Embed Size (px)
Citation preview

Apichat Tantraworasin M.D., Ph.D., FRCS(T) General Thoracic Surgery Unit, Department of
Surgery, Faculty of Medicine, Chiang Mai University
วัตถุประสงค์การเรียนรู้
1. ทราบถึงอุบัติการณ์ ปัจจัยเส่ียง พยาธิสภาพ อาการและอาการแสดง การวินิจฉัยและการรักษาผู้ป่วยมะเร็งปอด
2. ทราบถึงอุบัติการณ์ ปัจจัยเส่ียง พยาธิสภาพ อาการและอาการแสดง การวินิจฉัยและการรักษา ผู้ป่วยท่ีมีก้อนใน mediastinum

Lung Cancer Incidence
Risk factors
Pathology and staging
Clinical presentation
Diagnostic procedure
Treatment

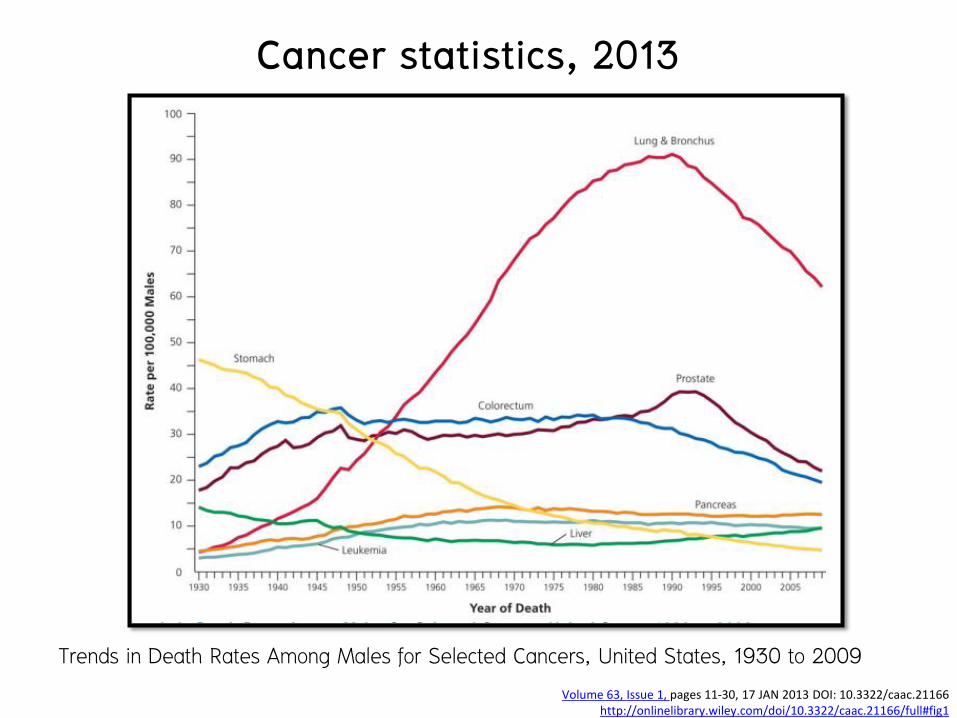
Cancer statistics, 2013
CA: A Cancer Journal for Clinicians Volume 63, Issue 1, pages 11-30, 17 JAN 2013 DOI: 10.3322/caac.21166
http://onlinelibrary.wiley.com/doi/10.3322/caac.21166/full#fig1

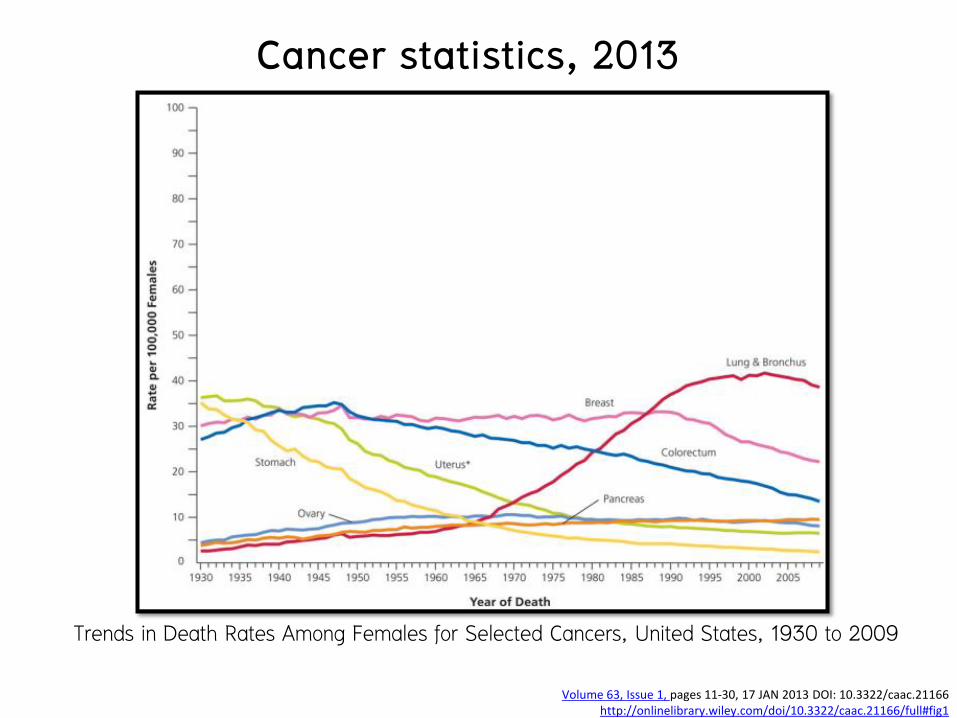
Cancer statistics, 2013
CA: A Cancer Journal for Clinicians Volume 63, Issue 1, pages 11-30, 17 JAN 2013 DOI: 10.3322/caac.21166
http://onlinelibrary.wiley.com/doi/10.3322/caac.21166/full#fig1
Trends in Cancer Incidence and Death Rates by Sex, United States, 1975 to 2009.
Cancer statistics, 2013
CA: A Cancer Journal for Clinicians Volume 63, Issue 1, pages 11-30, 17 JAN 2013 DOI: 10.3322/caac.21166
http://onlinelibrary.wiley.com/doi/10.3322/caac.21166/full#fig1
Trends in Death Rates Among Males for Selected Cancers, United States, 1930 to 2009
Cancer statistics, 2013
CA: A Cancer Journal for Clinicians Volume 63, Issue 1, pages 11-30, 17 JAN 2013 DOI: 10.3322/caac.21166
http://onlinelibrary.wiley.com/doi/10.3322/caac.21166/full#fig1
Trends in Death Rates Among Females for Selected Cancers, United States, 1930 to 2009

Lung Cancer: Risk factors
Cigarette smoking
• Primary cause of lung cancer
• Approximately 75% of all lung cancers worldwide in 2007
• Risk : Number of cigarettes smoked and the number of years of smoking
Polycyclic aromatic hydrocarbons DNA mutation

Lung Cancer: Risk factors Relative Risk of Lung Cancer in Smokers
Smoking Category Relative Risk
Never smoked 1.0
Currently smoke 15.8–16.3
Formerly smoked
Years of abstinence
1–9 5.9–19.5
10–19 2.0–6.1
>20 1.9–3.7

Lung Cancer: Risk factors
• Smoking cessation
• The risk never drops to that of people who never smoked
• 53% of cancers in women are not related to smoking
• 62% : adenocarcinomas
• Environmental tobacco smoke
• Residential radon
• Cooking oil vapors
• Indoor coal and wood burning
• Genetic factors: family history, CYP1A1 Ile462Val polymorphism, XRCC1 variants
• Viral factors: HPV 16 and 18

Lung Cancer: Risk factors
Other risk factors
Exposure to a number of industrial compounds
• Asbestos ( additive effect with cigarette smoking)
• Arsenic, and chromium compounds
COPD
History of tuberculosis with secondary scar formation

Lung Cancer: Pathology and staging
A. Preinvasive Lesions (Precancerous lesions)
1. Squamous Dysplasia and Carcinoma In Situ
2. Atypical Adenomatous Hyperplasia
3. Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia
B. Invasive or Malignant Lesions
1. Non–Small Cell Lung Carcinoma
2. Small cell lung carcinoma

Lung Cancer: Pathology and staging
Non-small cell carcinoma
• Squamous cell carcinoma
• Adenocarcinoma
• Adeno-squamous cell carcinoma
• Large cell carcinoma
• Neuroendocrine neoplasm

Lung Cancer: Pathology and staging
Squamous Cell Carcinoma • 30 - 40% of lung cancers
• Male > female
• Highly correlated with cigarette smoking
• Pathology
• Cells develop a pattern of clusters with intracellular bridges and keratin pearls

Lung Cancer: Pathology and staging
Squamous cell carcinoma
(A) Keratin pearl is an evidence of squamous cell differentiation. (H&E 200x )
(B) Intercellular bridges are also characteristic manifestation (H&E 400x )

Lung Cancer: Pathology and staging
Squamous Cell Carcinoma • Central lesion
• Often causing the typical symptoms of centrally located tumors • Hemoptysis
• Bronchial obstruction with atelectasis
• Dyspnea
• Pneumonia (obstructive pneumonia)
• Peripheral lesion
• Develop in a tuberculosis scar or in the wall of a bronchiectatic cavity

Lung Cancer: Pathology and staging
Central necrosis
• Air-fluid level
• Infection >> abscess formation
Mukherjee S et al 2011
Lung Cancer: Pathology and staging
Adenocarcinoma • 25 - 40% of all lung cancers
• Female > male
• Most often a peripherally based tumor
• Incidental finding on routine chest radiographs
• Symptoms
• Chest wall invasion or malignant pleural effusions

Lung Cancer: Pathology and staging
(A) Acinar adenocarcinoma consists of round to oval shaped malignant glandular structures with stromal infiltration (H&E 100x ) (B) Papillary adenocarcinoma composed of papillary proliferation along fibrovascular cores lined by malignant cuboidal to columnar tumor cells (H&E 100x )

Lung Cancer: Pathology and staging Preinvasive lesions
• Atypical adenomatous hyperplasia
• Adenocarcinoma in situ (≤ 3 cm, pure lepidic growth without invasion, formerly BAC)
• Nonmucinous
• Mucinous
• Mixed mucinous/nonmucinous
Minimally invasive adenocarcinoma
(≤ 3 cm lepidic predominant tumor with ≤ 5mm invasion)
• Nonmucinous
• Mucinous
• Mixed mucinous/nonmucinous
• Note: BAC, bronchioloalveolar carcinoma.
IASLC/ATS/ERS Classification of Lung Adenocarcinoma in Resection Specimens
Modified from Van Schil PE et al.(Van Schil et al. 2013)

Lung Cancer: Pathology and staging Invasive adenocarcinoma
Lepidic predominant (formerly nonmucinous BAC pattern, with >5mm
invasion)
Acinar predominant
Papillary predominant
Micropapillary predominant
Solid predominant with mucin production
Variants of invasive adenocarcinoma
Invasive mucinous adenocarcinoma (formerly mucinous BAC)
Colloid
Fetal (low and high grade)
Enteric Note: BAC, bronchioloalveolar carcinoma.
IASLC/ATS/ERS Classification of Lung Adenocarcinoma in Resection Specimens
Modified from Van Schil PE et al.(Van Schil et al. 2013)
Lung Cancer: Pathology and staging
Large Cell Carcinoma
• 10 - 20% of lung cancers
• Located centrally or peripherally
• cells are large, with diameters of 30 - 50 m
• Often admixed with other cell types such as squamous cells or adenocarcinoma

Lung Cancer: Pathology and staging
Neuroendocrine carcinoma (NEC)
• IHC : chromogranins, synaptophysin, CD57, and neuron-specific enolase
• 3 grade

Lung Cancer: Pathology and staging Neuroendocrine carcinoma (NEC) • Grade I NEC (classic or typical carcinoid)
• Low-grade NEC • Young patient • Central airways
• Hemoptysis with or without airway obstruction and pneumonia
• 15 % regional LN metastasis, rarely systemic metastasis • Histology
• Cells are arranged in cords and clusters with a rich vascular stroma.



Lung Cancer: Pathology and staging Neuroendocrine carcinoma (NEC) • Grade II NEC (atypical carcinoid)
• Cigarette smoking • Peripheral lesion • Histology
• Areas of necrosis, nuclear pleomorphism, and higher mitotic rates. • Much higher malignant potential
• 30 - 50% LN metastases • 25% metastases at time of diagnosis

Lung Cancer: Pathology and staging
Neuroendocrine carcinoma (NEC)
• Grade III NEC large cell–type tumors
• Heavy smokers
• Middle to peripheral lung fields
• Often large with central necrosis and a high mitotic rate

Lung Cancer: Pathology and staging Neuroendocrine carcinoma (NEC) • Grade III NEC small cell type [small cell lung carcinoma
(SCLC)] • Most malignant NEC and accounts for 25% of all lung cancers • Centrally located and consist of smaller cells with a diameter of
10 - 20 mm that have little cytoplasm and very dark nuclei. • High mitotic rate and areas of extensive necrosis • Multiple mitoses • Paraneoplastic syndromes


Lung Cancer: Pathology and staging
Salivary Gland–Type Neoplasms • Salivary-type submucosal bronchial glands at tracheobronchial tree
• Central lesion : site of origin
• 2 most common
1. Adenoid cystic carcinoma
• Slow-growing tumor : locally and systematically invasive
• Grow submucosally and infiltrate along perineural sheaths
2. Mucoepidermoid carcinoma
• Squamous and mucous cells : low or high grade, depending on the mitotic rate and degree of necrosis
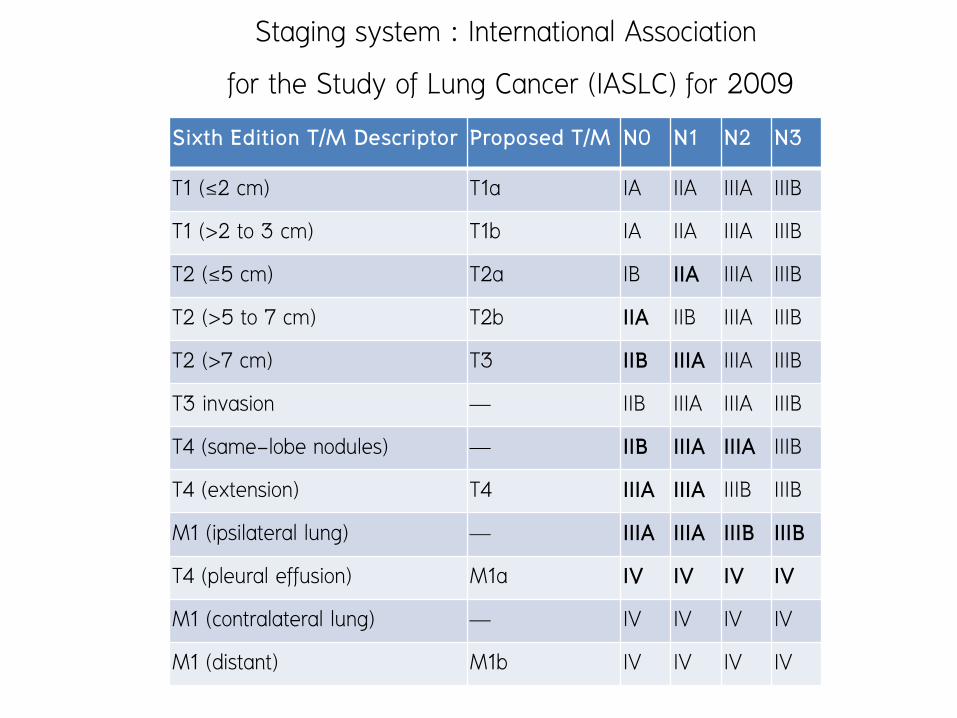
Staging system : International Association for the Study of Lung Cancer (IASLC) for 2009
Sixth Edition T/M Descriptor Proposed T/M N0 N1 N2 N3
T1 (≤2 cm) T1a IA IIA IIIA IIIB
T1 (>2 to 3 cm) T1b IA IIA IIIA IIIB
T2 (≤5 cm) T2a IB IIA IIIA IIIB
T2 (>5 to 7 cm) T2b IIA IIB IIIA IIIB
T2 (>7 cm) T3 IIB IIIA IIIA IIIB
T3 invasion — IIB IIIA IIIA IIIB
T4 (same-lobe nodules) — IIB IIIA IIIA IIIB
T4 (extension) T4 IIIA IIIA IIIB IIIB
M1 (ipsilateral lung) — IIIA IIIA IIIB IIIB
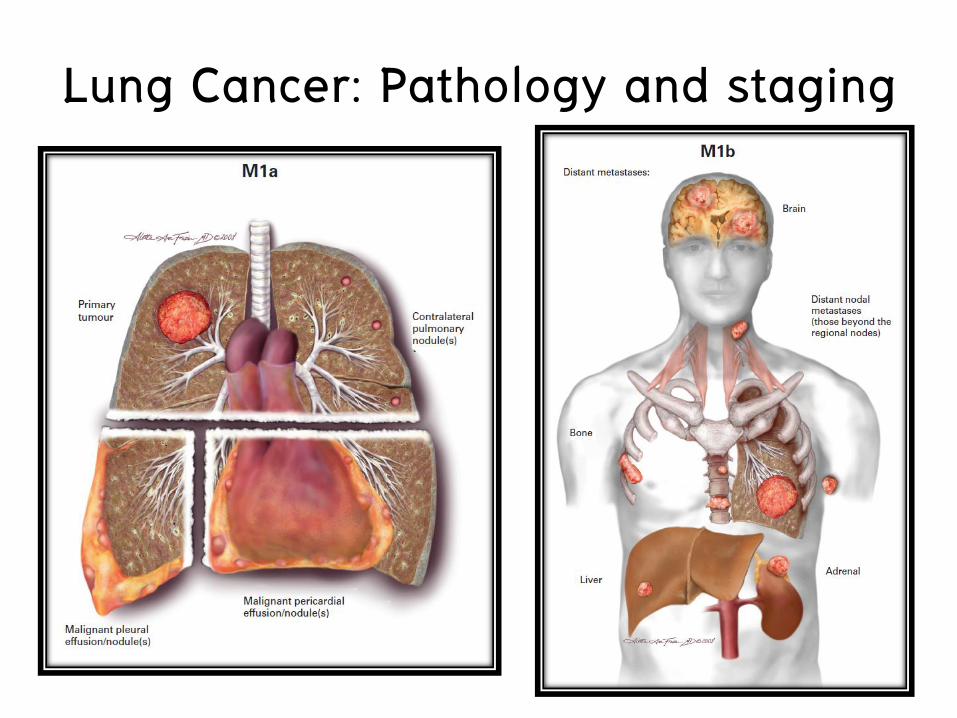
T4 (pleural effusion) M1a IV IV IV IV
M1 (contralateral lung) — IV IV IV IV
M1 (distant) M1b IV IV IV IV

Lung Cancer: Pathology and staging

Lung Cancer: Pathology and staging

Lung Cancer: Pathology and staging N1 = intrapulmonary node N2 = mediastinal LN N3 = cervical LN and supraclavicular LN

Lung Cancer: Pathology and staging

Lung Cancer: Pathology and staging
Lung Cancer: Pathology and staging

Lung Cancer: Clinical Presentation
Asymptomatic >>>> life threatening conditions related to ..
1) Histologic features
2) Specific tumor location
3) Biologic features, and the production of a variety of paraneoplastic syndromes
4) Presence or absence of metastatic disease

Lung Cancer: Clinical Presentation Category Symptom Cause
Pulmonary symptoms Cough Bronchus irritation or compression
Dyspnea Airway obstruction or compression
Wheezing >50% airway obstruction
Hemoptysis Tumor erosion or irritation
Pneumonia Airway obstruction
• Central airway symptoms : squamous cell and small CA • Incidental findings or asymptomatic peripheral lesion : adenocarcinoma

Lung Cancer: Clinical Presentation Category Symptom Cause
Nonpulmonary thoracic symptoms
Pleuritic pain Parietal pleural irritation or invasion
Local chest wall pain Rib and/or muscle involvement
Radicular chest pain Intercostal nerve involvement
Pancoast's syndrome Stellate ganglion, chest wall, brachial plexus involvement
Hoarseness Recurrent laryngeal nerve involvement
Swelling of head and arms Bulky involved mediastinal lymph nodes
Medially based right upper lobe tumor

Lung Cancer: Clinical Presentation BAC (a variant of adenocarcinoma)
a) Solitary nodule b) Multifocal nodules
c) Diffuse infiltrate mimicking an infectious pneumonia (pneumonic form)
• Severe dyspnea and hypoxia • Expectoration of large volumes (over 1 L/d) of light tan fluid
–Dehydration and electrolyte imbalance. – Typical invasion, destruction, and compression of lung
architecture
–Air bronchograms.
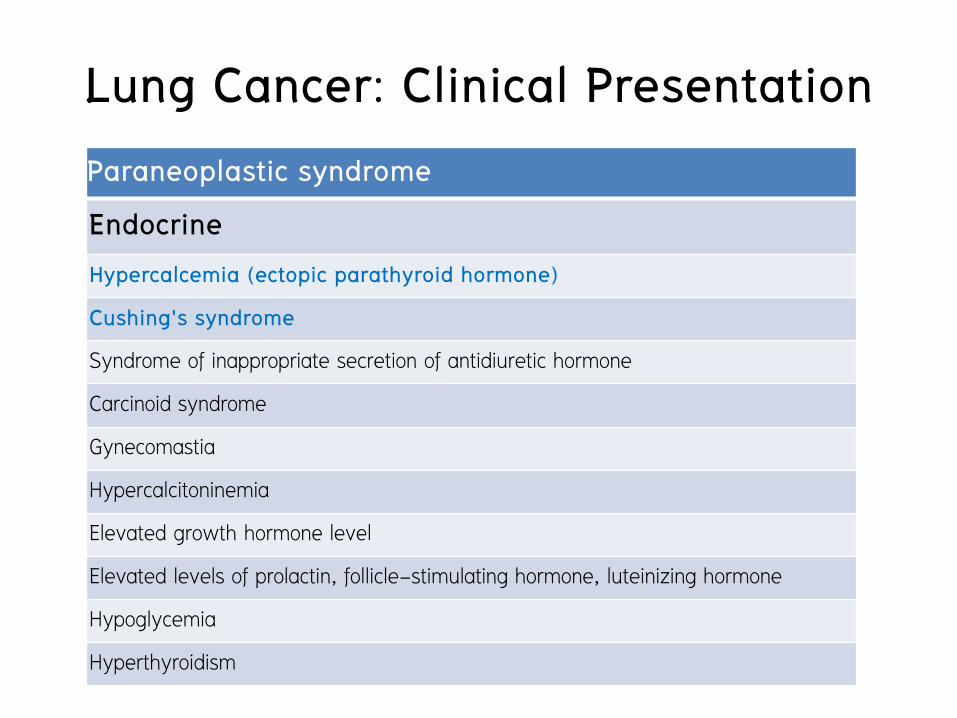
Lung Cancer: Clinical Presentation Paraneoplastic syndrome
Endocrine
Hypercalcemia (ectopic parathyroid hormone)
Cushing's syndrome
Syndrome of inappropriate secretion of antidiuretic hormone
Carcinoid syndrome
Gynecomastia
Hypercalcitoninemia
Elevated growth hormone level
Elevated levels of prolactin, follicle-stimulating hormone, luteinizing hormone
Hypoglycemia
Hyperthyroidism
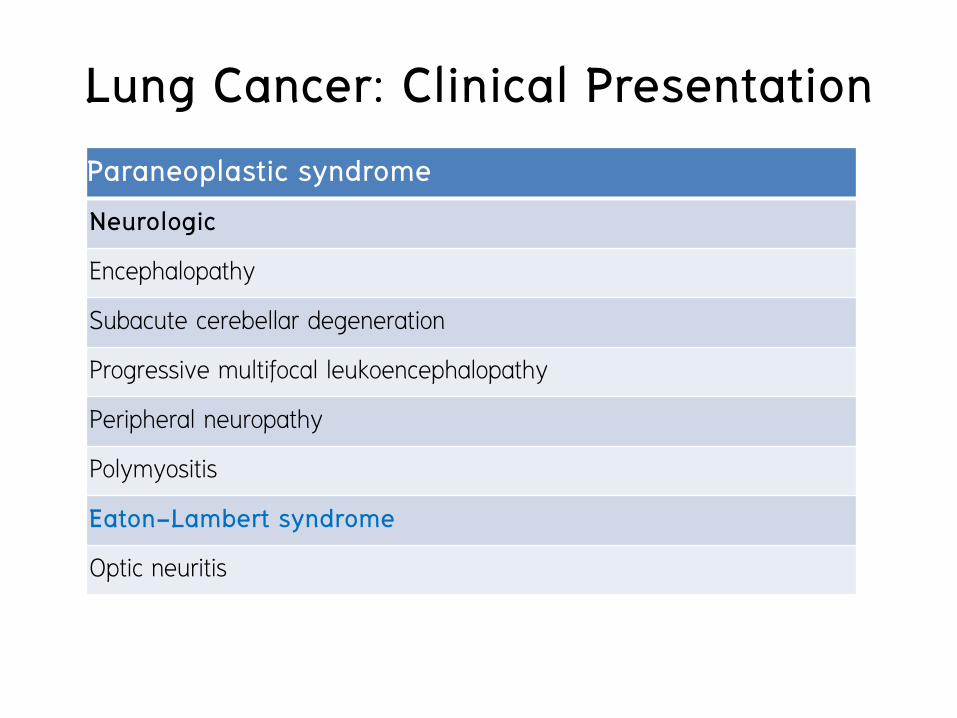
Lung Cancer: Clinical Presentation Paraneoplastic syndrome Neurologic
Encephalopathy
Subacute cerebellar degeneration
Progressive multifocal leukoencephalopathy
Peripheral neuropathy
Polymyositis
Eaton-Lambert syndrome
Optic neuritis

Lung Cancer: Clinical Presentation Paraneoplastic syndrome Skeletal
Clubbing
Pulmonary hypertrophic osteoarthropathy
Hematologic
Anemia Leukemoid reactions
Thrombocytosis Thrombocytopenia
Eosinophilia Pure red cell aplasia
Leukoerythroblastosis Disseminated intravascular coagulation
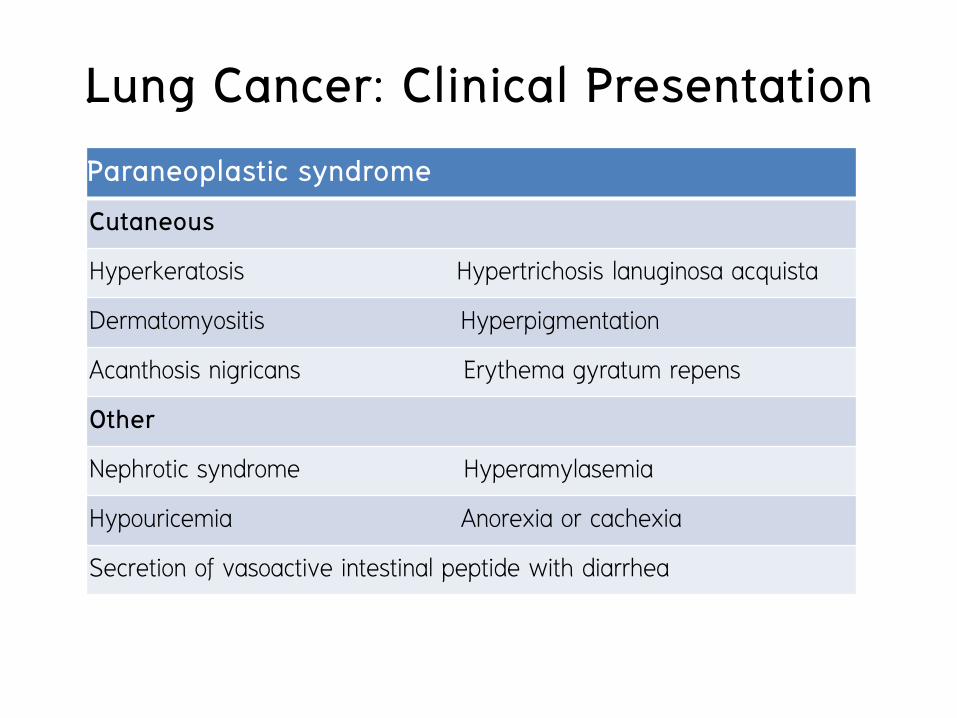
Lung Cancer: Clinical Presentation Paraneoplastic syndrome Cutaneous
Hyperkeratosis Hypertrichosis lanuginosa acquista
Dermatomyositis Hyperpigmentation
Acanthosis nigricans Erythema gyratum repens
Other
Nephrotic syndrome Hyperamylasemia
Hypouricemia Anorexia or cachexia
Secretion of vasoactive intestinal peptide with diarrhea
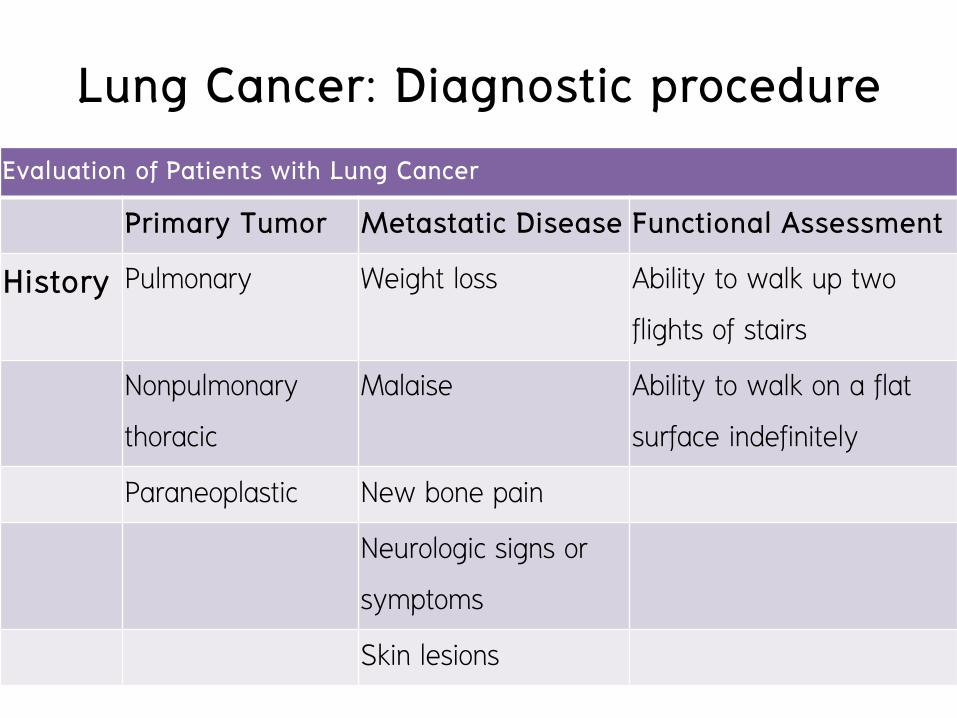
Lung Cancer: Diagnostic procedure Evaluation of Patients with Lung Cancer
Primary Tumor Metastatic Disease Functional Assessment
History Pulmonary Weight loss Ability to walk up two flights of stairs
Nonpulmonary thoracic
Malaise Ability to walk on a flat surface indefinitely
Paraneoplastic New bone pain Neurologic signs or
symptoms
Skin lesions
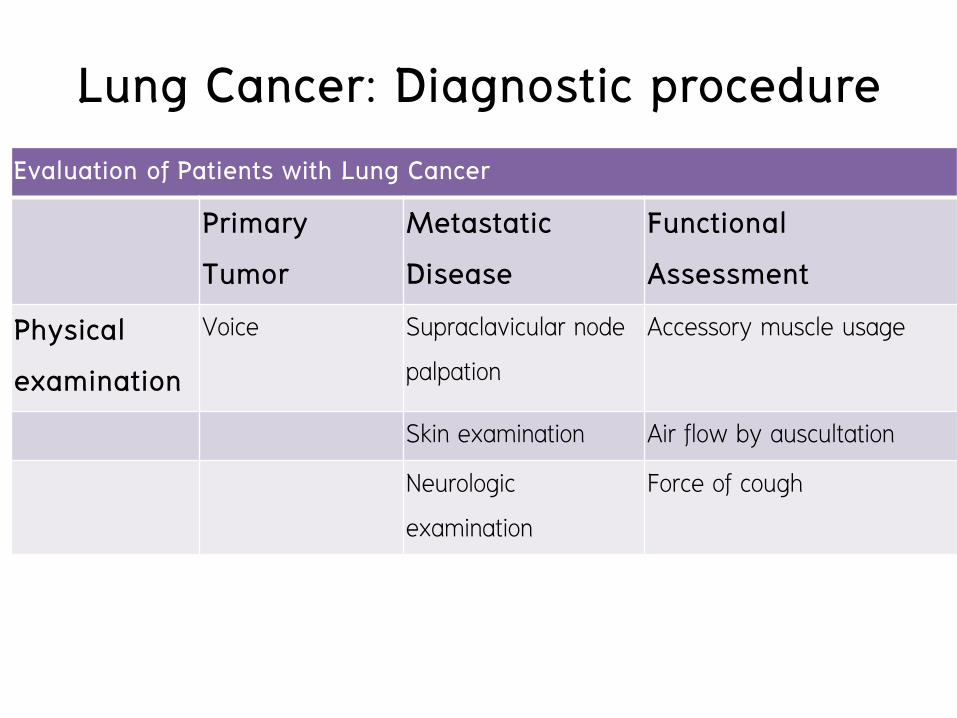
Lung Cancer: Diagnostic procedure Evaluation of Patients with Lung Cancer
Primary Tumor
Metastatic Disease
Functional Assessment
Physical examination
Voice Supraclavicular node palpation
Accessory muscle usage
Skin examination Air flow by auscultation
Neurologic examination
Force of cough

Lung Cancer: Diagnostic procedure Evaluation of Patients with Lung Cancer
Primary Tumor Metastatic Disease
Functional Assessment
Radiographic examination
CXR, Chest CT CXR, Chest CT, PET Chest CT: tumor anatomy, atelectasis
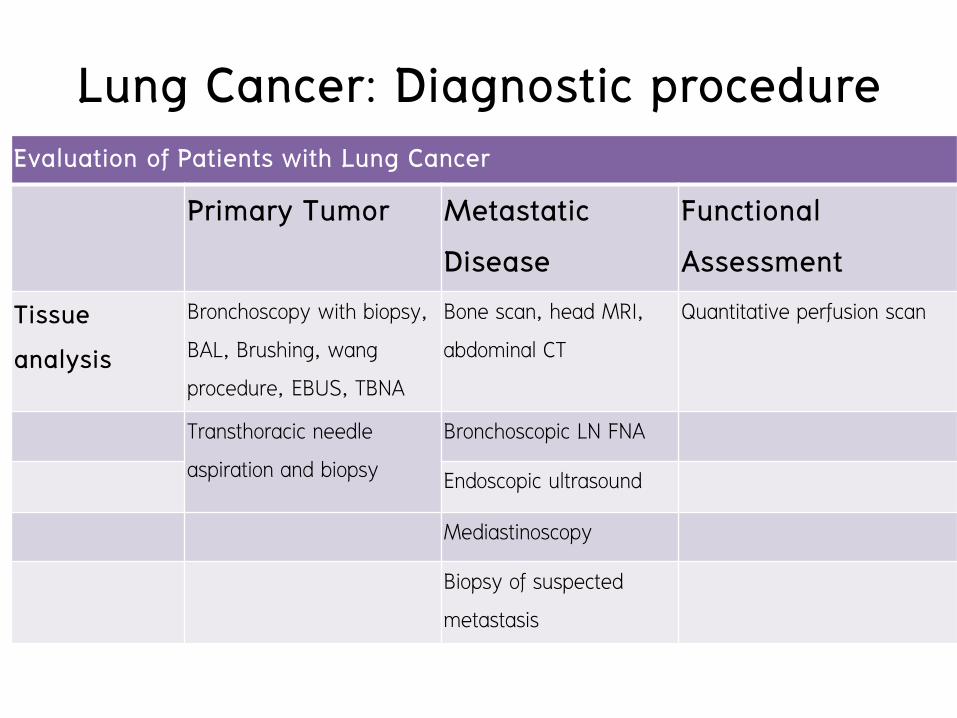
Lung Cancer: Diagnostic procedure Evaluation of Patients with Lung Cancer
Primary Tumor Metastatic Disease
Functional Assessment
Tissue analysis
Bronchoscopy with biopsy, BAL, Brushing, wang procedure, EBUS, TBNA
Bone scan, head MRI, abdominal CT
Quantitative perfusion scan
Transthoracic needle aspiration and biopsy
Bronchoscopic LN FNA
Endoscopic ultrasound
Mediastinoscopy
Biopsy of suspected metastasis

Lung Cancer: Diagnostic procedure Evaluation of Patients with Lung Cancer
Primary Tumor Metastatic Disease
Functional Assessment
Other Thoracoscopy Thoracoscopy Pulmonary function tests (FEV1, DLCO, O2 consumption)

Lung Cancer: Diagnostic procedure

Lung Cancer: Diagnostic procedure
CT scan with contrast
(Chest and upper abdomen)

Lung Cancer: Diagnostic procedure
Positron Emission Tomography • Measure metabolic activity of cell ( glucose metabolism -
uptake of 18 –flurodeoxyglucose )
• Taken up by cells in glycolysis but is bound cells (cannot enter normal glycolytic pathway )
• Most tumors have greater uptake of FDG than normal tissue

Lung Cancer: Diagnostic procedure Positron Emission Tomography • For identifying a malignancy
• Sensitivity is 96.8 % • Specificity 77.8 %
• Fasle negative: Slow growing tumor • BAC • Carcinoids • Tumor < 1 cm



Lung Cancer: Diagnostic procedure PET & CT scan

Lung Cancer: Diagnostic procedure
Fiberoptic bronchoscopy

Lung Cancer: Diagnostic procedure
Rigid bronchoscope
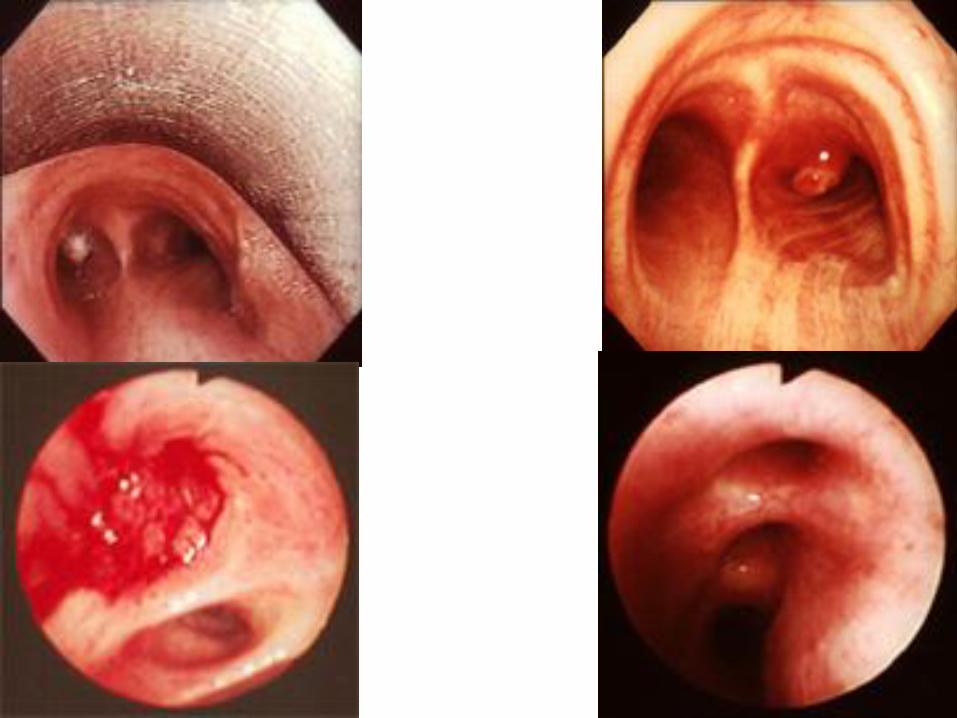

Transbronchial needle aspiration (TBNA)
Lung Cancer: Diagnostic procedure

Endobronchial ultrasound-guided fine needle aspiration (EBUS)
Lung Cancer: Diagnostic procedure

Mediastinoscopy
Lung Cancer: Diagnostic procedure
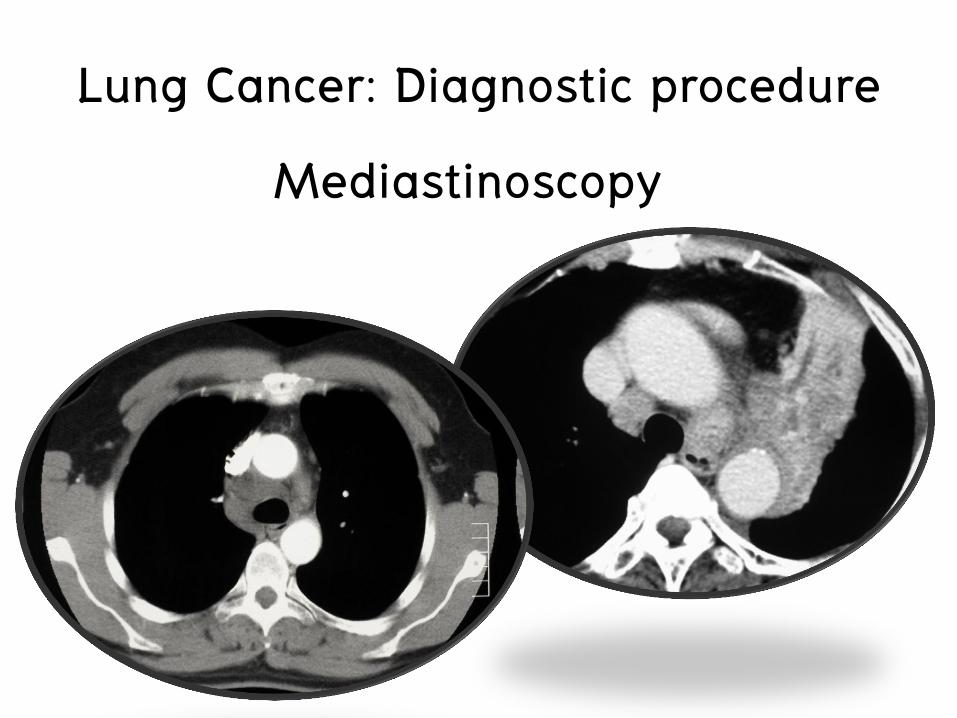
Mediastinoscopy
Lung Cancer: Diagnostic procedure


Lung Cancer: Diagnostic procedure
VATS (video-assisted thoracoscopic surgery)

Lung Cancer: Diagnostic procedure
VATS (video-assisted thoracoscopic surgery)

Lung Cancer: Diagnostic procedure
Assessment of Functional status
• Clinician’s assessment
• Daily activity
• Smoking status
• Pulmonary function test (PFT)

Lung Cancer: Diagnostic procedure
Assessment of Functional status Clinician’s assessment
• Walk on a flat surface indefinitely • Likely to tolerate thoracotomy and lobectomy
• Walk up two flights of stairs (up two standard levels) • Likely tolerate pneumonectomy
• ABG : no CO2 retention : tolerate periods of single-lung ventilation and wedge resection

Lung Cancer: Diagnostic procedure
Assessment of Functional status Clinician’s assessment
• Walk on a flat surface indefinitely • Likely to tolerate thoracotomy and lobectomy
• Walk up two flights of stairs (up two standard levels) • Likely tolerate pneumonectomy
• ABG : no CO2 retention : tolerate periods of single-lung ventilation and wedge resection

Lung Cancer: Diagnostic procedure Assessment of Functional status Clinician’s assessment • Smoking status and sputum production
• Current smokers : increase risk of postoperative pulmonary complications • Respiratory failure requiring ICU or reintubation • Pneumonia • Atelectasis requiring bronchoscopy • Pulmonary embolism • Discharge with oxygen supplementation

Lung Cancer: Diagnostic procedure
Assessment of Functional status
Clinician’s assessment
• Recommendation for cessation of smoking
• Ideally, at least 8 weeks preoperatively in benign cases
• 2 weeks before surgery in cancer cases

Lung Cancer: Diagnostic procedure
Assessment of Functional status
Pulmonary function test (PFT)
• FEV1 (forced expiratory volume in 1 second)
• DLCO (carbon monoxide diffusion capacity)
• VO2max (maximum oxygen consumption)


Lung Cancer: Treatment
Depend on T N M stage of disease
Surgery
Radiotherapy Chemothorapy
Target therapy

Lung Cancer: Treatment
Surgery
• Lobectomy
• Combined wedge and lobectomy
• Pneumonectomy
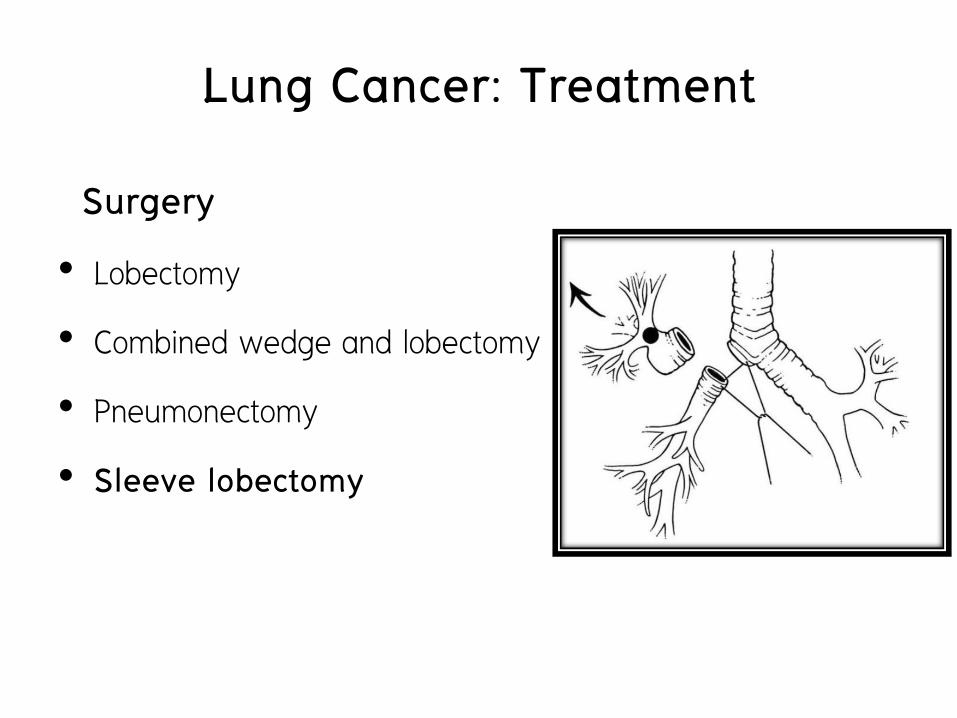
Lung Cancer: Treatment
Surgery
• Lobectomy
• Combined wedge and lobectomy
• Pneumonectomy
• Sleeve lobectomy

Lung Cancer: Treatment
Surgery
• Lobectomy
• Combined wedge and lobectomy
• Pneumonectomy
• Sleeve lobectomy
• Sublobar resection
• Clinical stage I and II NSCLC with
decreased pulmonary function or comorbid
disease • Margin :
• Tumor < 2 cm • Margin > maximal tumor
diameter • Tumors > 2 cm
• At least 2 cm gross margins
3rd Edition of ACCP guideline (2013)

Lung Cancer: Treatment Systematic mediastinal LN dissection or sampling

Lung Cancer: Treatment
Surgery
Approach : Open thoracotomy or VATS
Position: lateral decubitus position



Lung Cancer: Treatment Chemotherapy
• Platinum-based regimen : Cisplatin or Carboplatin
• Adjuvant
• Neoadjuvant chemotherapy
• Adjuvant chemotherapy
• Treatment
• 1st, 2nd, 3rd, 4th …. Line

Lung Cancer: Treatment
Chemotherapy : Neoadjuvant and adjuvant therapy
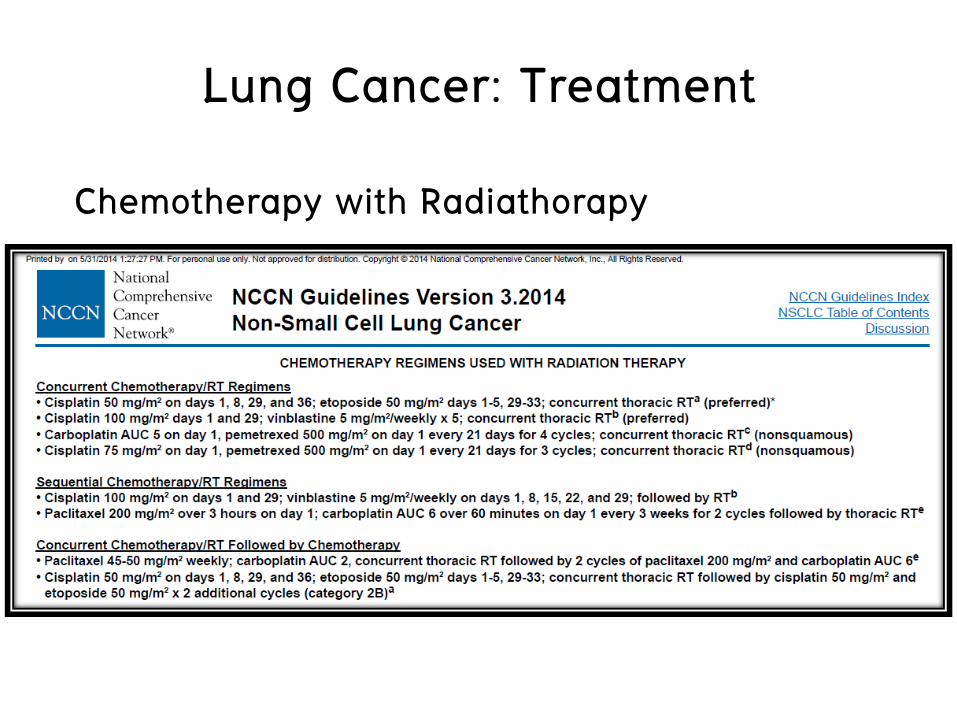
Lung Cancer: Treatment
Chemotherapy with Radiathorapy

Lung Cancer: Treatment
Chemotherapy : Advanced disease

Lung Cancer: Treatment
Radiotherapy Early stage(stage I)
• SABR (stereotactic ablative radiotherapy) • Medically inoperable or refuse to have surgery
Locally advanced (stage II, III)
• Resectable cases: preoperative concurrent chemoRT
• Unresectable cases : Concurrent chemoRT
Advanced or metastasis (stage IV)
• Local palliation or prevention of symptoms
http://cancer.stanford.edu/radiationoncology/treatment/stereotactic_radiotherapy.html

Lung Cancer: Treatment
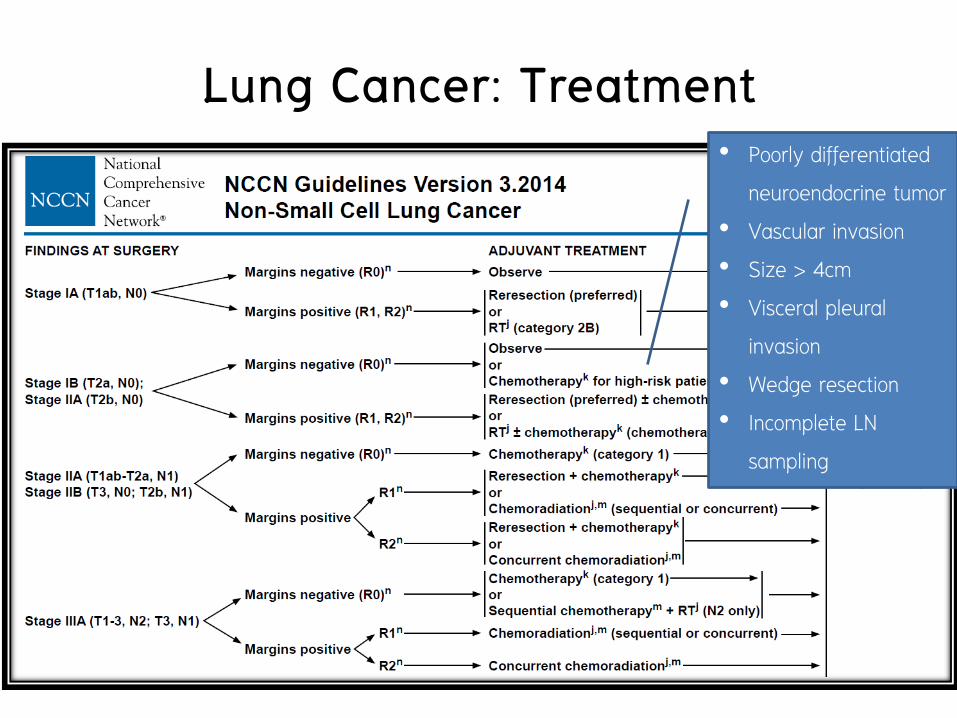
Lung Cancer: Treatment
• Poorly differentiated
neuroendocrine tumor • Vascular invasion • Size > 4cm • Visceral pleural
invasion • Wedge resection • Incomplete LN
sampling
Lung Cancer: Treatment

Lung Cancer: Treatment

Lung Cancer: Treatment

Lung Cancer: Treatment
Long-term follow-up care
Cancer Surveillance
• H&P and chest CT ± contrast every 6-12 mo for 2 yr, then H&P and a non-contrast-enhanced chest CT annually
• Smoking cessation advice, counseling, and pharmacotherapy
Immunizations
• Annual influenza vaccine, herpes zoster vaccine
• Pneumococcal vaccination with revaccination as appropriate
Lung Cancer: Treatment

Long-term follow-up care
Health promotion and wellness
• Maintain a healthy weight
• Regular physical activity: 30 minutes of moderate-intensity physical activity on most days of the week)
• Consume a healthy diet with emphasis on plant sources
• Limit consumption of alcohol if one consumes alcoholic beverages
Lung Cancer: Treatment

Long-term follow-up care
Additional health monitoring
• Routine BP, cholesterol, and glucose monitoring
• Bone health: bone density testing as appropriate
• Dental health : routine dental examination
• Routine sun protection
Lung Cancer: Treatment

Mediastinal mass

Mediastinal mass
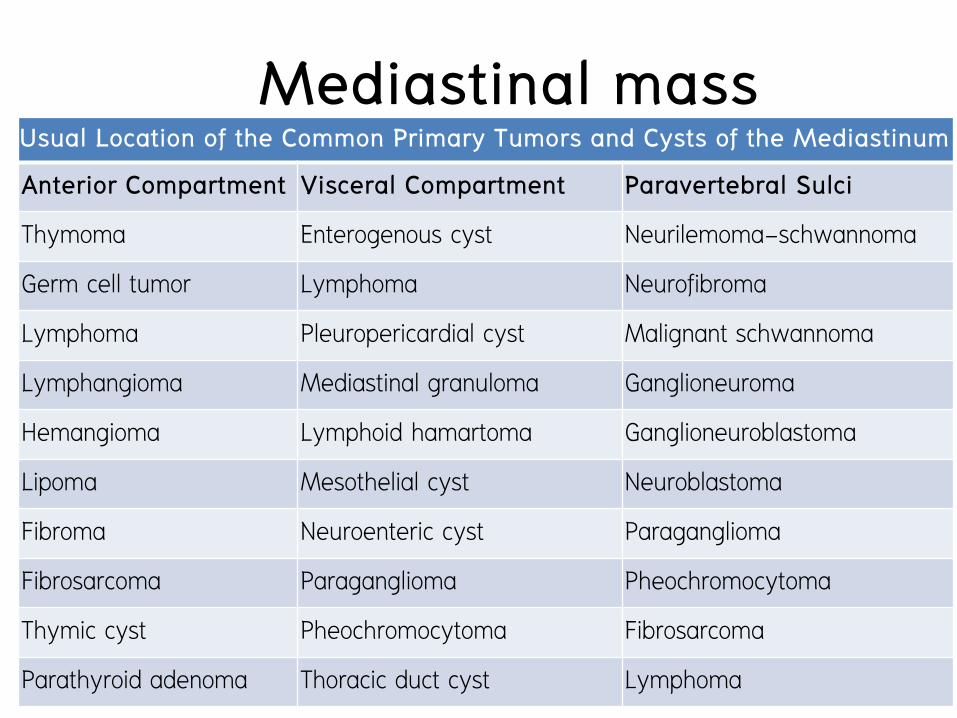
Mediastinal mass Usual Location of the Common Primary Tumors and Cysts of the Mediastinum
Anterior Compartment Visceral Compartment Paravertebral Sulci
Thymoma Enterogenous cyst Neurilemoma-schwannoma
Germ cell tumor Lymphoma Neurofibroma
Lymphoma Pleuropericardial cyst Malignant schwannoma
Lymphangioma Mediastinal granuloma Ganglioneuroma
Hemangioma Lymphoid hamartoma Ganglioneuroblastoma
Lipoma Mesothelial cyst Neuroblastoma
Fibroma Neuroenteric cyst Paraganglioma
Fibrosarcoma Paraganglioma Pheochromocytoma
Thymic cyst Pheochromocytoma Fibrosarcoma
Parathyroid adenoma Thoracic duct cyst Lymphoma

Mediastinal mass Mediastinal Tumors in Adults
Tumor Type Percentage of Total Location
Neurogenic tumors 21 Posterior
Cysts 20 All
Thymomas 19 Anterior
Lymphomas 13 Anterior/middle
Germ cell tumors 11 Anterior
Mesenchymal tumors 7 All
Endocrine tumors 6 Anterior/middle

Mediastinal mass Mediastinal Tumors in Children
Tumor Type Percentage of Total Location Neurogenic tumors 40 Posterior
Lymphomas 18 Anterior/middle
Cysts 18 All
Germ cell tumors 11 Anterior
Mesenchymal tumors 9 All
Thymomas Rare Anterior

Mediastinal mass Symptoms and signs
• 2/3 of mediastinal tumors in adults
• Asymptomatic abnormalities
• Incidental finding from radiologic studies
• Symptomatic : malignant
• Size, location, rate of growth, and associated inflammation

Mediastinal mass Symptoms and signs • Cough, dyspnea on exertion, or stridor
• Large, bulky tumors, expanding cysts, and teratomas • Compression of mediastinal structures : trachea
• Chest pain or dyspnea • Pleural effusion, cardiac tamponade, or phrenic nerve
involvement
• Hoarseness • Mass or LN at AP window compress LRLN

Mediastinal mass Signs and Symptoms Suggestive of Various Diagnoses in the Setting of a Mediastinal Mass
Diagnosis History and Physical Findings Compartment Location of Mass
Lymphoma Night sweats, weight loss, fatigue, extrathoracic adenopathy, elevated erythrocyte sedimentation rate or C-reactive protein level, leukocytosis
Any compartment

Mediastinal mass Signs and Symptoms Suggestive of Various Diagnoses in the Setting of a Mediastinal Mass
Diagnosis History and Physical Findings Compartment Location of Mass
Thymoma with myasthenia gravis
Fluctuating weakness, early fatigue, ptosis, diplopia
Anterior
Mediastinal granuloma
Dyspnea, wheezing, hemoptysis Visceral (middle)
Germ cell tumor Male gender, young age, testicular mass, elevated levels of human chorionic gonadotropin (B-hCG) and/or alpha-fetoprotein (AFP)
Anterior

Mediastinal mass Diagnostic Evaluation
Imaging • Contrast-enhanced CT scans
• MRI : invasion of vascular structures or spinal involvement
• PET scan : unclear, benign vs malignancy
• Single-photon emission computed tomography (SPECT) • 3D localization of some tumors of endocrine origin

Mediastinal mass Nuclear Imaging Relevant to the Mediastinum
Radiopharmaceutical, Radionuclide, or Radiochemical
Label Disease of Interest
Iodine 131I, 123I
Retrosternal goiter, thyroid cancer
Monoclonal antibodies 111In, 99mTc
NSCLC, colon and breast cancer, prostate cancer metastases
Octreotide 111In
Amine precursor uptake decarboxylation tumors: carcinoid, gastrinoma, insulinoma, small cell lung cancer, pheochromocytoma, glucagonoma, medullary thyroid carcinoma, paraganglioma
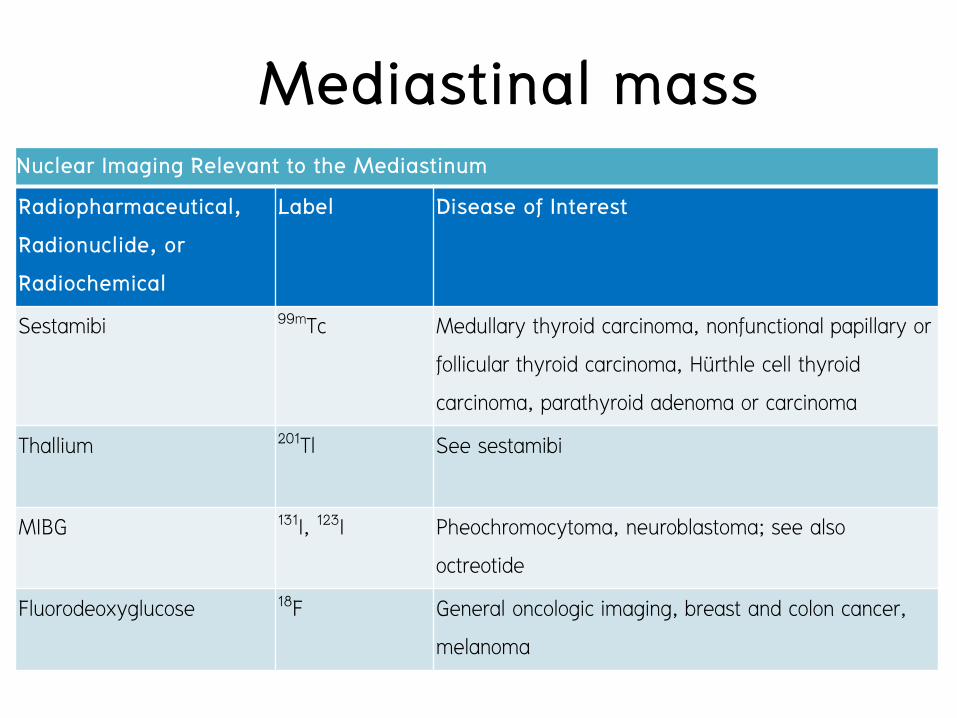
Mediastinal mass Nuclear Imaging Relevant to the Mediastinum
Radiopharmaceutical, Radionuclide, or Radiochemical
Label Disease of Interest
Sestamibi 99mTc
Medullary thyroid carcinoma, nonfunctional papillary or follicular thyroid carcinoma, Hürthle cell thyroid carcinoma, parathyroid adenoma or carcinoma
Thallium 201Tl
See sestamibi
MIBG 131I, 123I
Pheochromocytoma, neuroblastoma; see also octreotide
Fluorodeoxyglucose 18F
General oncologic imaging, breast and colon cancer, melanoma

Mediastinal mass Diagnostic Evaluation Serum markers • Alpha-fetoprotein (AFP) and human chorionic gonadotropin (hCG)
• Nonseminomatous germ cell tumors • > 90 % • > 500 ng/mL specificity close to 100% • Definite diagnosis without tissue biopsy (some center)
• Seminoma • Normal AFP • 10 % : hCH < 100 ng/mL
Mediastinal mass Diagnostic Evaluation
Serum markers
• Parathyroid hormone
• Ectopic parathyroid adenoma

Mediastinal mass Diagnostic Nonsurgical Biopsy of the Mediastinum Noninvasive imaging and history • Surgical removal in resectable disease : thymoma, substernal
goiter etc. Biopsy • Nonsurgical disease : lymphoma, germ cell tumor etc. • Limited by overlying bony thoracic cavity and the proximity to
lung tissue, the heart, and great vessels • Core-needle technique or surgery > FNA
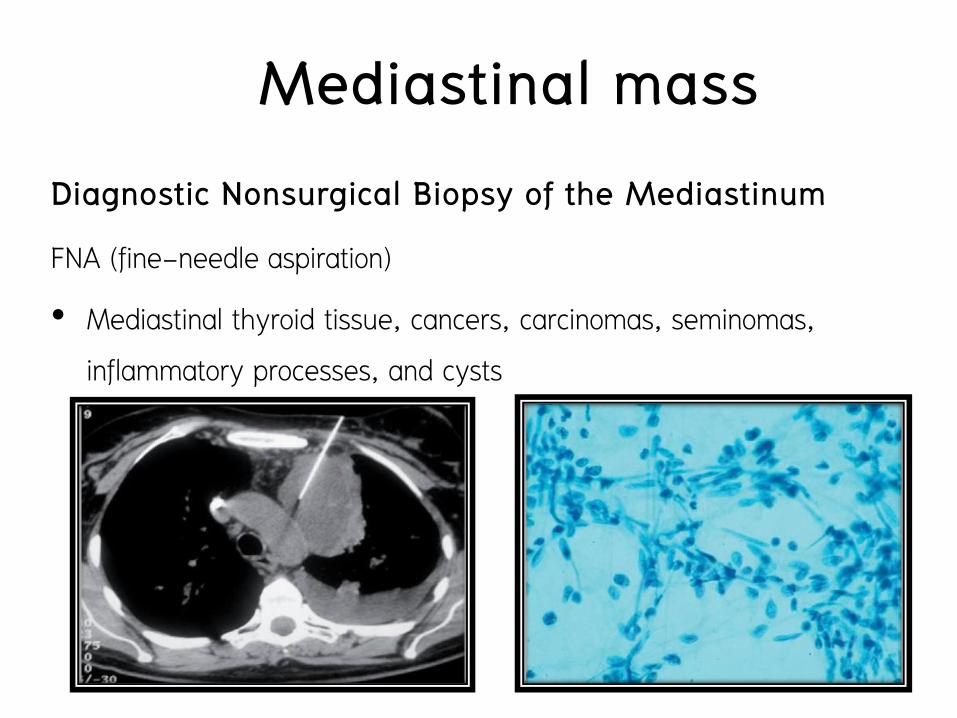
Mediastinal mass Diagnostic Nonsurgical Biopsy of the Mediastinum
FNA (fine-needle aspiration)
• Mediastinal thyroid tissue, cancers, carcinomas, seminomas, inflammatory processes, and cysts
Virginia et al 2010

Mediastinal mass Diagnostic Nonsurgical Biopsy of the Mediastinum
Core-needle biopsy
• Nonsurgical disease : lymphoma, germ cell tumor etc.
Li Li et al 2005

Mediastinal mass Surgical Biopsy and Resection of Mediastinal Masses
• Failed to FNA or CNB
• Completely removed evaluated by CT scan
• Median sternotomy or lateral thoracotomy (gold standard)
• VATS : romoval of the thymus gland in MG cases or small encapsulated thymomas ( < 2 cm)

Mediastinal mass Surgical Biopsy and Resection of Mediastinal Masses
• Large or incompletely removed due to invade vital structure such as heart, SVC or great vessels
• Parasternal biopsy
• Mediastinoscopy
• VATS to biopsy
Mediastinal mass Neoplasms :Thymus
Thymic Hyperplasia
• Children after treating lymphoma : Diffuse thymic hyperplasia
• Adult : Rebound thymic hyperplasia
• 2-12 months (mean 9 months) after chemotherapy for lymphoma or germ cell tumors
• Requiring careful follow-up with serial CT scans
• PET scan


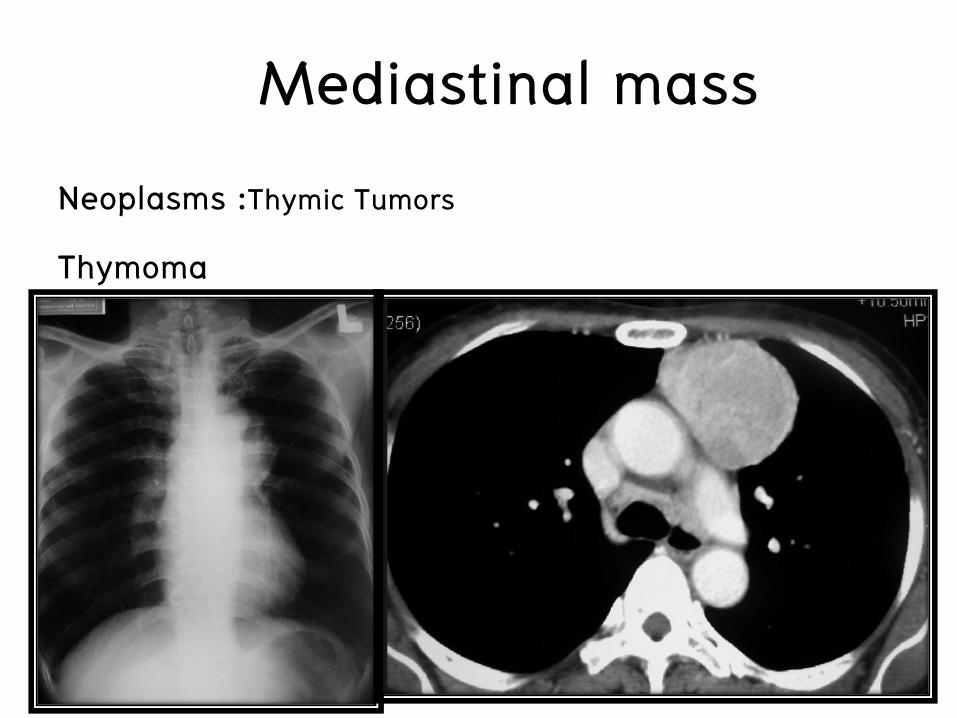
Mediastinal mass Neoplasms :Thymic Tumors
Thymoma
• Most common of anterior mediastinal mass
• 40-60 years of age, rare in children
• Asympthomatic
• Symptomatic : mass effect • Cough, chest pain, dyspnea, or superior vena caval syndrome

Mediastinal mass Neoplasms :Thymic Tumors
Thymoma • 10-50% of thymoma have MG or circulating antibodies to
acetylcholine receptor • < 10 % of MG are found to have a thymoma on CT • MG with thymoma
• Improvement or resolution of symptoms of MG in only approximately 25% after treated with thymectomy
• Mg without thymoma • 90 % improve and up to 50% complete remission treated with
thymectomy

Mediastinal mass Neoplasms :Thymic Tumors
Thymoma
• 5% of patients with thymomas
• Red cell aplasia, hypogammaglobulinemia, SLE, Cushing's syndrome, or syndrome of inappropriate secretion of antidiuretic hormone

Mediastinal mass Neoplasms :Thymic Tumors
Thymoma Diagnosis • CT scan and history
• CT : solitary encapsulated mass
• PET (thymic cancer vs thymoma)
• Tissue diagnosis • Surgical resection • FNA sen 87% spec 95% • Cytokeratin (thymoma vs lymphoma)

Mediastinal mass Neoplasms :Thymic Tumors
Thymoma
Mediastinal mass Neoplasms :Thymic Tumors
Thymoma

Mediastinal mass Staging system : Masaoka • Presence or absence of gross or microscopic invasion of the capsule and
surrounding structures, as well as on the presence or absence of metastases
Masaoka Staging System for Thymoma Stage I Encapsulated tumor with no gross or microscopic evidence of capsular
invasion
Stage II Gross capsular invasion or invasion into the mediastinal fat or pleura or microscopic capsular invasion
Stage III Gross invasion into the pericardium, great vessels, or lung
Stage IVA Pleural or pericardial dissemination
Stage IVB Lymphogenous or hematogenous metastasis

Mediastinal mass

Mediastinal mass

Mediastinal mass Treatment • Definitive treatment : complete surgical removal of all resectable
tumors include all of thymus tissue and surrounding fat
• Approach • Median sternotomy with extension to hemiclamshell in more advanced cases
• VATS
• Adjuvant or neoadjuvant therapies : unclear
• Advanced cases : platinum-based chemotherapy and corticosteroids combination with radiotherapy


VATS thymectomy in MG

Mediastinal mass
Mediastinal mass Thymic carcinoma
• Low-grade tumors
• Well differentiated with squamous cell, mucoepidermoid, or basaloid features.
• High-grade thymic carcinomas
• Lymphoepithelial, small cell neuroendocrine, sarcomatoid, clear cell, and undifferentiated or anaplastic features

Mediastinal mass Thymic carcinoma
• Compared with thymomas
• More heterogeneous group of malignancies
• Early local invasion and widespread metastases
• Drop metastasis or pleural metastasis in malignant thymoma
• Complete resection is occasionally curative, but most thymic carcinomas will recur and are refractory to chemotherapy
• Poor prognosis

Mediastinal mass Thymolipoma
• Rare benign tumors that may grow to a very large size before being diagnosed
• Generally well-encapsulated, soft, and pliable masses that do not invade surrounding structures

Mediastinal mass Thymolipoma • Resection is recommended for large masses
Fat density dotted by isolated areas of soft tissue density representing islands of thymic tissue

Mediastinal mass Nerve Sheath Tumors
• 20% of all mediastinal tumors
• More than 95% of nerve sheath tumors
• Benign neurilemomas or neurofibromas
• Malignant neurosarcomas : less common

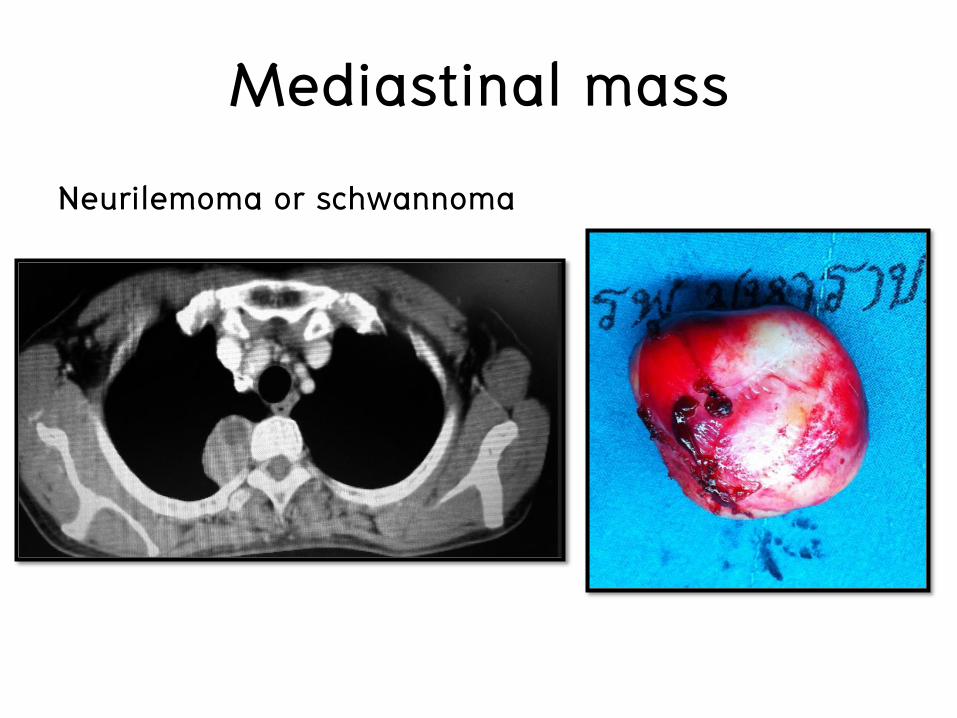
Mediastinal mass Neurilemoma or schwannoma
• Schwann cells in intercostal nerves
• Firm, well encapsulated, and generally benign
• Histologic component
• Antoni type A : compact spindle cells with twisted nuclei and nuclear palisanding
• and Antoni type B : loose and myxoid connective tissue with a haphazard cellular arrangement
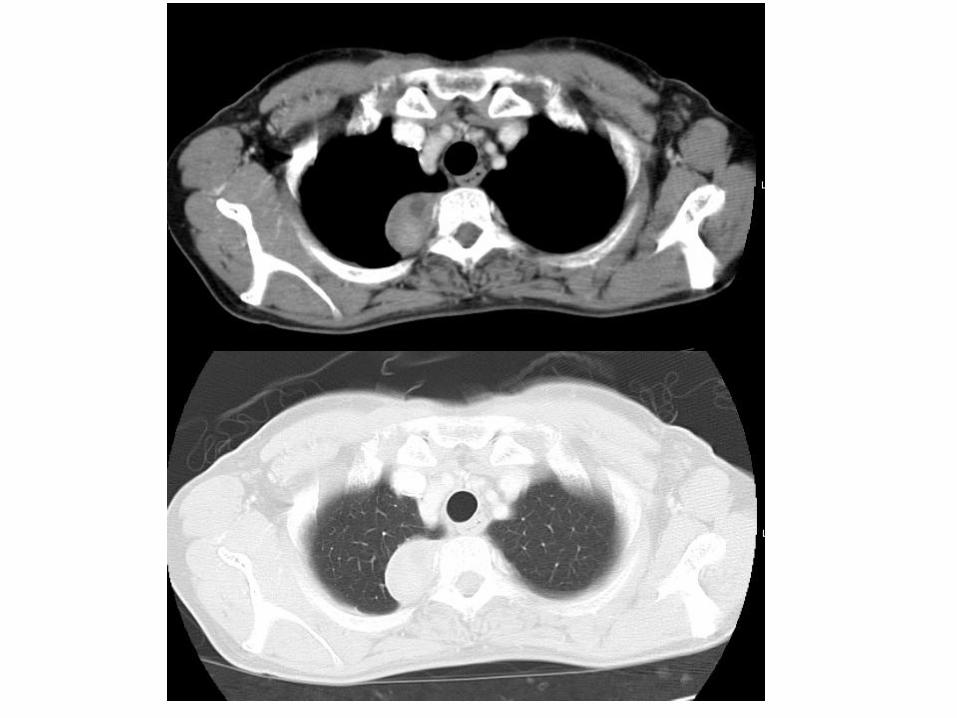
Mediastinal mass Neurilemoma or schwannoma

Mediastinal mass Neurilemoma or schwannoma
Dumbbell configuration (MRI) • Cord compression and paralysis

Mediastinal mass Neurofibroma
• Up to 25 % of nerve sheath tumors
• Component : nerve sheaths and nerve cells
• Up to 40 % of patients with mediastinal fibromas have generalized neurofibromatosis (von Recklinghausen's disease)
• 70 % : benign, 25-30 % : malignancy
• Treatment : complete resection

Mediastinal mass Neurofibroma

Cervicothoracic sign



Mediastinal mass Neurofibrosarcoma
• Risk of malignancy • Advanced age
• Von Recklinghausen’s disease
• Previous exposure to radiation
• Poor prognosis : rapid growth and aggressive local invasion along nerve bundles
• Treatment : complete resection

Mediastinal mass Ganglion Cell Tumors
• Ganglioneuroma
• Ganglioneuroblastoma
• Neuroblastoma
Paraganglionic Tumors
• Chemodectomas
• Pheochromocytomas

Mediastinal mass Lymphomas
• Most common malignancy of the mediastinum
• ~ 50 % of both Hodgkin's and non-Hodgkin's lymphoma, mediastinum is primary site
• Location • Anterior compartment (most commonly involve)
• Middle compartment ( extension to hilar nodes)
• Posterior compartment :rare
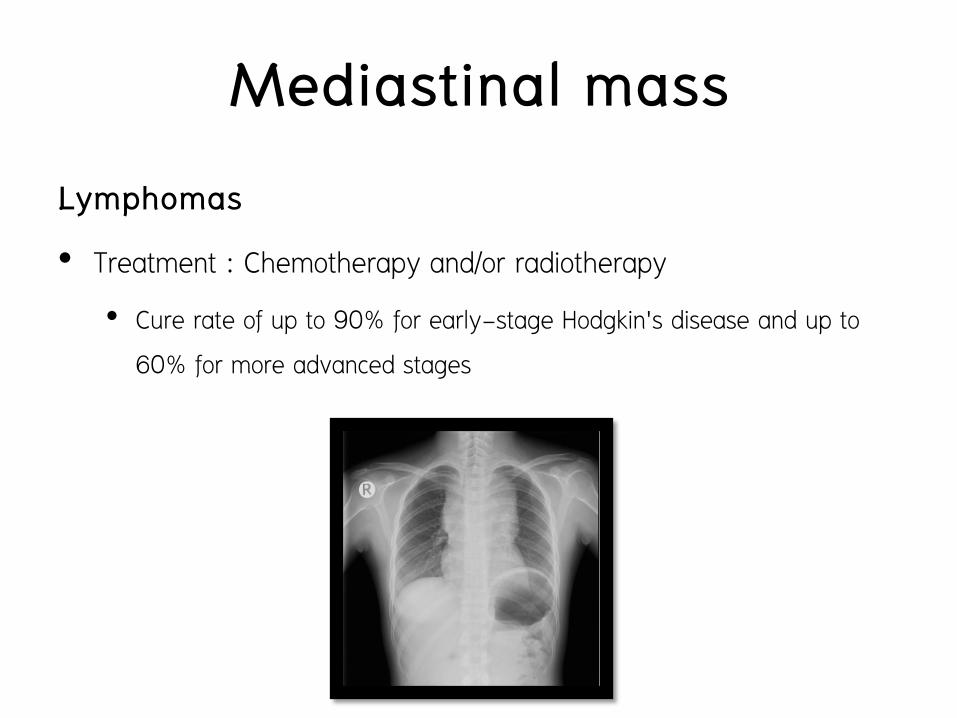
Mediastinal mass Lymphomas
• Treatment : Chemotherapy and/or radiotherapy
• Cure rate of up to 90% for early-stage Hodgkin's disease and up to 60% for more advanced stages

Mediastinal mass Mediastinal Germ Cell Tumors
• Most common malignancy in young men (15-35 yrs)
• Most germ cell tumors are gonadal in origin
• Primary site are rare
• Less than 5 % of all germ cell tumors
• Less than 1 % of all mediastinal tumors

Mediastinal mass Mediastinal Germ Cell Tumors
Seminomas (1/3)
• Advanced disease at time of diagnosis
• Local compressive symptoms • SVC syndrome, dyspnea, or chest discomfort
• Diagnosis • FNA or core-needle biopsy or surgical biopsy (anterior mediastinotomy
(chamerlain procedure) or thoracoscopy)
• Normal level of hCG and AFP
Mediastinal mass Mediastinal Germ Cell Tumors
Seminomas (1/3)
• Treatment • Cisplatin-based chemotherapy regimens with bleomycin and either
etoposide or vinblastine
• More than 75 % : complete response
• Surgery
• Curative for small asymptomatic seminomas
• Resection of residual masses after chemotherapy

Mediastinal mass Mediastinal Germ Cell Tumors
Nonseminomas
• Endodermal sinus tumors
• Embryonal cell carcinomas
• Choriocarcinoma
• Mixed types


Bulky, irregular tumors of the anterior mediastinum with areas of low attenuation on CT scan (necrosis, hemorrhage, or cyst formation)
Mediastinal mass Mediastinal Germ Cell Tumors
Nonseminomas Treatment • Chemotherapy : combination therapy with cisplatin, bleomycin, and
etoposide : Survival is 67% at 2 years and 60% at 5 years • Surgical resection
• Residual masses • up to 20% of residual masses contain additional tumors; in another
40%, mature teratomas; and the remaining 40%, fibrotic tissue

Mediastinal mass Mediastinal Germ Cell Tumors
Teratomas
• Most common type of mediastinal germ cell tumors (60-70%)
• Mature (benign) and immature teratomas (malignant teratomas)
• Containing two or three embryonic layers
• Ectodermal : teeth, skin, hair
• Mesodermal : cartilage and bone
• Endodermal : bronchial, intestinal, or pancreatic tissue

Mediastinal mass Mediastinal Germ Cell Tumors Teratomas • Treatment
• Mature teratoma (benign) : surgical resection , excellent prognosis • Malignant teratomas
• Locally aggression (unresectable) • Poor response to chemotherapy • Limited manner to radiotherapy • Poor prognosis Mature teratomas : benign • CT scan : multilocular cystic tumor, encapsulated with combinations of
fluid, soft tissue, calcium, and/or fat attenuation in the anterior compartment


Mediastinal mass Mediastinal Cysts
Primary Mediastinal Cyst
• Benign cysts account for up to 25% of mediastinal masses
• Most are located in the middle compartment
• CT scan showing characteristic features of near-water density in a typical location is virtually 100% diagnostic

Mediastinal mass Pericardial Cyst • Most common type of mediastinal cysts
• Asymptomatic and detected incidentally
• Contain a clear fluid
• Location : right cardiophrenic angle
• Cyst wall lining is a single layer of mesothelial cells
Mediastinal mass Pericardial Cyst • Treatment
• Observation alone for most simple, asymptomatic pericardial cysts
• Surgical resection or aspiration for complex cysts or large symptomatic cysts

• ภาพ pericardial cyst

Mediastinal mass Bronchogenic cyst
• Abnormality during embryogenesis
• Abnormal budding of the foregut of tracheobronchial tree
• Most occur in mediastinum, 15 % in lung parenchyma
• Location : just posterior to the carina or main stem bronchus


Figure 1. A, Contrast enhanced computed tomographic (CT) scan of the thorax showing a well-defined 7-cm subcarinal mass (curved arrow) of
predominantly fluid attenuation with wall enhancement.
Browne R et al. Circulation. 2002;106:e209-e210
Copyright © American Heart Association, Inc. All rights reserved.

Mediastinal mass Bronchogenic cyst
Pathology
• Thin walled and lined with respiratory epithelium containing with a protein-rich mucoid material and varying amounts of seromucous glands, smooth muscle, and cartilage
• They may communicate with the tracheobronchial tree

Mediastinal mass Bronchogenic cyst Treatment In children : most of these are symptomatic • Large cyst may cause complications
• Airway obstruction • Infection • Rupture • Malignant transformation (rare)
In adults : incidentally asymptomatic found during work-up for an unrelated problem or during screening

Mediastinal mass Bronchogenic cyst
Treatment
In adults : some of these (up to 67%) develop symptoms later
• Chest pain, cough, dyspnea, and fever
• Serious complications : less common
• Hemodynamic compromise, airway obstruction, pulmonary artery obstruction, hemoptysis, and malignant degeneration

Mediastinal mass Bronchogenic cyst
Treatment
• Symptomatic bronchogenic cysts should be removed
• Complete removal of the cyst wall
• Approach
• Posterolateral thoracotomy
• VATS
• Small cysts with minimal adhesions

Enteric Cyst
• Esophageal cysts
• Prone to enlargement >> propensity for serious complications
– Hemorrhage, infection, or perforation
• Resection for both adults and children : regardless of the presence or absence of symptoms
Mediastinal mass

Mediastinal mass Enteric cyst

Thymic Cyst
• Asymptomatic , incidental finding during radiographic work-up for an unrelated problem
• Simple cysts without any consequence
• However, the occasional cystic neoplasm must be ruled out
• Cystic components occasionally are seen in patients with thymoma and Hodgkin's disease
Mediastinal mass


Ectopic Endocrine Glands : Substernal thyroid or intrathoracic goiter
• Thyroid : up to 5% of all mediastinal masses
• 3 types by location of major part of goiter
a) Small substernal extension (> 80%)
b) Partial intrathoracic goiter
c) Complete intrathoracic goiter (rare)
• Non toxic goiter, less than 2 % thyrotoxicosis
Mediastinal mass
Ectopic Endocrine Glands : Substernal thyroid or intrathoracic goiter
• Age > 50 yrs (many in 70-80 yrs)
• Female > male (3-4 times)
• History of previous thyroid operation
Mediastinal mass

Ectopic Endocrine Glands : Substernal thyroid or intrathoracic goiter
S&S
• Asymptomatic , incidental finding
• Cervical mass, dysphagia, dyspnea, stridor, cough or wheezing, and facial flushing
• Serious symptoms : acute tracheal obstruction with severe respiratory compromise after respiratory tract infection
Mediastinal mass
Ectopic Endocrine Glands : Substernal thyroid or intrathoracic goiter
Diagnostic procedure
• CT scan neck and chest
• Radionuclide scintigraphy
Mediastinal mass





Lung cancer Signs and Symptoms
• Asymptomatic • Central lesion symptoms • Peripheral lesion symptoms
Diagnostic procedure • Non-invasive : CT, PET-CT, MRI • Invasive : bronchoscopy biopsy, EBUS, TBNA, Direct lung
tapping, mediastinoscopy, mediastinotomy, VATS
Staging : TNM system Treatment : Surgery, chemotherapy, and radiotherapy
Summary
Mediastinal mass Anatomy of mediastinum
• 3 compartment
• Disease : organ in each compartment • Anterior : thymoma, intrathoracic thyroid, teratory, lymphoma
• Middle : pericardial cyst, bronchogenic cyst
• Posterior : neurogenic tumors
Summary
Mediastinal mass • Diagnostic procedure : CT scan, FNA, CNB, serum marker,
nuclear imaging
• Treatment
• Surgery : thymoma, intrathoracic thyroid, mature teratomy
• Chemotherapy and radiotheorapy : lymphoma , malignant teratoma, seminoma, non-seminoma
Summary

Reference • Schwartz’s Principles of
Surgery, 9th Edition
• General thoracic surgery, Tomas W. Shields, 7thedition
• Staging Manual in Thoracic Oncology
• NCCN guideline 2014