Embed Size (px)
Citation preview

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
22
Litvinova et al. World Journal of Pharmacy and Pharmaceutical Sciences
ANTINEOPLASTIC DRUGS: A FOCUS ON FEATURES OF
REGISTRATION, IMPROVING THE QUALITY OF CLINICAL
TRIALS USING A PATIENT-CENTERED LOGISTICS APPROACH
Elena Litvinova*, Olga Posilkina, Svitlana Kovalenko and Anastasiia Lisna
Department of Management, Economy and Quality Assurance in Pharmacy, National
University of Pharmacy of the Ministry of Health of Ukraine, Kharkiv, Ukraine.
ABSTRACT
The aim of the work is to analyze and summarize existing scientific
approaches and mechanisms for fast-track approvals, improving the
quality of antineoplastic drugs clinical trials using a patient-centered
logistics approach. Materials and methods: Databases of the Internet,
such as PubMed, the Food and Drug Administration, the European
Medicines Agency, State Expert Center of the Ministry of Health of
Ukraine were used. The retrospective, logical, and graphical methods
of research, as well as the content analysis were applied. Results: One
of the main problems of antineoplastic drugs authorization is often
significant uncertainty about the degree of clinical benefit of new drugs
when entering the market. In order to improve the quality of clinical
research in the authorization of antineoplastic drugs, post-marketing
studies with clinically significant endpoints and a representative
composition of participants, pharmacovigilance, are of great importance. Within clinical
research, endpoints should be clinically relevant, sensitive to therapy, well measurable and
interpretable. A comprehensive evaluation of performance indicators allows an adequate
assessment of the ratio of the expected benefit to the possible risk of using antineoplastic
drugs. The introduction of a patient-centered logistics approach, including the use of modern
information technologies, social networks, crowdsourcing, patient self-education,
personalized medicine in clinical trials of antineoplastic drugs also contributes to improving
their quality during authorization. Conclusions: The analysis of the most acceptable
endpoints and the use of a patient-centered logistics approach is becoming increasingly
WORLD JOURNAL OF PHARMACY AND PHARMACEUTICAL SCIENCES
SJIF Impact Factor 7.632
Volume 10, Issue 7, 22-37 Research Article ISSN 2278 – 4357
*Corresponding Author
Dr. Elena Litvinova
Department of Management,
Economy and Quality
Assurance in Pharmacy,
National University of
Pharmacy of the Ministry of
Health of Ukraine, Kharkiv,
Ukraine.
Article Received on
26 April 2021,
Revised on 16 May 2021,
Accepted on 06 June 2021
DOI: 10.20959/wjpps20217-19279

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
23
Litvinova et al. World Journal of Pharmacy and Pharmaceutical Sciences
important in clinical trials of antineoplastic drugs, contributing to an increase in the efficiency
and quality of research.
KEYWORDS: quality assurance, patient-centered logistics approach, clinical trials,
antineoplastic drugs.
INTRODUCTION
Cancers occupy a significant place in the structure of morbidity and mortality of the
population, being the cause of 15% of all deaths in the world. Cancer ranks second in the
global mortality pattern, and first in a number of economically developed countries. In 2018,
9.6 million people in the world died of cancer. Overall, 70% of malignant deaths occur in
low- and middle-income countries, where mortality is 75%, compared with 46% in high-
income countries.[1]
Due to the aging population and the prevalence of risk factors (obesity, smoking, poor
nutrition, etc.), the incidence of oncopathology is increasing. In 2012, 14.1 million cases were
diagnosed in the world, in 2018 – 18.1 million, in 2030 21.4 million cases are predicted, and
by 2035 the incidence of cancer may double compared to 2012. The fastest increase in
incidence is predicted in low- and middle-income countries, which currently account for 60%
of first-time diagnosed cancers and only 5% of global economic spending.[2-4]
The results of
the University College and Health Data Research Centre study suggest that COVID-19 can
also increase mortality by 20% in first-time diagnosed oncopathology.[5]
According to the updated data of the National cancer registry of Ukraine in 2018, 137,968
new cases of oncopathology were identified, the crude rate was 384.7 per 100 000 of
population. The crude rate was 381.4 per 100 000 of population in 2017, 349.5 per 100 000
of population in 2016. Statistics show that the incidence increases from year to year. It should
also be noted that the world standardized rate is 225.0 per 100 000 of population, while in
Ukraine this rate is 350.9, respectively.[6]
Thus, the problem of oncology is one of the most relevant problems of the healthcare system
and Ukraine as a whole. Reasons for the high morbidity and mortality are the late diagnosis
and inaccessibility of modern antineoplastic drugs, a long period of clinical trials, the lack of
an individual approach to cancer patients.

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
24
Litvinova et al. World Journal of Pharmacy and Pharmaceutical Sciences
Cancer control is one of the priority areas of health care around the world. According to the
United Nations Sustainable Development Goals, cancer mortality is planned to be reduced by
one third by 2030. To achieve this goal, it is necessary to provide all patients with high-
quality medical care, including high-quality, effective, safe and economically affordable
medicines, which play a significant role in improving prognosis.[7]
Antineoplastic drugs are one of the largest groups of newly registered medicines. According
to a report by the European Medicines Agency (EMA), more than 25% of drugs approved in
2017 are antineoplastic drugs.[8]
According to a report by Center for Drug Evaluation and
Research (CDER, USA), in 2019, 48 innovative medicines were recommended for use, of
which 11 were antineoplastic drugs.[9]
This is primarily due to the high level of morbidity and
mortality in the world from cancers, the concentration of efforts of world organizations,
scientists, manufacturers in this direction, and scientific breakthroughs in the field of studying
the tumor process.
Despite this, the problem of deficiency of effective antineoplastic agents remains in the
world. This precedent created the conditions for introducing approaches to the global
regulatory practice, which are aimed at reducing the time for registration of medicines.[10]
The approaches of the regulatory authorities of the USA, the European Union, despite some
differences, share a common objective of accelerated approval of drugs that fill an unmet
medical need. One of the main problems of antineoplastic drugs authorization is often
significant uncertainty about the degree of clinical benefit of new drugs when entering the
market. The simplified authorization procedure is introduced in Ukraine for medicinal
products registered by competent authorities of the United States of America, Switzerland,
Japan, Australia, Canada and medicinal products registered via the centralized procedure by
the European Union competent authority. In the case of providing an opinion on registration,
the Ministry of Health within 7 working days decides on the state registration of medicines or
the refusal of the approved order of the Ministry of Health.
A huge number of scientific works are devoted to the problems of creating and
implementation of antineoplastic drugs into medical practice. Fundamental theoretical and
practical aspects of the quality of clinical research and their authorization are considered in
the works of many scientists, in particular, Peter B.Bach,[11]
Nathan Cherny,[12]
Melina
Arnold,[13]
Ushkalova E.A,[14]
etc.
www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
25
Litvinova et al. World Journal of Pharmacy and Pharmaceutical Sciences
In addition, in some cases there is insufficient clinical effectiveness, high toxicity of
antineoplastic drugs. These circumstances, despite a wide range of extensive research, require
improving the quality of clinical research, taking into account the logistics approach to the
patient, using in some cases a simplified registration procedure in accordance with the
adopted legislation and implementation new antineoplastic drugs.[15,16]
One of the main problems of antineoplastic drugs authorization is often significant
uncertainty about the degree of clinical benefit of new medicine when entering the market. In
oncology, new medicines and new indications are often approved in earlier stages of
development based on surrogate endpoint data or data from non-randomized studies, which
may lead to a reassessment of clinical benefit. Although this is largely due to the desire to
facilitate rapid access to promising treatments in the area of unmet medical need.
The aim of the work is to analyze and summarize existing scientific approaches and
mechanisms for fast-track approvals, improving the quality of antineoplastic drugs clinical
trials using a patient-centered logistics approach.
MATERIALS AND METHODS
Studies were conducted using databases on the Internet: PubMed; Food and Drug
Administration, the European Medicines Agency, State Expert Center of the Ministry of
Health of Ukraine. The retrospective, logical, and graphical methods of research, as well as
the content analysis were applied.
RESULTS AND DISCUSSION
The high level of antineoplastic drugs authorization is associated with scientific
breakthroughs in the field of oncology research and the expectations of patients for whose
diseases today there is no effective therapy. The FDA, EMA and other regulators allow for
some medicines to have fast-track approvals to get to patients earlier. Antineoplastic drugs
are registered under a simplified protocol more often than medicines of other groups.
Table 1 shows the elapsed time between date of first marketing authorization (out of the
sample countries) and marketing authorization in subsequent countries/regions for each
product/indication pair in the sample approved since 2014 (n = 31). Among 31 new
product/indication pairs in the sample approved since 2014, 26 obtained their first marketing
authorization in the United States, while 4 were first approved in Japan and 1 in Switzerland.

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
26
Litvinova et al. World Journal of Pharmacy and Pharmaceutical Sciences
All European countries except Switzerland have been grouped into the European Economic
Area (EEA) as marketing authorization is centralized for oncology products. On average,
products and indications were approved in individual countries/regions 12 to 17 months after
their first marketing authorization in the sample of countries surveyed (range 2 to 52 months
for individual pairs).[17]
Table 1: Time between first marketing authorization and marketing authorization in
subsequent countries/regions for product/indications approved since 2014 (n=31 pairs).
Indication Active
pharmaceutical
ingredient
First marketing
approval
Time since first marketing approval and
subsequent approval in each country/region in
months (number of pairs approved, with
information on dates1)
Country Date USA
(31)
EEA
(29)
JPN
(25) ISR
2
(20)
CHE
(25)
KOR
(21)
CHL (9)
Metastatic
breast cancer
Abemaciclib USA Sep-17 0 12 12 15 20 20 27
Olaparib USA Dec-14 0 52 43 b 13 8 a
Palbociclib USA Feb-15 0 21 31 b 23 18 b
Ribociclib USA Mar-17 0 5 a b 7 a b
Talazoparib USA Oct-18 0 8 a a a a a
Non-small
cell lung
cancer
Alectinib JPN Sep-15 3 17 0 7 16 13 c
Atezolizumab USA May-16 0 16 20 13 12 8 9
Brigatinib USA Apr-17 0 19 a 19 a 19 a
Ceritinib USA Apr-14 0 13 23 13 16 9 8
Dacomitinib USA Sep-18 0 7 4 a 11 a a
Durvalumab USA May-17 0 16 14 9 13 19 a
Lorlatinib JPN Sep-18 2 8 0 a a a a
Necitumumab USA Nov-15 0 3 43 17 a a a
Nivolumab USA Dec-14 0 10 12 3 11 3 12
Osimertinib USA Nov-15 0 3 4 6 8 6 31
Pembrolizumab USA Oct-15 0 9 14 c 16 c c
Ramucirumab USA Apr-14 0 21 26 25 9 12 12
Colorectal
cancer
Nivolumab USA Dec-14 0 a a 3 11 3 12
Pembrolizumab USA Sep-14 0 a 51 5 29 6 a
Ramucirumab USA Apr-14 0 21 25 25 18 12 12
Trifluridine /
Tipiracil
JPN Mar-14 18 25 0 a 41 a a
Melanoma Binimetinib USA Jun-18 0 3 7 a a a a
Cobimetinib CHE Aug-15 3 3 a 10 0 3 8
Encorafenib USA Jun-18 0 3 7 b a a a
Nivolumab JPN Jul-14 5 11 0 8 16 8 b
Pembrolizumab USA Sep-14 0 10 24 5 29 6 b
Talimogene
Laherparepvec
USA Oct-15 0 2 A 28 9 a a
Multiple
myeloma
Daratumumab USA Nov-15 0 6 22 14 13 24 b
Elotuzumab USA Nov-15 0 6 10 10 13 12 b

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
27
Litvinova et al. World Journal of Pharmacy and Pharmaceutical Sciences
Ixazomib USA Nov-15 0 12 16 9 15 20 a
Panobinostat USA Feb-15 0 6 5 a 10 24 b
Average length of time per country/region for
pairs studied
1 12 17 15 15 12 15
Median length of time per country/region for
pairs studied
0 10 14 13 13 12 12
Note: a = product/indication pair not approved (or not launched); b = product/indication pair
approved but marketing authorization date not provided; c = no data provided for that
product/indication pair
All European countries except Switzerland have been grouped as marketing authorization in
the European Economic Area (EEA) is centralized for oncology products. Australia did not
provide data on dates.
1. Israel and Chile provided information on dates only for a subset of product/indication
pairs indicated as “approved and covered”
2. For products with several indications, data represent product-level dates only. Indication-
specific dates are not available. Source: Authors based on 2019 OECD survey on
challenges in access to oncology medicines.
Globally, between 2013 and 2017, 45 new oncology drugs entered the market, many of them
approved for multiple indications or for use within a combined therapy regimen. The number
of approved indications increased by 265 to 935 during this period, an average of five
indications per new active substance. In 2018, 75% of targeted therapies were used in
multiple indications.[17]
The use of medicines outside the indications approved by the regulator (“off-label use”) is
very common in cancer. Because oncology remains a therapeutic area of high unmet need,
prescribers and patients are often willing to accept the use of medicines in circumstances in
which their efficacy and safety profiles have not yet been clearly established.[18,19]
Thus, significant progress has been made in recent years in the prevention and treatment of
certain forms of cancer, for example, cancer of the esophagus, stomach, pancreas, lung,
ovarian and colorectal cancer, but the implementation of new methods of prevention and
therapy, especially in low- and middle-income countries, which include Ukraine, limited by
their high cost, including the high price of antineoplastic drugs.

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
28
Litvinova et al. World Journal of Pharmacy and Pharmaceutical Sciences
We have established that antineoplastic drugs authorization in Ukraine is most often carried
out according to the following types: full application; generic, hybrid or similar biological
application, accelerated approval of drugs. According to the Report of the State Expert Center
of the Ministry of Health of Ukraine, a nosological group – oncology (it has been registered
56 drugs) is leading among registered medicines in Ukraine in 2020. It was established that
among them there are no original domestic medicines. The percentage of registered generic
domestic antineoplastic drugs of their total number in the pharmaceutical market of Ukraine
is 4%. The analysis also revealed that the largest number of foreign antineoplastic drugs was
registered by groups: alkylating compounds, antimetabolites.
Table 2 shows the data of analysis and systematization of clinical data on the effectiveness of
antineoplastic drugs, which are registered according to the accelerated procedure abroad.
Table 2: Analysis and systematization of clinical data on the effectiveness of
antineoplastic drugs, which are registered according to the accelerated procedure
abroad.
Type of study Result
Meta-analysis, 2019 Analysis of surrogate validation studies (n=78), it has been found most
surrogates in oncology had low or modest correlation with overall
survival, which suggests that caution should be used when making
conclusions based on surrogate markers[20]
Review of FDA
(1992-2017)
The FDA published a review of 93 cancer drug indications for which
accelerated approval was granted from 1992, through 2017.
Confirmatory trials for 19 of 93 (20%) cancer drug approvals reported an
improvement in overall survival, 19 (20%) reported improvement in the
same surrogate used in the preapproval trial, and 20 (21%) reported
improvement in a different surrogate. Confirmatory trials for one-fifth
(n = 19 of 93) of cancer drug indications approved via the FDA’s
accelerated approval pathway demonstrated improvements in overall
patient survival[21]
Review of
antineoplastic drugs
that are approved,
FDA 2009-2017, and
EMA through 2018
The study cohort included 63 drugs approved by the FDA and the EMA
during the study period. 46 (73%) were approved for solid tumors, and
17 (27%) were approved for hematologic malignancies. Overall, median
cancer drug prices in included European countries were 52% lower than
US prices. There was no statistically significant association between
monthly treatment cost and ASCO-VF or ESMO-MCBS scores in any
country. There was also no association between price differential
between US and median European drug prices and either ASCO-VF or
ESMO-MBCS scores. Thus, cancer drug prices in the US were
significantly higher than in the compared European countries. Drug
prices of cancer drugs were not associated with clinical benefit in the US
or in European countries[22]

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
29
Litvinova et al. World Journal of Pharmacy and Pharmaceutical Sciences
This data suggest that most surrogates in oncology had low or modest correlation with overall
survival, which suggests that caution should be used when making conclusions based on
surrogate markers.
In addition, ensuring the economic accessibility of antineoplastic drugs is currently one of the
main tasks of international organizations in the field of oncology. Potential ways to address
the challenges associated with high prices of new cancer medicines, and at times limited
health gain versus current standards, could include agreeing among European authorities
what is meant by a “meaningful clinical benefit” for a new cancer medicine. Ferguson and
colleagues in the United Kingdom suggested that no premium should be paid for a new
cancer medicine unless it prolonged survival by at least three months compared with existing
standards. There were similar timescales for deliberations regarding the value of new
medicines at the end of life in the United Kingdom. The American Society of Clinical
Oncology Cancer Research Committee recently identified an improvement in median overall
survival in a range of 2.5-6 months across a range of tumors as the minimum incremental
improvement that would define a clinically meaningful outcome for a new cancer medicine
(extent would depend on the tumor type).[23,24]
By order No. 593 of the Ministry of Health of Ukraine of March 29, 2021, the guideline for
state assessment of medical technologies for medicines was approved. According to the
guideline, the methodological quality of each study included in the target-analysis or
systematic examination should be assessed, since this affects the reliability and validity of the
test data. Assessment of the quality of any study should take into account: compliance of the
study design with the research goal; risk of bias (due to improperly planned study design or
data collection, analysis, interpretation, publication or inspection); other issues related to the
quality of the study; selection of the result measurement tool statistical analysis issues;
quality of primary source reporting; quality of intervention; general conclusion. Based on
expert opinions and recommendations, medical technology is selected for the appropriate
treatment regimen, which will be the most clinically effective, safe and cost-effective and
will cover the most patients to address unmet needs.
Among the main measures aimed at ensuring the economic accessibility of antineoplastic
drugs is the wider implementation of generics and biosimilars into medical practice,[25]
and
their fast-track approvals in accordance with the law.
www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
30
Litvinova et al. World Journal of Pharmacy and Pharmaceutical Sciences
Analysis and systematization of data on current requirements for antineoplastic drugs
authorization in Ukraine found that post-marketing studies with clinically significant
endpoints and representative composition of participants, pharmacovigilance, are of great
importance.
Analysis of problems related to selection of the most acceptable endpoints of clinical
effectiveness of antineoplastic drugs has been carried out. It is shown that currently the
criteria for assessing the clinical effectiveness of antineoplastic drugs are “patient- centered”
(overall survival and quality of life) and “tumor- centered” (response to therapy, progression-
free survival, disease-free survival) endpoints.[26]
The overall survival score as the primary endpoint is the “gold standard” demonstrating the
clinical efficacy of antitumor therapy for patients. The FDA recognized this indicator as a
universal criterion for assessing clinical efficacy and the best endpoint for phase III clinical
trials. Predicting the exact life expectancy for an individual patient is an extremely difficult
task. To assess survival, doctors use statistics obtained from clinical studies in which a large
number of patients with certain types and stages of tumors participated.
In clinical studies of antineoplastic drugs, particular importance is given to the indicator of
quality of life of patients assessing the subjective response to treatment with the help of
special questionnaires, which are completed during treatment.
Currently, in oncology practice, the use of a “tumor-oriented” clinical endpoint has acquired
relevance – progression-free survival, which has an earlier time frame for evaluating efficacy
and reduced impact of further therapy regimens. As a rule, this term refers to the period of
time from the moment of randomization to the moment of tumor recurrence or death for any
reason after receiving antitumor therapy.
In studies, the indicator of disease progression is defined differently: as clinical or
radiological progression (criteria for assessing the response of solid tumors RECIST,
Response Evaluation Criteria In Solid Tumors, take into account linear sizes of neoplasms) or
as laboratory measurements of progression, which makes it difficult to compare the results.
Subjective response rate is assessed by change in status, reduction or disappearance of
disease symptoms (particularly pain), and change in body weight. Perfomance status is
assessed before the start of treatment, during treatment and after its completion according to

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
31
Litvinova et al. World Journal of Pharmacy and Pharmaceutical Sciences
the WHO 5-stage system (ECOG-WHO, Eastern Cooperative Oncology Group - World
Health Organization).
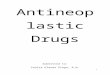
The characteristics of the recommended endpoints of clinical effectiveness of antineoplastic
drugs,[26]
including the advantages and disadvantages of using a particular indicator, as well
as the requirements for its evaluation, are systematized and presented in Figure 1.
Criteria for assessing the clinical effectiveness of antineoplastic drugs
Should be: clinically relevant, sensitive to therapy, well-measurable and interpreted
“Patient- Centered” endpoints
Direct Clinical Efficacy
“Tumor-centered” endpoints
Indirect clinical efficacy
Overall survival
(beginning of study - death)
Time from the start of the
study (randomization,
patient inclusion, drug
initiation, etc.) to death from
any cause.
Need a large patient
population and long-term
follow-up
Quality of life
Reduce study duration and be
able to assess clinical benefit
The criterion is subjective,
characterized by insufficiency
of data and lack of
standardized approaches for
analysis and presentation of
results
Evaluation of treatment
response with validated
questionnaires:
to determine quality of life -
QLQ-C30 EORTC
for functional evaluation of
antitumor therapy - FACT
Rotterdam Symptom Checklist
- RSCL
Functional Living Index-
Cancer - FLIC
Progression-free
survival
Earlier timing of
effectiveness
assessment while
reducing exposure
to detailed therapy
regimens
Time from the
start of the study
(randomization,
patient inclusion,
drug initiation,
etc.) to the
progression of
disease or death
from any cause.
Objective
response
Ability to change
or stop therapy in
a timely manner if
it is ineffective
The time from the
start of the study
(randomization,
patient inclusion,
drug initiation,
etc.) to the
objective
progression of
tumor growth
does not include
death.
Subjective
response
EGOS Status
Change
Disappearance of
disease symptoms
Body Weight
Change
Figure 1: Recommended endpoints of clinical efficacy of antineoplastic drugs.[26]
Therefore, “patient-centered” endpoints allow an assessment of the direct clinical benefit of
chemotherapy in patients, while “tumor- centered” endpoints that do not directly reflect the
clinical benefit to patients allow an assessment of efficacy at earlier stages. The analysis of
the most acceptable endpoints in order to interchange the primary criterion of effectiveness
(overall survival) is becoming increasingly relevant in oncology. The selection of clinical
efficacy criteria should take into account the characteristics of cancer, the study population
and the duration of therapy.
In recent decades, the use of a patient-centered logistics approach as a means of improving
the effectiveness of early and late phases of clinical research has gradually become

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
32
Litvinova et al. World Journal of Pharmacy and Pharmaceutical Sciences
increasingly popular, in particular by increasing the likelihood of success of the study and
obtaining patients with more effective and safe therapy.[27,28]
Thus, the patient-centered logistics approach focuses on the patient as the most important link
in clinical research. The service for delivering everything necessary to the patient is the main
and extremely necessary service in the field of clinical research. Deliveries can be performed
in various variations, depending on the requirements of the Sponsor, the storage temperature
of the drug, urgency, etc. Delivery of medicines directly to the patient helps to reduce the
number of visits, and also helps to reduce the research budget as a whole. To date,
temperature-controlled deliveries directly to the patient are simply necessary for clinical
research. The possibility of direct deliveries to the patient becomes a requirement of sponsors
when starting mainly studies. At the same time, a logistics chain must be built with
temperature control, storage of the drug, urgency, etc.
The pandemic COVID-19 highlighted the need to optimize logistical processes. After all, the
patient can participate in a clinical trial without leaving home. There is no need for travel or
forced visits to medical facilities – even for the preparation of initial documentation. This
flexible approach enables the patient to act. According to experts, there will be a “hybrid”
approach that will combine remote communication with patients along with their trips to the
nearest medical institutions.[29]
Ways to improve clinical research, based on a patient-centered logistics approach, also
include using open channels of communication between the company, doctors, patients and
the media, increasing the focus on education, attracting and maintaining patients through
technology. So, the FDA launched Project Patient Voice, an initiative of the FDA’s Oncology
Center of Excellence (OCE). The pilot phase of the project currently underway is limited to
one clinical trial (an open randomized phase III trial that would compare TAGRISSO
(osimertinib) with platinum-based doublet chemotherapy in patients with lung cancer). The
goal is to get feedback from the public about the practical aspects of using the resource.
Patient Voice is an online platform for patients, caregivers, and healthcare providers to
familiarize them with symptoms reported by clinical trial participants. These data are
generally not available in U.S. medicine prescribing information (instructions), but may
provide additional information for healthcare professionals to discuss with patients and
caregivers.[30]
www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
33
Litvinova et al. World Journal of Pharmacy and Pharmaceutical Sciences
Oncological diseases of the same type are characterized by significant differences in the
genetic composition and features of each patient. In the clinic, this variation results in patients
responding differently to therapy. To address this issue, the realm of personalized medicine
aims to combine genetic perceptions of cancers with other clinical and diagnostic information
to identify patterns that may allow clinicians to predict patients’ response to therapy and
select the most effective interventions.
Researchers from Queen Mary University of London have developed a machine learning
algorithm that ranks drugs based on their efficacy in reducing cancer cell growth. The
approach may have the potential to advance personalized therapies in the future by allowing
oncologists to select the best drugs to treat individual cancer patients. The method, named
Drug Ranking Using Machine Learning (DRUML), is based on machine learning analysis of
data derived from the study of proteins expressed in cancer cells. Having been trained on the
responses of these cells to over 400 drugs, DRUML predicts the best drug to treat a given
cancer model.[31]
Thus, the implementation of a patient-centered logistics approach is widely used in oncology.
The pharmaceutical industry, faced with significant organizational and financial challenges,
is looking for ways to improve the effectiveness and quality of clinical research.
CONCLUSIONS
1. Analysis of domestic and foreign literature shows that oncological diseases occupy a
significant place in the structure of morbidity and mortality of the population, being the
cause of 15% of all deaths in the world. In Ukraine, the problem of oncology is also one
of the most pressing problems of the healthcare system.
2. The approaches of the regulatory authorities of the USA, the European Union, despite
some differences, share a common objective of accelerated approval of drugs that fill an
unmet medical need. One of the main problems of antineoplastic drugs authorization is
often significant uncertainty about the degree of clinical benefit of new drugs when
entering the market. Antineoplastic drugs are registered under a simplified protocol more
often than medicines of other groups.
3. In order to improve the quality of clinical research in the authorization of antineoplastic
drugs, post-marketing studies with clinically significant endpoints and a representative
composition of participants, pharmacovigilance, are of great importance. Within clinical
research, endpoints should be clinically relevant, sensitive to therapy, well measurable

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
34
Litvinova et al. World Journal of Pharmacy and Pharmaceutical Sciences
and interpretable. A comprehensive evaluation of performance indicators allows an
adequate assessment of the ratio of the expected benefit to the possible risk of using
antineoplastic drugs.
4. The introduction of a patient-centered logistics approach, including the use of modern
information technologies, social networks, crowdsourcing, patient self-education,
personalized medicine in clinical trials of antineoplastic drugs also contributes to
improving their quality during authorization. The implementation of patient-centered
logistic strategies of clinical trials increases the level of patient satisfaction, loyalty and
preferences.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
REFERENCES
1. Latest global cancer data: The International Agency for Research on Cancer. WHO, 2018.
Press Releasen° 263. Available at : https://www.iarc.who.int/wp-
content/uploads/2018/09/pr263_E.pdf
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics
2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185
countries. CA: A Cancer Journal for Clinicians, 2018; 68(6): 394-424.
https://doi.org/10.3322/caac.21492
3. Soerjomataram I, Lortet-Tieulent J, Parkin DM, Ferlay J, Mathers C, Forman D, Bray F.
Global burden of cancer in 2008: A systematic analysis of disability-adjusted life-years in
12 world regions. The Lancet, 2012; 380(9856): 1840-1850.
https://doi.org/10.1016/S0140-6736(12)60919-2
4. Prager GW, Braga S, Bystricky B, Qvortrup C, Criscitiello C, Esin E, Sonke GS,
Martínez G, Frenel JS, Karamouzis M, Strijbos M, Yazici O, Bossi P, Banerjee S, Troiani
T, Eniu A, Ciardiello F, Tabernero J, Zielinski CC. Global cancer control: Responding to
the growing burden, rising costs and inequalities in access. ESMO Open, 2018; 3(2):
e000285. https://doi.org/10.1136/esmoopen-2017-000285
5. COVID-19 mozhet na 20% povyisit smertnost pri vpervyie diagnostirovannoy
onkopatologii v Anglii. Apteka, 2020; 17(18): 1238-1239. Available at :
https://www.apteka.ua/article/545630

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
35
Litvinova et al. World Journal of Pharmacy and Pharmaceutical Sciences
6. Natsionalniy kantser-reestr Ukrayini, 2020. Available at :
http://www.ncru.inf.ua/publications/ucr_data_2020.pdf
7. Transforming our world: the 2030 Agenda for Sustainable Development. 2015. Available
at : https://sustainabledevelopment.un.org/post2015/transformingourworld
8. Annual Report EMA, 2017. Available at :
https://www.ema.europa.eu/en/documents/annual-report/2017-annual-report-european-
medicines-agency_en.pdf
9. Impact innovation predictability access FDA’s center for drug evaluation and research,
New Drug Therapy Approvals, 2019. Available at : https://www.fda.gov/drugs/new-
drugs-fda-cders-new-molecular-entities-and-new-therapeutic-biological-products/new-
drug-therapy-approvals-2019
10. Goryachev DV, Uvarova NE, Shukshina GV. Marketing Authorisation Based on
Incomplete Clinical Data: International Experience and Prospects. The Bulletin of the
Scientific Centre for Expert Evaluation of Medicinal Products, 2020; 10(3): 152-163.
https://doi.org/10.30895/1991-2919-2020-10-3-152-163
11. Bach P. Price & Value of Cancer Drugs, 2019. Available at :
https://www.mskcc.org/research-programs/health-policy-outcomes/cost-drugs
12. Cherny NI, Sullivan R, Dafni U, Kerst JM, Sobrero A, Zielinski C, de Vries EGE, Piccart
MJ. A standardised, generic, validated approach to stratify the magnitude of clinical
benefit that can be anticipated from anti-cancer therapies: The European Society for
Medical Oncology Magnitude of Clinical Benefit Scale (ESMO-MCBS). Annals of
Oncology: Official Journal of the European Society for Medical Oncology, 2015; 26(8):
1547-1573. https://doi.org/10.1093/annonc/mdv249
13. Arnold M, Rutherford MJ, Bardot A, Ferlay J, Andersson TML, Myklebust TÅ, Tervonen
H, Thursfield V, Ransom D, Shack L, Woods RR, Turner D, Leonfellner S, Ryan S,
Saint-Jacques N, De P, McClure C, Ramanakumar AV, Stuart-Panko H. Progress in
cancer survival, mortality, and incidence in seven high-income countries 1995-2014
(ICBP SURVMARK-2): A population-based study. The Lancet. Oncology, 2019; 20(11):
1493-1505. https://doi.org/10.1016/S1470-2045(19)30456-5
14. Ushkalova EA, Zyryanov SK, Gopienko IA. Economic challenges of oncological
diseases’ pharmacotherapy. Farmakoekonomika. Modern pharmacoeconomic and
pharmacoepidemiology, 2020; 13(1): 64-70. https://doi.org/10.17749/2070-
4909.2020.13.1.64-70

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
36
Litvinova et al. World Journal of Pharmacy and Pharmaceutical Sciences
15. Bach PB. Indication-specific pricing for cancer drugs. JAMA, 2014; 312(16): 1629–1630.
https://doi.org/10.1001/jama.2014.13235
16. Cherny N, Sullivan R, Torode J, Saar M, Eniu A. Corrigendum to “ESMO European
Consortium Study on the availability, out-of-pocket costs and accessibility of
antineoplastic medicines in Europe.” Annals of Oncology, 2020; 31(11): 1589.
https://doi.org/10.1016/j.annonc.2020.09.002
17. Addressing challenges in access to oncology medicines. 2020. Available at :
https://www.oecd.org/health/health-systems/Addressing-Challenges-in-Access-to-
Oncology-Medicines-Analytical-Report.pdf
18. 18. Global Oncology Trends. 2019 Available at : https://www.iqvia.com/insights/the-
iqvia-institute/reports/global-oncology-trends-2019
19. Saiyed MM, Ong PS, Chew L. Off-label drug use in oncology: A systematic review of
literature. Journal of Clinical Pharmacy and Therapeutics, 2017; 42(3): 251-258.
https://doi.org/10.1111/jcpt.12507
20. Haslam A, Hey SP, Gill J, Prasad V. A systematic review of trial-level meta-analyses
measuring the strength of association between surrogate end-points and overall survival
in oncology. European Journal of Cancer, 2019; 106: 196-211.
https://doi.org/10.1016/j.ejca.2018.11.012
21. Gyawali B, Hey SP, Kesselheim AS. Assessment of the Clinical Benefit of Cancer Drugs
Receiving Accelerated Approval. JAMA Internal Medicine, 2019; 179(7): 906-913.
https://doi.org/10.1001/jamainternmed.2019.0462
22. Vokinger KN, Hwang TJ, Tibau A, Rosemann T, Kesselheim AS. Clinical Benefit and
Prices of Cancer Drugs in the United States and Europe. Journal of Clinical Oncology,
2019; 37 (15): 6638–6638. https://doi.org/10.1200/JCO.2019.37.15_suppl.6638.
23. Ferguson JSJ, Summerhayes M, Masters S, Schey S, Smith IE. New treatments for
advanced cancer: An approach to prioritization. British Journal of Cancer, 2000: 83(10):
1268-1273. https://doi.org/10.1054/bjoc.2000.1406
24. Access to new medicinesin Europe: technical review of policy initiatives andopportunities
forcollaboration and research. WHO. 2015. Available at :
https://www.euro.who.int/__data/assets/pdf_file/0008/306179/Access-new-medicines-
TR-PIO-collaboration-research.pdf
25. Gopienko IA, Ushkalova EA, Zyryanov SK. Generics and biosimilars in oncology.
Kachestvennaya klinicheskaya praktika. 2019; 4: 15-22.

www.wjpps.com │ Vol 10, Issue 7, 2021. │ ISO 9001:2015 Certified Journal │
37
Litvinova et al. World Journal of Pharmacy and Pharmaceutical Sciences
26. Tikhomirova AV. Criteria for Evaluation of Clinical Efficacy of Anticancer Medicines.
The Bulletin of the Scientific Centre for Expert Evaluation of Medicinal Products, 2019;
9(1): 34–40. https://doi.org/10.30895/1991-2919-2019-9-1-34-40
27. Sharma N. Patient centric approach for clinical trials: Current trend and new
opportunities. Perspectives in Clinical Research, 2015; 6(3): 134.
https://doi.org/10.4103/2229-3485.159936
28. 28. Dehtiarov O, Fesenko A. 2020 Practical and legal aspects of patient-centered
logistics of clinical trials. Available at https://www.dec.gov.ua/materials/presentations-of-
the-sixth-scientific-practical-conference-with-international-participation-clinical-trials-of-
medicinal-products-in-ukraine-new-challenges-and-responses-to-them-october-8/
29. Detsentralizovani klinichni doslidzhennya: shlyah do modernizatsiyi Farmi. Apteka,
2021; 14 (1285). Available at : https://www.apteka.ua/article/590721.
30. «Golos patsienta» – novyiy proekt FDA v sfere onkologii. Apteka, 2020; 23(24): 1244-
1245. Available at : https://www.apteka.ua/article/552583
31. Gerdes H, Casado P, Dokal A, Hijazi M, Akhtar N, Osuntola R, Rajeeve V, Fitzgibbon J,
Travers J, Britton D, Khorsandi S, Cutillas PR. Drug ranking using machine learning
systematically predicts the efficacy of anti-cancer drugs. Nature Communications, 2021;
12(1): 1850. https://doi.org/10.1038/s41467-021-22170-8