Embed Size (px)
Citation preview

Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 1
1
Carl T. Bergstrom
Department of Biology
University of Washington
Antibiotic Resistance
and Hospital-Acquired Infection
2
Pennsyl vania Health Care
Cost Containment Council
In the first nine months of 2005, Pennsylvania hospitals reported:
13,711 hospital acquired infections
1,456 deaths
227,000 extra days of hospitalization
$2.3 billion in extra expenses
PHC4 Research Brief, March 29, 2006
3
Pennsyl vania Health Care
Cost Containment Council
Scaling these numbers up to the entire United States, we expect each year approximately:
450,000 hospital acquired infections
50,000 deaths
7,500,000 extra days of hospitalization
$75 billion in extra expenses

Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 2
4
Antibiotic resistance
After decades of heavy antibiotic use in hospitals, many hospital-associated strains of bacteria
are resistant to multiple antibiotics
Infection with resistant strains:
Increases the probability of treatment f ailure
Extends the duration of hospital stay
Increases the mortality rate
Increases the economic cost of treatment
5
Staphylococcus aureusEnterococcus sp.
52 %
23 %
28 %
10 %
Resistance in the intensive care unitNational Nosocomial Infections Surveillance System Report, 2003
Klebsiella pneumoniae Pseudomonas aeruginosa
6
Playing catch-up ball
Linezolid?
MRSAVRE
Methicillin against
macrolide resistance
Vancomycin used
against MRSA
Linezolid
against VRE
0
Year
5
10
15
20
25
30
35
40
% Resistance

Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 3
7
Combating antibiotic resistance
is a problem in applied evolution
8
How evolution works
Variation: dif f erent indiv iduals
hav e dif f erent traits
Heritability: of f spring tend to be
somewhat like their parents
Selection: indiv iduals with certain traits
surv iv e better or reproduce more
Time: successf ul v ariations accumulate ov er many generations
9From “Battling bacterial evolution: The work of Carl Bergstrom”Understanding Evolution, University of California
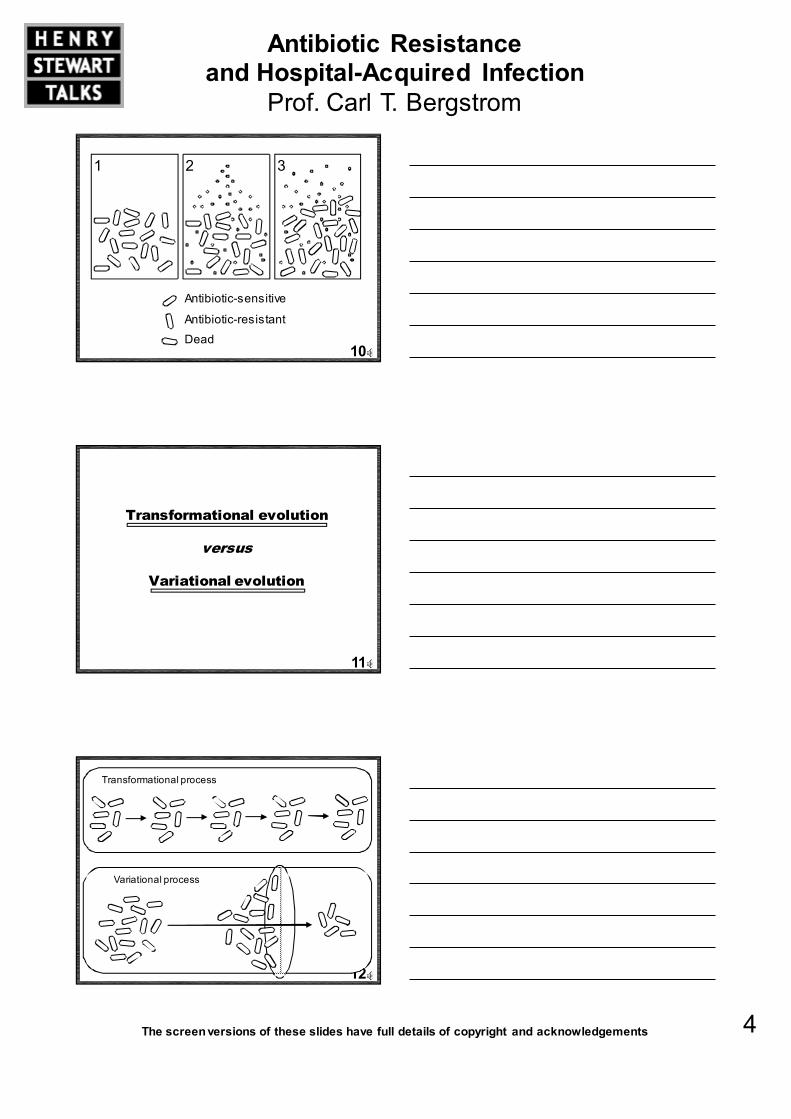
Natural selection, in a nutshell
Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 4
10
1
Antibiotic-sensitive
Antibiotic-resistant
Dead
2 3
11
Transformational evolution
versus
Variational evolution
12
Transformational process
Variational process

Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 5
13
1. Where does the variation come from?
2. What is the structure of selection?
3. How can we intervene?
1 2 3
14
Mutation
15
MutationMacrolide antibiotics block protein synthesis
by binding to bacterial ribosomes
From Hanson et al., (2002) Molecular Cell

Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 6
16
Mutation
A single point mutation in the green binding region can prevent macrolide binding and confer resistance
Modified from Hanson et al., (2002) Molecular Cell
17
Mutation
Genome size: ~ 5 x 106 base pairsMutation rate: ~ 2 x 10-3 per genome
Population size: 1010 to 1011 per g fecal matter
A single gram of f ecal matter is likely to contain
a nov el point mutation conf erring macrolide-resistance!
18
The E. coli efflux pump AcrB
Edward Yu, Iowa StateMore complex mechanisms

Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 7
19
“Nature makes penicillinI only found it”
- Alexander Fleming
Natural ecology of antibiotics
20
Soil microbes liv e in highly structured env ironments
with intense competition f or space and nutrients
Many microbes produce antibiotics to kill of f their competitors
Antibiotic producers must be resistant
to their own products;this generates a v ast reserv oir of resistance genes in bacterial populations
Natural ecology of antibiotics
21
Lateral gene transfer
ConjugationTransf ormationTransduction

Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 8
22
Enterococcus
A. orientalis
Unknown
Van R,S
Van A,H,X
Lateral gene transfer
23
2
1. Where does the variation come from?
2. What is the structure of selection?
3. How can we intervene?
24
Most resistant strains are commensals

Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 9
25
Extremely high rate of drug use
26
Hospital staff act as disease vectors
27
High rate of patient turnover
Community

Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 10
28
Antibiotic use by non-hospitalized patients
leads to resistance in the community at large
Resistance in the community
29
Agricultural use
25 million pounds per year into animal feed
Union of Concerned Scientists, 2001
30
Agricultural use

Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 11
31
1. Where does the variation come from?
2. What is the structure of selection?
3. How can we intervene?
1 32
32
Community
Hospital
A model of a hospital
Lipsitch, Bergstrom, and Levin (2000)
Proc. Nat. Acad. Sciences USA
33
Translate our model into equations
S: patients colonized with sensitiv e bacteria
R i: patients colonized with bacteria resistant to drug i
X: uncolonized patients
dS /dt = mµ+ βSX − (τ1 + τ 2 + γ +µ)S
dRi/dt = β(1− c)R
iX − (µ+ τ ~i + γ)Ri
dX /dt = (1− m)µ + (τ1 + τ 2 + γ)S + (τ2 + γ)R1
+(τ1 + γ )R2 − βSX − β(1− c)RiX −µX
Lipsitch, Bergstrom, and Levin (2000)
Proc. Nat. Acad. Sciences USA

Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 12
34
Things change fast
Non-specif ic controldoes appreciablyreduce resistance*
*When resistance is rare in the community
Formulary changescan rapidly eradicate resistant bacteria
We can study the dynamics using numerical solution
Infection control (70% transmission reduction)
Infection control + switch antibiotics
Time (days)
0
0.1
0.2
0.3
0.4
0.5
0.6
-30
Fraction resistant
-10 10 30 50 70
35
Odds ratios can be misleading
Patients treated with drug 2
have a higher chance
of carrying drug 1 resistance
Drug Y resistance
Treated with X
Untreated
Drug Y resistance
Drug X usage in hospital
Treated with X
Untreated
... but this is a poor measure of efficacy
In fact the net level
of drug 1 resistance drops as the use
of drug 2 increases
36
Antibiotic cycling
"The `crop rotation' theory of antibiotic use
[suggests] that if we routinely v ary
our ̀ go to' antibiotic in the ICU, we can minimize the emergence of resistance because the selectiv e pressure f or bacteria to dev elop resistance to a specif ic antibiotic would be reduced as organisms become exposed to continually v ary ing antimicrobials."
- M. Niederman (1997)
Am. J. Respir. Crit. Care Med.

Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 13
37
Based on sound ecological principles:
Populations have a hard time tracking rapidly fluctuating environmental conditions
38Toltzis et al.(2002) Pediatrics
Cycling
gentamicinpiperacillin/tazobactamceftazidime
Control
gentamicinpiperacillin/tazobactamceftazidime
Cycling in a neonatal ICU
39
Clinical consequencesToltzis et al. (2002)
Infection Control Cycling
(n = 548} (n = 514)
Resistant colonization 7.7% 10.7%
Blood stream 40 42
Meningitis 4 1
Pneumonia 7 13
Urinary tract 7 9
Necrot. enterocolitis 8 7
No significant difference in nosocomial infection rate

Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 14
40
Modelling the efficacy of cycling
Total resistant inf ections: R1 + R2
Baseline f or comparison: in each case, compare the outcomes under cy cling to an approximation of the status quo:
Mixing of the two drugs, in which at any giv en time half of the patients receiv e drug 1, the other half drug 2
Bergstrom, Lo, and Lipsitch (2004)
Proc. Nat. Acad. Sciences USA
41
Total resistant infections
Cycling Mixing
Three month cycling period
Time in days
Fraction resistant
42
Total resistant infections by cycle length
Cycling Mixing
One year Three months Two weeks

Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 15
43
Average total resistanceincreases with cycle period
Cycling Mixing
44
Why doesn'tcycling work?
Bed 1
TTime
2 3 4 5 6 7 8 9 10
45
Why doesn'tcycling work?
Time
Bed 1 2 3 4 5 6 7 8 9 10

Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 16
46
Mixing creates more heterogeneous
environment than does cycling!
Bed 1
TTime
2 3 4 5 6 7 8 9 10
Time
Bed 1 2 3 4 5 6 7 8 9 10
47
US infectious disease mortalitythroughout the 20th century
Sulfonamides
Penicillin
1918 flu pandemic
HIV
Armstrong et al., 2001
48
Acknowledgements
Marc Lipsitch
Harvard School of Public Health
Bruce Levin
Emory University
Diane Genereux
University of Washington

Antibiotic Resistance and Hospital-Acquired Infection
Prof. Carl T. Bergstrom
The screen versions of these slides have full details of copyright and acknowledgements 17
49