Embed Size (px)
Citation preview
©AP
Cerebellar cysts in children: a pattern-recognition approach
Andrea Poretti 1,2, Thierry A.G.M. Huisman1, Eugen Boltshauser 2
1Section of Pediatric Neuroradiology, Division of Pediatric Radiology, Russell H Morgan Department of Radiology and Radiological Science, The Johns Hopkins University School of Medicine, Baltimore, MD 2Department of Pediatric Neurology, University Children’s Hospital of Zurich, Switzerland
ASNR 53rd Annual Meeting, Chicago, April 25-30, 2015
eEdE-172
©AP
Disclosure• We have nothing to disclose • No relevant financial relations interfering with
our presentation
©AP
Learning objective• To provide an
1. Evaluation approach and
2. Differential diagnosis
of pediatric brain diseases associated with cerebellar cysts
©AP
Cerebellar cysts
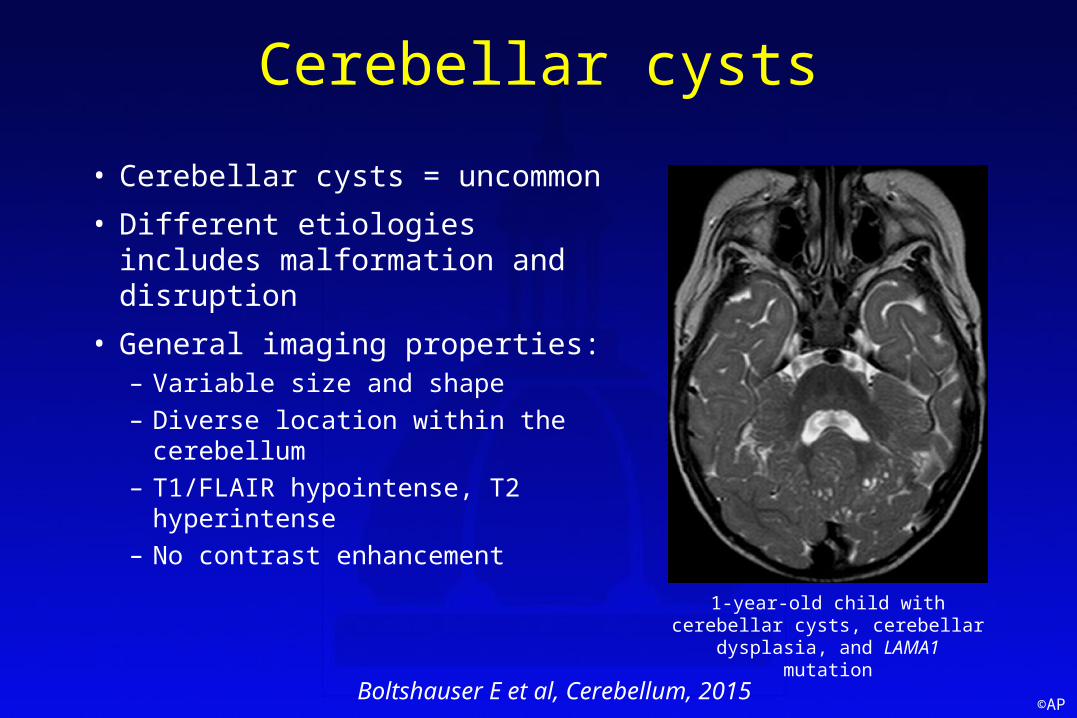
• Cerebellar cysts = uncommon • Different etiologies includes
malformation and disruption• General imaging properties:
– Variable size and shape– Diverse location within the
cerebellum– T1/FLAIR hypointense, T2
hyperintense – No contrast enhancement 1-year-old child with cerebellar cysts,
cerebellar dysplasia, and LAMA1 mutation
Boltshauser E et al, Cerebellum, 2015
©AP
Cerebellar cysts: Diagnostic work-up
• Neuroimaging = key role in the diagnostic work-up• Neuroimaging based pattern-recognition approach
taking into account clinical information facilitates correct diagnosis
• Correct diagnosis essential for optimal therapy, accurate prognosis, and correct genetic counseling
©AP
Purpose• Provision of checklists (based on pathogenesis) and
pattern-recognition approach for pediatric cerebellar cysts • The checklists and pattern-recognition approach should
facilitate correct diagnosis, narrow differential diagnosis, or, if required, help planning of targeted diagnostic work-up
• Cerebellar tumors with a cystic component, parasitic cysts, and postsurgical or posttraumatic cysts were excluded
©AP
Cerebellar cysts: Pathogenesis• Pathogenesis of cerebellar cysts heterogeneous:
1. Normal cystic structures: cystic perivascular spaces in mucopolysaccharidoses
2. Isolated cysts: e.g. neuroglial cysts3. Destructive cysts: pontocerebellar hypoplasia4. Malformative cysts: congenital muscular dystrophies,
Aicardi syndrome, GPR56 mutation, LAMA1 mutation5. Cysts associated with cerebellar dysplasia: Cohen
syndrome, disruptive 6. Various: leukoencephalopathy with calcifications and cysts,
early-onset multiple carboxylase deficiency
Boltshauser E et al, Cerebellum, 2015
©AP
Pattern-recognition approach for cerebellar cysts: What to look for
1. Cyst location: cortical/subcortical, within the white matter, focal, or widespread
2. Cerebellar morphology: areas of cortical dysplasia, hypoplasia3. Brainstem morphology: hypoplastic pons, clefts, tectal
dysplasia, and kinking4. Supratentorial abnormalities: migration anomalies, white
matter changes, cysts within the white matter, hydrocephalus5. Clinics: muscle involvement, ataxia, ocular motor apraxia,
intellectual disability, and ophthalmological abnormalities
©AP
1. Cysts involving normal structures• Cystic dilatation of cerebellar perivascular spaces (PVS) in
mucopolysaccharidoses:– Particularly types 1 and 2, also seen in type 3 Sanfilippo– Location: hilus of the dentate nucleus and the surrounding cerebellar
white matter– Typical constellation: cystic PVS dilatations in the region of the
dentate nucleus/cerebellar white matter in an otherwise normal cerebellum
– Diagnosis not problematic considering the overall clinical and neuroimaging aspects (PVS dilatation, white matter changes, ventriculomegaly, cortical atrophy)
Alqahtani E et al, Eur J Paediatr Neurol, 2014
©AP
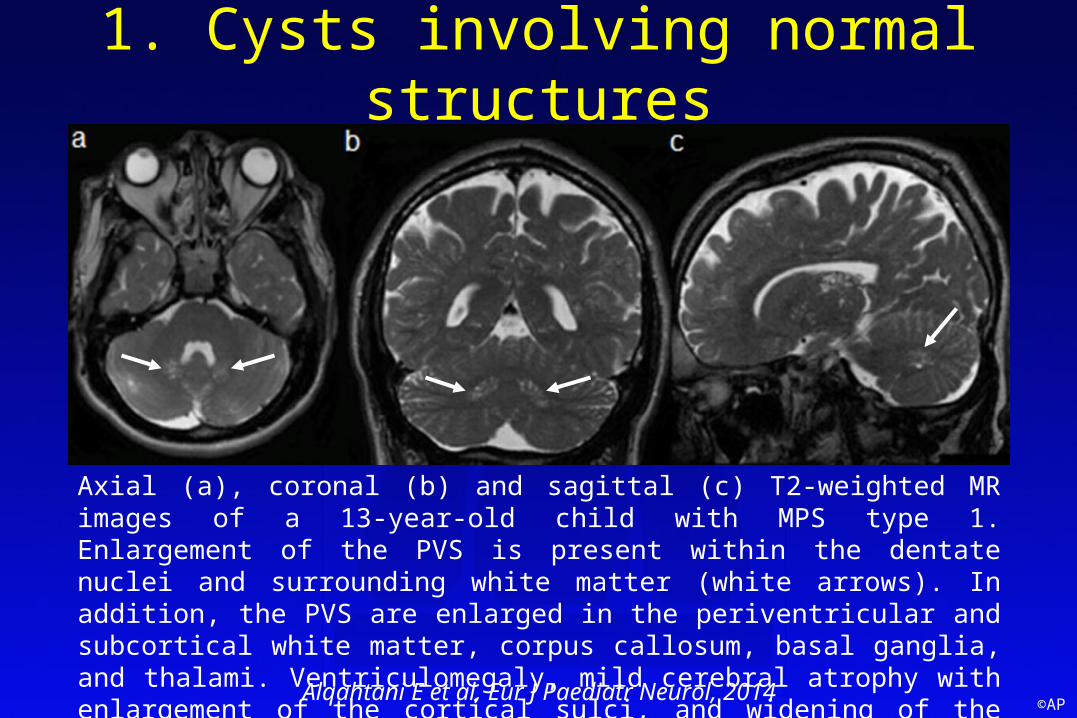
1. Cysts involving normal structures
Axial (a), coronal (b) and sagittal (c) T2-weighted MR images of a 13-year-old child with MPS type 1. Enlargement of the PVS is present within the dentate nuclei and surrounding white matter (white arrows). In addition, the PVS are enlarged in the periventricular and subcortical white matter, corpus callosum, basal ganglia, and thalami. Ventriculomegaly, mild cerebral atrophy with enlargement of the cortical sulci, and widening of the diploic space are also seen.
Alqahtani E et al, Eur J Paediatr Neurol, 2014
©AP
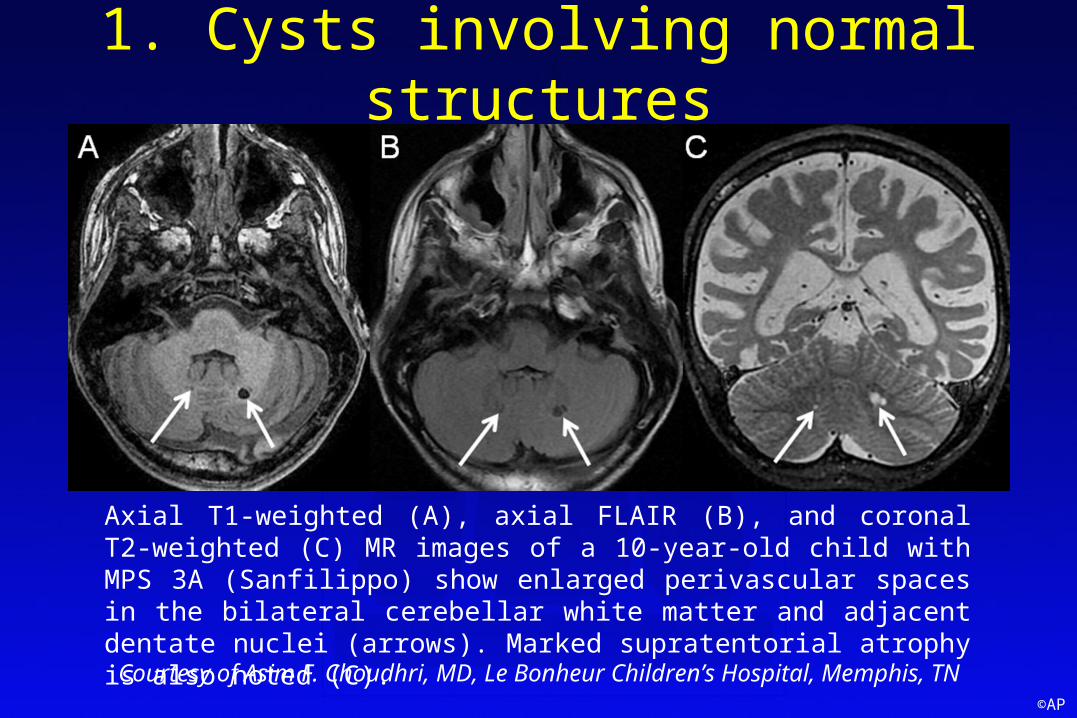
1. Cysts involving normal structures
Axial T1-weighted (A), axial FLAIR (B), and coronal T2-weighted (C) MR images of a 10-year-old child with MPS 3A (Sanfilippo) show enlarged perivascular spaces in the bilateral cerebellar white matter and adjacent dentate nuclei (arrows). Marked supratentorial atrophy is also noted (C).
Courtesy of Asim F. Choudhri, MD, Le Bonheur Children’s Hospital, Memphis, TN
©AP
2. Isolated cysts• Neuroepithelial cysts:
– Benign fluid-containing smooth, round, or ovoid cavities that occur throughout the entire neuraxis (most are supratentorial)
– No calcifications or hemorrhage– Rarely space-occupying in the posterior fossa– Typical constellation: mostly single cyst in the white
matter, usually an incidental finding in a normal cerebellum
©AP
3. Destructive cerebellar cysts• Pontocerebellar hypoplasia:
– Low prevalence, mostly type 2, but also reported in type 1 and 6
– Location: lateral aspects of the hemispheres– Size: large– Pathology: reactive astrocytes and macrophages at
the border of the cysts destructive process– Typical constellation: few cysts in the lateral aspects
of the cerebellar hemispheres in a severely abnormal cerebellum, dominated by atrophy (hemispheres >> vermis), and pontine hypoplasia
Barth PG et al, Acta Neuropathol, 2007
©AP
3. Destructive cerebellar cysts
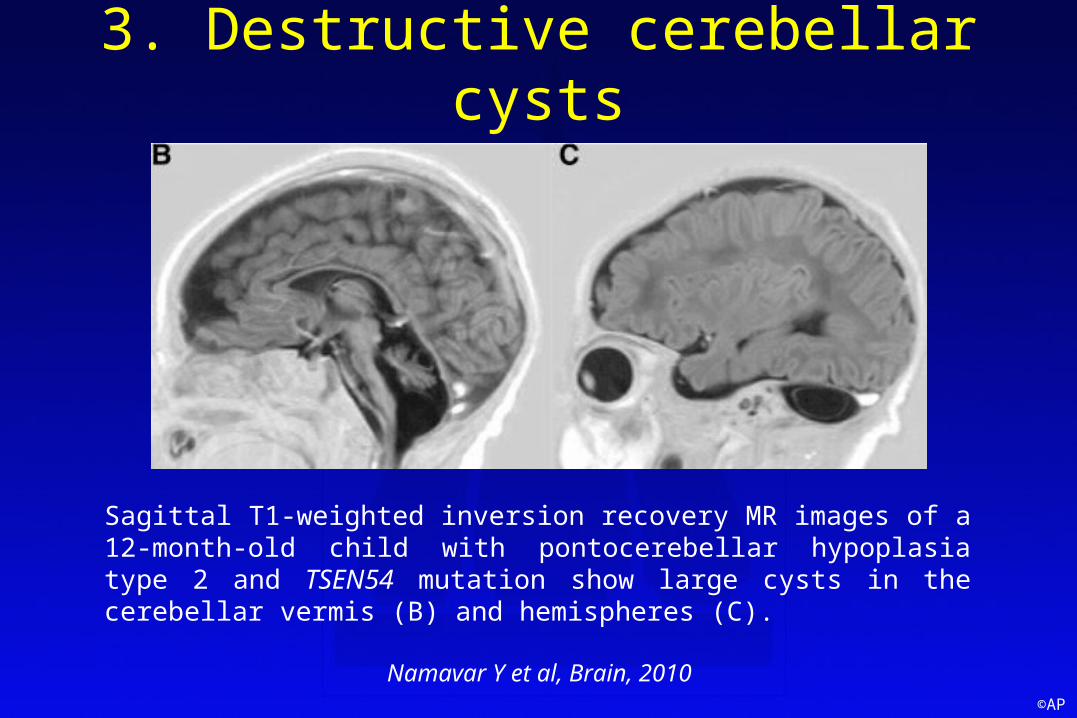
Sagittal T1-weighted inversion recovery MR images of a 12-month-old child with pontocerebellar hypoplasia type 2 and TSEN54 mutation show large cysts in the cerebellar vermis (B) and hemispheres (C).
Namavar Y et al, Brain, 2010
©AP
3. Destructive cerebellar cysts
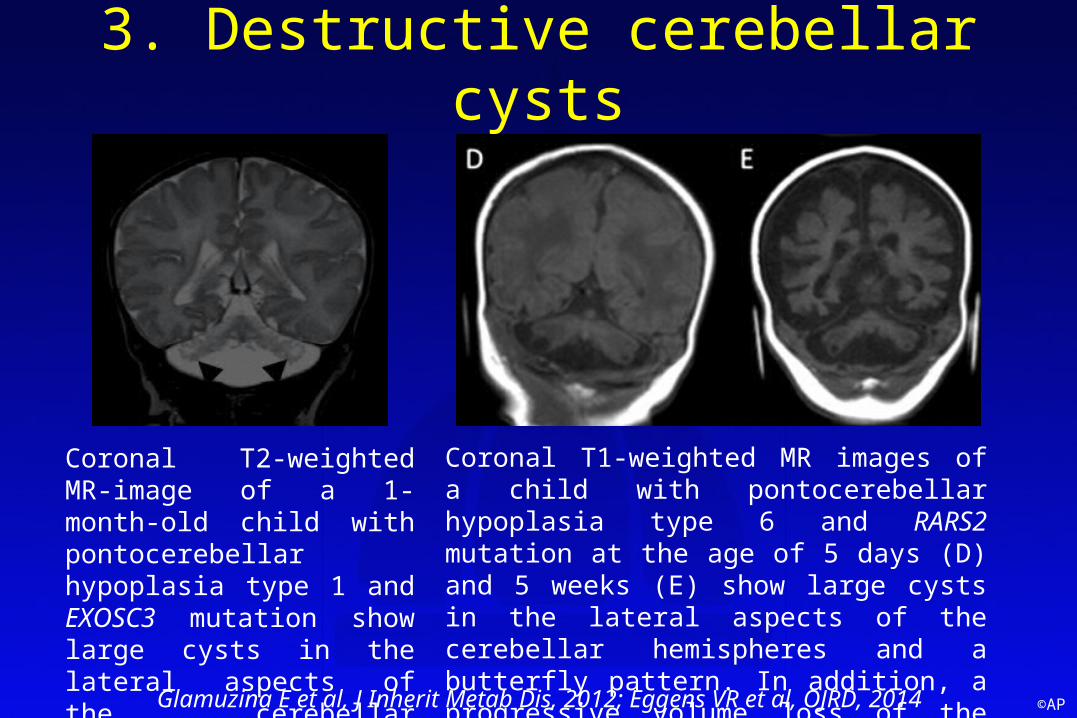
Coronal T2-weighted MR-image of a 1-month-old child with pontocerebellar hypoplasia type 1 and EXOSC3 mutation show large cysts in the lateral aspects of the cerebellar hemispheres.
Coronal T1-weighted MR images of a child with pontocerebellar hypoplasia type 6 and RARS2 mutation at the age of 5 days (D) and 5 weeks (E) show large cysts in the lateral aspects of the cerebellar hemispheres and a butterfly pattern. In addition, a progressive volume loss of the cerebellum and cerebrum is noted over time.
Glamuzina E et al, J Inherit Metab Dis, 2012; Eggens VR et al, OJRD, 2014
©AP
4. Malformative cysts• Congenital muscular dystrophies (CMD):
– Mostly seen in α-dystroglycanopathies, but rare in LAMA2 mutations (merosin-negative CMD)
– α-dystroglycanopathies:• Clinically heterogeneous including Walker-Warburg syndrome,
(WWS), muscle-eye-brain disease (MEB), and Fukuyama CMD • Genetically heterogenous: associated with 17 genes• Characterized by:
– Muscle weakness, hypotonia, contractures– Brain malformations such as cobblestone brain, cerebellar and
brainstem anomalies impaired cognitive and motor development, seizures
– Eye involvement such as retinal dysplasia and microophthalmia
©AP
4. Malformative cysts• Cerebellar cysts in α-dystroglycanopathies:
– Location: cortical/subcortical in vermis (anterior/superior part) and hemispheres (posterior/superior part)
– Associated with cerebellar dysplasia– Typically not seen on fetal and neonatal images, but
only on follow-up studies– Pathology: formed from the subarachnoid spaces
engulfed by the dysplastic cerebellar folia– Phenotype: mostly in MEB and Fukuyama CMD, rare
in WWS
©AP
4. Malformative cysts• Cerebellar cysts in α-dystroglycanopathies:
– Genetics: mostly associated with mutations in FKTN, FKRP, POMGnT1, LARGE, ISPD, TMEM5, GMPPB, POMT1, POMT2
– Typical constellation: cerebellar cysts with a cortical/ subcortical predilection in a hypoplastic and dysplastic cerebellum, often accompanied by brainstem anomalies (pontine hypoplasia and clefts), in various combinations with supratentorial abnormalities (migration abnormalities, white matter signal changes, ventriculomegaly)
©AP
4. Malformative cystsA B C D
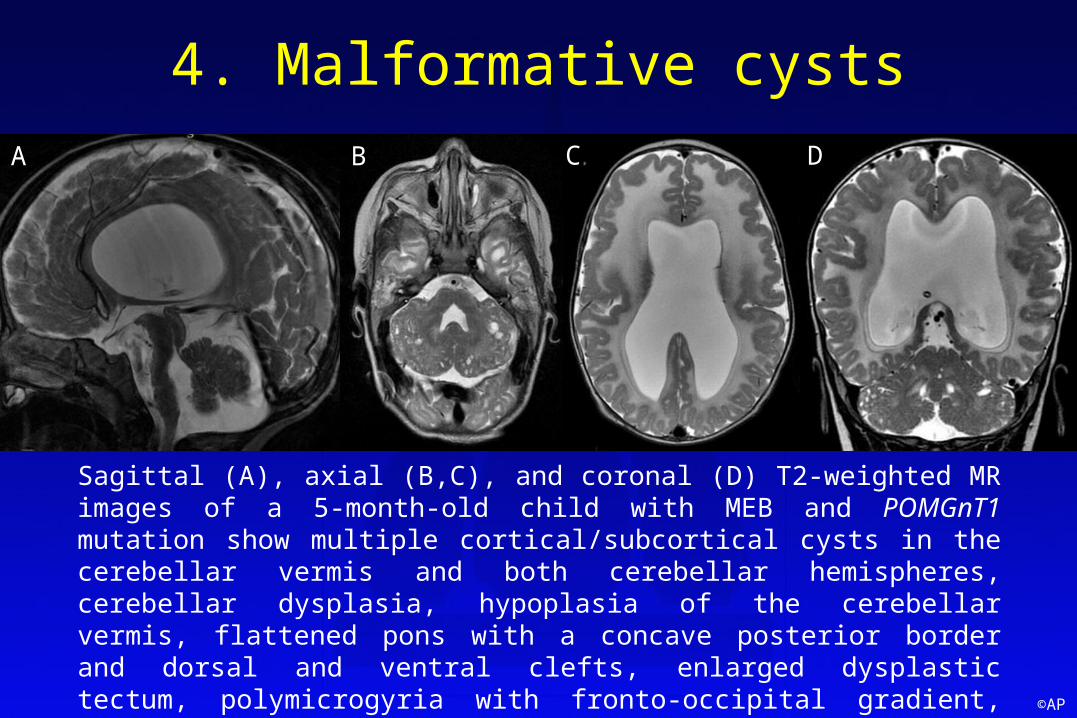
Sagittal (A), axial (B,C), and coronal (D) T2-weighted MR images of a 5-month-old child with MEB and POMGnT1 mutation show multiple cortical/subcortical cysts in the cerebellar vermis and both cerebellar hemispheres, cerebellar dysplasia, hypoplasia of the cerebellar vermis, flattened pons with a concave posterior border and dorsal and ventral clefts, enlarged dysplastic tectum, polymicrogyria with fronto-occipital gradient, thin corpus callosum, diffusely abnormal high signal intensity of the white matter, and ventriculomegaly.
©AP
4. Malformative cysts• Aicardi syndrome (OMIM 304050):
– “Classical” triad of infantile spasms, corpus callosum dysgenesis, and chorioretinal lacunae
– Additional imaging findings: interhemispheric cysts, polymicrogyria, subependymal and cortical heterotopias, tectal dysplasia, inferior vermis hypoplasia, and dysplastic or hypoplastic cerebellar hemispheres
– Cerebellar cysts in about 20% of patients– Typical constellation: female infant with infantile spasms,
retinal abnormalities, and combination of supratentorial (callosal dysgenesis) and infratentorial abnormalities
Hopkins B et al, Am J Med Genet A, 2008
©AP
4. Malformative cysts
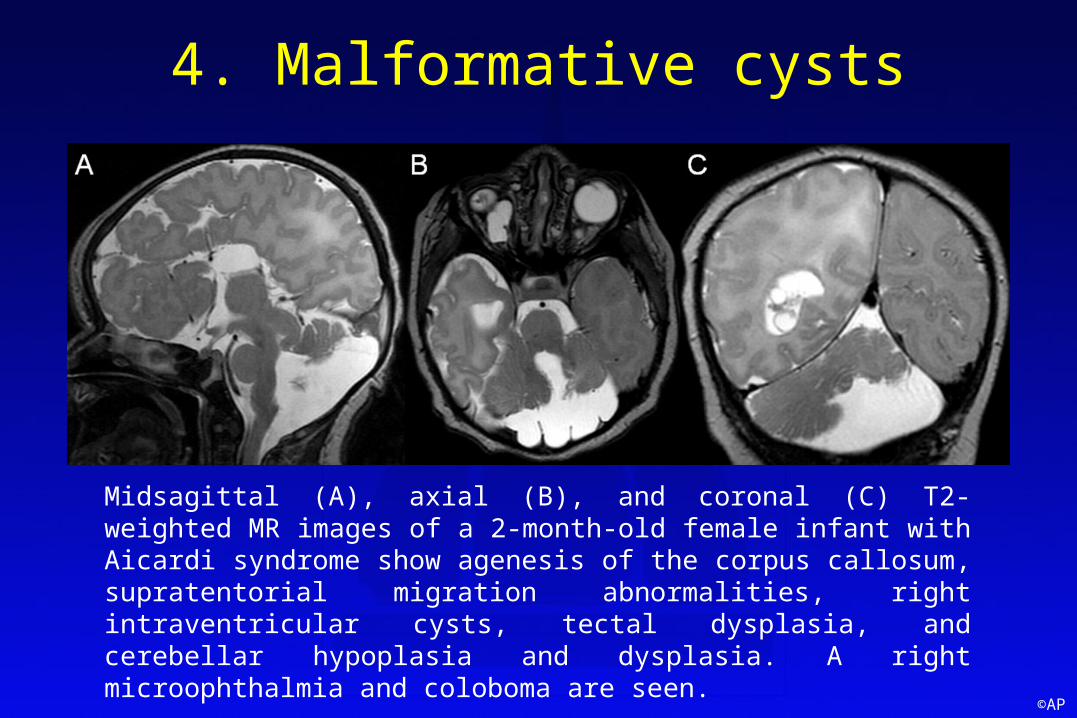
Midsagittal (A), axial (B), and coronal (C) T2-weighted MR images of a 2-month-old female infant with Aicardi syndrome show agenesis of the corpus callosum, supratentorial migration abnormalities, right intraventricular cysts, tectal dysplasia, and cerebellar hypoplasia and dysplasia. A right microophthalmia and coloboma are seen.
©AP
4. Malformative cysts• Mutations in GPR56 (OMIM 615752):
– Clinic: motor and cognitive delay, seizures, ataxia, nystagmus– Neuroimaging: generalized (antero-posterior gradient) or
fronto-parietal polymicrogyria, patchy or diffuse white matter changes, cerebellar dysplasia
– Cerebellar cysts: common, subpial and cortical location in the vermis and cerebellar hemispheres
– Typical constellation: multiple cysts associated with cerebellar dysplasia, abnormalities of the supratentorial white matter, and cortical architecture in a child with seizures and intellectual disability
Bahi-Buisson N, Brain, 2010
©AP
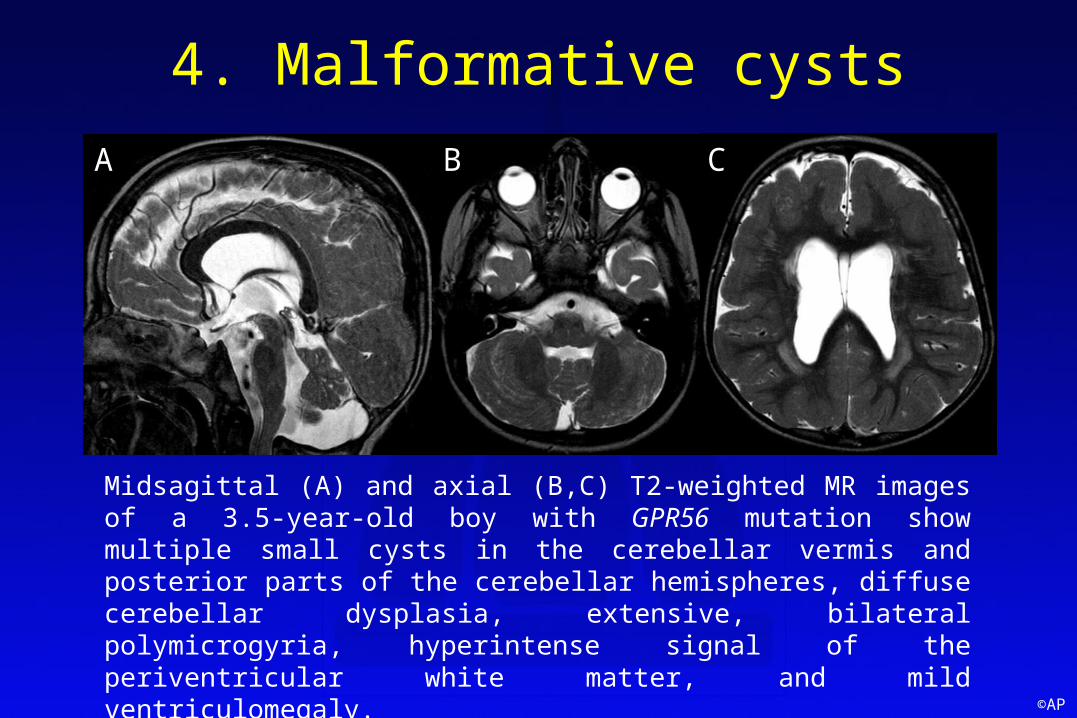
4. Malformative cysts
Midsagittal (A) and axial (B,C) T2-weighted MR images of a 3.5-year-old boy with GPR56 mutation show multiple small cysts in the cerebellar vermis and posterior parts of the cerebellar hemispheres, diffuse cerebellar dysplasia, extensive, bilateral polymicrogyria, hyperintense signal of the periventricular white matter, and mild ventriculomegaly.
A B C
©AP
4. Malformative cysts
• Mutations in LAMA1 (OMIM 615960):– Clinic: ataxia, intellectually disability, ocular motor apraxia,
severe myopia (inconsistent), retinal abnormalities (inconsistent)– Neuroimaging: cerebellar dysplasia, vermis hypoplasia, abnormal
shape of the fourth ventricle– Cerebellar cysts: common, cortical/subcortical in the vermis
(anterior/superior part) and cerebellar hemispheres (posterior/superior part)
– Typical constellation: multiple cortical/subcortical cysts in the vermis and hemispheres with cerebellar dysplasia, vermis hypoplasia, and no supratentorial abnormalities
Aldinger KA, Am J Hum Genet, 2014; Poretti A et al, Cerebellum, 2014
©AP
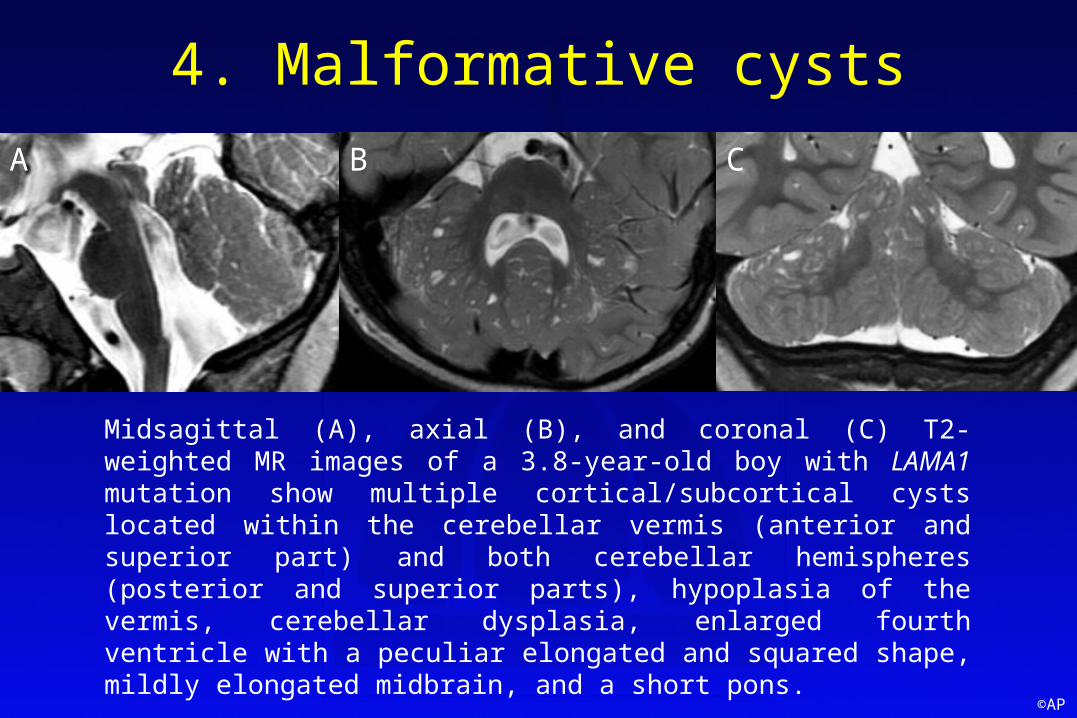
4. Malformative cysts
Midsagittal (A), axial (B), and coronal (C) T2-weighted MR images of a 3.8-year-old boy with LAMA1 mutation show multiple cortical/subcortical cysts located within the cerebellar vermis (anterior and superior part) and both cerebellar hemispheres (posterior and superior parts), hypoplasia of the vermis, cerebellar dysplasia, enlarged fourth ventricle with a peculiar elongated and squared shape, mildly elongated midbrain, and a short pons.
A B C
©AP
5. Cerebellar cysts in cerebellar dysplasia• Cerebellar dysplasia = deranged development of
the cerebellar tissue resulting in abnormal cerebellar foliation, fissuration, and white matter arborization
• Etiology = heterogeneous (genetic and acquired causes), unknown in the majority of patients
• Typical constellation: cerebellar dysplasia is the dominant feature; cysts: cortical/subcortical, confined to dysplastic areas, most likely in the upper vermis and hemispheres, diffuse or focal
©AP
5. Cerebellar cysts in cerebellar dysplasia• Cohen syndrome (OMIM 216550):
– Clinic: non-progressive mental retardation, microcephaly, hypotonia, and characteristic facial features (high-arched eyelids, short philtrum, thick hair, and low hairline)
– Neuroimaging: large corpus callosum, cerebellar hypoplasia, cerebellar dysplasia (exceptional)
– Genetic: mutations in VPS13B– Cerebellar cysts: exceptional, cortical/subcortical within
the vermis and cerebellar hemispheres
Kivitie-Kallio S et al, Neuropediatrics, 1998
©AP
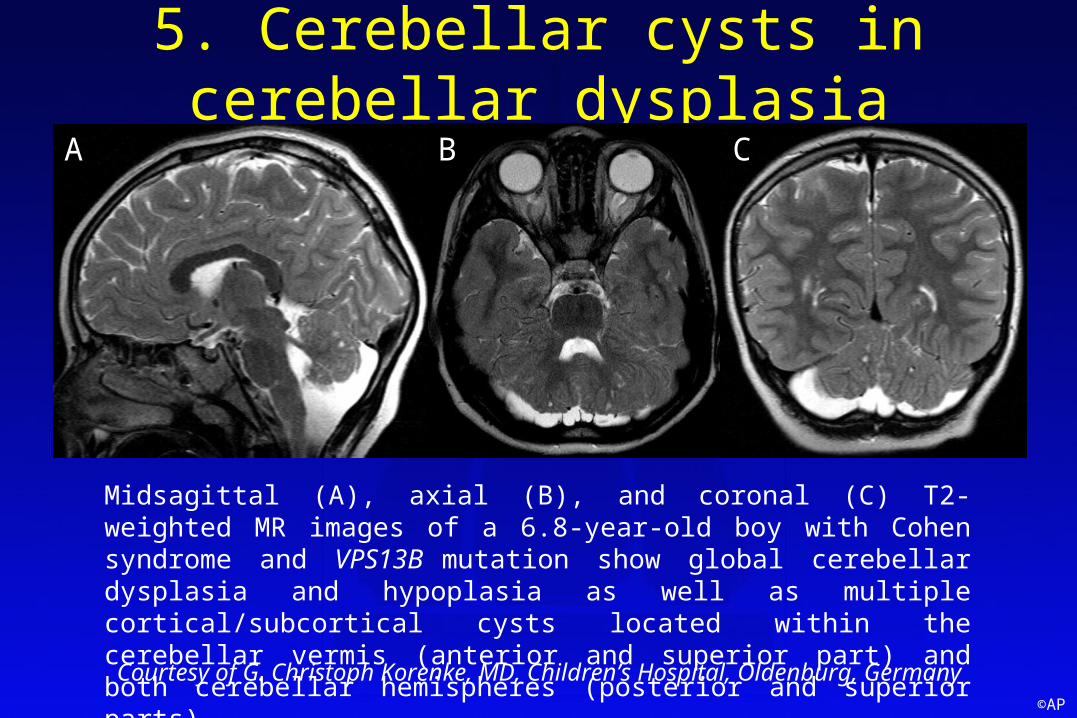
5. Cerebellar cysts in cerebellar dysplasia
Midsagittal (A), axial (B), and coronal (C) T2-weighted MR images of a 6.8-year-old boy with Cohen syndrome and VPS13B mutation show global cerebellar dysplasia and hypoplasia as well as multiple cortical/subcortical cysts located within the cerebellar vermis (anterior and superior part) and both cerebellar hemispheres (posterior and superior parts).
A B C
Courtesy of G. Christoph Korenke, MD, Children’s Hospital, Oldenburg, Germany
©AP
5. Cerebellar cysts in cerebellar dysplasia• Bilateral cerebellar dysplasia with cysts:
– Clinic: variable, including developmental delay or non-progressive ataxia
– Neuroimaging: bilateral cerebellar dysplasia and cysts– Etiology: unknown, most likely malformative– Cerebellar cysts: multiple, cortical/subcortical within
the vermis and cerebellar hemispheres
©AP
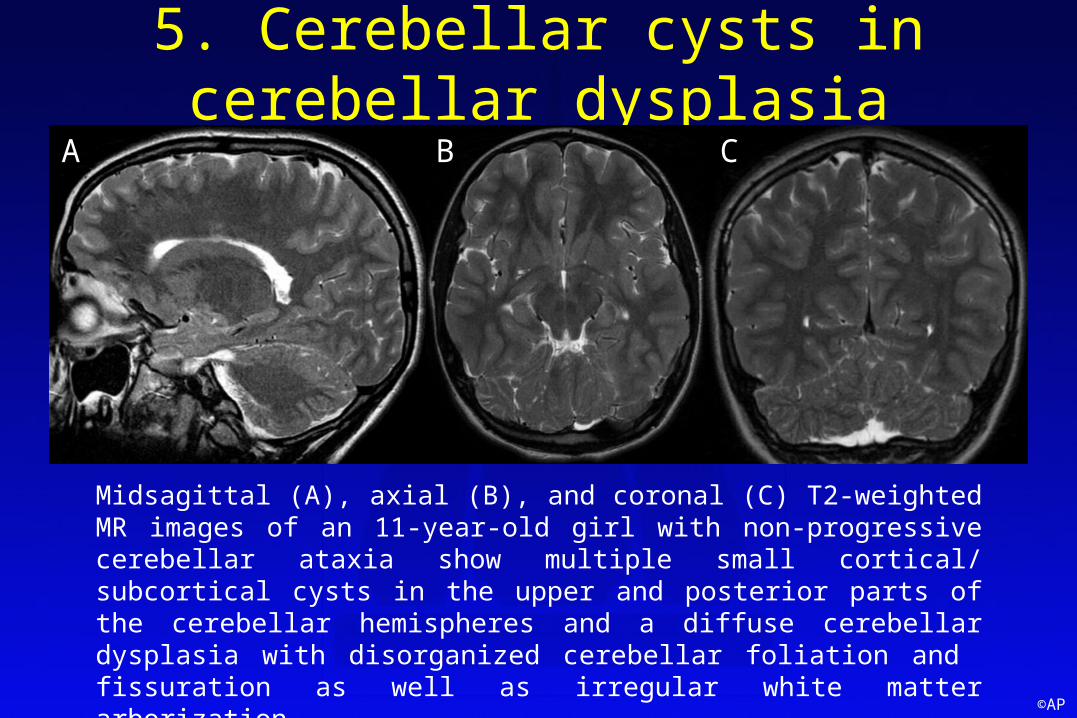
5. Cerebellar cysts in cerebellar dysplasia
Midsagittal (A), axial (B), and coronal (C) T2-weighted MR images of an 11-year-old girl with non-progressive cerebellar ataxia show multiple small cortical/ subcortical cysts in the upper and posterior parts of the cerebellar hemispheres and a diffuse cerebellar dysplasia with disorganized cerebellar foliation and fissuration as well as irregular white matter arborization.
A B C
©AP
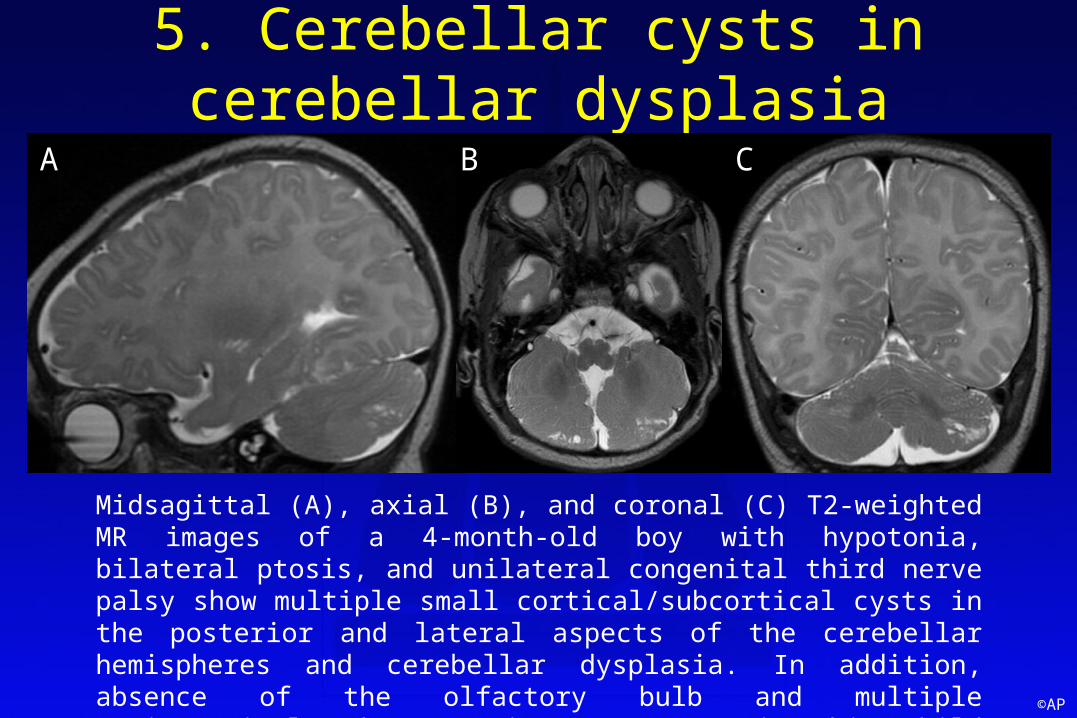
5. Cerebellar cysts in cerebellar dysplasia
Midsagittal (A), axial (B), and coronal (C) T2-weighted MR images of a 4-month-old boy with hypotonia, bilateral ptosis, and unilateral congenital third nerve palsy show multiple small cortical/subcortical cysts in the posterior and lateral aspects of the cerebellar hemispheres and cerebellar dysplasia. In addition, absence of the olfactory bulb and multiple periventricular heterotopias were seen in this child (not shown).
A B C
©AP
5. Cerebellar cysts in cerebellar dysplasia• Unilateral cerebellar dysplasia with cysts:
– Clinics: variable, including developmental delay or non-progressive ataxia; imaging findings may be “incidental”
– Neuroimaging: unilateral cerebellar dysplasia and cysts in a cerebellar hemisphere of reduced volume
– Etiology: unknown, most likely disruptive in view of the “focal” nature of the anomalies
– Cerebellar cysts: cortical/subcortical within a small cerebellar hemisphere with focal dysplasia
©AP
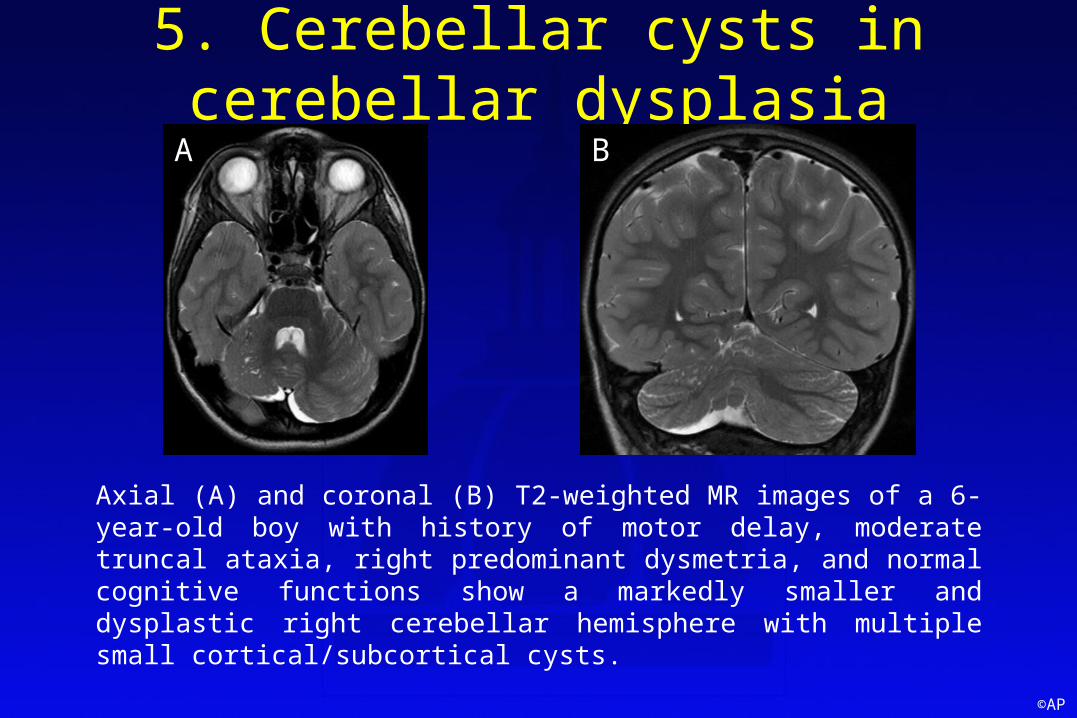
5. Cerebellar cysts in cerebellar dysplasia
Axial (A) and coronal (B) T2-weighted MR images of a 6-year-old boy with history of motor delay, moderate truncal ataxia, right predominant dysmetria, and normal cognitive functions show a markedly smaller and dysplastic right cerebellar hemisphere with multiple small cortical/subcortical cysts.
A B
©AP
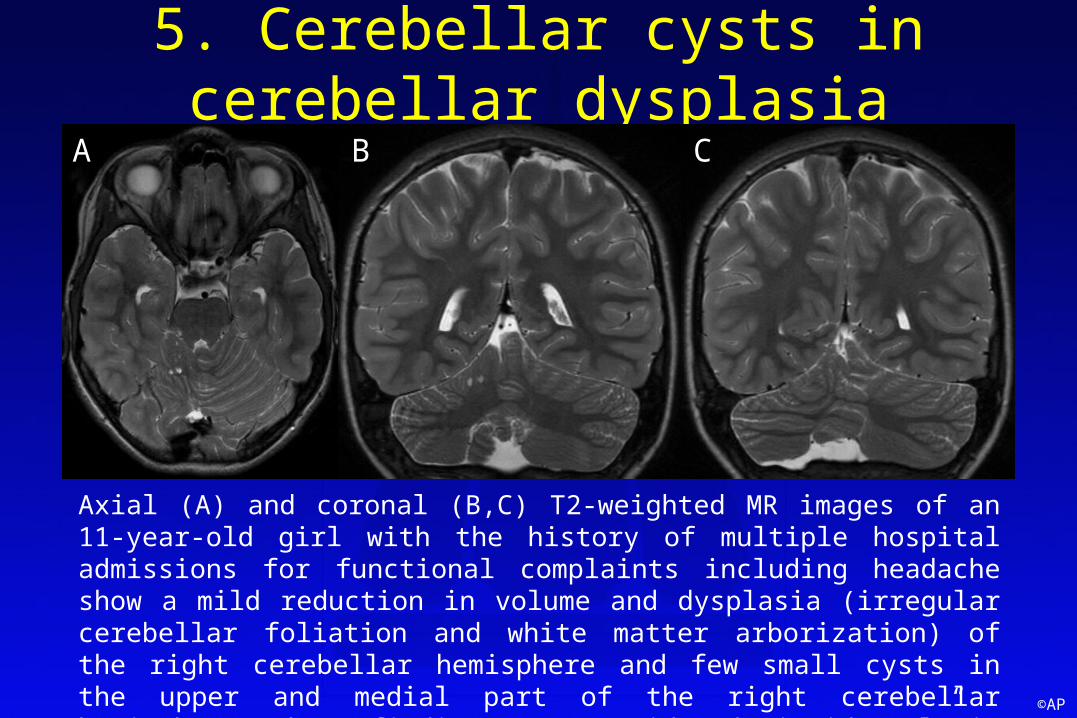
5. Cerebellar cysts in cerebellar dysplasia
Axial (A) and coronal (B,C) T2-weighted MR images of an 11-year-old girl with the history of multiple hospital admissions for functional complaints including headache show a mild reduction in volume and dysplasia (irregular cerebellar foliation and white matter arborization) of the right cerebellar hemisphere and few small cysts in the upper and medial part of the right cerebellar hemisphere. These findings are considered “incidental” in view of the clinical presentation.
A B C
©AP
6. Others• Leukoencephalopathy with
calcifications and cysts (OMIM 614561):– Clinic: spasticity, dystonia,
seizures, and cognitive decline – Neuroimaging: white matter
changes, intracranial calcifications, and enlarging brain cysts
– Cerebellar cysts: uncommon, postcontrast enhancement of the cyst wall
• Early-onset multiple carboxylase deficiency (OMIM 253270):– Disorder of biotin metabolism– Clinic: lactic acidosis, alopecia,
keratoconjunctivitis, perioral erosions, and seizures
– Neuroimaging: cerebral atrophy, ventriculomegaly
– Cerebellar cysts: exceptional
Livingston JH et al, Neuropediatrics, 2014 Tsutsumi Y et al, Ultrasound Obstet Gynecol, 2010
©AP
Take-home messages
1. Cerebellar cysts rare finding with different pathomechanisms
2. Correct diagnosis essential for optimal therapy, accurate prognosis, and genetic counseling
3. Neuroimaging key role in the diagnostic work-up
4. Imaging based pattern-recognition approach taking into account clinical information very helpful for correct diagnosis














![SCYCLE OPERATING UNIT POM, WEEE Generated & Flows in various EU Countries Tallinn, October 1, 2015 Jaco Huisman – Huisman [at] unu.edu](https://img.pdfslide.us/doc/110x75/5697bf8c1a28abf838c8bf7e/scycle-operating-unit-pom-weee-generated-flows-in-various-eu-countries-tallinn.jpg)