Embed Size (px)
Citation preview

Anticoagulation et chirurgie à risque :to bridge or not to bridge?
Charles Marc SAMAMAPôle Anesthésie Réanimations Thorax Explorations
!

Companies and products (DCI):
AstraZeneca (ximelagatran - ticagrelor) – Bayer (rivaroxaban) – BMS (apixaban)
Boehringer-Ingelheim (dabigatran)- CSL Behring (CCP) – Covidien (CPI)
Daïchi Sankyo (edoxaban) - GSK (fondaparinux – nadroparin)
LFB (CCP - fibrinogen) - Lilly+Daichii Sankyo (prasugrel) - Mitsubishi (argatroban) – Octapharma (CCP)
Portola (betrixaban – andexanet) - Pfizer (dalteparin, apixaban) – Roche (POC)
Rovi (bemiparine) - Sanofi-Aventis (enoxaparin, idrabiotaparinux, aspirine, clopidogrel)
Stago (specific anti-Xa test)
Agencies, Societies and Guidelines:ACCP : 8th and 9th Guidelines – SFAR : recos 2004 et 2011
EMA : efficacy working party (expert consultant)
INSERM : laboratory of experimental thrombosis (UMR 1140)
Slides – aknowledgements :Pierre Albaladejo (Grenoble), Anne Godier (Paris), Philippe de Moerloose (Genève),
Patrick Mismetti (St Etienne), Gilles Pernod (Grenoble), Nadia Rosencher (Paris), Pierre Sié (Toulouse), and Michel Meyer Samama (Paris)
Disclosures - Slides

Two Very Old Studies…
Katholi RE Am Heart J 197636 patients, mechanical valves, 44 non-cardiac procedures• anticoagulation by warfarin
discontinuedaortic valves : 0/25 eventmitral valve : 2/10 events
• oral anticoagulation continued:4/9 haemorrhages
Katholi RE Am Heart J 197839 patients, mechanical valves, 45 non-cardiac procedures• anticoagulation by warfarin
discontinuedaortic valve : normal PTmitral valve : stop anticoagulation 24 hours pre-op + vit K + heparinpost-op
• 0 thrombotic events
Katholi RE et al. Am Heart J 1976; 92: 162;Katholi RE et al. Am Heart J 1978; 96: 163

Thrombosis when interrupted ? Bleeding if maintained ?
+

Thrombosis versus Haemorrhage
Myocardial ischemiaTroponin: 0,5 ng/ml
TIAMI
Stent thrombosisMHV thrombosisStroke
Death
DressingHematoma
Hb: 10 g/dl 1-4 RBC units
>10 RBC units
Infection
Death

Mitral Aortic
BileafletTilting discCaged-ball
%
From Heit J, J Thromb Thrombolysis 2001; 12:81-7

Congestive Heart Failure 1Hypertension 1Age ≥ 75 yo 1Diabetes 1Stroke – TIA 2
%
Atrial Fibrillation: CHADS2 Score

Facteur de risque ScoreC : insuffisance cardiaque congestive / dysfonction ventriculaire gauche 1
H : hypertension artérielle 1
A : âge ≥ 75 ans 2
D : diabète 1
S : AVC / Accident ischémique transitoire / Thrombo-embolie 2
V : maladie vasculaire (ATCD d’infarctus du myocarde, maladie artérielle périphérique ouplaque aortique)
1
A : âge 65–74 ans 1
S : sexe (féminin) 1
Score CHA2DS2
-VASc
Patients (n = 7329)
Taux d’AVC ajusté(%/an)* (d’après 3)
0 1 0,0
1 422 1,3
2 1230 2,2
3 1730 3,2
4 1718 4,0
5 1159 6,7
6 679 9,8
7 294 9,6
8 82 6,7
9 14 15,2
1. Lip G et al. ; Refining Clinical Risk Stratification for Predicting Stroke and Thromboembolism in Atrial Fibrillation Using a Novel Risk Factor-Based Approach : The Euro HeartAtrial Fibrillation Survey on Atrial Fibrillation. Chest 2010 ; 137 : 263-72.
2. Camm J et al. ; Eur Heart J 2010;Guidelines for the management of atrial fibrillation ; 31 : 2369-2449. 3. Lip G et al. Identifying Patients at High Risk for Stroke Despite Anticoagulation : A Comparison of Contemporary Stroke Risk Stratification Schemes in an Anticoagulated Atrial
Fibrillation Cohort. Stroke 2010 ; 41 : 2731-2738.
ScoreCHA2DS2-VASc

0
2
4
6
8
10
12
0 30 60 90 120 150 180
Venous Thomboembolism Recurrence%
cum
ulat
ed
days
Heit JA, Arch Intern Med 2000; 160: 761-8

• Annual risk: 4%
• Theoretical risk for 7 days: 0.08%
• Actual rate: >0.8%(including bridging or not)
Dunn AS, Arch Intern Med 2003;163:901-8
Global thrombotic risk for patients with mechanical heart valves, AF or VTE, when OAC are withdrawn

• Hypercoagulability associated with VKA interruption
• Prothrombotic state associated with surgerySamama CM et al, Anesthesiology 2001;94:74-8
Raskob GE, Blood 1995
VKA Interruption


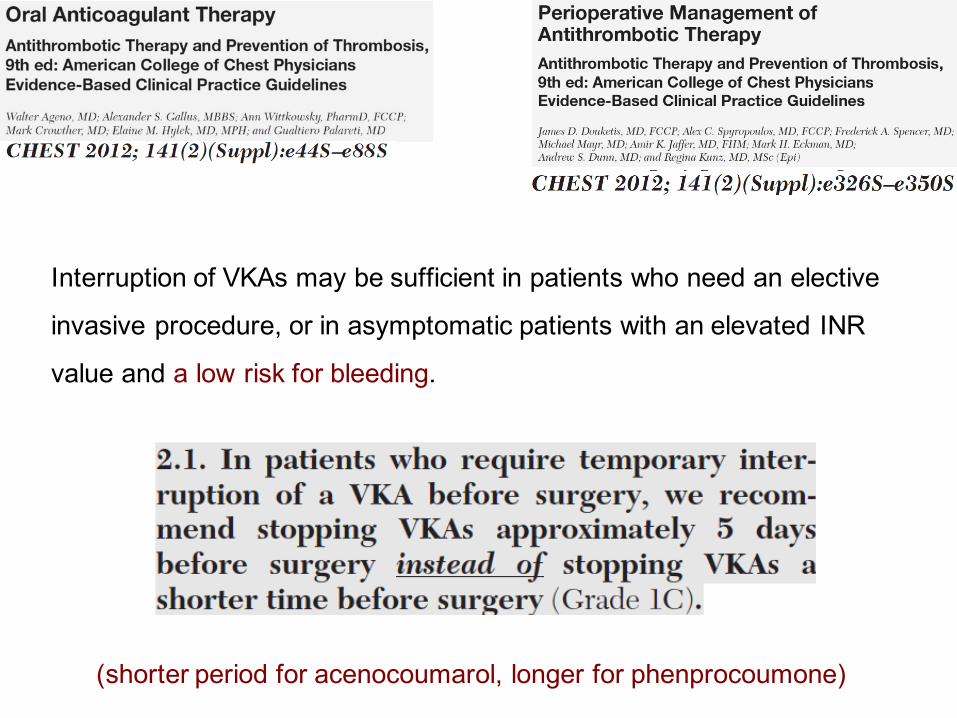
Interruption of VKAs may be sufficient in patients who need an elective
invasive procedure, or in asymptomatic patients with an elevated INR
value and a low risk for bleeding.
(shorter period for acenocoumarol, longer for phenprocoumone)


High ≠ Moderate ≠ Low risk

Modalités du relais
• J-5: dernière prise fluindione, warfarine
• J-4: pas d’héparine (sauf si acénocoumarol) ni d’AVK
• J-3 première dose d’HBPM curatif ou d’HNF, 48h après dernière prise AVK
• J-2: HBPM X2 ou HNF sc X2 ou X3
• J-1: hospitalisation, contrôle INR
– HBPM curatif matin J-1
– HNF sc soir J-1
– Si contrôle INR veille OP > 1,5: vit K 5 mg per os
• J0 : chirurgieIl est souhaitable que les interventions aient lieu le matin.



Patient porteur d’une valve mécanique cardiaquePour les patients traités par AVK pour une valve cardiaque mécanique, dans le cadre d’unechirurgie ou d’un acte invasif programmé, et en dehors des procédures ne nécessitant pasd’arrêt systématique des antivitamines K:
1.Le relais des AVK par des héparines est recommandé en péri-opératoire (grade C).
2.Ce relais peut être effectué par HBPM (hors AMM) à doses curatives en deux injectionssous-cutanées quotidiennes, par HNF intraveineuse à la seringue électrique, ou par HNFsous-cutanée (2/3 injections/j) à doses curatives. Ces trois options sont possibles (grade B).Les HBPM étudiées dans cette situation sont l’enoxaparine et la dalteparine (niveau 2).
3. En l’absence de données de la littérature en péri-opératoire, pour les procédures à risquehémorragique modéré ou élevé, l’utilisation à dose curative d’HBPM en une injection parjour, ou du fondaparinux, ne peut être recommandée.
4. Les héparines doivent être administrées à doses curatives dans les 6 à 48 h postopératoires, selon le risque hémorragique et le risque thromboembolique. Il est recommandéde ne pas reprendre les héparines avant la 6ème heure.

Vitamin K


Patients on long-term VKAs were randomized either to heparin bridging after the last VKA dose on day –5 before surgery (group H) or to VKA treatment until day –2, followed by 1 mg of oral vitamin K on the day before surgery (group K).
If the target INR was not achieved 2 h before incision, surgery was deferred or performed after injection of prothrombin complex concentrate (PCC).
Oral vitamin K (1 mg) cannot substitute for heparin bridging before surgery


Patients on long-term VKAs were randomized either to heparin bridging after the last VKA dose on day –5 before surgery (group H) or to VKA treatment until day –2, followed by 1 mg of oral vitamin K on the day before surgery (group K).
If the target INR was not achieved 2 h before incision, surgery was deferred or performed after injection of prothrombin complex concentrate (PCC).
Oral vitamin K (1 mg) cannot substitute for heparin bridging before surgery
Prothrombin Complex Concentrates (PCC)

Prospective, observational study.
Neurosurgical intensive care unit, university hospital.
18 patients with OAC-associated intracranial hemorrhage requiring urgent
neurosurgical intervention.
All patients received 20 UI/kg of PCC (Kaskadil®, LFB, factor II (37 UI/ml), VII
(10 UI/ml), IX (25 UI/ml), X (40 UI/ml), and heparin (5 UI/ml)) as an intravenous
bolus infusion(3 min) and 5 mg of enteral vitamin K.
Surgery was started immediately, without waiting for blood sample results.

No hemorrhagic or thrombotic adverse
effect was observed intra- or postoperatively.

Meta-analysis of 27 studies providing data on incidence of thromboemboliccomplications in VKA-treated patients. (1,032 patients).
Incidence of thromboembolic events: 1.8% (95% CI 1.0–3.0) in patients treated with 4-factor PCCs, and 0.7% (95% CI 0.0–2.4) in patients treated with 3-factor PCCs.
Low but quantifiable risk of thromboembolism in VKA-treated patients receiving PCCs for anticoagulation reversal

0
0,5
1
1,5
Arrêt simple Substitution
Evénements thrombo-emboliques
Evénements hémorragiques
13%
%
GarciaDetal,ArchIntern Med2008;168:63-69


Thrombotic events
Bleeding
19 vs 32
52 vs 16
BridgingNo bridging
Three times increase in the bleeding risk
Thrombotic risk : no difference
Siegal D et al.

MEDLINE,EMBASE,andCochranedatabases (2001–2010)were searched forEnglish-language studies including patientsreceiving heparin bridging during interruptionofvitamin Kantagonists forelective procedures.

SteinbergBAetal.Circulation2015;131:488-94.
Tendancedéfavorablesurlerisquethrombo-embolique
Risquehémorragiquemultipliépar4

J Arthroplasty. 2014 Jun;29(6):1185–8.
« Current ACCP guidelines recommending bridging therapy for high-risk patients receiving oral anticoagulation and undergoing major orthopaedic procedures are associated with a high rate of bleeding complications and reoperations following primary TKA»
Retrospective study: 38 patients under long-term warfarin match-paired with 76 control patients. Significant increased rate of complications (42.1% vs. 6.9%, P < 0.001) and re-operation (21.1% vs. 5.2%, P < 0.001) in the warfarin group.


BridgeStudy

BridgeStudyEvénements sansrelais avecrelais
n=918 n=895
PrimairesAVC 4(0.4) 3(0.3)AIT 2 3
Saigntsmajeurs 12(1.3) 29(3.2) 0.005
SecondairesIDM 7(0.4) 14(1.6) 0.1TVP 0 1 0.25EP 0 1 0.25
Saigntsmineurs 110(12) 187(20.9) <0,001Décès 5(0.5) 4(0.4) 0.88
- The mean CHADS2 score (CHADS2 scores range from 1 to 6) was 2.3; 38.3% of patients had a CHADS2 score of 3 or higher. - 34.7% of the patients were taking aspirin, and 7.2% were taking another AP drug. - The mean (±SD) number of doses of study drug administered was 5.0±1.1 before the procedure and 16.0±7.9 after the procedure

26 patients, opérés de chirurgie prothétique. score CHA2DS2-Vasc :5,0±0,6 - score HAS-BLED 4,2±0,8
Le soir de la chirurgie, injection d’HBPM à dose prophylactique relayée par un AODà dose prophylactique pendant 24 à 48h puis à dose curative selon l’AMM. Il n'y a pas eu de reprise chirurgicale

Suggestions…

Modalités du relais, si relais…
• J-5: dernière prise fluindione, warfarine dabigatran, rivaroxaban, apixaban
• J-4: pas d’héparine ni d’ACO
• J-3 première dose d’HBPM curatif ou d’HNF, 48h après dernière prise d’ACO
• J-2: HBPM X2 ou HNF sc X2 ou X3
• J-1: hospitalisation,
– HBPM curatif matin J-1
– HNF sc soir J-1
• J0 : chirurgieIl est souhaitable que les interventions aient lieu le matin.



Risk of major bleeding during the at-risk period was similar in rivaroxaban-treated and warfarin-treated participants (0.99% vs. 0.79% per 30 days; HR(CI) = 1.26 (0.80, 2.00), P=0.32
Stroke/SE rates during TIs with bridging compared with those without bridgingwere not different.
Rates of major bleeding were similar between bridged and non-bridged TIs, while rates of major/non major clinically relevant bleeding appearednumerically higher in patients receiving bridging therapy (4.83% vs. 3.02%).


Forprocedures with immediate andcomplete haemostasis,theNOACcanbe resumed6– 8hafter theintervention.Thesame applies after atraumatic spinal/epiduralanaesthesia orcleanlumbar puncture (i.e.non-bloody tap).
Formany surgical interventions,however,resuming fulldoseanticoagulationwithinthefirst48– 72hafter theproceduremay carryableeding risk that could outweightherisk ofcardio-embolism.Onealso hastotake into account theabsenceofaspecific antidoteincasebleeding should occur and/orre-intervention is needed.
Forprocedures associatedwith immobilization, it is considered appropriate toinitiate areduced venous thromboprophylactic (e.g.0.5mg/kg/dayofenoxaparin) orintermediate doseofLMWHs (e.g.1mg/kg/day ofenoxaparin)6– 8hafter surgery ifadequate haemostasis hasbeenachieved,whereas full therapeutic anticoagulationbyrestarting NOACs is deferred 48– 72hafter theinvasiveprocedure.

Suggestions…deux ans plus tard

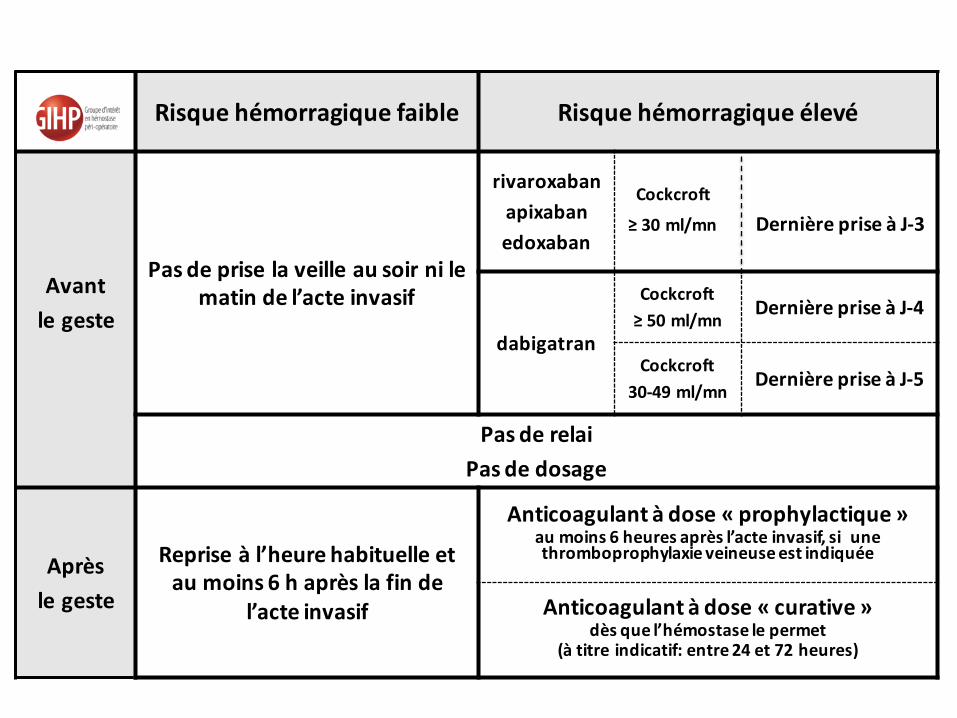
Risquehémorragiquefaible Risquehémorragiqueélevé
Avantlegeste
Pasdepriselaveilleausoirnilematindel’acteinvasif
rivaroxabanapixabanedoxaban
Cockcroft
≥30ml/mnDernièrepriseàJ-3
dabigatran
Cockcroft≥50ml/mn
DernièrepriseàJ-4
Cockcroft30-49ml/mn
DernièrepriseàJ-5
PasderelaiPasdedosage
Aprèslegeste
Repriseàl’heurehabituelleetaumoins6haprèslafinde
l’acteinvasif
Anticoagulantàdose« prophylactique »aumoins6heuresaprèsl’acteinvasif,siunethromboprophylaxie veineuseestindiquée
Anticoagulantàdose« curative »dèsquel’hémostaselepermet
(àtitreindicatif:entre24et72heures)

En pratique…AVK• Risque hémorragique avéré du bridging/relais dans tous les cas• Pas d’efficacité antithrombotique évidente dans la FA: abandon à prévoir• Peu ou pas de données pour la maladie thrombo-embolique veineuse aigue
(attention) ni pour les valves mécaniques (bridging/relais à conserver)
AOD- Pas de bridging/relais
Et surtout…• Les accidents hémorragiques surviennent en post-op en raison du cumul
des héparines et des AVK• Risque faible avec les AOD mais reprise progressive avec HBPM dose
préventive 48 à 72h


www.esahq.org
![L’infarctus veineux hémorragique (IVH) du nouveau …pe.sfrnet.org/Data/ModuleConsultationPoster/pdf/2008/1/cd4c1774-1a... · transformation hémorragique [1] à partir d’une](https://img.pdfslide.us/doc/110x75/5b9a152a09d3f29c338d7f32/linfarctus-veineux-hemorragique-ivh-du-nouveau-pe-transformation-hemorragique.jpg)