Embed Size (px)
Citation preview

http://www.diva-portal.org
This is the published version of a paper published in Antimicrobial Agents and Chemotherapy.
Citation for the original published paper (version of record):
Stylianou, M., Kulesskiy, E., Lopes, J., Granlund, M., Wennerberg, K. et al. (2014)
Antifungal Application of Nonantifungal Drugs.
Antimicrobial Agents and Chemotherapy, 58(2): 1055-1062
http://dx.doi.org/10.1128/AAC.01087-13
Access to the published version may require subscription.
N.B. When citing this work, cite the original published paper.
Permanent link to this version:http://urn.kb.se/resolve?urn=urn:nbn:se:umu:diva-86824

Published Ahead of Print 25 November 2013. 10.1128/AAC.01087-13.
2014, 58(2):1055. DOI:Antimicrob. Agents Chemother. UrbanMargareta Granlund, Krister Wennerberg and Constantin F. Marios Stylianou, Evgeny Kulesskiy, José Pedro Lopes, DrugsAntifungal Application of Nonantifungal
http://aac.asm.org/content/58/2/1055Updated information and services can be found at:
These include:
REFERENCEShttp://aac.asm.org/content/58/2/1055#ref-list-1at:
This article cites 56 articles, 15 of which can be accessed free
CONTENT ALERTS more»articles cite this article),
Receive: RSS Feeds, eTOCs, free email alerts (when new
http://journals.asm.org/site/misc/reprints.xhtmlInformation about commercial reprint orders: http://journals.asm.org/site/subscriptions/To subscribe to to another ASM Journal go to:
on March 17, 2014 by U
ME
A U
NIV
ER
SIT
Y LIB
RA
RY
http://aac.asm.org/
Dow
nloaded from
on March 17, 2014 by U
ME
A U
NIV
ER
SIT
Y LIB
RA
RY
http://aac.asm.org/
Dow
nloaded from

Antifungal Application of Nonantifungal Drugs
Marios Stylianou,a,b Evgeny Kulesskiy,c José Pedro Lopes,a,b Margareta Granlund,a Krister Wennerberg,c Constantin F. Urbana,b
Department of Clinical Microbiology, Umeå University, Umeå, Swedena; Laboratory for Molecular Infection Medicine, Sweden (MIMS), and Umeå Centre for MicrobialResearch, Umeå University, Umeå, Swedenb; Institute for Molecular Medicine Finland (FIMM), University of Helsinki, Helsinki, Finlandc
Candida species are the cause of 60% of all mycoses in immunosuppressed individuals, leading to �150,000 deaths annually dueto systemic infections, whereas the current antifungal therapies either have toxic side effects or are insufficiently efficient. Weperformed a screening of two compound libraries, the Enzo and the Institute for Molecular Medicine Finland (FIMM) oncologycollection library, for anti-Candida activity based on the European Committee on Antimicrobial Susceptibility Testing(EUCAST) guidelines. From a total of 844 drugs, 26 agents showed activity against Candida albicans. Of those, 12 were standardantifungal drugs (SADs) and 7 were off-target drugs previously reported to be active against Candida spp. The remaining 7 off-target drugs, amonafide, tosedostat, megestrol acetate, melengestrol acetate, stanozolol, trifluperidol, and haloperidol, wereidentified with this screen. The anti-Candida activities of the new agents were investigated by three individual assays using opti-cal density, ATP levels, and microscopy. The antifungal activities of these drugs were comparable to those of the SADs found inthe screen. The aminopeptidase inhibitor tosedostat, which is currently in a clinical trial phase for anticancer therapy, displayeda broad antifungal activity against different Candida spp., including Candida glabrata. Thus, this screen reveals agents that werepreviously unknown to be anti-Candida agents, which allows for the design of novel therapies against invasive candidiasis.
The number of immunocompromised patients is increasingworldwide, and these individuals are at high risk for acquiring
severe microbial infections, which are frequently caused by Can-dida spp. (1). Most commonly, cases of bloodstream infectionswith Candida spp. (candidemia) are related to surgery, intensivecare, solid tumors, or hematological malignancies (2). The mor-tality rate that is directly attributable to candidemia ranges from 5to 71%, depending on the clinical cohort (3, 4). Particularly highmortalities occur in patients with solid tumors (65%) and hema-tologic malignancies (46%) (5). Severe mycoses are frequentlycaused by species of the Candida clade, such as C. albicans, C.dubliniensis, and C. glabrata (6, 7). Although these species causesevere invasive infections in immunocompromised persons, theyare also common as part of the commensal flora on mucous mem-branes. C. albicans is the most common human fungal pathogenand is able to switch back and forth from yeast to hyphal growth.This revertible morphogenetic switch plays a key role in the viru-lence of C. albicans (8–10). C. albicans and C. dubliniensis arephylogenetically closely related, sharing a polymorphic and oblig-atory diploid nature (11). However, C. dubliniensis differs in vir-ulence-associated gene families, such as the agglutinin-like se-quences (ALS), which render C. dubliniensis less virulent than C.albicans (12). Nevertheless, C. dubliniensis causes candidemia as-sociated with equally high mortality rates (13). C. glabrata is ahaploid yeast and is often referred to as the second most frequentyeast causing candidemia (7). Importantly, C. glabrata has de-creased in vitro susceptibility against fluconazole. This suggests anincreased risk for C. glabrata infections due to prophylactic flu-conazole treatment of patients at high risk for invasive candidiasis(14).
Despite the urgent requirement for efficient antifungal thera-pies, the available standard antifungal drugs (SADs) are few andhave a restricted set of fungal targets. Polyenes, azoles, allylamines,morpholines, antimetabolites, and echinocandins are the 6 majorantifungal drug categories (15). The first three directly or indi-rectly target ergosterol, a major fungal membrane component.The long-term use of drugs that target ergosterol, such as flucona-
zole or amphotericin B, can result in renal and liver toxicity (16).The following two categories interfere with DNA/RNA synthesis.Antimetabolites are known human carcinogens, causing liver tox-icity and bone marrow depression and thus are less frequentlyused (16, 17). The relatively newly introduced echinocandins in-hibit 1,3-�-glucan synthesis in the cell wall and have few notableside effects. The emergence of echinocandin-resistant isolates,however, is a cause for clinical concern (18). Taken together, thereis a demand for new antifungal substances, preferably those withnovel fungal targets.
The scope of this study was to find previously unknown anti-fungal activities in agents from the Enzo drug library and the In-stitute for Molecular Medicine Finland (FIMM) oncology collec-tion (19). We rationalized that knowledge about antifungalactivity against common human fungal pathogens in off-patentdrugs from the Enzo library should be beneficial to increase thetreatment possibilities for severe mycoses. Moreover, we screenedthe FIMM oncology collection, which contains antineoplasticdrugs, with the purpose of identifying agents that affect both pri-mary immune-suppressive cancer disease and a possible second-ary Candida infection, which occurs frequently in cancer patients.This additional information is beneficial for patients if a choice oftherapy is possible. We performed the screen with C. albicans andconfirmed antifungal activities for 19 drugs that have been previ-ously described for their antimycotic capacities, approving thevalidity of our methods. We identified 7 novel agents previouslyunknown to inhibit the growth of C. albicans (Table 1). Notably,
Received 21 May 2013 Returned for modification 12 July 2013Accepted 22 November 2013
Published ahead of print 25 November 2013
Address correspondence to Constantin F. Urban, [email protected].
Copyright © 2014, American Society for Microbiology. All Rights Reserved.
doi:10.1128/AAC.01087-13
February 2014 Volume 58 Number 2 Antimicrobial Agents and Chemotherapy p. 1055–1062 aac.asm.org 1055
on March 17, 2014 by U
ME
A U
NIV
ER
SIT
Y LIB
RA
RY
http://aac.asm.org/
Dow
nloaded from

the susceptibility of C. albicans to SADs was comparable to theantifungal effect of the seven agents identified in this screen.
MATERIALS AND METHODSDrugs and fungal strains. The in vitro susceptibility of C. albicans strainSC5314 was tested against 844 drugs from the Enzo FDA-approved druglibrary (640 drugs) and the FIMM oncology collection (19) (FDA-ap-proved anticancer drugs [n � 119] and preclinical compounds [n � 85]).Thirteen FDA-approved antifungal drugs, 12 of which were active againstC. albicans SC5314, and five nonantifungal drugs with antifungal activityserved as controls. The screen was performed with C. albicans SC5314,and hits were further confirmed with the type strains C. dubliniensisCD36/CBS7987 and C. glabrata ATCC 90030, as well as with unrelatedclinical strains of C. albicans UBC3-7922, C. glabrata UCB3-7268, and C.dubliniensis UCB-3892 from the strain collection of Norrland’s UniversityHospital, Umeå, Sweden.
Media and antifungal microdilution testing. Cell concentration anddrug microdilution analyses were performed according to the EuropeanCommittee on Antimicrobial Susceptibility Testing (EUCAST) guide-lines, with modifications (20). Candida yeast cells were grown overnightat 30°C with shaking in yeast peptone medium plus 2% glucose (YPD).Subcultures of 107 cells/ml in YPD grew for 4 h at 30°C. Drugs in theamounts of 15 to 150 nl from the Enzo and FIMM oncology collectionswere distributed by a liquid handling platform (Labcyte Echo 550 acousticdispenser) in black 96-well plates with clear bottoms in six different con-centrations from 0.17 nM to 10 �M. Subsequently, 50 �l RPMI 1640 wasadded to each well and the start plates were shaken (30 rpm) prior to theassay for 1 h to ensure equal distribution of the agents within the well. Theyeast suspension, 100 �l of 5 � 105 cells/ml in RPMI 1640 without phenolred, and 10 mM HEPES (Lonza) were transferred to the 96-well platescontaining medium and agents using a robotic device (Matrix WellMate;
Thermo Scientific), resulting in a final volume of 150 �l in each well. Theplates were incubated at 37°C, 5% CO2, for 6 or 24 h.
Determination of fungal growth using absorbance. The growth of C.albicans SC5314 was analyzed using a microdilution plate assay accordingto EUCAST recommendations (20). One-hundred-microliter suspen-sions of yeasts (5 � 105 cells/ml) in RPMI 1640 were incubated in thepresence or absence of drugs in a total volume of 150 �l at 37°C, 5% CO2,for 6 h and 24 h. The optical densities at 450 nm (OD450) in the plates weredetermined using a plate reader (Tecan Infinite F200). ODs of �0.1 for 6h and 0.2 for 24 h for the 100% growth control were considered to repre-sent poor growth and were not taken into account for the evaluation. Asdescribed above, 100% and 0% growth controls were included with everyplate. All assays were performed at least as two biological replicates intriplicate (n � 2 [3]).
Determination of fungal viability using ATP levels. In order to de-termine the viability of the C. albicans, C. glabrata, and C. dubliniensisstrains, the CellTiter-Glo luminescent cell viability kit (Promega) wasused. One hundred-microliter suspensions of yeasts (5 � 105 cells/ml) inRPMI 1640 were incubated in the presence or absence of drugs in a totalvolume of 150 �l at 37°C, 5% CO2, for 6 h and 24 h. An equal volume ofthe CellTiter-Glo reagent was added to the medium and incubated for 15min at room temperature with shaking at 900 rpm. The luminescent sig-nals after 6 h and 24 h were detected using a luminometer (Tecan InfiniteF200). The resulting signal intensity corresponds to ATP amounts andthus to the number of viable microbial cells upon drug exposure. In all96-well plates, 100% and 0% growth controls were included as microbesplus dimethyl sulfoxide (DMSO) (0.1%) and microbes plus benzetho-nium chloride (BzCl) (100 �M), respectively. All assays were performed atleast as two biological replicates in triplicate (n � 2 [3]).
Microscopic analysis of morphological changes occurring upondrug treatment. For a morphological analysis of C. albicans SC5314treated with antifungal agents (1 �M), an IncuCyte automated micro-scope was used (Essen Bioscience). The plates were incubated at 37°Cunder 5% CO2. After the indicated time points, prior to analysis, the fungiwere fixed with 2% paraformaldehyde (PFA) and phase-contrast imageswere captured. In this study, 4 pictures per well were taken from twobiological and three technical replicates.
Statistical and data analysis. Percent growth inhibition (%Inh) wascalculated from the ATP and OD measurements resulting from the meanvalues from all biological replicates, using the equation %Inh � 100 �(valuesample/valuecontrol) � 100. The %Inh values (y axis) were plottedagainst the drug concentration (x axis), and the according trend line of thedose-response curve was defined and the resulting linear equation wasapplied to calculate the MICs using Microsoft Office Excel 2007. The MICwas the lowest drug concentration resulting in �50% growth inhibitioncompared to that of the drug-free control according to the EUCASTguidelines for flucytosine, azole antifungal agents, and echinocandins(20). Additionally, we defined MIC0.3 as the lowest drug concentrationresulting in �30% growth inhibition compared to that of the drug-freecontrol.
The data were analyzed and evaluated from 3 biological replicates intriplicate (n � 3 [3]) (Tables 2 and 3), as well as from 4 biological repli-cates in triplicate (n � 4 [3]) (Table 4). The strains C. dubliniensis CD36/CBS7987 and C. glabrata ATCC 90030 shown in Table 4 were analyzed in2 biological replicates in triplicate (n � 2 [3]). The R2 values for all dose-response curves ranged between 0.87 and 0.92. Additionally, the coeffi-cients of variation (the ratio of the standard deviation to the mean) ex-pressed as a percentage (also referred to as relative standard deviation) forall biological replicates ranged from 13 to 28%.
RESULTSOutline of the study. Our main goal was to identify antifungalactivities in drugs that were designed for other purposes. Twocollection libraries, Enzo and FIMM oncology, comprising a totalof 844 agents, were screened for activity against C. albicans. A
TABLE 1 All drugs with antifungal activity identified in this study(n � 26)
Identified drug
Previouslydescribed asantifungal
Previouslydescribed asanti-Candida
Therapeuticuse
Referenceno. orsource
Haloperidol HCl Yes No Antipsychotic 21, thisstudy
Trifluperidol 2HCl No No Antipsychotic This studyStanozolol No No Anemia,
angioedemaThis study
Melengestrol acetate No No Anticancer This studyMegestrol acetate No No Anticancer This studyTosedostat No No Anticancer This studyAmonafide No No Anticancer This studyMethiothepin
maleateYes Yes Antipsychotic 25
Rapamycin Yes Yes Anticancer 26Auranofin Yes Yes Antirheumatic 27Bleomycin sulfate Yes Yes Anticancer 40Disulfiram Yes Yes Anticancer 41Artemisinin Yes Yes Antimalarial 42Tamoxifen citrate Yes Yes Anticancer 43Tioconazole Yes Yes Antifungal NAa
Oxiconazole nitrate Yes Yes Antifungal NAKetoconazole Yes Yes Antifungal NAClimbazole Yes Yes Antifungal NAMiconazole Yes Yes Antifungal NAMyclobutanil Yes Yes Antifungal NAFluconazole Yes Yes Antifungal NAAmorolfine Yes Yes Antifungal NABifonazole Yes Yes Antifungal NASertaconazole Yes Yes Antifungal NAItraconazole Yes Yes Antifungal NATerbinafine HCl Yes Yes Antifungal NA
a NA, not applicable.
Stylianou et al.
1056 aac.asm.org Antimicrobial Agents and Chemotherapy
on March 17, 2014 by U
ME
A U
NIV
ER
SIT
Y LIB
RA
RY
http://aac.asm.org/
Dow
nloaded from

major challenge for screenings with C. albicans is the characteristicof the fungus to grow as hyphal filaments (8). Filamentation com-plicates assessments of growth using OD, for instance, since thenumber of individual cells does not increase and hyphae tend to
clump excessively. Therefore, we used a luciferase-based quanti-fication of ATP to assess fungal viability. We additionally con-firmed the screening results by quantifying fungal growth usingOD measurements. Both methods resulted in highly comparableresults for all tested drugs.
Seven off-target drugs revealed to have anti-Candida activi-ties. The screen identified a total of 26 agents that are active againstC. albicans (Table 1). Of those, 12 were SADs and 7 were off-targetdrugs with known antifungal activities. Additionally, the screenrevealed 7 drugs from 4 different categories of therapy with pre-viously unidentified potent anti-Candida activities (Table 2). Twoare antipsychotic (haloperidol and trifluperidol), one is used forthe treatment of anemia (stanozolol), and 4 are used for cancertherapy (melengestrol acetate, megestrol acetate, tosedostat, andamonafide). Haloperidol, but not trifluperidol, has previouslybeen identified in a chemical-genetic screen to have antimicrobialactivity against Saccharomyces cerevisiae (21). Four agents areFDA-approved drugs and 2 are anticancer agents (amonafide andtosedostat) that are currently being tested in clinical trials (22, 23).Although it has been applied in animal husbandry, of the identi-fied drugs, only melengestrol acetate is not currently used in hu-mans (24). Moreover, we identified the antipsychotic drug me-thiothepin maleate, which only very recently has been identified ina repurposing screen for anticryptococcal agents (25). We usedthe immunosuppressant drug rapamycin and the antirheumaticdrug auranofin as references for the antifungal activities of thenewly identified agents (Table 2). Interestingly, rapamycin wasoriginally identified as an antifungal agent (26), and gold (I) com-plexes, such as auranofin, have been recognized for their antimi-crobial activities (27).
We determined the MIC and MIC0.3 values for C. albicans byOD and ATP measurements. As mentioned above, the methodsresulted in highly similar values, and thus one value for each agentis presented (Table 2). In general, the MICs were slightly lowerafter 6 h than after 24 h of incubation. However, the activities ofthe 7 compounds against C. albicans were stable over a period of24 h (Table 2). Importantly, in this screen, we did not use concen-
TABLE 2 MIC and MIC0.3 values against Candida albicans type straina
Antifungal agent
This study
Other studiesc
Concn range(�g/ml)
ATP level and OD450b
MIC at: MIC0.3 at:
6 h 24 h 6 h 24 h Cmax (�g/ml) Ref. for Cmax
Haloperidol HCl 6.4 � 10�5 to 3.76 0.38 3.76 0.04 0.35 2.00–3.00 44Trifluperidol 2HCl 7 � 10�5 to 4.00 4.00 4.00 0.40 0.40 UAd UAStanozolol 3.3 � 10�5 to 3.29 3.29 3.29 0.30 0.30 0.007 45Melengestrol acetate 6.8 � 10�5 to 3.97 2.20 3.97 0.40 0.22 0.01 46Megestrol acetate 6 � 10�5 to 3.85 2.10 3.85 0.39 0.40 0.50–0.70 47Tosedostat 4 � 10�3 to 4.00 4.00 4.00 4.00 4.00 0.15 23Amonafide 2.8 � 10�3 to 2.83 2.83 2.83 1.50 2.83 4.00 22Methiothepin maleatee 7 � 10�5 to 3.57 0.35 3.57 0.044 0.25 UA UAAuranofine 1 � 10�4 to 6.78 0.70 0.38 0.007 0.07 6.60 48Rapamycine 1.55 � 10�5 to 9.14 0.001 0.005 1 � 10�5 1 � 10�5 0.01–0.21 49a The data were determined from three biological replicates in triplicate (n � 3 [3]). MIC, minimal concentration of drug resulting in �50% growth inhibition; MIC0.3, minimalconcentration of drug resulting in �30% growth inhibition.b OD450, optical density at 450 nm.c Cmax, plasma peak concentrations reachable in humans upon first dose of the drugs; Ref., literature reference.d UA, unavailable.e The anti-Candida albicans activities of these drugs were demonstrated previously.
TABLE 3 Comparison of SADs with off-target antifungal agentsidentified in this study at a concentration of 1 �Ma
Drugs MIC MIC0.3
Standard antifungalb
Tioconazole 0.39 �g/mlOxiconazole nitrate 0.40 �g/mlKetoconazole 0.50 �g/mlClimbazole 0.29 �g/mlMiconazole 0.40 �g/mlFluconazole 0.30 �g/mlAmorolfine 0.32 �g/mlMyclobutanil 0.29 �g/mlBifonazole 0.30 �g/mlSertaconazole 0.40 �g/mlItraconazole 0.70 �g/mlTerbinafine HCl 1 �MNystatin 1 �M
Off-target antifungalHaloperidol HCl 0.38 �g/mlMethiothepin maleate 0.36 �g/mlAuranofin 0.68 �g/mlTrifluperidol 2HCl 0.40 �g/mlStanozolol 0.30 �g/mlMelengestrol acetate 0.40 �g/mlMegestrol acetate 0.39 �g/mlTosedostat 1 �MAmonafide 1 �M
a SADs, standard antifungal drugs. C. albicans SC5314 was challenged with SADs andantifungal agents identified in this study.b MIC, minimal concentration of drug resulting in �50% growth inhibition; MIC0.3,minimal concentration of drug resulting in �30% growth inhibition. The MIC andMIC0.3 were determined by ATP measurement after 6 h of incubation. Nystatin did notshow any activity against C. albicans SC5314 in this assay. The data are determinedfrom three biological replicates in performed triplicate (n � 3 [3]).
Dual Use of Known Drugs as Antimycotics
February 2014 Volume 58 Number 2 aac.asm.org 1057
on March 17, 2014 by U
ME
A U
NIV
ER
SIT
Y LIB
RA
RY
http://aac.asm.org/
Dow
nloaded from

trations of 10 �M (corresponding to 3 to 10 �g/ml, dependingon the molecular weight of the agent), since in the therapy ofsystemic mycoses, maximal peak blood serum concentrationsabove this level are unlikely to be reached. Haloperidol, trifluperi-dol, stanozolol, melengestrol acetate, and megestrol acetateshowed MIC values of �4 �g/ml. For tosedostat and amonafide,the MIC0.3 values were determined to be 4 and 2.8 �g/ml, respec-tively. All 7 substances displayed a dose-dependent effect on C.albicans SC5314. The antifungal activities of amonafide and tose-dostat (Table 2) increased slowly over a wide concentration range,from approximately 3 � 10�3 �g to 4 �g/ml.
Novel antifungal off-target drugs and SADs have similaranti-Candida activities. We next compared the antifungal activ-ities of the 7 identified agents to 13 established SADs present in theEnzo library. Notably, the novel candidates were inhibitoryagainst C. albicans at a level similar to those of 12 of the SADs at aconcentration of 1 �M, ranging from 0.3 �g to 0.7 �g/ml, depend-ing on individual molecular weights (Table 3). Terbinafine HCl,tosedostat, and amonafide had an MIC0.3 at a concentration of 1�M. At this concentration, nystatin was the only SAD that lackedanti-Candida activity after 6 h. Additionally, five off-target drugswith previously known antifungal activities were also identified inthis screen, confirming that the applied methods were suitable toidentify antifungal activity against C. albicans (Table 5).
Microscopic analysis of morphological changes in C. albicansoccurring upon treatment with newly identified agents. The an-
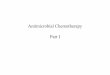
tifungal effects of tosedostat and amonafide were milder thanthose of other drugs (Tables 2 and 3). To verify the possible effectsof the selected agents identified in this study on C. albicans, weadditionally performed a direct microscopic investigation oftreated C. albicans (Fig. 1). DMSO- and BzCl-treated C. albicansserved as 100% and 0% growth controls, respectively (Fig. 1A andB). Haloperidol and trifluperidol (Fig. 1E and G) show a verysimilar effect as fluconazole (Fig. 1C). The hyphae are consider-ably shorter, with the tendency to form branches more frequentlythan with untreated control hyphae. Notably, tosedostat andamonafide (Fig. 1F and H) caused similar morphological changesas those observed in the samples treated with rapamycin (Fig. 1D).The hyphae are significantly shorter, with the germ tubes having acurved shape. The control hyphae, in contrast, are longer andstraight. Thus, our screen identified substances with comparableeffects on C. albicans morphology as the well-known antifungalagent fluconazole or the immunosuppressant drug with antifun-gal activity, rapamycin. This indicates that the identified agentsindeed inhibit the growth of C. albicans.
Confirmation of antifungal activities of identified drugs onclinical isolates from different Candida spp. To assess whetherthe 7 new antifungal candidate agents were also effective againstother clinical isolates of C. albicans, as well as other Candida spe-cies, we compared C. albicans SC5314 to other clinical isolatesfrom C. albicans, C. dubliniensis, and C. glabrata (Table 4). C.albicans SC5314 and the off-target drugs with known antifungal
TABLE 4 MIC and MIC0.3 values of antifungal agents for type strains and clinical isolates of Candida spp.a
Antifungal agentConcn range(�g/ml)
C. albicans C. dubliniensis C. glabrata
SC5314 (typestrain)b
UBC3-7922 (clinicalstrain)
CD36/CBS7987(type strain)c
UBC3-3892 (clinicalstrain)
ATCC 90030(type strain)c
UBC3-7268(clinical strain)
MIC MIC0.3 MIC MIC0.3 MIC MIC0.3 MIC MIC0.3 MIC MIC0.3 MIC MIC0.3
Haloperidol HCl 6.4 � 10�3 to 3.76 3.76 0.46 3.76 0.38 3.76 0.38 3.76 0.38 3.76 3.76 3.76 3.76Trifluperidol 2HCl 7 � 10�3 to 4.00 4.00 0.40 4.00 0.40 4.00 4.00 4.00 0.40 4.00 4.00 4.00 4.00Stanozolol 3.3 � 10�3 to 3.29 3.29 0.33 3.29 0.33 3.29 3.29 3.29 3.29 3.29 3.29 3.29 3.29Melengestrol acetate 6.8 � 10�3 to 3.97 3.97 0.37 3.97 0.40 3.97 3.97 3.97 1.80 3.97 3.97 3.97 3.97Megestrol acetate 6 � 10�3 to 3.85 3.85 0.39 3.85 0.39 3.85 3.85 3.85 3.85 3.85 3.85 3.85 3.85Tosedostat 4 � 10�3 to 4.00 4.00 4.00 4.00 4.00 4.00 4.00 4.00 4.00 4.00 4.00 4.00 2.00Amonafide 2.8 � 10�3 to 2.83 2.83 1.40 2.83 2.83 2.83 2.83 2.83 1.40 2.83 2.83 2.83 2.83Methiothepin maleate 7 � 10�3 to 3.57 3.30 0.31 3.30 0.36 3.57 0.36 3.57 0.36 3.57 0.36 3.57 0.36Auranofin 4 � 10�3 to 6.78 0.68 0.08 0.61 0.07 0.68 0.04 0.62 0.04 1.10 0.62 3.73 3.73Rapamycin 9 � 10�3 to 9.14 0.002 �9 � 10�3 0.002 �9 � 10�3 0.009 �9 � 10�3 0.01 �9 � 10�3 0.50 0.04 0.09 0.009
a Candida clinical strains were tested with the 7 identified drugs.b MIC, minimal concentration of drug resulting in �50% growth inhibition; MIC0.3, minimal concentration of drug resulting in �30% growth inhibition. MIC and MIC0.3 weredetermined by ATP measurement after 24 h of incubation. The data were analyzed and evaluated from 4 biological replicates in triplicate (n � 4 [3]).c The type strains C. dubliniensis CD36/CBS7987 and C. glabrata ATCC 90030 were analyzed in 2 biological replicates in triplicate (n � 2 [3]).
TABLE 5 Nonantifungal drugs with known antifungal activitya
Antifungal agent
This study Previous studies
Reference(s)Tested concn(�g/ml)
Incubationtimes (h)
Tested concn(�g/ml)
Incubationtimes (h)
Rapamycin 1.55 � 10�5 to 9.14 6 and 24 0.09–100 48 and 72 26, 38Auranofin 1 � 10�4 to 6.78 6 and 24 12.5–200 48 27Methiothepin maleate 7 � 10�5 to 3.57 6 and 24 64 48 25Bleomycin sulfate 2.6 � 10�4 to 15 6 and 24 1.56 6 and 12 40Disulfiram 5.1 � 10�5 to 2.97 6 and 24 1–8 24 41Artemisinin 4.8 � 10�5 to 2.82 6 and 24 8–50 24 42Tamoxifen citrate 9.7 � 10�5 to 5.63 6 and 24 8–32 24 43a The tested concentrations of off-target drugs with previously demonstrated antifungal activity used in this study were compared to concentrations used in previous studies withsimilar incubation times.
Stylianou et al.
1058 aac.asm.org Antimicrobial Agents and Chemotherapy
on March 17, 2014 by U
ME
A U
NIV
ER
SIT
Y LIB
RA
RY
http://aac.asm.org/
Dow
nloaded from

activity, methiothepin maleate, rapamycin, and auranofin, wereincluded. Since the MICs calculated from the OD and ATP mea-surements were very similar, we exclusively applied ATP measure-ment. Rapamycin was effective against all tested strains (MIC,�0.1 �g/ml). The C. albicans strains SC5314 and clinical isolateUBC3-7922 were affected by the 10 agents to a similar extent (Ta-ble 4). A slightly lower level of inhibition was seen for UBC3-7922than for SC5314. Auranofin was efficient against both C. dublini-ensis strains tested. Haloperidol, in contrast, inhibited the C. dub-liniensis type strain (MIC, 3.76 �g/ml) but inhibited the UBC3-3892 isolate less efficiently. Together, the C. dubliniensis strains
were more resistant against the tested agents than the C. albicansstrains. The two C. glabrata strains were affected to an even lowerextent; however, they were inhibited by 6 of the 10 agents tested.Remarkably, methiothepin maleate reached an MIC of 3.57 �g/mlin both C. glabrata strains (Table 4).
DISCUSSION
Therapy against invasive fungal infections remains a challenge inhealth care. Many patients in surgery, intensive care, oncology, orhematology wards suffer from bloodstream infections caused byCandida spp. However, the dreary outcomes for severe mycosesdo not stem solely from a lack of efficient antifungal drugs (28).Disease progression is also determined by the immune status ofthe afflicted host. Our screen aimed to identify previously un-known anti-Candida activities in drugs already in use with knownpharmacokinetics. We believe that this knowledge for a largeamount of available pharmaceutical agents may enable (i) the de-velopment of new applications as antimycotic therapy for thesetypes of agents, (ii) a future evaluation of the potential synergisticeffects between these drugs and SADs, and (iii) therapy for pa-tients with a primary disease, such as cancer, with drugs that haveadditional known antifungal activities to reduce the risk of severesecondary mycosis. Of course, the latter is only possible in cases inwhich a choice between several drugs is amenable.
The screening of 844 approved drugs or agents in clinical trialsrevealed 26 substances that are active against Candida spp., 7 ofwhich were newly identified. We showed these antifungal activi-ties in three independent assays, metabolic activity measurement,optical densitometry according to EUCAST guidelines, and mi-croscopy, to validate our screening results. The indicated drugshave anti-Candida activities at 6 h and 24 h (Table 2). The MICs ofthe tested agents against C. albicans SC5314 were determined byOD and ATP measurements, and the assays correlated well. Lu-ciferase-based quantification of ATP concentrations recorded thegrowth of C. albicans in a similar fashion as the tetrazolium dyeXTT (data not shown). XTT has been widely used by manygroups, including ours, to quantify fungal viability (29, 30),whereas ATP quantification is more sensitive than the determina-tion of XTT metabolism, allowing for the use of fewer fungal cellsper assay. This indicates that the determination of metabolic ac-tivity is a reliable measure of antifungal activity. ATP measure-ment has, to our knowledge, not been used in antifungal drugscreening; however, it was successfully applied in an S. cerevisiae-based small-molecule screen published in the PubChem BioAssaydatabase (31). We confirmed the validity of our screen by identi-fying the FDA-approved antifungal drugs in the Enzo library (Ta-ble 3), with the exception of nystatin. In agreement with this find-ing, nystatin-resistant C. albicans isolates were reported (32–34).At a concentration of 0.3 to 0.7 �g/ml, the SADs and the newlyidentified agents showed comparable degrees of inhibition againstC. albicans, such as with fluconazole (MIC, 0.3 �g/ml) and halo-peridol (MIC, 0.38 �g/ml). Our focus was to apply drug concen-trations that are likely to be reached in human therapy, and there-fore, we used maximal concentrations of 10 �M. The bloodplasma peak concentrations (Table 2, Cmax and references) andthe concentrations for C. albicans inhibition of the novel antifun-gal candidate agents were within a similar range. This suggests thattherapeutic antifungal concentrations for the treatment of sys-temic mycoses are accomplishable. For the trifluperidol and me-thiothepin maleate, such data were not obtained.
FIG 1 C. albicans SC5314 challenged for 6 h with novel and control drugs. Thepictures are taken from an IncuCyte microscope with a 20� objective lens; thescale bar corresponds to 200 �m. The drug solvent DMSO (A) and the anti-septic BzCl (B) correspond to the 100% and 0% growth controls, respectively.Fluconazole (C) and rapamycin (D) are representative control drugs. Repre-sentative images from C. albicans SC5314 were treated with haloperidol (E),trifluperidol (G), tosedostat (F), and amonafide (H). Morphological changesin C. albicans upon treatment with haloperidol (E) and trifluperidol (G) re-sembled those caused by fluconazole (C), whereas morphological changes inC. albicans upon treatment with tosedostat (F) and amonafide (H) resembledthose of rapamycin (D).
Dual Use of Known Drugs as Antimycotics
February 2014 Volume 58 Number 2 aac.asm.org 1059
on March 17, 2014 by U
ME
A U
NIV
ER
SIT
Y LIB
RA
RY
http://aac.asm.org/
Dow
nloaded from

To broaden the impact of our study, we included additionalCandida strains. We tested the 7 novel agents with referencestrains and clinical isolates of C. albicans from bloodstream infec-tions. The C. albicans strains showed similar susceptibilities to-ward all 7 novel candidate agents, confirming that our findings arevalid beyond common laboratory strains. The C. dubliniensis andC. glabrata strains were more resistant against treatment withthese agents (Table 4). C. glabrata is known to be less susceptible toantifungal therapy (14). In agreement with this, C. glabrata wasless susceptible to auranofin than the other two Candida spp. No-tably, methiothepin maleate and tosedostat were active againstboth C. glabrata strains. This possibly suggests a broad anti-Can-dida activity for methiothepin maleate and tosedostat.
The cellular targets of the identified drugs are known in hu-mans. The dopaminergic drugs haloperidol and trifluperidol acton G-protein-coupled receptors (GPCRs) (Table 6) (35, 36). Hal-operidol has previously been described as a potential antifungalagent in a S. cerevisiae-based chemical-genetic screen to identifymolecular targets for off-target drugs (21). In this screen, we iden-tified the derivative drug trifluperidol and demonstrated the anti-Candida activities of both peridols. GPCRs also exist in Candidaspp.; however, the major cellular pathways targeted by dopami-nergic drugs are amino acid biosynthesis and metabolism (21).The antineoplastic agent tosedostat is an aminopeptidase inhibi-tor (Table 6) (23). The targeted cellular pathways of this drug ineukaryotic cell lines are amino acid metabolism and reduced ac-tivity of target of rapamycin (TOR) kinases (37). Remarkably,rapamycin targets TOR kinases in C. albicans (38), and we re-corded a very similar morphological effect for tosedostat andrapamycin (Fig. 1), indicating that the drugs might have the sametarget against fungi. Amonafide is a topoisomerase inhibitor (22).It is therefore likely, though not proven, that amonafide targetstopoisomerases in fungi. Gene knockout of topoisomerase II in S.cerevisiae resulted in severely attenuated DNA replication (39).Stanozolol, melengestrol, and megestrol acetate are all pseudoste-roids, and thus, their molecular targets are less predictable (Ta-ble 6).
In summary, three independent assays identified 7 novel drugswith dosage-dependent activities against C. albicans with MICs of�4 �g/ml. This study conclusively adds a new pharmacologicalapproach to these drugs, and more importantly, it may help phy-sicians select antineoplastic therapeutics with the antifungal activ-ities identified here for groups of patients that are at high risk foracquiring invasive candidiasis.
ACKNOWLEDGMENTS
This work was supported by grants to C.F.U. from the Swedish ResearchCouncil VR-M (grant no. K2012-99X-21961-01-3), the Laboratory forMolecular Medicine Sweden (MIMS), the Medical Faculty Umeå (grantno. 316-886-10), and the Cancer Research Foundation in Northern Swe-den (grant no. AMP 11-684).
Personnel at the High-Throughput Biomedicine Unit (FIMM Tech-nology Centre, Helsinki, Finland) are acknowledged for their expert tech-nical support. We thank Laura Turunen for her excellent assistance withdrugging compounds. Research infrastructure support was provided byBiocenter Finland.
REFERENCES1. Patterson TF. 2005. Advances and challenges in management of invasive
mycoses. Lancet 366:1013–1025. http://dx.doi.org/10.1016/S0140-6736(05)67381-3.
2. Tortorano AM, Kibbler C, Peman J, Bernhardt H, Klingspor L, GrillotR. 2006. Candidaemia in Europe: epidemiology and resistance. Int. J.Antimicrob. Agents 27:359 –366. http://dx.doi.org/10.1016/j.ijantimicag.2006.01.002.
3. Zilberberg MD, Shorr AF, Kollef MH. 2008. Secular trends in candidemia-related hospitalization in the United States, 2000–2005. Infect. Control Hosp.Epidemiol. 29:978–980. http://dx.doi.org/10.1086/591033.
4. Falagas ME, Apostolou KE, Pappas VD. 2006. Attributable mortality ofcandidemia: a systematic review of matched cohort and case-control stud-ies. Eur. J. Clin. Microbiol. Infect. Dis. 25:419 – 425. http://dx.doi.org/10.1007/s10096-006-0159-2.
5. Bergamasco MD, Garnica M, Colombo AL, Nucci M. 2013. Epidemi-ology of candidemia in patients with hematologic malignancies and solidtumours in Brazil. Mycoses 56:256 –263. http://dx.doi.org/10.1111/myc.12013.
6. Pfaller MA. 2012. Antifungal drug resistance: mechanisms, epidemiology,and consequences for treatment. Am. J. Med. 125:S3–S13. http://dx.doi.org/10.1016/j.amjmed.2011.11.001.
TABLE 6 Putative targets of identified drugs in Candida spp.
Drug
Humans Candida spp.
Function Therapeutic use Reference(s) Suggested target Reference(s)
Haloperidol HCl 5-HT agonist and dopamine receptorantagonist class of G-protein-coupled receptors
Antipsychotic agent 50–52 Gpr1 protein belongs to theG-protein-coupled receptors
35, 36
Trifluperidol 2HCl Dopamine receptor antagonist classof G-protein-coupled receptors
Antipsychotic agent 53 Gpr1 protein belongs to theG-protein-coupled receptors
35, 36
Stanozolol Synthetic steroid Anemia and hereditaryangioedema
54, 55
Melengestrol acetate Progesterone agonist androgen andestrogen receptor antagonist
Antineoplastic agent forendometrial, breast,and prostate cancers
56, 57
Megestrol acetate Progesterone agonist androgen andestrogen receptor antagonist
Antineoplastic agent forendometrial, breast,and prostate cancers
58, 59
Tosedostat Aminopeptidase inhibitor Antileukemic agent andmyelodysplasia
23 Amino acid metabolism, reducedphosphorylation of TORsubstrates
37
Amonafide Topoisomerase inhibitor Antineoplastic agent 22 Topoisomerase II knockout affectsthe DNA replication in buddingyeasts
39
Stylianou et al.
1060 aac.asm.org Antimicrobial Agents and Chemotherapy
on March 17, 2014 by U
ME
A U
NIV
ER
SIT
Y LIB
RA
RY
http://aac.asm.org/
Dow
nloaded from

7. Pfaller MA, Moet GJ, Messer SA, Jones RN, Castanheira M. 2011.Candida bloodstream infections: comparison of species distributions andantifungal resistance patterns in community-onset and nosocomial iso-lates in the SENTRY Antimicrobial Surveillance Program, 2008 –2009.Antimicrob. Agents Chemother. 55:561–566. http://dx.doi.org/10.1128/AAC.01079-10.
8. Sudbery P, Gow N, Berman J. 2004. The distinct morphogenic states ofCandida albicans. Trends Microbiol. 12:317–324. http://dx.doi.org/10.1016/j.tim.2004.05.008.
9. Lo HJ, Köhler JR, DiDomenico B, Loebenberg D, Cacciapuoti A, FinkGR. 1997. Nonfilamentous C. albicans mutants are avirulent. Cell 90:939 –949. http://dx.doi.org/10.1016/S0092-8674(00)80358-X.
10. Bastidas RJ, Heitman J. 2009. Trimorphic stepping stones pave the way tofungal virulence. Proc. Natl. Acad. Sci. U. S. A. 106:351–352. http://dx.doi.org/10.1073/pnas.0811994106.
11. Coleman DC, Moran GP, McManus BA, Sullivan DJ. 2010. Mechanismsof antifungal drug resistance in Candida dubliniensis. Future Microbiol.5:935–949. http://dx.doi.org/10.2217/fmb.10.51.
12. Moran GP, Coleman DC, Sullivan DJ. 2012. Candida albicans versusCandida dubliniensis: why is C. albicans more pathogenic? Int. J. Micro-biol. 2012:205921. http://dx.doi.org/10.1155/2012/205921.
13. Khan Z, Ahmad S, Joseph L, Chandy R. 2012. Candida dubliniensis: anappraisal of its clinical significance as a bloodstream pathogen. PLoS One7:e32952. http://dx.doi.org/10.1371/journal.pone.0032952.
14. Lee I, Fishman NO, Zaoutis TE, Morales KH, Weiner MG, SynnestvedtM, Nachamkin I, Lautenbach E. 2009. Risk factors for fluconazole-resistant Candida glabrata bloodstream infections. Arch. Intern. Med.169:379 –383. http://dx.doi.org/10.1001/archinte.169.4.379.
15. Khan ZK, Jain P. 2000. Antifungal agents and immunomodulators insystemic mycoses. Indian J. Chest Dis. Allied Sci. 42:345–355.
16. Dixon DM, Walsh TJ. 1996. Chapter 76: antifungal agents. In Baron S(ed), Medical microbiology, 4th ed. University of Texas Medical Branch atGalveston, Galveston, TX.
17. Vermes A, Guchelaar HJ, Dankert J. 2000. Flucytosine: a review of itspharmacology, clinical indications, pharmacokinetics, toxicity and druginteractions. J. Antimicrob. Chemother. 46:171–179. http://dx.doi.org/10.1093/jac/46.2.171.
18. Beyda ND, Lewis RE, Garey KW. 2012. Echinocandin resistance inCandida species: mechanisms of reduced susceptibility and therapeuticapproaches. Ann. Pharmacother. 46:1086 –1096. http://dx.doi.org/10.1345/aph.1R020.
19. Pemovska T, Kontro M, Yadav B, Edgren H, Eldfors S, Szwajda A,Almusa H, Bespalov MM, Ellonen P, Elonen E, Gjertsen BT, Karj-alainen R, Kulesskiy E, Lagström S, Lehto A, Lepistö M, Lundán T,Majumder MM, Lopez Marti JM, Mattila P, Murumägi A, Mustjoki S,Palva A, Parsons A, Pirttinen T, Rämet ME, Suvela M, Turunen L,Västrik I, Wolf M, Knowles J, Aittokallio T, Heckman CA, Porkka K,Kallioniemi O, Wennerberg K. 1 September 2013. Individualized Sys-tems Medicine (ISM) strategy to tailor treatments for patients withchemorefractory acute myeloid leukemia. Cancer Discov. http://dx.doi.org/10.1158/2159-8290.CD-13-0350.
20. Arendrup MC, Cuenca-Estrella M, Lass-Flörl C, Hope W, EUCAST-AFST. 2012. EUCAST technical note on the EUCAST definitive docu-ment EDef 7.2: method for the determination of broth dilution mini-mum inhibitory concentrations of antifungal agents for yeasts EDef 7.2(EUCAST-AFST). Clin. Microbiol. Infect. 18:E246 –E247. http://dx.doi.org/10.1111/j.1469-0691.2012.03880.x.
21. Ericson E, Gebbia M, Heisler LE, Wildenhain J, Tyers M, Giaever G,Nislow C. 2008. Off-target effects of psychoactive drugs revealed by ge-nome-wide assays in yeast. PLoS Genet. 4:e1000151. http://dx.doi.org/10.1371/journal.pgen.1000151.
22. Allen SL, Lundberg AS. 2011. Amonafide: a potential role in treatingacute myeloid leukemia. Expert Opin. Investig. Drugs 20:995–1003. http://dx.doi.org/10.1517/13543784.2011.585756.
23. Lowenberg B, Morgan G, Ossenkoppele GJ, Burnett AK, Zachée P,Dührsen U, Dierickx D, Müller-Tidow C, Sonneveld P, Krug U, BoneE, Flores N, Richardson AF, Hooftman L, Jenkins C, Zweegman S,Davies F. 2010. Phase I/II clinical study of tosedostat, an inhibitor ofaminopeptidases, in patients with acute myeloid leukemia and myelodys-plasia. J. Clin. Oncol. 28:4333– 4338. http://dx.doi.org/10.1200/JCO.2009.27.6295.
24. Ganellin CR, Triggle DJ, Macdonald F. 1997. Dictionary of Pharmaco-logical Agents. Chapman & Hall, London, United Kingdom.
25. Butts A, DiDone L, Koselny K, Baxter BK, Chabrier-Rosello Y, WellingtonM, Krysan DJ. 2013. A repurposing approach identifies off-patent drugs withfungicidal cryptococcal activity, a common structural chemotype, and phar-macological properties relevant to the treatment of cryptococcosis. Eukaryot.Cell 12:278–287. http://dx.doi.org/10.1128/EC.00314-12.
26. Sehgal SN, Baker H, Vézina C. 1975. Rapamycin (AY-22,989), a newantifungal antibiotic. II. Fermentation, isolation and characterization. J.Antibiot. (Tokyo) 28:727–732.
27. Ozdemir I, Temelli N, Günal S, Demir S. 2010. Gold(I) complexes ofN-heterocyclic carbene ligands containing benzimidazole: synthesis andantimicrobial activity. Molecules 15:2203–2210. http://dx.doi.org/10.3390/molecules15042203.
28. Brown GD, Denning DW, Levitz SM. 2012. Tackling human fungalinfections. Science 336:647. http://dx.doi.org/10.1126/science.1222236.
29. Meshulam T, Levitz SM, Christin L, Diamond RD. 1995. A simplifiednew assay for assessment of fungal cell damage with the tetrazolium dye,(2,3)-bis-(2-methoxy-4-nitro-5-sulphenyl)-(2H)-tetrazolium-5-carboxanil ide (XTT). J. Infect. Dis. 172:1153–1156. http://dx.doi.org/10.1093/infdis/172.4.1153.
30. Urban CF, Ermert D, Schmid M, Abu-Abed U, Goosmann C, NackenW, Brinkmann V, Jungblut PR, Zychlinsky A. 2009. Neutrophil extra-cellular traps contain calprotectin, a cytosolic protein complex involved inhost defense against Candida albicans. PLoS Pathog. 5:e1000639. http://dx.doi.org/10.1371/journal.ppat.1000639.
31. Nunnari JM. 2010. qHTS assay for small molecule inhibitors of mitochon-drial division or activators of mitochondrial fusion. PubChem BioAssay AID485298. National Center for Biotechnology Information, Bethesda, MD. http://pubchem.ncbi.nlm.nih.gov/assay/assay.cgi?aid�485298.
32. Martin MV, Dinsdale RC. 1982. Nystatin-resistance of Candida albicansisolates from two cases of oral candidiasis. Br. J. Oral Surg. 20:294 –298.
33. Mas J, Piña E. 1980. Disappearance of nystatin resistance in Candidamediated by ergosterol. J. Gen. Microbiol. 117:249 –252.
34. Broughton MC, Bard M, Lees ND. 1991. Polyene resistance in ergosterolproducing strains of Candida albicans. Mycoses 34:75– 83.
35. Miwa T, Takagi Y, Shinozaki M, Yun CW, Schell WA, Perfect JR,Kumagai H, Tamaki H. 2004. Gpr1, a putative G-protein-coupled recep-tor, regulates morphogenesis and hypha formation in the pathogenic fun-gus Candida albicans. Eukaryot. Cell 3:919 –931. http://dx.doi.org/10.1128/EC.3.4.919-931.2004.
36. Sciascia QL, Sullivan PA, Farley PC. 2004. Deletion of the Candidaalbicans G-protein-coupled receptor, encoded by orf19.1944 and its alleleorf19.9499, produces mutants defective in filamentous growth. Can. J.Microbiol. 50:1081–1085. http://dx.doi.org/10.1139/w04-095.
37. Krige D, Needham LA, Bawden LJ, Flores N, Farmer H, Miles LE, StoneE, Callaghan J, Chandler S, Clark VL, Kirwin-Jones P, Legris V, OwenJ, Patel T, Wood S, Box G, Laber D, Odedra R, Wright A, Wood LM,Eccles SA, Bone EA, Ayscough A, Drummond AH. 2008. CHR-2797: anantiproliferative aminopeptidase inhibitor that leads to amino acid depri-vation in human leukemic cells. Cancer Res. 68:6669 – 6679. http://dx.doi.org/10.1158/0008-5472.CAN-07-6627.
38. Cruz MC, Goldstein AL, Blankenship J, Del Poeta M, Perfect JR,McCusker JH, Bennani YL, Cardenas ME, Heitman J. 2001. Rapamycinand less immunosuppressive analogs are toxic to Candida albicans andCryptococcus neoformans via FKBP12-dependent inhibition of TOR. An-timicrob. Agents Chemother. 45:3162–3170. http://dx.doi.org/10.1128/AAC.45.11.3162-3170.2001.
39. Baxter J, Diffley JF. 2008. Topoisomerase II inactivation prevents thecompletion of DNA replication in budding yeast. Mol. Cell 30:790 – 802.http://dx.doi.org/10.1016/j.molcel.2008.04.019.
40. Jayaguru P, Raghunathan M. 2007. Group I intron renders differentialsusceptibility of Candida albicans to bleomycin. Mol. Biol. Rep. 34:11–17.http://dx.doi.org/10.1007/s11033-006-9002-1.
41. Khan S, Singhal S, Mathur T, Upadhyay DJ, Rattan A. 2007. Antifungalpotential of disulfiram. Nihon Ishinkin Gakkai Zasshi 48:109 –113. http://dx.doi.org/10.3314/jjmm.48.109.
42. Galal AM, Ross SA, Jacob M, ElSohly MA. 2005. Antifungal activity ofartemisinin derivatives. J. Nat. Prod. 68:1274 –1276. http://dx.doi.org/10.1021/np050074u.
43. Dolan K, Montgomery S, Buchheit B, Didone L, Wellington M, KrysanDJ. 2009. Antifungal activity of tamoxifen: in vitro and in vivo activitiesand mechanistic characterization. Antimicrob. Agents Chemother. 53:3337–3346. http://dx.doi.org/10.1128/AAC.01564-08.
44. Kudo S, Ishizaki T. 1999. Pharmacokinetics of haloperidol: an update.
Dual Use of Known Drugs as Antimycotics
February 2014 Volume 58 Number 2 aac.asm.org 1061
on March 17, 2014 by U
ME
A U
NIV
ER
SIT
Y LIB
RA
RY
http://aac.asm.org/
Dow
nloaded from

Clin. Pharmacokinet. 37:435– 456. http://dx.doi.org/10.2165/00003088-199937060-00001.
45. Zofková I, Kancheva RL, Hampl R. 1995. A decreasing CD4/CD8
ratio after one month of treatment with stanazolol in postmenopausalwomen. Steroids 60:430 – 433. http://dx.doi.org/10.1016/0039-128X(94)00036-C.
46. Tsukada A, Suemizu H, Murayama N, Takano R, Shimizu M, Naka-mura M, Yamazaki H. 2013. Plasma concentrations of melengestrolacetate in humans extrapolated from the pharmacokinetics established inin vivo experiments with rats and chimeric mice with humanized liver andphysiologically based pharmacokinetic modeling. Regul. Toxicol. Phar-macol. 65:316 –324. http://dx.doi.org/10.1016/j.yrtph.2013.01.008.
47. Femia RA, Goyette RE. 2005. The science of megestrol acetate delivery:potential to improve outcomes in cachexia. BioDrugs 19:179 –187. http://dx.doi.org/10.2165/00063030-200519030-00004.
48. Blodgett RC, Jr. 1983. Auranofin: experience to date. Am. J. Med. 75:86 –89. http://dx.doi.org/10.1016/0002-9343(83)90480-1.
49. Zimmerman JJ, Kahan BD. 1997. Pharmacokinetics of sirolimus instable renal transplant patients after multiple oral dose administration.J. Clin. Pharmacol. 37:405– 415. http://dx.doi.org/10.1002/j.1552-4604.1997.tb04318.x.
50. Granger B, Albu S. 2005. The haloperidol story. Ann. Clin. Psychiatry17:137–140. http://dx.doi.org/10.1080/10401230591002048.
51. Leysen JE, Janssen PM, Gommeren W, Wynants J, Pauwels PJ, JanssenPA. 1992. In vitro and in vivo receptor binding and effects on monoamineturnover in rat brain regions of the novel antipsychotics risperidone andocaperidone. Mol. Pharmacol. 41:494 –508.
52. Kroeze WK, Hufeisen SJ, Popadak BA, Renock SM, Steinberg S, Ern-sberger P, Jayathilake K, Meltzer HY, Roth BL. 2003. H1-histaminereceptor affinity predicts short-term weight gain for typical and atypicalantipsychotic drugs. Neuropsychopharmacology 28:519 –526. http://dx.doi.org/10.1038/sj.npp.1300027.
53. Gallant DM, Bishop MP, Timmons E, Steele CA. 1963. A controlledevaluation of trifluperidol: a new potent sychopharmacologic agent. Curr.Ther. Res. Clin. Exp. 5:463– 471.
54. Resegotti L, Dolci C, Bertero L, Genovese A, Podestà F, Testa D. 1981.Treatment of aplastic anaemia with methenolone, stanozolol and nan-drolone. A report of 130 cases. Panminerva Med. 23:243–248.
55. Sheffer AL, Fearon DT, Austen KF. 1987. Hereditary angioedema: adecade of management with stanozolol. J. Allergy Clin. Immunol. 80:855–860. http://dx.doi.org/10.1016/S0091-6749(87)80277-4.
56. Cooper JM, Elce JS, Kellie AE. 1967. The metabolism of melengestrolacetate. Biochem. J. 104:57P–58P.
57. Perry GA, Welshons WV, Bott RC, Smith MF. 2005. Basis of me-lengestrol acetate action as a progestin. Domest. Anim. Endocrinol. 28:147–161. http://dx.doi.org/10.1016/j.domaniend.2004.07.002.
58. Johnson PA, Bonomi PD, Anderson KM, Wolter JM, Economou SG.1986. Megestrol acetate: first-line therapy for advanced breast cancer. Se-min. Oncol. 13:15–19.
59. Ross MB, Buzdar AU, Blumenschein GR. 1982. Treatment of advancedbreast cancer with megestrol acetate after therapy with tamoxifen. Cancer49:413– 417. http://dx.doi.org/10.1002/1097-0142(19820201)49:3�413::AID-CNCR28204903033.0.CO;2-S.
Stylianou et al.
1062 aac.asm.org Antimicrobial Agents and Chemotherapy
on March 17, 2014 by U
ME
A U
NIV
ER
SIT
Y LIB
RA
RY
http://aac.asm.org/
Dow
nloaded from