DIC?What is DIC? How do you diagnose DIC?How do you diagnose DIC?

Diagnosis of DIC Hemorrhage is often the recognized Hemorrhage is often the recognized
manifestation of DIC,but the manifestation of DIC,but the initialinitial major major problem is thrombosis of the micro-vasculature problem is thrombosis of the micro-vasculature sometimes leading to microembolization of sometimes leading to microembolization of multiple organsmultiple organs
Although DIC is a well recognized clinical Although DIC is a well recognized clinical condition, there is no consensus on its definition condition, there is no consensus on its definition and diagnostic criteria. and diagnostic criteria.
There is also no method to quantify the severity There is also no method to quantify the severity of DIC and to recognize “non-overt” DICof DIC and to recognize “non-overt” DIC
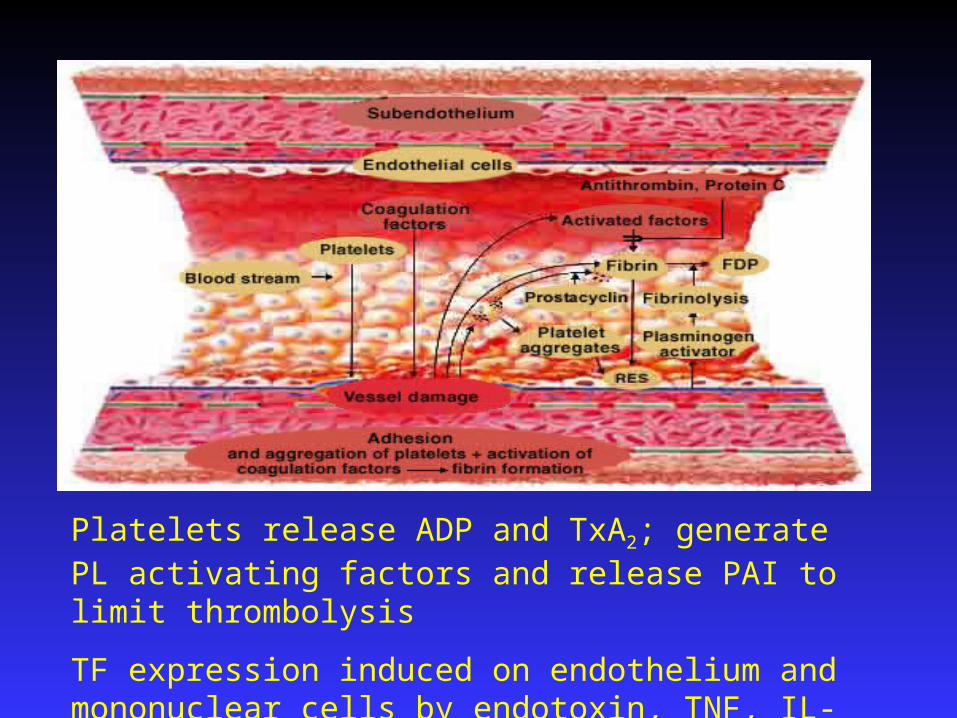
Platelets release ADP and TxA2; generate PL activating factors and release PAI to limit thrombolysis
TF expression induced on endothelium and mononuclear cells by endotoxin, TNF, IL-1

Definition of disseminated intravascular coagulation
““DIC is an acquired syndrome DIC is an acquired syndrome characterized by the intravascular characterized by the intravascular activation of coagulation with loss of activation of coagulation with loss of localization arising from different causes. localization arising from different causes. It can originate from and cause damage It can originate from and cause damage to the microvasculature, which if to the microvasculature, which if sufficiently severe, can produce organ sufficiently severe, can produce organ dysfunction.”dysfunction.”
Scientific Subcommittee on DIC of the International Society on Thrombosis and Haemostasis. July 9, 2001

DIC
An acquired An acquired syndrome syndrome characterized by characterized by systemicsystemic intravascularintravascular coagulationcoagulation
Coagulation is Coagulation is alwaysalways the initial the initial eventevent
SYSTEMIC ACTIVATION OF COAGULATION
Intravascular deposition of
fibrin
Depletion of platelets and coagulation
factors
Thrombosis of small and
midsize vessels Bleeding
Organ failureDEATHDEATH

Disseminated intravascular coagulation Microvasculature is defined as a transport Microvasculature is defined as a transport
organ composed of blood and the vascular organ composed of blood and the vascular structures in contact with the blood, including structures in contact with the blood, including endothelium and mononuclear cells endothelium and mononuclear cells (RES/microvasculature)(RES/microvasculature)
Homeostasis is maintained by a COMPLEX Homeostasis is maintained by a COMPLEX balance between vascular, RES and blood balance between vascular, RES and blood component factorscomponent factors
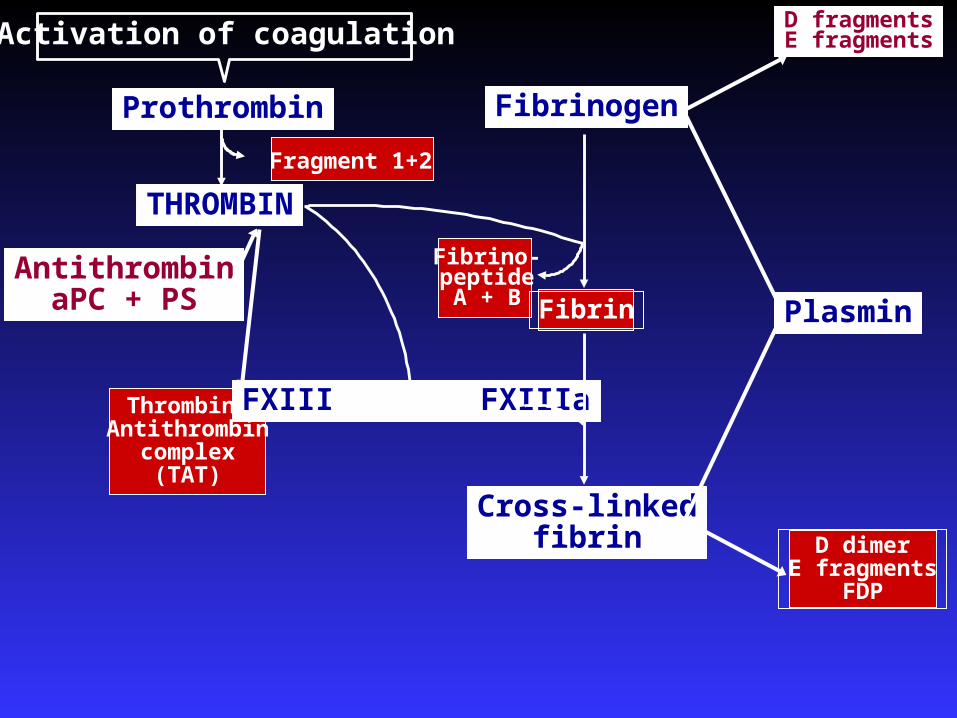
D dimerE fragments
FDP
THROMBIN
AntithrombinaPC + PS
Thrombin-Antithrombin
complex(TAT)
PlasminFibrin
FXIII FXIIIa
Fragment 1+2
Cross-linkedfibrin
Fibrino-peptideA + B
Prothrombin Fibrinogen
D fragmentsE fragmentsActivation of coagulation

Laboratory Studies
D-dimer and FDP: complex products D-dimer and FDP: complex products produced from fibrinolysisproduced from fibrinolysis FDP more sensitive; D-dimer more specificFDP more sensitive; D-dimer more specific
PT: extrinsic (I, PT: extrinsic (I, IIII, , VV, , VIIVII, , XX); international ); international normalization ratio (INR) better expresses valuenormalization ratio (INR) better expresses value
aPTT: intrinsic (aPTT: intrinsic (XIIXII, , XIXI, , XX, , IXIX, , VIIIVIII, , VV, II & I), II & I) TAT: Thrombin-antithrombin; reflects activation of TAT: Thrombin-antithrombin; reflects activation of
thrombin and inhibitory pathwaythrombin and inhibitory pathway Fragment 1+2: prothrombin activationFragment 1+2: prothrombin activation

Symptoms of DIC Dysfunction of multiple organsDysfunction of multiple organs
The pulmonary microembolism syndromeThe pulmonary microembolism syndromeAcute: vascular and bronchAcute: vascular and bronchooconstrictionconstrictionLate: ARDSLate: ARDS
Acute renal failureAcute renal failureOliguria, increasing serum creatinine, Oliguria, increasing serum creatinine,
hematuriahematuria Cerebral dysfunctionCerebral dysfunction
Confusion, blurred consciousness, comaConfusion, blurred consciousness, coma Cutaneous hemorrhagic necrosesCutaneous hemorrhagic necroses Failure of liver, endocrine glands etc.Failure of liver, endocrine glands etc.
Causes of DIC (Clinical conditions, I)
Infections (responInfections (responsible for 50% of cases)sible for 50% of cases) SepticaemiaSepticaemia – – Gram negative (endotoxin)Gram negative (endotoxin)
– – Gram positive (polysaccharides, Gram positive (polysaccharides, peptides)peptides)
ViremiasViremias – – VaricellaVaricella
– – HepatitisHepatitis– – Cytomegalovirus Cytomegalovirus – – HIVHIV
Causes of DIC TraumaTrauma
Crush injuriesCrush injuries Other trauma with tissue necrosisOther trauma with tissue necrosis Severe burnsSevere burns Extensive surgeryExtensive surgery TBI – high concentration of TFTBI – high concentration of TF
Obstetric complicationsObstetric complications Amniotic fluid embolismAmniotic fluid embolism Placental abruption Placental abruption (Pre)eclampsia(Pre)eclampsia Dead fetus syndromeDead fetus syndrome

Causes of DIC
HemolysisHemolysis Hemolytic transfusion reactionsHemolytic transfusion reactions Massive transfusionsMassive transfusions MalariaMalaria Other severe hemolysisOther severe hemolysis
Malignant disordersMalignant disorders Metastatic malignancyMetastatic malignancy Tumors producing cancer Tumors producing cancer
procoagulantprocoagulant Tumor with tissue necrosisTumor with tissue necrosis

Causes of DIC Vascular abnormalitiesVascular abnormalities
Giant hemangiomaGiant hemangioma Heriditary teleangiectasisHeriditary teleangiectasis Prosthetic devicesProsthetic devices
– – Aortic balloon assist devicesAortic balloon assist devices – – Denver shuntsDenver shunts
Other conditionsOther conditions PancreatitisPancreatitis Acute liver necrosisAcute liver necrosis Transplant rejectionTransplant rejection Heat strokeHeat stroke

Criteria for overt DIC Must have a condition associated with DICMust have a condition associated with DIC Platelet count (>100K = 0; <100K = 1; Platelet count (>100K = 0; <100K = 1;
<50K =2)<50K =2) Increased fibrinolysis-related marker (eg. FDP, Increased fibrinolysis-related marker (eg. FDP,
soluble fibrin; no increase = 0; moderate = 2; strong soluble fibrin; no increase = 0; moderate = 2; strong increase = 3)increase = 3)
PT (<3 secs=0; >3 but < 6 sec = 1; >6 sec=2)PT (<3 secs=0; >3 but < 6 sec = 1; >6 sec=2) Fibrinogen (> 100 mg%=0; <100 mg%=1)Fibrinogen (> 100 mg%=0; <100 mg%=1) If score > 5, compatible with overt DIC; repeat If score > 5, compatible with overt DIC; repeat
daily. If <5 suggestive of non-overt DIC. Repeat daily. If <5 suggestive of non-overt DIC. Repeat dailydaily
Criteria for non-overt DIC More complex and less agreementMore complex and less agreement Consider measurement of AT, protein C Consider measurement of AT, protein C
and TAT complexes in addition to and TAT complexes in addition to previous criteria. previous criteria.
Also need to recognize that DIC is Also need to recognize that DIC is different depending on the time course different depending on the time course of the disease processof the disease process

Systemic hyperactive disorders of hemostasis
Hyperfibrinolyticsyndrome
Increased plasmin formation
DIC
Increased fibrin formation
Typical, acute DIC
TTP: Thrombotic Thrombocytopenic PurpuraHELLP: Hemolysis, Elevated Liver enzymes, Low PlateletsHUS: Hemolytic Uremic Syndrome
TTP HELLP HUS
Thrombotic
microangiopathyIncreased platelet aggregation

Course of DIC Accelerating factors Shock Acidosis Hypoxemia Stasis Dehydration
Fever Stress Renal insufficiency Liver disease Malnutrition
Deficient antithrombotic mechanisms:– Deficient antiplatelet mechanisms– Deficient anticoagulant mechanisms– Decreased fibrinolytic activity– Dysfunction of the reticulo-endotelial system
Treatment of DIC
Stop the triggering processStop the triggering process . . The only proven treatment!The only proven treatment!
Supportive therapySupportive therapy No specific treatmentsNo specific treatments
Plasma and platelet substitution therapyPlasma and platelet substitution therapy AnticoagulantsAnticoagulants Physiologic coagulation inhibitorsPhysiologic coagulation inhibitors

Heparin Acts by binding to AT leading to confirmational Acts by binding to AT leading to confirmational
change. change. The AT-heparin complex inhibits IIa most The AT-heparin complex inhibits IIa most
potentlypotently Xa is next most potently inhibited and does Xa is next most potently inhibited and does
not require simultaneous binding by heparinnot require simultaneous binding by heparin Also inhibits IXa, XIa, and XIIa. Also inhibits IXa, XIa, and XIIa.
Binding to AT is through unique penta-Binding to AT is through unique penta-saccharidesaccharide Only one-third of heparin molecules can bind Only one-third of heparin molecules can bind
to AT-IIIto AT-III

Heparin

Heparin Once AT is bound to the serine Once AT is bound to the serine
protease site, it releases heparinprotease site, it releases heparin Released heparin can then bind to Released heparin can then bind to
another ATanother AT The binding of AT to its target is The binding of AT to its target is
covalentcovalent Heparin pharmacokinetics: larger Heparin pharmacokinetics: larger
molecules are cleared more quicklymolecules are cleared more quickly
Treatment of DIC: Heparin Heparin has an immediate antithrombotic effect but Heparin has an immediate antithrombotic effect but
its value in the treatment of DIC is doubtful because:its value in the treatment of DIC is doubtful because: Heparin increases the effect of a number of Heparin increases the effect of a number of
proteases from neutrophil granulocytes and proteases from neutrophil granulocytes and bacteriabacteria
Heparin aggregatHeparin aggregateses activated platelets activated platelets Heparin inhibits antithrombin-induced release of Heparin inhibits antithrombin-induced release of
prostacyclin from endothelial cells by binding to prostacyclin from endothelial cells by binding to glycosaminoglycansglycosaminoglycans
Heparin requires adequate concentrations of AT, Heparin requires adequate concentrations of AT, which is often depeleted in DICwhich is often depeleted in DIC
Antithrombin In Sepsis Multicenter trial to determine if high-dose AT Multicenter trial to determine if high-dose AT
within 6 hours of sepsis onset improved survival within 6 hours of sepsis onset improved survival (KyperSept Trial)(KyperSept Trial)
Double-blind, placebo controlled trialDouble-blind, placebo controlled trial 2314 adult patients randomized to 30,000 units 2314 adult patients randomized to 30,000 units
AT over 4 days or 1% albuminAT over 4 days or 1% albumin Overall 28-day mortality was 38.9% in AT group Overall 28-day mortality was 38.9% in AT group
vs. 38.7% in placebovs. 38.7% in placebo In subgroup who did not receive heparin In subgroup who did not receive heparin
(n=698), AT group (37.8% vs. 43.6% (p=.08)(n=698), AT group (37.8% vs. 43.6% (p=.08) AT+heparin increased serious bleeding (23.8% AT+heparin increased serious bleeding (23.8%
vs. 13.5% placebo)vs. 13.5% placebo)
JAMA 2001; 286:1896-78 (October 17)

Randomised trials on antithrombin in patients with sepsis or evidence of DIC

Determine antithrombin activityDetermine antithrombin activity The antithrombin activity is increased to 100% The antithrombin activity is increased to 100%
by infusion of (100 - AT%) X (kg body weight) by infusion of (100 - AT%) X (kg body weight) IU i.v.IU i.v.
Determine the antithrombin level every 4–6 hrs Determine the antithrombin level every 4–6 hrs
and repeat infusion when necessaryand repeat infusion when necessary If acute determination of antithrombin is not If acute determination of antithrombin is not
available, treatment can be initiated with a available, treatment can be initiated with a dose dose of 50 X (kg body weight) IU i.v.of 50 X (kg body weight) IU i.v.
Simultaneous use of heparin Simultaneous use of heparin increasesincreases the the bleeding tendencybleeding tendency
Treatment of DIC: Antithrombin

Activated protein c
Faust et al. Dysfunction of endothelial protein c activation in severe meningococcal sepsis. NEJM 2001; 345:408
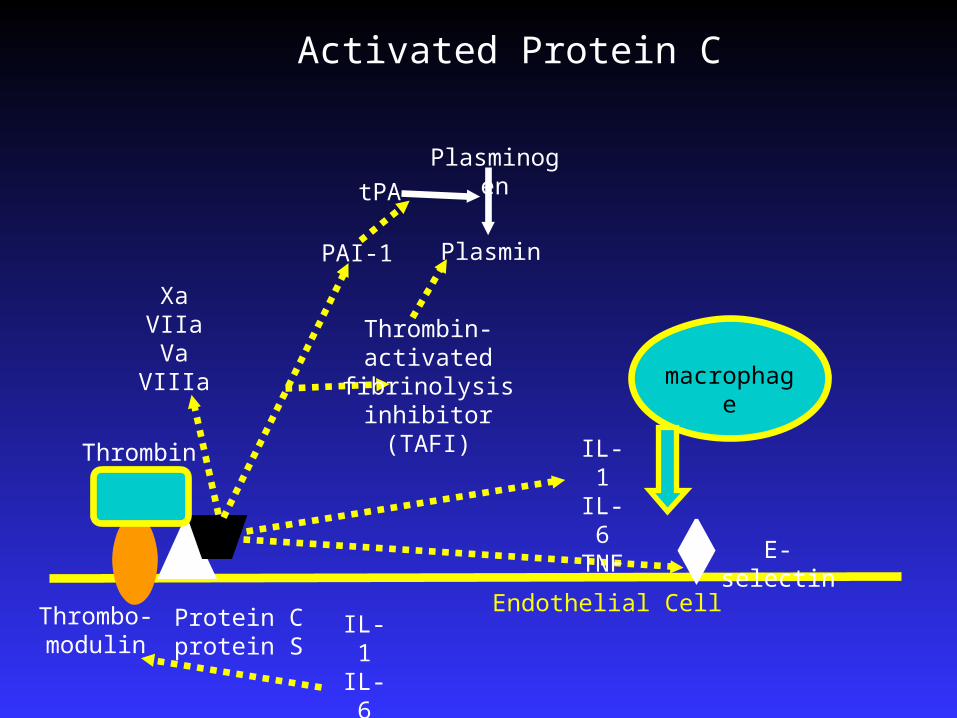
Protein Cprotein S
Endothelial Cell
E-selectin
IL-1IL-6TNF
macrophage
Activated Protein C
IL-1IL-6TNF
Thrombo-modulin
Thrombin
Thrombin-activated fibrinolysis inhibitor
(TAFI)
PAI-1 Plasmin
tPA
Plasminogen
XaVIIaVa
VIIIa

Activated Protein C
164 center study of patients with severe sepsis164 center study of patients with severe sepsis Known or suspected sepsisKnown or suspected sepsis >>3 signs of systemic infection w/in 24 h3 signs of systemic infection w/in 24 h Sepsis-induced organ dysfunction for <24 hSepsis-induced organ dysfunction for <24 h Begin therapy within 24 h of entry criteriaBegin therapy within 24 h of entry criteria
aPC infused for 96 haPC infused for 96 h 1728 randomized; 1690 received drug or placebo1728 randomized; 1690 received drug or placebo
~75% on ventilator and ~75% on vasopressor~75% on ventilator and ~75% on vasopressor + blood cultures in ~32.5%+ blood cultures in ~32.5%
Bernard et al. NEJM 2001; 344:699-709.

Activated Protein C
259/840 (30.8%) versus 210/850 259/840 (30.8%) versus 210/850 (24.7%) died at 28 days (p=0.005)(24.7%) died at 28 days (p=0.005) ARR = 6.2%; NNT = 16ARR = 6.2%; NNT = 16
Normal PC concentration:Normal PC concentration: 28/105 (26.7%) vs 14/90 (15.6%) 28/105 (26.7%) vs 14/90 (15.6%)
survivedsurvived

Summary
DIC is complex process; often non-overtDIC is complex process; often non-overt Recognition based on clinical condition Recognition based on clinical condition
and laboratory studiesand laboratory studies Treatment based on reversing Treatment based on reversing
underlying causeunderlying cause Heparin not helpful; AT may be helpful, Heparin not helpful; AT may be helpful,
but activated Protein C is useful in DIC but activated Protein C is useful in DIC complicating septic shockcomplicating septic shock





























