Embed Size (px)
Citation preview
ORIGINAL RESEARCH
ANTIOXIDANTS AND OTHER NUTRIENTSDO NOT INTEREERE WITH CHEMOTHERAPY ORRADIATION THERAPY AND CAN INCREASE KILE
AND INCREASE SURVIVAE, PART 1Charles B. Simone II, Ml); Nicole L. Simone, .MD; Victoria Simoiu-, KN: Chark'S B. Siiiione, MD
Purpose • Some in the oncology community contend thatpatients undergoing chemotherapy and/or radiation therapyshould not use food supplement antio.xidant.s and other nutri-ents. Oncologists at an influential oncolog}' institution contend-ed that antioxidants interfere with radiation and somechemotherapies because those modalities kill by generating freeradicals that are neutralized by antioxidants, and that folic acidinterferes with methotrexate. This is de.spite the common use ofamifbstine and dexrazoxane. 2 prescription antioxidants, duringchemotherapy and/or radiation therapy.Design • To assess all evidence concerning antioxidant andother nutrients used concomitantly with chemotherapy and/orradiation therapy, the MEDLINE® and CANCERLIT® databaseswere searched from 1965 to November 2003 using the words vit-amins. antioxidants, ebemotherapy, and radiation therapy.Bibliographies of articles were searched. All studies reportingconcomitant nutrient use with chemotherapy and/or radiation
therapy (280 peer-reviewed articles including 62 in vitro and 218in vivo) were indiscriminately included.
Results • Fifty human clinical randomized or observationaltrials have been conducted, involving 8,521 patients usingbeta-carotene: vitamins A, C, and E: selenium; cysteine: B vita-mins: vitamin D.,: vitamin K3: and glutathione as single agentsor in combination.
Conclusions • Since the 1970s, 280 peer-reviewed in vitro and invivo studies, including 50 human studies involving 8,521patients, 5,081 of whom were given nutrients, have consistentlyshown tiiat non-prescription antioxidants and other nutrientsdo not interfere with therapeutic modalities for cancer.Furthermore, they enhance the killing of therapeutic modalitiesfor cancer, decrease their side effects, and protect normal lissue.In 15 human studies, 3,738 patients wbo took non-prescriptionantioxidants and other nutrients actually had increased survival.{Altern Ther Health Med. 2007:13(l):22-28.)
Charles B. Simone II, \m, and Nicole L. Simone, MD, areconsulting physicians, Victoria Simone, RN, is a researchnurse, and Charles B. Simone, MD, is a consulting physicianand medical director, all at the Simone Protective CancerInstitute in Lawrencevilk', NJ.
Editor's mUe: The following is part I oja 2-part article. Part 2
will appear in the March/April 2007 issue D/ Alternative "Hierapies
in Health and Medicine.
Two of every 5 Americans will develop cancer, and theincidence of most cancers has increased annuallysince 1930.'' In addition, since 1930, despite the useof radiation therapy, chemotherapy, immunothera-py, and improved surgical and diagnostic tech-
niques, there has been limited improvement in cancer survival
rates for most adult cancers.'' Chemotherapy and radiation ther-apy, however, continue to have a large role in cancer treatmentbut produce great morbidity. Two prescription medicines, ami-fostine and dexrazoxane, both antioxidants, reduce cancer thera-py side effects without interfering with antitumor killing.Amifo.stine {VVR-2721) is an antioxidant analog of cysteaminethat was discovered by the armed forces at Walter Reed ArmyMedical Center, Washington. DC, and became the first antioxi-dant agent to be approved by international regulatory agencies."According to 29 studies, amifbstine reduces side effects andincreases response rates of chemotherapy and radiation therapywithout interfering with their antitumor killing activity.""Twenty-one studies indicate that dexrazoxane (ICRF-I87) pro-tects the heart from adriamycin toxicity without interfering withthe antitumor effect'"" by chelating iron that would otherwiseform free radicals.-'-"
Despite the common use of amifostine and dexrazoxane, andin direct opposition to clear scientific findings since the 1970s,
22 ALTERNATIVt THFRAPIES. lAN/FLB 2007. VOL 13, NO. I Ann,ui<hntsand()tl,er\iitrienlsWi
many patients have been told not to use food supplement antioxi-dants and other nutrients wbile undergoing chemotherapy and/orradiation therapy because there is an erroneous but seemingly log-ical belief that antioxidants interfere with radiation and somechemotherapies because those modalities kill hy generating freeradicals tbat are neutralized by antioxidants, and another erro-neous belief that folic acid interferes with methotrexate.^''^
In an article that appeared on the front page of The NewYork Times on October 26, 1997, Larry Norton, Ml), of MemorialSloan Kettering Cancer Center, New York, was quoted as saying."Researcb at [Memorial Sloan Kettering] showed that largedoses of vitamin C could blunt the beneficial etTects ofebemotherapy for breast cancer. . . . It is also known that folicacid can negate the effects of methotrexate, a drug used to treatcancer."'" The researcb referred to was finally published almost 2years later and demonstrated only the mechanism by which can-cer cells obtain vitamin C and that more vitamin C was found inmice cancer cells compared to normal mice cells."" However, thesenior author of tbat paper stated in a news release on the day ofpublication (September 15, 1999), "It's possible that taking largeamounts of vitamin C could Interfere witb the effects ofchemotherapy or even radiation therapy."'" So a single interviewin The New York Times in 1997 that was not based on publishedscientific work and a single research paper involving mice, alongwith a press release by its author in 1999, led lo the erroneousnotion that vitamin C interferes with chemotherapy and radia-tion in humans. Tbis notion soon applied to al! antioxidants asphysicians, patients, the media, the American Cancer Society," "and scores of websites took the same position without reviewingthe scientific evidence.
This 2-part article presents the scientific data that antioxi-dants do not interfere with chemotherapy and/or radiation thera-py. Furthermore, it is not folic acid that interferes with the actionof methotre.xate, but rather folinic acid, a prescripiion drug that isneither a vitamin nor an antioxidant.'"' This article reviews dataabout vitamin A, beta-carotene, and vitamin E. Part 2 will reviewdata about antioxidant combinations, K vitamins, vitamins D^and K , and the glutathione-selenium complex.
METHODSMEDLINE® and CANCERLIT® searches were done using
key words: vitamins, antioxidants, chemotherapy, and radiationtherapy. All studies reporting food supplement nutrients usedconcomitantly with chemotherapy and/or radiation therapywere indiscriminately included; however, in cases in which anauthor had published bis or her findings in multiple sources,only the most recently published paper was used as it usuallycontained the greatest number of patients.
BACKGROUNDRadiation and certain chemotherapies produce cellular kill by
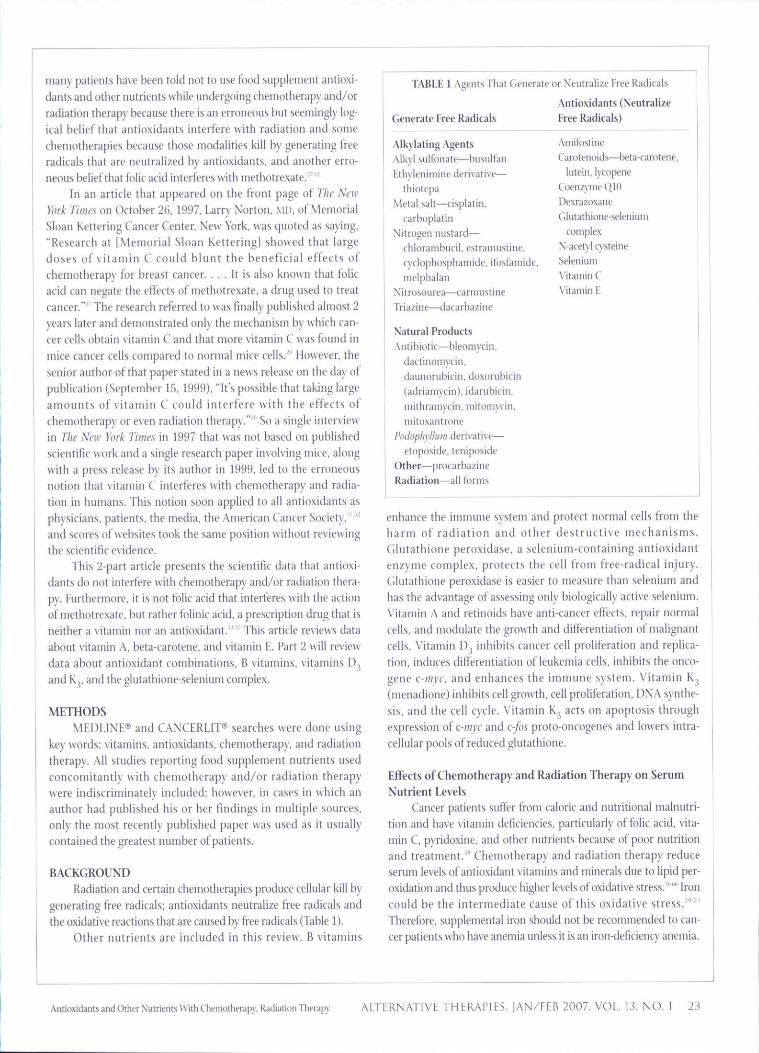
generating free radicals; antioxidants neutrahze free radicals andthe oxidative reactions that are caused by free radicals (Table 1).
Other nutrients are included in this review. B vitamins
TABLE 1 Agents That Generate or Neutralize Free Radicals
Generate Free Radicals
Alkylating AgentsAlkvl suKonate—biisult'an
Ethylenimine deri\'ative—thiotepa
Metal salt—cisplatin.carboplatin
Nitrogen nustard—cblorambucil, estramustine.cvclopbospliamide, ifosfamide.
nielptialaiiNitrosuurea—tariniistine
Triazine—dacarbazine
Natural ProductsAntibiotic^ileomycin,
dactinomycin.
diiiinorubicin, doxtiriibicin
{adriamycin), idarubicin.
mithramycin, mitomycln.
mitoxanlniiu'
Pihtophyllii'ii derivative—
etoposide, tcnipiiside
Other—procarbazine
Radiation—all forms
Antioxidants (NeutralizeFree Radicals)
Amifostine
Carotenoids—beta-carotene.lutein, lycopene
Coenzyme QIODexrazoxane
Glutat bione-seleniutncomplex
\'-acet\! cysteineSeleniumX'itamin C\'itaniin F
enhance the immune system and protect normal cells from theharm of radiation and other destructive mechanisms.Glutathione peroxidase. a selenium-containing antioxidantenzyme complex, protects the cell from free-radical injury.Cilutathione peroxidase is easier to measure than selenium andbas tbe advantage of assessing only biologically active selenium.Vitamin A and retinoids have anti-cancer eftects, repair normalcells, and modulate the growth and differentiation of malignantcells. Vitamin D^ inhibits cancer cell proliferation and replica-tion, induces differentiation of leukemia cells, inhibits the onco-gene c-myc. and enhances the immune system. Vitamin K3(menadione) inhibits cell growth, cell proliferation, DNA synthe-sis, and the cell cycle. Vitamin K acts on apoptosis throughexpression of c-mtc and c-fos proto-oncogenes and lowers intra-cellular pools of reduced glutathione.
Effects of Chemotherapy and Radiation Therapy on Serum
Nutrient LevelsCancer patients suffer from caloric and nutritional malnutri-
tion and have vitamin deficiencies, particularly of folic acid, vita-min C, pyridoxine, and other nutrients because of poor nutritionand treatment. " Chemotherapy and radiation therapy reduceserum levels of antioxidant vitamins and minerals due to lipid per-oxidation and thus produce higher levels of oxidative stress.""' Ironcould be the intermediate cause of this oxidative stress.""^'Therefore, supplemental iron should not be recommended to can-cer patients who have anemia unless it is an iron-deficiency anemia.
Antioxidants and Other Nutrients Wiih Chemoiherapy, Radiation Therapy ALTERNATIVE THERAIMES. |AN/FEB 2007, VOL 13. NO. 1 23
Early Studies
Five early studies showed that N-acetyl cysteine, an antioxi-dant, protects the heart from the cardiac toxicity of adriamycinwithout interfering with the tumor-killing capability of adri-amycin."' Seven cellular studies."'"" 22 animal studies;"' andhuman studies'"'' have demonstrated that vitamins A, E, C, andK, as well as beta-carotene and selenium—as single agents or incombination—all protect against the toxicity of adriamycin andactually enhance its cancer-killing eftects.
Cellular and Animal Studies
Titty-one cellular '" and 81 animal studies'"""" using nutrientsthat include vitamins A. B . B .,, C, D, E. and K. beta-carotene,other retinoids, selenium, or cysteine as single agents or in combi-nation gi\en concomitantly with chemotherapy, radiation, orcombinations of these modalities show the same effect—no inter-ference, increased protection of normal tissues, increased tumorkilling, and, in some studies, increased animal survival.
Observational Versus Randomized Clinical Studies
Compared to randomized studies, observational studies arcless costly, can be done more quickly, and have a broader rangeof patients. Observational studies provide valid information andvirtually the same results as randomized studies, a finding that dif-fers from previous conclusions.'""- Furthermore, "Observationa!studies do not overestimate the magnitude of the effects oftreatment compared with those in randomized trials on thesame topic."'"'""" In this 2-part article, we will summarize 50human studies, 36 observational and 14 randomized, thatreported concomitant nutrient use with chemotherapy and/orradiation therapy,
Re iew of Human StudiesFifty human studies, involving 8,521 patients, have been
conducted using single or multiple nutrients in combinationwith systemic treatment and/or radiation treatment and demon-strate that nutrients do not interfere with treatment. In fact, 47of these 50 studies indicated that nutrients decrease side effectsof treatment, and the other 3 studies showed no difference. Inaddition, many of the studies reported that nutrients producehigher response rates and higher survival rates when adminis-tered concomitantly with chemotherapy and/or radiation thera-py. This part of the 2-part article reviews data about vitamin A,beta-carotene, and vitamin E.'""' "
VITAMIN A (RETINYL PALMITATE)
In a randomized study of 100 postmenopausal patients withmetastatic breast carcinoma undergoing chemotherapy(cyclophosphamide, 5-fluorouracil, bleomycin. adriamycin, mit-omycin), patients were given daily doses of vitamin A (350,000-500.000 IU, according to body weight). \'itamin A—which manypeople erroneously believe is an antioxidant—^signitlcantlyincreased the complete response rate, duration of response, andprojected survival,'"
In an observational study of 275 patients with head andneck cancer, patients were treated with 5-fluorouracil and cobalt-tiO radiation, as well as vitamin A. Vitamin A enhanced the cellu-lar sensitivity to irradiation, increased treatment response rate,and lowered toxic side effects."'
In a randomized study of 153 patients with chronic myel-ogenous leukemia (CML), patients were randomized to receivepulse oral busuifan with or without the daih' administration oforal vitamhi A (50,000 IU). Patients receiving only busulfan hada shorter survival, with a 42% greater risk of death. In addition toincreasing survival, vitamin A decreased side effects andincreased treatment response rate.""
In an observational study of 40 patients with stage IIIB orstage iV non-small cell lung cancer, patients were treated withcisplatin (120 nig/nr divided into 5 days), vindesine (3 mg/m-on days 1 and 5), 5-flourouracil (500 mg/nr on days 1 and 5),beta-interferon (1 million IU 3 times a week), and retinyl palmi-tate (50,000 IU twice a day). Vitamin A produced fewer sideeffects, a higher response rate, and increased survival comparedto historical controls,"'
In an observational study. 23 patients with unresectable orrecurrent advanced oral cavity cancer were treated with 5-flourouracil (1,000 mg/m') and cisplatin (20 mg/m') for 5 days.Vitamin A (15,000 IL' twice a day) was also given throughout thetreatment. Vitamin A decreased side effects, increased responserate, and slightly increased survival.""
In an observational study of 36 patients with stage IV breastcancer, patients were treated with cyclophosphamide, 5-flourouracil, 4-epidoxorubicin, vincristine, and prednisone every3 weeks for 6 courses, followed by 2 courses of methotrexate,mitomycin-C, and mitoxantrone. Treatment continued withtamoxifen and vitamin A. Sixty-four percent of patients bad aclinical response, 19% had stable disease, and side effects wereminimal. Median overall survival was 32 months. These resultscompare favorably with historical controls.""
In an observational study of 22 patients with unresectableand/or metastatic pancreatic cancer, patients were treatedwith folinic acid (200 mg/m'), 5-flourouracil (370 mg/m'),epirubicin (60 mg/nr), mitomycin-C (10 mg/nr), interferon(1 million lU/nr' 3 times a week), and vitamin A (50,000 IUtwice a day). Response rates and survival were similar to his-torical controls.'"'
In an observational study of 49 patients with metastaticbreast cancer, 33 were treated with tamoxifen (30 mg/d), inter-feron (1 million iU 3 times a week), and vitamin A (15,000 IUtwice a day). Sixteen patients were treated with tamoxifen (30mg/d), interferon (3 million IU 3 times a week), and vitamin A(50,000 IU twice a day). There was no statistically significant dif-ference in the response rate, response duration, or survival in the2 groups treated with different dose levels of vitamin A and inter-feron. Compared to the Surveillance, Epidemiology, and EndResults (SEER) Program data of the National Cancer Institute,however, these patients bad a higher response rate and longersurvival with fewer side effects.'-'
24 AlTERNATIVf THERAriES, lAN/FEP 2007, VOL. \3. NO. 1 and ()thcrNulrienU With Chmmtierapy, Raciiatkin Therapy

BETA-CAROTENEIn a randomized study of 20 patients with advanced sqiia-
mous carcinoma of the mouth, patients were given 60 Ciy cobaltradiation therapy in 30 fractions. The week before and after radi-ation, and also during the third and sixth weeks of radiation,patients were given synchronous injections of chemotherapyconsisting of vincristine (2 mg), methotrexate (200 mg). andbleomvcin (30 mg). Patients were randomized to receive supple-mental beta-carotene (250 mg for days 1-21; 75 mg daily there-after). No toxic side effects of beta-carotene were observed.Patients who received supplemental beta-carotene had lesssevere acute mucosal reactions,'"
In an observational study of 15 patients treated withchemotherapy for various advanced cancers, patients were givenchemotherapy/radiation therapy and beta-carotene. Beta-carotene decreased side effects and allowed for a longer thanexpected disease-free interval in all surviving patients.'"'
VITAMIN E (ALPHA-TOCOPHEROL)
In an observational study of 66 patients with transfusion-dependent myelodysplastic syndrome, patients received eitherhigh-dose 13-cis-retinoic acid only or high-dose 13-cis-retinoicacid with alpha-tocopherol. Patients who received alpha-toco-pherol bad decreased measures of skin and constitutional toxici-ties and were able to achieve longer treatment continuation with13-cis-retinoic acid. As a result, fewer of these patients experi-enced progression to acute leukemia (28%) when compared topatients who received 13-cis-retinoic acid only (60'!'o). A 2-foldincrease in median survival also was observed in tbe group treat-ed with vitamin E.'""*
In an observational study of 39 patients with head andneck, skin, or lung cancer, study participants were treated withhigh-dose 13-cis-retinoic acid (100 mg/nr orally per day) andalpha-tocopherol administered in escalating dose schedules ot800, 1200, 1600, and 2000 IU per day for each subsequent 4-week treatment cycle. Over a 3-month period, patients experi-enced fewer grade 2 and grade 3 toxicities from high-dose13-cis-retinoic acid without altering its plasma concentration.'^
In an observational study of 17 patients with myelodyspla-sia, patients were treated with a!l-trans-retinoic acid (45 mg/m^in 2 divided doses), granulocyte colony-stimulating factor (start-ed at 1 microgram/kg per day), erythropoietin (5.000 \V per daystarting on day 2), and vitamin E (400 IU per day). Vitamin Ereduced the toxicity and increased the response rate withoutaffecting the performance of all-trans-retinoic acid.'"''
In an observational study involving 1 patient, the patientdeveloped a skin carcinoma in a chest wall scar from having amastectomy and radiation therapy 17 years earlier. After surgicalexcision of the carcinoma, she was treated with radiation therapyto the site. She also was given a vasodilator (pentoxifylline 1,200mg/d) and vitamin E (400 IL' per day) in an attempt to reducetbe new scar formation. The authors concluded that vitamin Edecreased the side effects of radiation, and the skin conditionbegan to improve by the fourth month.'"'
ln an observational study of 21 patients with metastatic
breast cancer, patients had endomyocardial biopsies and weregiven alpba-tocopherol orally al 2 g/nr daily starting 7 daysbefore cyclophospbamide, adriamycin, and 5-fluorouracil admin-istration. Vitamin E did not compromise the antitumor activity ofthe chemotherapy. Fifteen of 21 achieved an objective response—similar to the authors' previous experience. Vitamin E allowed foran additional 100 mg/nr of adriamycin to be given, but theauthors stated tbat vitamin E did not protect the heart.''
In a randomized study of 12 patients with metatstaticbreast cancer, patients were treated with doxorubicin as an intra-venous bolus infusion (60 mg/nr), and 6 were randomized toreceive 200 mg alpha-tocopherol given intramuscularly 6 hoursbefore infusion and 60 mg nifedipine given orally each day for 2days before treatment. A higher response rate was achieved andcardiac toxicity was prevented in those who received vitamin Eand nifedipine.'"
In a randomized study of 20 patients with acute myeloge-nous leukemia, patients were given vitamin E daily and treatedwith induction chemotherapy (10 patients) and intensivechemotherapy followed by bone marrow transplantation (10patients). Vitamin E increased treatment response rate and pre-vented mucositis—an inflammatory response of the oral cavitycaused by radiation therapy—especially during induction thera-py for acute myelogenous leukemia.'""
In a randomized study of 18 patients with various cancers,patients received chemotherapy appropriate for their cancer siteand were randomized to receive either placebo oil or topical vita-min II (400 !U/cc) to control mucositis. For tbe 16 patients witbhead and neck cancer, 5-flnorouracil (1,000 mg/m' as a continu-ous infusion for 5 days) and cisplatin (100 mg/m' on day 2) weregiven. For the patient with hepatocellular carcinoma, doxoru-bicin (45 nig/m' every 3 weeks) was given. The patient withacute myelogenous leukemia (AML) received Ara-C (100mg/nr/d tor 7 days) and doxorubicin (45 mg/m-' on days 1-3).Oral mucositis lesions were observed daily before and 5 daysafter the application of either vitamin E or placebo oil. Vitamin Eprevented chemotherapy-induced mucositis. In fact, whereasonly 1 of 9 patients receiving placebo achieved complete resolu-tion of their oral lesion, 6 of 9 patients receiving vitamin Eachieved complete resolution.'"''
In a randomized study of 16 patients with various cancers,all participants were treated with a regimen containing adri-amycin appropriate for the cancer site. Seven were randomized toreceive 1,800 II' tocopherol daily starting 24 hours before adri-amycin administration and continuing for at least 1 week afteradriamycin administration. Vitamin E did not interfere withfheniotberapy but also did not protect against cardiac toxicity.''
Sixteen evaluable cancer patients in an observational studyof 18 patients receiving adriamycin were given dl-alpha-toco-pberol acetate (1,600 IL! a day) to determine whether vitamin Ewould protect against alopecia (hair loss), which occurs in virtu-ally all patients receiving adriamycin. Sixty-nine percent ofpatients given adriamycin and vitamin E did not have alopecia.
.Antioxidants and Other Ntitrients With Chemothenipy,liadbtionrherapy ALTERNATlVIi THERAPIES, [AN/EEB 2007. VOL. 13. NO. 1 25

[•urthermore. a correlation was found between the time vitaminE was taken and the degree of alopecia. Most patients who begantaking tocopherol more than 72 hours before chemotherapytreatment did not have alopecia.""
SUMMARY
These studies show that vitamin A, beta-carotene, and vita-min E do not Interfere uith and actually can enhance the killingcapabilities of therapeutic modalities for cancer, decrease theirside effects, protect normal tissues, and, in some studies, prolongsurvival. Part 2 will review antioxidant combinations, B vita-mins, vitamins D^ and K.,, and the glutathione-selenium com-plex. A summary and discussion will then be presented.
REFERilNCES1. Jtnial A, Murray T, Ward E. Samuels A, et al. Cancer Statistii-s, :ilKI5. Ol Cuitit-r I Clin.
200ri;55(U:10-30.
2. US Bureau of Vital SialiMics. 19(llhnpresfni.
;j . Bail4. U.S
5
tTiieiit of Health and Human Services, Public Health Service. The Surf-eonG™r((/\/;(;«]rt(wAWr/te'«ii»i;//iiiW^VVashiiif;ti)ii. D.C: US('ptiv Print ()ffii-e: 1990.National Kesearth Council (I'.S.). Did itiid Ikulth: ImpHaitlons for Rcduaiii- CluonifDiMmeRisk. Washingion, P.I.: National Aiadimi)' Press: 1989.
I). C"ajii?ziRI.. (.liiiii-al status and optimal use of AmitiiMine.Oniolo),'). 1994; 1.1(1 ):47-5ii.
7. Bohii\li]vizki K!!, Klutntann S. Breninr VV, et al. Salivan' gLiiiil pmtei'tion by aiiiifes-tiiic in high-dnse radiiiimline trealnicnt: restills of a douiili'-blind plaiebn-coiitrollfd.Mudy../t/;jy Oiiiol. li)9«;lti:;i542-3549.
8. Brizd DM, Wa\.semiaiiTH. HenkeM,el al. Phase III randoiiiized trial olaiiiLroMint'asa radiiiprotci'tor in hratl and neck caniiT../ Clin Oiiml. 2001); IS( 19);.S339-;(:i45.
9. (iiieinau CN, Bump EA, Kramer KA, Chemical niiHiifiers ol ranct-r trtaimmt. / ClinOnail. m&:6(4}:7m-7y^.
W. C'onstine LS, Zagars G, Kubin P. Kligi'rman M. Prntectioii hy WK-2721 of humanbun t marrow function lollowinp i rradiat ion. Init I Hudiiil Omol Huil I'hyi.
11. Oouay I., Mu C, Giarratana MC, et al, ATTiifustiiiL- iiiiprovfs tlie antili-ukrinic iherapeu-tif index (if mafosfamidc; iiiijilifations fur boiif m; rr lv^ purjiinj!, Hlond. 1995:86(7):2a49-28.'iri,
12, Ki'iup G. Rose P, Luraiii J, et al. Aniifiistini' pretrcatment for priitection againslcyfliiphipspliamiile-iiiduied and cisplallii-iiiduced toxicities; rtsults iif a randoniii^ed iiiri-inil trial in paticntMiithaihjncedovarian(an«r,yC//HO/ii(j/, 199li;I4(7);:fltH-2112,
i:i, KligiTtiian M,\1, liluivr HI. Turrisi Al", iM al. Toxicity of Wk-272] administered in sin-gle and multiple doM's,/i/(,/ftiJw;()Hi»/B/WPyjv.v l!)84:10(9):177:i-!77(i,
14, Santini \ . Gilts V). The potential uf amifiistine; from cjtopruti'ttanl to therapeuliiagent, Hmimitiiltigini. 1999:84(11);1O3.';-1(I42,
15, Schdn, PS. Resnit.sof chmioiherapy and radiaiiwi ilicniin iiriitettion (rials wilh WR-272\.CtimrrImvsl. im2:\0(iy2A-2^.
16, Schiller jH, SUirer B. Berlin I, el al Amifostine, dsplaiin and viiihlastine in metaMaticnon-small ceil lunji raiuer: a repi)rt of high response rales and priiionged survivaiy
/ /
17, Tannehill SP, Mehla MP, Amifostine and radiation therapy: pasl, present, and Intiirv.Sanin Omol. 199ti:2:i(4 Suppl H);t!9-77,
IK, Wasserman IH. Brizel DM. The role olamilbstinc as a radioproLctlor. Omolni^r.2()01;ir.(10):1349-B54,
lit, Carlion, K,W. Reducing lhe cardio toxic ity of the anLhraiiiline.s. Oniolof^w
1992:fi((i);95-llKUI)4,K)7,2t>. Hellniann K, Anthrao'iline cardiotii.iiiity prevention by dexraziixaiie: breaktiirough of
a ba t r ie r - ' iha rpens ant i tumor prnflle and therapeutic index, / Clin Oncol.199(1:14(2 );:i:i2-^33,
21, Klein P. Muggia FM, Cytnprnteet i im; shelter from the s turm. (hiailiiiii.^!.
22. Suain SM, iVhaky fS, Gerber MC, Ewer MS, iJianchiiie jR, Gams Ka. Delayed adminis-tratiiin of dexrazo.vane proiides rardioproteiiiiin for patient,s with adv-anted lireast can-cer treated witli do>;(irubidn-rontainingtherapy,./C//ji O/;ni/. I997:15(4):133:M:i4l),
2:1, Myers C, (Uanni L Simiine C B, Klecker R, Greene R, Oxidative destruction of erythro-cyte ghost membranes catalyzed liv the doxurubicin-irim lomiilet, Bioilifini^ln.1982;21(8):!707-1712,
24, ( armine 7C, E\an.s I'. Brucheil (',. r,\ans R. Iiaiidj;retinger R, Niethammer D, Halliivell B.Presence ol iroti catalytic fur h-ee radical reactions in patients undergouig cheniotherapi:implicatioiisfiirtht'ra|icutic management, (li(mi'r/,rt/,1995;94(2):2l9-226.
25, (iordeuk \ K, Brittenham ( ; M . BleuIIIVCin-reactive iron in patients with atutc non-lym-phticyticleukemia.I'tBSLett. l!:l92,iO8(l);4-li.
2ij. llalliwell B, Aruoma 01. Mufti G, Bomford A, Bleomycin detectable iron in serumIriim leukaemic paticiiis liefiire and after chemotherapy. Therapeutic implications torireatnienlwithiixidanl-generatingdruj^s,/•M.V/cH, 1988:24l(l-21;2fl2-204.
27. Briid\ JE, In vitamin mania, millions take a gamble on health. The .Vcii' York Tima.October 2ti. 1997: 1, 20, 21 (quoting l.arry Norton, MU uf Menmrial SliianKetterin;;. NVri.
28. l.abriola D, Livingslmi R, Possible iTileraitiiins betucen dietary antio.^idanls andcbemiitherajiy, Oncologw 1999:i:)(7):1003-l(MI8,
29. ,\gus DB. Vera JC. Golde nW. Striimal cell oxidation; a mechanism by which tumorsobtain vitamin C,CiJHi(Tft\s,19H9:59(18);45G5-4,S58.
3(1. Gottlieb N, Cancer treatment and vitamin C: rhe debate lingers, /;VC7. !999;91(24 );2U7:S-2()75.
:il. Brown J. Byers T, Thompson K, Eldridge H, [loyle C, Williams AM, Nutriiioii during
and alter cancer treatmeni: a guide I'nr informed choice.s by cancer survivors, C.\
33,
35.
The American Cancer Socielv. Selecting which drugs to use lor chemotherapy treat-ments, .•\vailablf al: http://wivw,cancer.urg/docroot/ETO/content/ET0_l_4\_Si!leciin^Which_Drugs_to_lse_For_Cheniotherapy_TreaImenis,asp?sitearea=^ETO,Accessed November 30, 21106,
Leeb BK, Witzmann G, Ogris Ei, et al, Folic add and tyanocobalamiii levels in serumand erythrocytes during low-dose methotrexaie therapy of rheumatoid arthritis andpsoriaticarthritispalients.Cfty&VfA'/jij/mi/K/, l995:13(4):45ii-4G:i,Morgan SI., Baggott JE. \auglm WH, et al. Supplementation with folic atid duringmethotrexate therapy lor rheumatoid arthritis. A double blind, placebo-con trolledtria!. Am Intern Med. 1994:121(11);833-841.
Hunt I'd, Rose CD, Mcllvain-Simpson ti, Tejani S. I'heelleds of daily intake of lolicacid on the efficacy iit melbotrexate therapi in children with juvenile rheumatoidarthritis, A controlled study,./ klteimmlphg}: 1997:24( 11 ):2230-2232.Basu TK, Significance ot vitamins in cancer. OmvlD^v. 1976:33(4); IKH-187,Rhuvarahamurihy \ , Balasubramanian N, Govindasamy S, Effect of radiotherapy andchem0radiotherapy un the circulating antioxidant system of human uterine cervicalcarcinoiiia, M cdl Biodim. 19HH:158( 1): 17-23,
Clemens MR. Udner C, Ehninger G, et al. Plasma vitamin E and beta-camiene concen-trations during radiochemotherapy preceding bone i]iarr(m transplantaliiwi,,-!/»/ ClinNulr. 199O:r)l(2);216-219,
Clemens MR, Eadner C, Schmidl H, el al. Decreased essential antiosidants andincreased lipid hydroperoxides following high-dose radiochemotherapy. frir Rad ResCommun. 19SF):7(3-6):227-232,
Clemens MR, Eadner C, Schmidt H, t i al. Decrease of alpha-tocopherol and beia-carotene by high-dose radiochemotht-rapy preceding bone marrow transplantation,.•\mi .V y.Acid.So. I989:57O:4:!1-4:M,
Clemens MR, Muller-l.adner Cl. Gey KE. [Vilamins during high dose chemo- andradiotherapy! I Article in Germa[i|.Z/.>W(i^irMH^ii7w,1992;31(2):110-12(l,Clemens MR. [Vitamins and therapy of malignancies] [Article in GermanI, TIUT(/w«/;, lfl94:,'>l(7);483-488,
Drei/,en S, McCredic KB. Keating MJ, Andersson GS, Nutritional deficiencies inpatients receiving cancer Lhemiithera;iy,/ViWi,'ni(/mifi'Afn/, 199O:87(1):!G3-167.170,Durkeii M, Herrnring C. linckh B, et al. Impaired plasma antioxidative defense andincreased nonirans ler r in-bound iron during high-dose chemotherapy andradioihemotherapy preceding bone marrow trans|ilantation, f'm- R,idii Hii'l Mnl.20()();28(6):887-K94'.
DurkiEi M, Agbenu J, Einckli B, et al. Deteriorating tree radical-trapping capacity andanlioxidant status in plasma during bone marrow transplantation. Biwi' Murrou-7hiHV''""'-199r,:15(5);757-7(i2,
Erhoia M, Kellokumpu-I.ehtinen P, Metsa-Ketela T, .Alaiiko K, Nieminen MM FUedsof anthracyclin-based chemotherapy on total plasma antioxidanl capacity in smali celllung cancer patients,/^>('(K(ii/;iffiii/AJ«/, 1996:21(3): 383-35)0,Krhohi M, Nieminen MM, Ojala A, Metsa-Kelela T, Ketlokumpu-I.ehiinen P, .\lho H.Human plasma antioxidant capacity during radiotherapy lor hmg cancer: a clinicalstudy./£r/'C7/;iC<iHi(T«n,199a:l7|3):32r.-3:i(l.
Eaber .\l,('ouiiray C, IlidaH, Moussean M. Eavier A, Eipid peroxidalion products, and\ itamin and trace element status in patients wilh cancer betore and after cheinothenipy,including adriamycin, A preliminary study. ftW7"raicA/mfes,1995:47(l-3):117-123,Eaure II, Coudray C, Mousseau M, Duc-ros V, Douki T, Bianchini i. Cadet I, 5-Hydroxymetbyluradl e,'4cretion, plasma TBARS and plasma antioxidant vitamins inadriamycin-treated patients, free ftii//iB/i>/AIivy.l996:20(7):979-9H:i,Henquin N. llavivi E, Reshef A, Barak E, Horn Y, N'uiritional monitoring and coun-selling tor cancer patients during chemotherap}', O«rii/iii;i', 1989:46(3):173-177.Henriksson, Rogo KO, (;rank\ist K, Interaction between cyto.statics and nutrients. jVferfOmol TmnrPharmacolhcr. \mi:»(2):79-m.
Kakar S, Wilson C. Bell J. Plasma and Ieueocyte ascorbic acid conceniration in acutelymphobiastic leukaemia,/f./,Vt,'i/,Vn. 1975:144:227-232,
Udner C, Ehninger G. Gey KF, demons MR. Effed of etopnside (VP-l(i-213) un lipidperoxidation and antioxidant status in a high-dose radiochemotherapy regimen.CaiHcr Chcmdlm PhariiiMfll. 1989:25(3):21(1-212,
Eonk MP, Musch E, Lipid peroxides in the polychemotherapy of cancer patients.Chmolhcriipy. 1994;4()(1):8-15,Ohnuma T, Holland JF, Nutritional consequences of cancer ch emu therapy andimmunotherapy,0/«iwAli.\, 1977:3717 Pt2):2395-24O6.
Ojiro \\, Takenoshila M, Toshinaga T, Shimazu H. [Significance of vilamin K (\ K)administration in patients under chemotherapy during postoperative fasting periodi[Article in Japanese!. :V;/7m»{;cl(ii:;iij(iii//i/sv;j/. 1992:93(11:9-1:1Putischnian N, Byers T, Houghton L, Root M, Nemoto T, Campbell TC, Effects ofbreast cancer treatments on plasma nutrient levels: implications for epidemiological
26 ALTERNATIVE TI IEKAPIES , l A N / E E B 2 0 0 7 , VOL. 13, N O , 1 Attlioxidants and Other Xtitrients With Chetnotherapy, Kadiytion Therapy

studies. C(iH(iT^y>irf,'m/-'/«/»jniJrjl</,\;V
58. Sangeetha P. Das I'N, Koratkar R, Suryaprabha P, Increase in free radical generationand lipid peroxidation tbllow ing i hemotherapy for patients with cam er. lyec liiidit Biiil
Schreurs VVH.OdinkJ, Egger RJ, VVedel M, BruuingPI-, The influence of radiotiierapyand chemotherapy on the vitamin status of cancer patients, liil I Vitiini ,\'iilr Ris.1985:55(4):425-432.
Sentiirker S, Karahalil B, Inal M. et al. Osidalive DNA base damage and antioxidantenzyme levels in chi ldhood acute lymphublas t i r leukemia, I'l-BS Lett.1997:41 ti(;»:286-290,SohoISM, CimoyerJM, Zill R, Thawley SK, Ogura Jll, NutriunalioMcepts in the man-agement of the head and neck cancer patient, IL Management concepts, Lar\'ngoKopc.l<i7!):89((>Pt l),962-979,
Stahelin I IB. Critical reappraisal of vitamins and trace minerals in mitritional supportof cancer patients. ,Vfl/y;i'«t'«n'C'(im('r, 199li:l(ii);295-297.Subramaniam S. Shyama S, Jagadeesan M, Sliyamala Devi CS, Oxidant and antiiixi-dant levels in the erythroeyiesnf breast cancer patients treated withCMF, Mi'i/.S(ift'.v,1993:21(2):79-80.Wayner DD. Burton CW, Ingold Kl', Barclay I.R, Liicke SJ, The relative contributiixisof vitamin i'., urate, ascorbate and proteins to the total peroxyl ratliea It rapping antiiix-idam activity of human blood plaJima.Bwc^//ffl/i/('/'Ai'j,'lf/fl.l987:924{:tl:4()S-41(i.WeijI Nl. Hopman C.n, Wipkink-Bakker A, et al. Cisplatin cnmhination chemothera-py induces a fall in p lasma an t iox idants of cancer pa t i en t s . .'IHW Oni-cl.
59.
60.
t)6. Yang KC, Li X, and Tsui ZC, lhe reiatiiiriship between nvitritifinal antioxidants andserum lipid periixides in cancer patients. In Vivo, 19)i9::i(!l):211-214,
(17. Diirr RT, Cytaproiective agents for anthracyclines. Scmin Oiitvl I99ri:2:i(4 Suppl 8):2Ii-:i4.tiS. Ciaccio M, Tesoriere 1., Pintaudi AM, et al. Vitamin A preser\'es the cytotoxic acti\'ity of
adriamycin while ctiunteracting its peroxidative etfects in human leukemic cells in vitro.
RipoU, EA, Rama BN, Webber MM. Vitatiiin i: enhances the chemotherapeutic eftectsof adriamycin or! liuttian prostatic carcinoma cells in vitro,./ Cro/, 1986:136(2):529-5!il,Shimpo K, Nagat.su T, Yamada K, et al. Ascorbic acid and adriamycin texicity. Am J<7w,Vu;r,1991:54((isuppl):1298S-i:!(>lS,
(leetha A, Sankar K, Marar T, Devi CS, ,\lpha-tocophen>i ritliicc doxiiriiliiciii-induiedtoxicity in rats-histological and biochemical evidences. Indian I I'hysinl I'lniriiniiol.1990:34(2):94-<i8.Jiitti A, Maiorino M, Paracchini L Piccinini K Ur.sini l\ Protective eHect ol dietan' sele-nium suppieifientation on delayed cardiotiixicity of adriamycin in rat: is PH(~rPX butnot C.PX involved? Fref Rmlii Biol Med. 1994:16(2):284-28S,Myers CE, Midiiire W, Young R, Adriamycin: amelioration iil toxicily by iilpha-toco-phernl, Cumrr Tnal Ri-p. 197fi:60(7):9til-!)'ti2,Sinj;ai PK, Tong IG, Vitamin E deficiency accentuates adriamycin-indticed cardiomy-i.pathy and cdl suriace changes, .W"/f,///i™ft,™, lS)88:84(2):16:i-17l,Siveski-llskovic N, Kaul N. Singal PK, Probiicol protnotes endogenous antiiixidantsand provides protection against adriamycin-induced cardiomyopathy in rats.
I.egha SS, Wang YM, Mackay B, et al. Clinical and pharmacologic investigation <il theetTects of alpha-tocopherol on adriamycin cardiiitoxicity, .Ann N Y Aiiid ,Vii.1982;:i9:5:411-41K.Lenzhofer R, tianzinger V. Rameis H, Moser K. Acute cardiac toxicity in patients afterdoxorubicin treatment and the effed of ciimbiried tocophero! and nifedi|iiiu' pretreat-ment,./C<i»irfft'.\(7j>; (II/.VJA I983:lfl«2):14,'i-I47,
Weil/man S.\, l.orell E, {"are>' RW, Kuufiiian S, Stossel TP, Prospective study ot toco-pherol prophylaxis for antliracycline cardiac toxicit}: Curr Tlier ft',v, 19H0:28:t382-(i86.Anderson D. Basaran N, Bloviers SD, Edwards Aj. The effect iif antioxidants onbleomycin treatment in in vitrii and in vivo genotoxicity assays. Muln! Res.1995::i29(l):37-47.
liianchi I,, Taten F, Pizzala R. Carotenoids reduce the chromosomal damage induced1)\ bieoitiycin in htiman c«lttire<l lymphnqte^. Anliciiticer Res. 1993:13(4): 1007-1010.BiimpE,\, BraunhutS], Palayoor ST, et al, Novel concepts in modificailon of radiationsensitivity, InlJ Rmlitil Oncoiliwl l'hy<,. 1994:29(2): 2 4 9-253,
Chiang CD, Song EJ, Yang VC, Chao CC. Ascorbic acid increases lirug accumulationani! reverses vincristine resi,stance of human non-small cell lung-cani'er tells, BUnhemI. l994::illl(Pt:i):759-7ii4,Harapanhalii RS, Narra VR, Yaj limai \ . et al. Vilamins as radioproteitors in vi\o, II.Prtitectidii by vitamin A and soybean oil against radiation damage caused h\ internaltadionudide^. Radial Rey 1994:I39{1):115-122.Komiyatna S, Kudoh S, Yanagita T, KiiHanii M. Synergistic combinaliiin ol S-lhui-rouracil, vitamin A, and cobaii-(i(l radiation for head and neck tumors-antitumor com-liiiiaiion therapy with vilamin A. .lurijjVdvftv/./jnvu, 1985:12(S«ppl2):S23!)-,S24:i,Prusad KN. I lernandez C, Edwardi-Prasad J, Neisnn ], Biirus T, Robinson WA,Modilicatimi iif the elfect nf tanuixilen, cis-platin, DTIC, and interieron-aljiha 2b unhuman melanoma tel ls in culture by a mixture oi vi tamins, Niilr Ciimer.
8(i, Salvadori DM, Ribeiro I,R, Xatarajan ,\T, Effect of Iwta-carotene on clastogenic etteetsof niiiumycin C, methyl methanestiiplionaie anil bleomycin in Chinese hamster ovarycells, Mii'htgenc>.i!.. 1994:9(l]:53-57,Sweetman SE, Strain JJ, McKelvey-Martin \'J- Effect of atitio\idant vitami!i supplemen-iation (in DNA damage and repair in human lymphoblastoid cells, Nuir Canter.
The PowerfulProven ProbioticsDDS'- PLUS PROBIOTICCAPSULESDESCRIPTION: DDS"' Plus is the sourceot H Special strain Lactobacillus acidoptiilus(DDS-1 straini, Bifidobsctenum longum,and Frjctooligosaccbarides. DDS' • Plus isfree of dairy products, com, soy andpreservatives.POTENCY: Each gram (2 capsules)contains 5 biilton viable Lactobacillusacidophilus (DD&l strain) andBifidobacteriumlongumst the timeof mariLjIactunngINDICATIONSAND USAGES:As an aid inmaintaining iwi:i i.ilintestinal ftota withbeneficialLactobacillusacidophilusBifidotacteriumlongum and undeiconditions of diges-tive disorders andfdloviiing antibiotic tfiefapy. DDS, is a reg-istered trademark of UAS Laboratories.
The Safe & HeaHhy Choicefor Kids & InfantsDDS'- JUNIOR PROBIOTIC FORCHILDRENDESCRIPTION: DDS™* Junior is the sourceof a speciai stiain Lactobacillus acidophilus(DDS-1 strain), Bifidobacterium infantis,and Fructoobgosaccharides DDS" - JuniorIS free of dairy products, corn, soy andpreservatives.POTENCT Each gram 11/4 levelteaspoon) contains 5 billion viableLactobacillus acidophilus (DDS-1 strain)and Bifidobactenuminfantisat the time ofmanufacturingINDICATIONS ANDUSAGES: As an aidin maintaining no'malintestinal flora withbeneficialLactobacillusaddophilu5Bifidobactenuminfantis and underconditions ofdigestive disorders andfollovifing antibiotic thera-py. DDS, IS a registered trademark ofUAS Lafwratones
.•\nfioxi(lanls and OthtT Nutrients Wilh Cliemofherapy, Kaciiation fherapy
15 Reasons fen DDS PROBIOTICS1. Contains Superior &Viable (Live) Strains
2. High Potency
3. Non Dairy
4. Human Origin, So Adapts to Human Body
5. Acid & Bile Resistant iSui^'ives Stomach Acid)
6. PnDduces Hydrogen Penaxide, Lactic Acid & Natural Antibiotics
7. Fortified with Prebiotics (It \s a Synbiotic)
8. Freeze-dried and Packaged with Nitrogen to ImpnDve Stability
9. Stable at Room Temperature for Two Years(Refri;^er-;ition at -OT Recommended for Temperature Fuctuaton)
10. Available in Veggie Capsules
11. Generaiiy Recognized As Safe (GRAS)
12. Helps Maintain a Healthy Flora
13. Backed by University Research, US Patent & Trademark
14. Listed in Physicians' Desk Reference & Doaor Kecommended
15. Americas Favorite PnDbiotic Since 1979
UAS LABORATORIES9953 Valley View Road, Eden Prairie, MN 55344, USA
Tel: (800) 422-3371 • Fax: 1952) 935-1650E-mail: info@uaslabs,com • Website: www.uaslabsxom
DDS® ProBiolics by UAS Labs ace more Ihan multivitamins and are to be taken daily on anamply stomach before breaktasl ODS® Probiotics by UAS Labs riisel all the charactetisttcs
of a Super Probiotic Supplemenl S Dr Dasn s TOP PICKS.

88. Vadgama JV. Wu V, Shen 0. Hsia S. Btock J. Effm of selenium in combinaiion withAdriamyLin oi ln\o\ nn SL'VtTa! differenl ca iue r cells. Anliiiiitner ffc.v.
S!(. A|jf)enrotli H, Winni'tHd K. Role of glu!alhi<ine kir dsplaiin ncpliroirainty Ind d l /
90. Baldi'wC.S, MollG, de KanlerH.ian Rawr B. dc (ku-ijJJ, Vermeiilen NP. The riierha-nism of imeracl ion behvccn l ispla i in and sfliTiiie. Hiotlum Phurmnioi.
99,
KIO,
105.
108.
UJ9.
110.
111.
IU.
I i:i.
114,
I Hi.
117,
Baraboi VA, Olelnik SA, liliuiii IA, Khmelevskii hi\'. U'ro-iixidaiil and antiuxidaiilhonii'sostasU l[i giiliipa pij s lollowinp fractioiiaied x-iav irradiahtin al low dosfs andthe correctitin of diwirders mtli an antiiwidaiit complral [Artklc in Ri]\sian|, KadhiD,liiiil Riulmmi 1994;34(2):24()-24ti,
Ren-Amotz A, Rsclimilevich B, tlrtriibtr^ S, Seta M, Wf^hlur Z. Natural bcta-iiiriiiiTii'and whole body irradiatinn in rats. Ruiiktl Fnviwii Hinjiliyi. lHHIJ;.ir)(4);2Kri-288.t'rary Kl, Milarty MF. Potential diniciil apfilicaiiims liir hiyh-dose iiLitritional aiitioxi-datits, Af.i/%;»//;«•(•,(. I984:]:«l):77-im.El-Nahas ,SM, Matlar FE, Mohatned AA. Radiopr.itectivr etfi'U ol'vilamins (. and E.Miikil Ren. ]H9:i:301(2):143-147.kageriid. A. Peterson HI, Iifikt of toiojilicrol in irradiation iit artilidally hyposk mltumours. Second Rome International Symposium: Binlogical liases ami Clinicallni|)licatinns. September21, IHSO; .1-S).kilinc {', 0/ ian <). Karaoz T, Snngnroglu K, knlluay T. Karaia \.. Vitamin T reducesbleomycin induced lun^ fibrosis in iiiice; biochemical and iriorpholopcat studies. /Hmk Clin PliytMl Pharmncai I993;4(:j);249-26!l.\'agai Y, llorieT. Awazu S. \ ilaniin A, a iisd'iil biucheniical modulator capable of pre-venting intestinal daniagi- during nii'thotrexale treatment. Pharmiiail Toxhnl.
Nakanuira F, Pinnell SR, Darr D, et al. Vitamin C abrogates lhe deleterious efiecls nfliVB radiation on lutaneoiis immunity by a mechanism that dnes nol dejiend on TNF-alpha,//»i»(;)c™(i(»/. 1997;in9(l):2fl-24,Odagiri V, Kanibe T. Katayania H. Takenuito K, Mmlifualion nl lhe dasiopenic aclivityol X-ray and 6-mercaptopurine in mice In prefeeding uith vitamins (' anil F, / ,Vw/f.
(Ikunielf, i'. Interactions between ascorbic acid and lhe radiation of bnne niarrou.skin, and tumor..4»i./(7/>)A'u(r. 1991:54(liSuppl):ll!SIS-1283S.Perez JH, Macchiavelli M, Leone BA, et al. High-dose alpha-tiiciipherol as a preventiveofdoxnruhidn-induced alopecia. (i/i;i(T7"r(((/wjm//;(;j. 198H:70(10):12B-1214.
102. Ravi R, Somani SM, Rybak I.!', Mechanism of cisplatin otoliaidiy: anlioxidant system.
101.
1113. liiabdienkii \ l , Ivannik BP, Khorokhnrina \A, Riabchenko \ I, Sin'kova RV, CrnshevaIP, Dzikovskaia, | Fhe molecular, cellular and systemic mechanisms of lhe radioproiec-tivc action of miiltivitamin antiosidant ciimplews] lArticle in RussianI, K(i,luil\ HwlRmiiimil I99<i:36(fi):895-899.
104, Satoh M, Nagamima A, Imura N. Effect of co-administralinn of splenite on lhe toxitilyanti anti-tumor activity ni ti.splaliii given repeatedly tn mice, CiiiHir Clinnolhmipy
Sminia P, van der Kradit All, Irederiks VVM, lansen W. Hyiwrlhermia, radiation car-cinogenesis and the protective potential ut vitamin A and N'-acety I cysteine. / (um if fii.tClin Omol 1996:122(e):343-:irj0.Sriniva.san V, Weiss JK, Radioprotection by vilamin F.: injectable vitamin V. adminis-tered akine or with WR-,if;8!! enhances the snrvival of irradiated mice, Inl I RiiiliiitOmol Biol Phys. ]992;2:t(4):K41-84.'",,\ initha R, "Fhangaraju M, Sachdanandam P. Iilit'ct of ad ministering c\clophosphamidcand vilamin E on the levels ol tumor-marker en/ymes in rats ivith esperinieniallvinduced r!lirnsarcoma,;/w,/,W('(/.SV/W,f/.l<19.5:48(3):145-l'i(i.Wiseman JS. Senagore ,\J. Oiaudry IIF Methods to prevent colonic in|ury in [lelvicradiation./)/.vtW(»/ftrrMjH, I99'5:37(ll): 1090-1094,
Zidenberg-Cherr S. Keen t'l.. Inlluenre nf dieiary manganese and \itairiin K on adii-aniycin toxicity in mice, Toxicnl l.ttl. lH8ti::i()( 1 ):79-87.Zuiiino F, Pratesi G. Michdoni A, tavalletti E, Sala F, Tolanetti O, Proteclive effect nfreduced glulathione against cisplatin-induced renal and syslcmic toxicity and itsintluence on lhe therapeulic activily ol lhe antitumnr drug. Chem Hiol Inlmid.
liensun K, llartz A], A comparison of observational studies and randnmi/.ed, lon-trnlled trials. A'%/,/Mr(/.20(X);:M2(2.'^):lS7S-188ti,llLteniiacher K. Impact nt ratidom assignment nn .study outcome: an cinjiirical i'\ami-\\M\im.Cimi!olCiin Trials. 1992;i.3(n:,Sli-iil.( oncatn ], Shah N. Hnrwit/ Rl, Randomized, cmitrnlled trials, observational sludies,and the hierarchy of research designs, ,V linfilj Miul. 2O<IO; J42(2.'i): 1887-IH92.Israel I, Hajji (1, (ireflt-Alanii A. el a!, [Vitamin A augmentation of lhe cilects nfchemoiherapy in metastalic breast cancers after menopause, Randomi/ed trial in 100jiaiienis! I Article in French],,lfi» Mil//n(m/.\ l!i85;13ti(7):r)SI-.''..'V4.Komiyama S, Kudoh S, ^'auagita T, Kuivaiio M, SjTiergixtic combination iherapy of S-floutouradl. vitamin A. and iiibalt-liO radiation for head and neck tumiirs-antittimoruimbination therapy ivith vitamin A. ,^j;m(V,nv(ii,in'Wj. 198ri:12(Suppi2):S2:!9-^S2'I.S.Meyskens Fl, Koperky KJ. Phast III randomised trial nf the treatment of chronic slage("Ml, with pulse, intcnnitienl busulfan therapy (SW(Ki 7984): improved siirtival withthe addition of oral vitamin A (50,(100 lU/day). Seventh Intemalional ( onierence mllhe .Adjmant Therapy ot'Caiicer.Tnc-ioii, Ariz, March It>-13,199:1:3r).Recchia F, de I ilippis S, Rea S, Corrao ti, Frati F, tisplatin, viiidcsiiie, 5-lluorouracil,
beta-iliterteron and retiny! palmitaie m advanced non-sniall cell luiii; cancer. A p[iase IIstudy Proc Aiinu Mir! .Am SoiCli'i Onml. 1993:12:A1144,
118- Recdiia !•, l.dli S. Di Matteo (I, Rea S, Frati F. |SFT), cisplatin and retinni palmitate inthe manageinenl nf advanced cancer ofthe oral cavity. Phase 11 studyl lArticle inItalianI, Clin Tcr. l9!!3:142(,'"j|:4(IH-4O9,
Kecchia F, Rea S, Poinpili P. el al, Beia-inierteron, retinoids and tamoxifen as inainic-nance therapy in melastatic hreast canter, A pilot slutiy. Clin Tn. 199,'i;14lil l(l);hll!-ij!(),Recchia F. Seraliiii F, Rea S, Frati I,, Phase II sliidy of,'>-lhiorouracil, lolinii acid, epiru-bicin, mitomycin-I", beta-interfer<in and retinoi palmitate in patienis with unresectablepancreatic carcinoma. Pfi« Annu .Mtvl Am Aisoc Cuiictr Res. 1992;:i:i:A12i)fi.Recchia F, Sica G. de Filippis S, et al, Interferon-beta, retinoids. and tamnxifen in thetreatment of metaslatic breast cancer: a phase II study../ Inlnji-nm Cvlokiiif Riy
122,
123,
12fi,
129,
Mills EF. Tile modifying etluct of heta-carutene on radiation and chemotherapyindttced oral mucositis, HrJ Ciimu. 1988;.'"i7(4):41()-417,Santaniaria I, Bianchi-Saniamaria A. dell'Orti M, Carotenoids in cancer, niastalgia.and AinS: preventinn and treatment—an overview, / Dfi'irnji t'athol Toxiinl Omoll996:IS(2-4):89-9r).Bcsa FC, .'\hrahm 11., Barthdliimeu M|, Hy^inski M, Nowell PC, Ircalnient vviih liicis-retinoic acid in tratisfusiim-dependent patients wilh myelodysplaslit syndrome anddecreased toxidty with addition of alpha-tocoplierol .Ami Mid. 199O:89(6):739-747,Dimery I. Shirinian M, Heyne K, et al. Reduction in toxicity nf high dose 1."! ds-relinoicacid with alpha-tocopherol, PriK Amiu Mrvl Am Soc Clin Omol. l992;ll:A3i!9.Oanser A. ,Maurer A, t onizen i', et al. Improved multi l ineage response nfhemalfipoiesis in patients wilh mydixlysplastic syndromes to a combination therapywith all-lrans-retinoic acid, grannlocyte colony-stimulating factor, erylhr<p[)iiif'tin andaipha-tocopherol..!//» llemalol 1996;72(4):237-244.<;<illlolier P, Krahn G, Kiitling IK, Siiick VV, Peler RU, |The trealnient ofculaneousradialioii-indneed librosis wilh pentoxify'lline and vitamin E, An empirical reporti|ArlicleiiiGennan|,,VmiW,w/kr(ln((i/. 1996:172(l):34-:iS.lope? I, (^ondou C Ribrag V, Sauvage C, Hazebroucq, Dreyfus l\ (Freatinent ol'mucosilis wilh vitamin E during administration of neulrojienic anlineo|ilastic agentsiI Article in Kretuh |. .\mi Mai Inlam: 1994; I4ii((i):4(15-4O8.Wadleigh RG. Redman RS, (;raham Ml., Krasimu Sll, Anderson A, fiihen Mil.Vitamin t! in lhe t real ment nf chemotherapy induced mucositis. Am I Mai.IW2;92(5):481-4N4.WiKid I.A, Possible prevention of adriamycin-induced alopecia by locopherni, N hitl IAf / lF )85312( I6 ) l ( i
Invitation to All NCCAMGrant Recipients
Applying for a grant requires a substantial commit-ment of time and effort to review the relevant literaliire forthe particular field of research heingpursued. However.much ofthe excellent scholarship is read only by NationalCenter tor Complementary and Aitemative Medicine(NCCAM) or other grant providing institutions.
Therefore, we invite all NCAAM grants recipientsand any other researchers to submit for publication toAlterniilive Therapies in Health and Medicine reviews thatwere integral to grant applications. The field of integrativeand complementary and alternative medieine will beiietitfrom an enlarging body of thorough review papers rele-vant to the field.
Please send your submission to:[email protected]
Sincerely,
Mark Hyman, MtiEditor-in-ChiefAlternative Therapies in Health and }\4edicine.
28 ALTtKNATiVH THt:RAPIES, |AN/FEB 2Q07, VOL 13, NO. 1 AnlioxidytUs ami (1IIUT Nutrients With Chenm















![14] Antioxidants](https://img.pdfslide.us/doc/110x75/577ccfa61a28ab9e78904327/14-antioxidants.jpg)













