Embed Size (px)
Citation preview

Anti-Platelet Therapy in Primary Coronary Intervention
Paul Gordon, MDDirector
Cardiac Catheterization LaboratoryThe Miriam Hospital
Discosures: research/grant support:Eli LillySanofiAccumetricsBristol Meyers

Treatment of STEMITreatment of STEMITreatment of STEMI
Primary PCI with stenting is the preferred treatment to establish reperfusion and improve outcomeDrug eluting stents are safe and have improved late outcomes c/w bare metal stents (mainly lower TVR and TVF)

ANTITHROMBOTIC DRUGS USED IN STEMI
I. ANTIPLATELET DRUGS
II. ANTICOAGULANT DRUGS
• COX-1 inhibitor (aspirin)• ADP P2Y12 receptor inhibitors (ticlopidine; clopidogrel; prasugrel) • Glycoprotein IIb/IIIa inhibitors (abciximab; eptifibatide; tirofiban)
• Anti-Factor II (anti-thrombins) - Indirect Thrombin Inhibitors (UFH & LMWH)- Direct Thrombin Inhibitors (Bivalirudin)
ORAL

Options for Transport of Patients With STEMI and Initial Reperfusion Treatment
EMS Transport
Onset of symptoms of
STEMI
9-1-1EMS
Dispatch
EMS on-scene• Encourage 12-lead ECGs.• Consider prehospital fibrinolytic if
capable and EMS-to-needle within 30 min.
GOALS
PCIcapable
Not PCIcapable
Hospital fibrinolysis: Door-to-Needle within 30 min.
EMS Triage Plan
Inter-HospitalTransfer
Golden Hour = first 60 min. Total ischemic time: within 120 min.
Patient EMS Prehospital fibrinolysisEMS-to-needlewithin 30 min.
EMS transportEMS-to-balloon within 90 min.
Patient self-transportHospital door-to-balloon
within 90 min.Dispatch
1 min.
5 min.
8 min.
Antman EM, et al. J Am Coll Cardiol 2008. Published ahead of print on December 10, 2007. Available athttp://content.onlinejacc.org/cgi/content/full/j.jacc.2007.10.001. Figure 1.
Aspirin 325 mg

Aspirin post-PCI
After the PCI procedure, in patients without allergy or increased risk of bleeding, ASA 162-325 mgdaily should be given for at least 1 month after bare-metal stent implantation, 3 months after drug-eluting stent implantation, after which daily chronic ASA use should be continued indefinitely at a dose of 75 to 162 mg.
Those with an increased risk of bleeding:ASA 81 mg a day indefinitely

6
Recommendations for the use of Thienopyridines
A loading dose of thienopyridine is recommended for STEMI patients for whom PCI is planned. Regimens should be one of the following:
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIIIClopidogrel at least 300 mg to 600mg† should be given as early as possible before or at the time of primary or non-primary PCI.
Prasugrel 60 mg should be given as soon as possible for primary PCI.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII or

Platelet ADP PPlatelet ADP P22YY1212 Receptor InhibitorsReceptor Inhibitors
Clopidogrel,Prasugrel, and Ticagrelor: Biotransformationand Mode of Action
Clopidogrel,Prasugrel, and Ticagrelor: Biotransformationand Mode of Action
SchomigSchomig A.A.NEJM 2009;361:1108.NEJM 2009;361:1108.

PrasugrelPrasugrelTRITON TRITON –– TIMI 38 Trial: TIMI 38 Trial: PrasugrelPrasugrel vsvs ClopidogrelClopidogrel
13,608 Patients 13,608 Patients -- ACS and PCIACS and PCI
WiviottWiviott S et al. NEJM 2007;357:2001.S et al. NEJM 2007;357:2001.
CV death, MI, or stroke
TIMI Major Bleed
Clopidogrel
Prasugrel
Clopidogrel
Prasugrel
"Placebo"
0.0
0.1
0.2
0.3
0.4
0.0
0.1
0.2
0.3
0.4
IPA(% )-20 0 20 40 60 80 100
0.0
0.1
0.2
0.3
0.4
C lopidogrel
Prasugrel
"Placebo"
0.0
0.1
0.2
0.3
0.4
0.0
0.1
0.2
0.3
0.4
IPA (% )-20 0 20 40 60 80 100
0.0
0.1
0.2
0.3
0.4
C lopidogrel
Prasugrel

9
0
2
4
6
8
0 1 2 3
1
0 306090 180 270 360 450
HR 0.82P=0.01
HR 0.80P=0.003
5.6
4.7
6.9
5.6
Days
Prim
ary
Endp
oint
(%)
Prasugrel
Clopidogrel
Prasugrel
Clopidogrel
Loading Dose Maintenance Dose
Timing of BenefitTiming of Benefit(Landmark Analysis (Landmark Analysis -- 3 days)3 days)
Adapted with permission from Antman EM JACC 2008.
TRITON TIMI-38

10
0
5
10
15
0 30 60 90 180 270 360 450
Perc
ent (
%)
Days From Randomization
9.5%
6.5%
HR 0.68(0.54-0.87)
P=0.002
12.4%
10.0%HR 0.79
(0.65-0.97)P=0.02
Clopidogrel
PrasugrelNNT = 42
CV Death / MI / Stroke
TIMI Major NonCABG Bleeds
Clopidogrel
Prasugrel 2.42.1
STEMI CohortSTEMI CohortN=3534N=3534
Montalescot et al Lancet 2008.Adapted with permission from Antman EM.
TRITON TIMI-38
Prasugrel not indicated in patients with:prior strokeage > 75 (relative)low body weight (<60kg) -- 5 mg dosing

PLATO TrialPLATO TrialTicagrelor vs Clopidogrel in ACSTicagrelor vs Clopidogrel in ACS
Wallentin L et al. NEJM 2009;361:1045Wallentin L et al. NEJM 2009;361:1045
Ischemic EndpointIschemic EndpointIschemic Endpoint
11.7%
9.8%HR = 0.84(0.77–0.92)
p<0.001
11.6%
11.2%HR = 1.04(0.95–1.13)
p = 0.43
Bleeding EndpointBleeding EndpointBleeding Endpoint

12
Thienopyridines
The duration of thienopyridine therapy should be as follows:
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII a. In patients receiving a stent (BMS or DES) during PCI for ACS, clopidogrel 75 mg daily or prasugrel 10 mg daily should be givenfor at least 12 months;
b. If the risk of morbidity from bleeding outweighs the anticipated benefit affordedby thienopyridine therapy, earlier discontinuation should be considered.

Urgent Non-cardiac SurgeryIf possible, operate on ASA 81 mg a dayBMS: 4 weeks of DAPT, then operate week 5-6DES: 3-6 months of DAPT
hold thienopyridine 5-7 days (daily PRA testing)
resume thienopyridine as soon as possible post-op
Elective surgery: wait 1 year
Bleeding: tailored treatment to individualECASA 81mg a day vs thienopyridine
alone

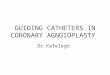
Cellular FactorsCellular Factors• Accelerated platelet turnoverAccelerated platelet turnover•• Reduced CYP3A metabolic activityReduced CYP3A metabolic activity•• Increased ADP exposure Increased ADP exposure •• UpUp--regulation of the P2Yregulation of the P2Y1212 pathwaypathway•• UpUp--regulation of the P2Yregulation of the P2Y11 pathway pathway •• UpUp--regulation of P2Yregulation of P2Y––independent pathwaysindependent pathways
(collagen, epinephrine, TXA(collagen, epinephrine, TXA22, thrombin), thrombin)
Clinical FactorsClinical Factors• Failure to prescribe/poor complianceFailure to prescribe/poor compliance•• UnderUnder--dosing dosing •• Poor absorptionPoor absorption•• DrugDrug--drug interactions involving CYP3A4drug interactions involving CYP3A4•• Acute coronary syndromeAcute coronary syndrome•• Diabetes mellitus/insulin resistanceDiabetes mellitus/insulin resistance•• Elevated body mass indexElevated body mass index
Genetic FactorsGenetic Factors• Polymorphisms of CYPPolymorphisms of CYP•• Polymorphisms of Polymorphisms of GPIaGPIa•• Polymorphisms of P2YPolymorphisms of P2Y1212•• Polymorphisms of Polymorphisms of GPIIIaGPIIIa
ClopidogrelClopidogrel Response VariabilityResponse Variability
Angiolillo DJ et al. J Am Coll Cardiol. 2007; 49: 1505-1516 .
Variability in individual responsiveness to Variability in individual responsiveness to antiplateletantiplatelet agents is an agents is an emerging clinical problem: poor responsiveness has been associatemerging clinical problem: poor responsiveness has been associated with ed with an increased risk of ischemic events, including an increased risk of ischemic events, including stentstent thrombosis.thrombosis.

Clopidogrel - Pharmacogenetic Information
Clopidogrel product information. Revised March 2010
WARNING: DIMINISHED EFFECTIVENESS IN POOR METABOLIZERS
The effectiveness of clopidogrel is dependent on its activation to an active metabolite by the cytochrome P450 (CYP) system, principally CYP2C19. Clopidogrel at recommended doses forms less of that metabolite and has a smaller effect on platelet function in patients who are CYP2C19 poor metabolizers. Poor metabolizers with acute coronary syndrome or undergoing percutaneous coronary intervention treated with clopidogrel at recommended doses exhibit higher cardiovascular event rates than do patients with normal CYP2C19 function. Tests are available to identify a patient's CYP2C19 genotype; these tests can be used as an aid in determining therapeutic strategy. Consider alternative treatment or treatment strategies in patients identified as CYP2C19 poor metabolizers.

Hazard Ratio 1.53(95% CI 1.07-2.19)
P=0.014
8.0
12.1
1064 1009 999 980 870 755 542
Number at Risk:Days After Randomization
Non-Carrier
395 364 360 348 306 270 181Carrier
CV
Dea
th, M
I, or
Str
oke
(%)
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
0 30 90 180 270 360 450
Non-carriers
Carriers
* Carriers ~30% of the population
CYP2C19 Reduced-Function Allele Carriers
N=1,459
Mega JL et al. N Eng J Med. 2009; 360:354-62.
P=0.014
P=0.015
Mega JL et al. N Eng J Med. 2009; 360:354-62.
CYP2C19 and Outcomes: Prasugrel and Clopidogrel, N=2,933
Hazard Ratio 0.89(95% CI 0.60-1.31)
P=0.27
9.8
8.5
1048 991 982 951 849 750 541407 383 376 364 320 276 188
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
0 30 90 180 270 360 450
Number at Risk:Days After Randomization
Non-CarrierCarrier
CV
Dea
th, M
I, or
Str
oke
(%) Non-carriers
Carriers
Mega et al Circulation. 2009;119
Clopidogrel Prasugrel

17
Days from randomization
10
8
6
4
2
00 60 120 180 240 300 360
K-M
est
imat
e (%
)12
Clopidogrel carrier
Ticagrelor Non carrier
11.2
8.68.8
10.0Clopidogrel non carrier
No. at riskClopidogrel LOFClopidogrel No LOF
Ticagrelor LOFTicagrelor No LOF
1,384 1,305 1,274 1,250 1,053 834 6833,554 3,352 3,301 3,222 2,718 2,127 1,761
1,388 1,275 1,259 1,226 1,027 801 6583,516 3,321 3,256 3,186 2,691 2,123 1,757
Ticagrelor carrier
CYP2C19 and Outcomes: Clopidogrel and Ticagrelor, N=10,285
CV Death, MI, Stroke
Wallentin et al. Lancet. 2010; Oonline, 2010 DOI:10.1016/S0140-6736(10)61274-3

Genetic Testing
• Predictor of adverse events including stentthrombosis, but
• Expensive test– Upward of $500– Not readily available
• Variable phenotypic response when checking platelet function testing:– Patients with LOF alelles may have variable plt reactivity
when functional testing performed

LTA 20 μmol/L ADP VerifyNow® P2Y12 Plateletworks®
INNOVANCE® PFA P2Y* PFA-100 COL/ADP IMPACT-R ADP
NPR 6.0%HPR 11.7%
HPR = high-on treatment platelet reactivity
NPR = non-HPR
NPR 6.2%HPR 12.0%
NPR 5.7%HPR 13.4%
NPR 6.1%HPR 12.6%
NPR 7.5%HPR 9.8%
NPR 7.1%HPR 10.8%
NPR 6.3%HPR 12.2%
NPR 6.9%HPR 9.7%
P=0.002p<0.0001p<0.0001 p<0.0001
Composite of death, non-fatal myocardial infarction, definite stent thrombosis and stroke
p=0.17 p=0.06 p=0.02p=0.18
LTA 5 μmol/L ADP
IMPACT-RTests are available, but should they be routinely done?Who should we test?
after clinical events such as stent thrombosishigh risk patients?diabetics, females?
What do we do with “abnormal” results?– more clopidogrel (reload, double dose?)-- switch to prasugrel?

Platelet Function TestsPlatelet Function Tests
•• Platelet Aggregation Platelet Aggregation Light transmittance Light transmittance aggregometryaggregometry (LTA)(LTA)Impedance platelet aggregationImpedance platelet aggregation
•• Flow Flow CytometryCytometryGPIIb/IIIaGPIIb/IIIa receptor activationreceptor activationPP--selectinselectin expressionexpressionMonocyteMonocyte--platelet aggregatesplatelet aggregatesVasodilatorVasodilator--associated stimulated associated stimulated phosphoproteinphosphoprotein (VASP)(VASP)
•• PointPoint--ofof--carecareUltegraUltegra rapid platelet function analyzer (rapid platelet function analyzer (VerifyNowVerifyNow))ThromboelastagraphThromboelastagraph (TEG)(TEG)PlateletworksPlateletworksCone and Cone and plate(letplate(let) analyzer (IMPACT)) analyzer (IMPACT)
•• Genetic testingGenetic testingadapted from Angiolillo DJ et al. J Am Coll Cardiol. 2007.
gold standardgold standard

“Standard Therapy”placebo loading dose
clopidogrel 75mg +placebo/day
“Standard Therapy”placebo loading dose, then
clopidogrel 75mg +placebo/day
“Tailored Therapy”clopidogrel 600-mg*, thenclopidogrel 150-mg/day
Successful PCI with DES (with 600mg clopidogrel load) without major complication or GPIIb/IIIa use
VerifyNow P2Y12 Assay 12-24 hours post-PCI
PRU ≥ 230?
Non-Responder
Clinical Follow-up And Platelet Function Assessment at 30 days, 6M
Primary Endpoint: 6 month CV Death, Non-Fatal MI, ARC definite/prob ST
Yes No
N = 1100 N = 583
Responder
A B C
Random Selection
N = 1100
Safety Endpoint: GUSTO Moderate or Severe Bleeding
ACSRR
G R A V T A S
*total first day dose Price MJ et al, Am Heart J 2009

Efficacy Outcomes: PCI Patients22
Days
Cum
ulat
ive
Haz
ard
0.0
0.01
0.02
0.03
0.04
0 3 6 9 12 15 18 21 24 27 30
ClopidogrelStandard
ClopidogrelDouble
HR 0.8595% CI 0.74-0.99
P=0.036
15% RRR
Days
Cum
ulat
ive
Haz
ard
0.0
0.00
40.
008
0.01
2
0 3 6 9 12 15 18 21 24 27 30
ClopidogrelStandard
ClopidogrelDouble
42% RRR
HR 0.5895% CI 0.42-0.79
P=0.001
CV Death, MI, Stroke Definite Stent Thrombosis

Days
Cum
ulat
ive
Haz
ard
0.0
0.01
0.02
0.03
0.04
0 3 6 9 12 15 18 21 24 27 30
Clopidogrel Standard
Clopidogrel Double
HR 0.7095% CI 0.54-0.92
P=0.011
30%RRR
STEMI-PCI: Myocardial Infarction or All Stent Thrombosis

2009 Updated Labeling for Clopidogrel–PPI Interaction
• FDA-required label changes:2
– Warning: “Co-administration of Plavix with omeprazole, a proton pump inhibitor that is an inhibitor of CYP2C19, reduces the pharmacological activity of Plavix if given concomitantly or if given 12 hours apart”
– Drug-Drug Interactions: “Avoid concomitant use of drugs that inhibit CYP2C19, including omeprazole, esomeprazole, cimetidine, fluconazole, ketoconazole, voriconazole, etravirine, felbamate, fluoxetine, fluvoxamine, and ticlopidine”
– Based on PK/PD studies showing concomitant omeprazole reduced clopidogrel active metabolite and effect on platelets1
• Did not include COGENT study data2
• EMEA warning extends to discourage concomitant use of all PPIs3
– Concomitant use of drugs that inhibit CYP2C19 discouraged; concomitant use of any PPI “should be avoided unless absolutely necessary”4
EMEA=European Medicines Agency; FDA=Food and Drug Administration; PD=pharmacodynamic; PK=pharmacokinetic.1Food and Drug Administration. http://www.fda.gov/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/DrugSafety InformationforHeathcareProfessionals/ucm190787.htm. Published November 17, 2009. Accessed January 22, 2010. 2Plavix [package insert]. Bridgewater, NJ: Bristol-Myers Squibb/Sanofi Pharmaceuticals Partnership; 2009. 3Wathion N. http://www.emea.europa.eu/humandocs/PDFs/ EPAR/Plavix/32895609en.pdf. Published May 29, 2009. Accessed January 22, 2010. 4Plavix [summary of product characteristics]. Paris, France: Sanofi Pharma Bristol-Myers Squibb SNC; 2009.

Clopidogrel is a prodrug; requires conversion by the liver primarily via CYP3A4 and CYP2C19 to an active metabolite
PPIs are strong inhibitors of CYP2C19 activity
ClopidogrelClopidogrel is a is a prodrugprodrug; requires conversion by the liver ; requires conversion by the liver primarily via CYP3A4 and CYP2C19 to an active metaboliteprimarily via CYP3A4 and CYP2C19 to an active metabolite
PPIsPPIs are strong inhibitors of CYP2C19 activityare strong inhibitors of CYP2C19 activity
ClopidogrelClopidogrel and and PPIsPPIs –– The OCLA studyThe OCLA study
-32.6
-43.3-50-45-40-35-30-25-20-15-10-50
PRI V
aria
tion
(%)
Omeprazole (n=64)Placebo (n=60)
PRI: Platelet Reactivity Index as measured by vasodilator stimulated phosphoprotein (VASP)
Gilard et al. J Am Coll Cardiol 2008;51:256-60.
p<0.0001

Risk of All-Cause Mortality and Recurrent ACS in Patients Taking Clopidogrel and PPI
Ho PM, Maddox TM, Wang L, et al. JAMA. 2009;301(9):937-944.
0.70
0.60
0.50
0.40
0.30
0.20
0.10
00 90 180 270 360 450 540 630 720 810 900 990 1080
Days Since Discharge
Prop
ortio
n of
D
eath
s or
Rec
urre
nt A
CS
Neither clopidogrel nor PPIPPI without clopidogrelClopidogrel + PPIClopidogrel without PPI

CV
deat
h, M
I or s
trok
e
Days
CLOPIDOGREL PPI vs no PPI: Adj HR 0.94, 95% CI 0.80-1.11
PPI use at randomization (n= 4529)
Clopidogrel
Prasugrel
PRASUGREL PPI vs no PPI: Adj HR 1.00, 95% CI 0.84-1.20
Primary endpoint stratified by use of a PPI
O’Donoghue ML, Braunwald E, Antman EM, et al. Lancet. 2009.

Days
Sur
viva
l Pro
babi
lity
0 30 60 90 120 150 180 210 240 270 300 330 360 390
0.90
0.92
0.94
0.96
0.98
1.00
Placebo
Treated
Survival Curves for PPI Treated vs PlaceboComposite Cardiovascular Events
Adjustment through Cox Proportional Hazards ModelAdjustment through Cox Proportional Hazards ModelAdjusted to Positive NSAID Use and Positive H. Pylori StatusAdjusted to Positive NSAID Use and Positive H. Pylori Status
HR = 1.0295% CI = 0.70; 1.51
Placebo: 67 events, 1821 at riskTreated: 69 events, 1806 at risk

Days
Sur
viva
l Pro
babi
lity
0 30 60 90 120 150 180 210 240 270 300 330 360 390
0.90
0.92
0.94
0.96
0.98
1.00
Placebo
Treated
Survival Curves for PPI Treated vs PlaceboComposite GI Events
HR = 0.5595% CI = 0.36; 0.85
p=0.007
(preliminary)
Placebo: 67 events, 1895 at riskTreated: 38 events, 1878 at risk

Thienopyridines after 1 year?
Very Late Stent Thrombosis
To be answered in “near future” by several large scale DAPT Trials
Event free patients at 12 months randomized to thienopyridine vs placebo along with daily aspirin

31
Diabetic SubgroupDiabetic Subgroup
0
2
4
6
8
10
12
14
16
18
0 30 60 90 180 270 360 450
HR 0.70P<0.001
Days
Endp
oint
(%) CV Death / MI / Stroke
TIMI Major NonCABG Bleeds
NNT = 21
N=3146N=3146
17.0
12.2
Prasugrel
Clopidogrel
Prasugrel
Clopidogrel 2.62.5
Wiviott SD et al Circulation 2008.Adapted with permission from Antman EM.
TRITON TIMI-38

32
StentStent ThrombosisThrombosis(ARC Definite + Probable)(ARC Definite + Probable)
0
1
2
3
0 30 60 90 180 270 360 450
HR 0.48P <0.0001
Prasugrel
Clopidogrel2.4
(142)
NNT= 77
1.1 (68)
Days
Endp
oint
(%)
Any Any StentStent at Index PCIat Index PCIN= 12,844N= 12,844
Adapted with permission from Wiviott SD et al Lancet 2008
Significant reductions both with BMS, DESSignificant reductions both with BMS, DESSignificant reductions in early and late Significant reductions in early and late stentstent thrombosesthromboses
TRITON TIMI-38
Prasugrel not indicated in patients with:prior strokeage > 75 (relative)low body weight (<60kg)—5 mg dosing