Embed Size (px)
Citation preview

PDFlib PLOP: PDF Linearization, Optimization, Protection
Page inserted by evaluation versionwww.pdflib.com – [email protected]

Review
Anterior chamber depth and primary angle-closure glaucoma:an evolutionary perspectiveRobert J Casson DPhil FRANZCOSouth Australian Institute of Ophthalmology, Adelaide University, South Australia, Australia
ABSTRACT
Anterior chamber depth is an inheritable trait which is affectedby age, gender and race. Over 30 years ago, Alsbirk proposedthat the shallow anterior chamber, which was typical of theGreenlandic Inuit, and which brings the iris in proximity to thecornea, may have evolved as a thermoregulatory adaptation toresist corneal freezing. Here, this hypothesis is revisited. Recentpopulation genetic data which provide evidence for migrationpatterns of early humans are discussed and the notions ofnatural selection and ocular adaptation to cold climates areconsidered. Problems with the hypothesis are examined, butthe idea that the shallow anterior chamber has a thermoregu-latory role appears sound and suggests that shallow anteriorchambers may have evolved in Homo sapiens living in north-east Asia during the last Ice Age.
Key words: anterior chamber, angle-closure glaucoma,evolution.
DEFINITIONS
Primary-angle closure glaucoma (PACG) has a particularlydevastating effect on vision and is thought to be responsiblefor about half of the world’s glaucoma blindness.1 Tradition-ally, the term PACG referred to a family of ocular conditionswhich share an anatomical predisposition for irido-trabecularcontact (ITC), leading to intraocular pressure (IOP) eleva-tion and glaucomatous optic neuropathy (GON). AlthoughPACG encompasses a range of clinical presentations fromthe dramatic to the insidious, it is the ITC which is pathog-nomonic: no ITC, no PACG.
To improve consistency among epidemiological studies,the International Society for Geographical and Epidemio-logical Ophthalmology has recently proposed definitionswhich reserve the term ‘glaucoma’ for those with GON.2
Those eyes with irido-corneal angles traditionally described
as ‘occludable’ have been renamed as primary angle closure sus-pects (PACS) and those meeting criteria for PACS butwith peripheral anterior synechiae (PAS) or elevated IOPand without GON are described as having primary angleclosure (PAC).2 These conditions are considered to representpreglaucomatous stages in the natural history of thedisease2–4 and reflect the long-term risk of visual morbidity.5
Hence, in the modern parlance, only those eyes with PACand GON are considered to have PACG. There is currentlyno agreed collective term for the three conditions (PACS,PAC and PACG); however, the term ‘angle-closure disease’has been used.6,7 In this review I will principally refer toPACG, but the conclusions will logically apply to eyes withPACS and PAC.
RISK FACTORS FOR PACG
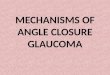
There are a number of well-described ocular risk factors forPACG, including shallow anterior chamber (AC), short axiallength, small corneal diameter, and thick crystalline lens.8 Ofthese, a shallow AC is the most consistent risk factor.8–15 Anteriorchamber depth (ACD) is an inheritable trait9 which is highlycorrelated with age and tends to be shallower in women.8 Inaddition, there is evidence that it is influenced by ‘race’,8
tending to be deeper in Caucasians than Asians and shallow-est in the Inuit (Eskimos) (Fig. 1).
The notion of ‘race’ is a controversial issue.17 It remainspoorly defined, and an increasing understanding of popula-tion genetics and biological diversity within related groupshas led to the view that ‘race’ is biologically meaningless.18
Carleton Coon’s categorization of humankind into five racialgroups (Caucasoid, Negroid, Mongoloid, Australoid andCapoid) has been considered scientifically naïve; however,despite controversy, this classification still remains in use.19
Others insist that self-identified race, inasmuch as it repre-sents genetic heritage, remains an important biologicalfeature with implications for Bayesian type clinical decisionmaking.20 Cavalli-Sforza suggests that the term ‘ethnic groups’
� Correspondence: Dr Robert Casson, South Australian Institute of Ophthalmology, Department of Ophthalmology and Visual Sciences, Adelaide University, SA
5000, Australia. Email: [email protected]
Received 13 September 2007; accepted 17 December 2007.
Clinical and Experimental Ophthalmology 2008; 36: 70–77doi: 10.1111/j.1442-9071.2008.01672.x
© 2008 The AuthorJournal compilation © 2008 Royal Australian and New Zealand College of Ophthalmologists

may be more acceptable than raceand implies differences inboth genetic and cultural heritage.21
There is an overwhelming clinical impression thatprimary open-angle glaucoma (POAG) is more commonthan PACG in white and black populations. In fact, thisimpression is so strong that robust data to support it arelimited, because in the majority of population-based oph-thalmic surveys on white and/or black populations, the anglehas been ignored. A recent, large, population-based study ona Hispanic population found a low rate of PACG (0.1%).22
However, PACG in Anglo-Europeans, particularly in itsacute form (acute angle-closure glaucoma) is a common clini-cal occurrence, and routine gonioscopy, as a component ofall glaucoma assessments, is likely to increase the yield ofPACG in white and black populations. Nevertheless, there isconvincing evidence that PACG is more common amongcertain ethnic groups.8
In 1971, Clemmenson and Alsbirk reported high rates ofPACG in Greenlandic Inuit.23 Shortly after, Drance reportedsimilar findings in Canadian Inuit.24 Alsbirk subsequentlydescribed the very shallow ACD in the Greenlandic Inuitpopulation,9,10 later confirmed by Wojciechowski et al.25 Highrates of PACG were reported by Arkell et al. among AlaskanInuit.26 and relatively high rates by Salmon et al. among the‘Cape Coloured’† people of South Africa.27 Foster et al.reported high rates in rural Mongolia28 and to a lesser degreein Chinese Singaporeans13 and Chinese in the Liwan Districtof southern China.29 Lower rates were reported from Bang-ladesh,30 Thailand31 and southern India,6,32,33 but Casson et al.recently reported high rates (but not as high as the Inuit)among the Burmese in central Myanmar.34 (The prevalenceof glaucoma in various population-based studies is shown inTable 1.) Why do certain ethnic groups have high rates ofPACG? Given that these groups are widely spread across
diverse habitats, a common environmental factor seems anunlikely explanation. Assuming that genes can influence thetendency to develop PACG, could a common genetic heri-tage be an explanation? Given that there is no evidence of arecent common genetic heritage, to know whether thesegeographically diverse groups share a common distantancestor, we need to understand the migration patterns ofantiquity.
A BRIEF HISTORY OF ANCIENTHUMAN MIGRATION
The origin of modern humans remains controversial: the twoprincipal palaeo-anthropological theories are (i) the multir-egional model which contends that ‘a worldwide network ofgenic exchanges, between evolving human populations thatcontinually divide and reticulate, provides a frame of popu-lation interconnections that allows both species-wide evolu-tionary change and local distinctions and differentiation’.37
(ii) the Out of Africa model (Replacement Hypothesis,recent single-origin hypothesis) which postulates a single,African origin for Homo sapiens.38,39
Recent developments in population genetics, particularlythe use of mitochondrial DNA (mtDNA) and the non-recombining portion of the Y-chromosome (NRY) to traceancestry have provided knowledge about early humanmigrations. Although not all genetic evidence is supportive,40
currently the preponderance of genetic evidence supportsthe view that modern humans are a relatively recent evolu-tionary phenomenon, supporting the Out of Africamodel.41–43 According to this model, H. sapiens evolved inAfrica about 200 000 years ago, with an exodus of onelineage along the east African coast44,45 about 70 000 yearsago. These peoples spread into Europe, Asia and Australia‘replacing’ other pre-existing Homo species, including Nean-derthals and Homo erectus.
Macauley et al. have shown that mitochondrial DNAvariation in isolated aboriginal populations in south-east Asiasupports the view that there was only a single dispersal fromAfrica, most likely via a coastal route, through India andonward into south-east Asia and Australasia.45 There was anearly offshoot, leading ultimately to the settlement of theNear East and Europe, and the main dispersal from Indiato Australia approximately 65 000 years ago was rapid,most likely taking only a few thousand years.45 UsingY-chromosome analyses, Su et al. have shown that southernpopulations in eastern Asia are more genetically polymor-phic than northern populations.46 This pattern indicatesthat the first settlement of modern humans in eastern Asiaoccurred in mainland South-east Asia.47 A northward migra-tion extended into northern China and Siberia,46,48 populat-ing southern Siberia by 45 000 years ago49 and arctic Siberiaby 30 000 years ago.50 These patterns of early human mi-gration are depicted in Fig. 2. Further migrations fromwestern Asia may have colonized the Russian Plains around40 000 years ago.51 There is evidence from immunologicalhaplotypes52,53 that the modern Chinese originated from two
†The term Cape Coloureds refers to a modern-day group of people in South
Africa with mixed ancestry, including East Asian.
2
2.2
40 50 60 70 80
2.4
2.6
2.8
3
3.2
3.4
3.6
Inuit
Latinos
Mongolians
Burmese
Singaporeans
Age
AC
D (
mm
)
Figure 1. Anterior chamber depths (ACD) in various populations.ACD decreases with age in all populations and is shallowest in theInuit9 and deepest in the Caucasian Latino population.16 (Data havebeen assimilated as an average of age-specific ACD and adaptedfrom Johnson and Foster.4)
Anterior chamber depth 71
© 2008 The AuthorJournal compilation © 2008 Royal Australian and New Zealand College of Ophthalmologists

distinct populations: one from the Yellow River valley andthe other from the Yangtze River valley. Yao et al. using morerecent mtDNA techniques analysis, provide supporting evi-dence of an initial south to north migration and of geneticdifferences between Han populations (the majority Chinesepopulation) in northern and southern China, but with con-siderable mixture, indicating subsequent migrations south-wards and east-west.54 Furthermore, there is genetic evidencethat the initial populations of south-east Asia (includingmodern day Myanmar) interbred with later waves ofmigrants from northerly latitudes during the last Ice Age.55
Although the precise ancestry of the indigenous people ofthe Americas remains controversial, there is strong evidencethat the primary migration of ancestral Asians expandedfrom south-central Siberia into the New World and gave riseto ancestral Amerindians.56 Using linguistic, dental andgenetic evidence, Greenberg et al. proposed three waves ofmigration into the New World.57 The precise migrationpattern is still disputed but there is considerable evidence
that the modern Inuit are derived from a later migration thanthe ancestors of the Amerinds.56,58,59 The initial migrationseems to have occurred between 20 000 and 15 000 yearsago, before the emergence of the Clovis sites (11500 yearsago) in North America‡ (the earliest undisputed archeologi-cal evidence of human habitation in North America).60 Theinitial migration appears to have brought mtDNA haplo-groups A–D to the New World, with these genetic lineagesbecoming widespread in the Americas.56,60 A second expan-sion that perhaps coincided with the opening of the ice-freecorridor probably brought mtDNA haplogroup X to Northand Central America.56 Finally, populations that formerlyinhabited north-eastern Asia expanded into northern NorthAmerica after the last glacial maximum, and gave rise toEskimo-Aleuts and Na-Dene Indians.56,61 Dating of the Ber-ingian (easternmost Siberian and western Alaskan) branch ofhaplogroup A (16192T) suggested that populations ancestralto the Aleuts, Eskimos and Athapaskan Indians emergedapproximately 13 000 years ago.61 Hence, the modern-day Inuit, inhabiting circumarctic regions stretching fromwestern Alaska to Greenland, are generally considered to bethe descendants of a wave of migration of people crossingthe Bering Land Bridge from north-eastern Asia around13 000 years ago, and because of their isolated environmentthere has subsequently been relatively little genetic dilution.Furthermore, Starikovskaya et al. recently analysed themtDNA of 531 individuals from nine indigenous populationsin Siberia and concluded that the immediate ancestors of theSiberian/Beringian migrants who gave rise to ancient (pre-Clovis) Palaeoindians have a common origin with aboriginalpeople of the area now designated the Altai-Sayan Upland,as well as the Lower Amur/Sea of Okhotsk region.62
Hence, assuming that the genetic tendency towardsPACG did not develop independently at multiple sites, theevidence suggests that the anatomical predisposition for ITCdeveloped in north-east Asia (in the region of modern-day
‡The fact that the earliest convincing evidence of human habitation in South
America predates similar quality evidence of habitation in North America
has caused considerable debate in the archeological community and an
acceptable explanation remains elusive.
Table 1. Prevalence of glaucoma in various population-based studies
Author (year) Location Number Age group(years)
PrevalencePACG
(%)
PrevalencePOAG
(%)
RatioPACG : POAG
Arkell et al. (1987)26 Alaska (Inuit) 786 �40 2.65 0.13 21:1Foster et al. (1996)28 Mongolia 942 �40 1.4 0.5 2.8:1Mitchell et al. (1996)35 Blue Mountains 3654 �50 0.3 3.0 1:10Foster et al. (2000)28 Tanjong Pagar, Singapore 1232 40–79 1.13 1.78 0.63:1Quigley et al. (2001)22 Aizona, USA 4774 �40 0.1 1.97 1:20Vijaya et al. (2005,36 20066) Chennai, India 3924 �40 0.87 1.62 0.54:1He et al. (2006)29 Liwan, Guangzhou 405 �50 1.5 2.1 0.71:1Casson et al. (2006)34 Meiktila, Myanmar 1997 �40 2.5 2.0 1.25:1
PACG, primary angle-closure glaucoma; POAG, primary open-angle glaucoma.
Figure 2. Schematic depiction of early Homo sapiens migrationpatterns. 1, initial exodus of H. sapiens out of Africa about70 000 years ago. 2, Early offshoot to Europe and Middle East.3, Southern Asian route to Oceania about 60 000 years ago.4, Into northern Asia about 45 000 years ago. 5, Offshoot intoarctic Siberia 35 000 years ago. 6, Beringian expansion about15 000 years ago. 7, Reverse migration back to south-east Asia.
72 Casson
© 2008 The AuthorJournal compilation © 2008 Royal Australian and New Zealand College of Ophthalmologists

Siberia) between 40 000 and 15 000 years ago, and that thelower the rate of subsequent genetic exchange the greaterthe tendency for a shallow AC and PACG. What evolution-ary pressures might have led humans to develop a tendencytowards shallow ACs in the late Pleistocene period in north-east Asia? During this period, conditions were considerablyharsher than they are today; in particular, it was even colderin this region then than it is today: in fact, it was an Ice Age.
NATURAL SELECTION AND ADAPTATIONTO COLD
Darwin proposed that biological diversity occurred by theprocess of evolution from a common ancestor (‘descent withmodification’) and that this process was driven by naturalselection.63 This concept was forged in the absence of amechanism for inheritance and random mutation andDarwin’s ideas have since been incorporated into a contem-porary understanding of evolution which involves molecularand population genetics: the modern evolutionary synthesis.Although the precise mechanisms of evolution are not fullyunderstood, the concept of natural selection remains a cor-nerstone of modern biology.
In The Origin of Species,63 Darwin wrote:
Can it, then, be thought improbable, seeing that variationsuseful to man have undoubtedly occurred, that othervariations useful in some way to each being in the great andcomplex battle of life, should sometimes occur in thecourse of thousands of generations? If such do occur, canwe doubt (remembering that many more individuals areborn than can possibly survive) that individuals having anyadvantage, however, slight, over others, would have thebest chance of surviving and of procreating their kind? Onthe other hand, we may feel sure that any variation in theleast degree injurious would be rigidly destroyed. Thispreservation of favourable variations and the rejection ofinjurious variations, I call Natural Selection. Inherited traitsthat lead to survival to reproductive age and production ofmore offspring are more likely to persist in the population.Why then did a predisposition to shallow ACs evolve innorth-east Asia during the late Pleistocene? Is a shallow ACassociated with a favourable, heritable ocular trait? Toanswer these questions we need to understand how naturalselection leads to phenotypic suitability to the prevailingconditions.
The process of natural selection leads inexorably to theevolution of creatures that are adapted to their environment.This notion is deduced from the premise that creaturesthat are not adapted to their environment produce feweroffspring. An important aspect of the environment whichaffects survival is the climate. This aspect affects internalphysiology and surface features at the body/environmentinterface and is generally believed to be the principal forcethat has driven phenotypic variability in humans leading todifferences in skin colour, stature, and body habitus.64 Astrong association exists between human morphology andtemperature, thermoregulation being a critical factor in
survival.65 A number of adaptations to a cold environmenthave been reported. Coon et al. first suggested that the rela-tively round, flat ‘Mongoloid face’, with ‘its reduced browridges, heavy malars and epicanthic folds’, is a product ofselection and adaptation to cold.66 Beals reported a correla-tion between low environmental temperature and roundheadedness,67 possibly because a spherical shape providesthe largest volume (and heat production) with the smallestsurface area (and heat loss). This is a manifestation of Berg-mann’s rule in zoology which states that mammals in colderclimates tend to have greater mass and reduced surface area;68
however, it has been argued that this simple mathematicalmodel may not actually apply, and that there is, in fact, littleevidence to suggest that mass to area ratios in biology sig-nificantly affect thermoregulation.69,70 Nevertheless, adapta-tions to a cold environment are likely to affect survival, andwe can ask what ocular adaptations occur in cold climates?Might an ocular adaptation to cold inadvertently cause apredilection to PACG?
There are scarce data concerning possible ocular adapta-tions to cold. However, in 1976, Alsbirk proposed that theshallow AC, bringing the vascularized, warm iris in closeproximity to the cornea, which was typical of GreenlandicInuit eyes may be a thermoregulatory adaptation to resistcorneal freezing.9 Alsbirk showed that the shallow AC inInuit had a familial tendency and he proposed a polygenicinheritance.9 Corneal freezing and dessication keratitits areuncommon conditions that have only ever been reported inthe context of freezing temperatures combined with highwind speeds and lack of eye protection.71–74 Alsbirk reports awitnessed case of ‘corneal congelation’ in an Inuit seal hunterin high winds and subfreezing conditions.9 Based on datafrom military free fall parachutists who have lost protectiveeye wear during descent from high altitudes, duration ofocular symptoms was significantly associated with subfreez-ing temperatures. Given that the terminal velocity of a para-chutist is about 200 km/h, at a temperature of -20°C thewind chill would be approximately -45°C (wind speed above65 km/h has little influence of the chill factor). Even atthese extremes, only temporary epithelial damage has beenreported;72 however, the duration of exposure was relativelyshort. It appears that the human cornea is relatively cold-tolerant, but in arctic conditions, particularly during the lastIce Age corneal freezing was a potential problem, a problemthat renders the individual temporarily blind72 and is likely tobe associated with increased mortality. Anatomical factorsmitigating against it would have a selection advantage;hence, the possibility that the tendency for a shallow ACdeveloped over time under these conditions. Furthermore,although the cost of a shallow AC is a greatly increased riskfactor for ITC and PACG, as pointed out by Alsbirk,9 this isunlikely to be a selection disadvantage, because it tends tooccur in old age, after reproduction. From the genes’ per-spective, the pros outweigh the cons. (This raises the inter-esting question: Why are there old people? Shouldn’t naturalselection have wiped them out long ago? This puzzle hasbeen addressed by many biologists over the years and still
Anterior chamber depth 73
© 2008 The AuthorJournal compilation © 2008 Royal Australian and New Zealand College of Ophthalmologists

has not been completely solved. Although morbidity andmortality is clearly age-related, natural selection wouldpredict a precipitous increase in mortality at menopause.How is it that humans seem to mostly avoid this ‘wall ofdeath’? Tulijapurkar et al.75 have described a mathematicalmodel which demonstrates a significant selection advantagewhen older men are reproducing with younger women. Thishas been called the ‘dirty old man’ hypothesis, and is perhapsthe best current explanation for the existence of old people!)
Hence, based on the evidence above, we can revisitAlsbirk’s idea and formulate the hypothesis that a shallowAC originated in H. sapiens in north-east Asia 40 000–15 000 years ago as an anatomical adaptation to resist cornealfreezing. From the principles of natural selection and geneticswe can make several deductions: (i) the consequent increasedrisk of ITC and PACG is not a negative selection factor; (ii) thetrait is inheritable; and (iii) with sufficient interbreeding thetendency towards a shallow AC would be lost.
PROBLEMS WITH THE HYPOTHESIS
We can recognize several problems with this hypothesis thatneed to be addressed. First, the hypothesis is neither directlytestable nor falsifiable; hence, an argument could be madethat it is unscientific (the same argument, albeit specious, hasbeen used against evolution per se76). However, it does haveexplanatory power and potentially has predictive power. Forexample, that ACs are likely to be shallow in Siberia andmore shallow in northern China than southern China. Also,although robust evidence is scarce, the apparent relativelylow rate of PACG in indigenous Americans compared withthe Inuit would support genetic evidence that there wereat least two waves of expansion from Asia,56 the earliestexpansion possibly from further west77 (ancestors of theAmerindians). Second, the notion that a shallow AC inhumans resists corneal freezing has no empirical support. Tomy knowledge, there has been only one attempt to assess theeffect of ACD on corneal temperature, and no associationbetween ACD and corneal temperature under cold condi-tions was found.78 However, this experiment would be worthrepeating with modern ocular thermography equipment andultrasound measurement of the AC. Third, to my knowledge,there is no evidence from a comparative anatomy perspectiveto support this hypothesis. Turner et al. have described theo-retical mechanisms which cold-blooded animals could use toavoid ocular freezing: (i) increasing aqueous saline con-centration, which depresses the freezing point (colligativemethod); (ii) glycopeptide antifreeze in the aqueous (non-colligative method); and (iii) maintaining aqueous in a super-cooled state and avoiding ice-forming nucleation.79 Theyprovide evidence that this latter method is adopted byAntarctic fish.79 However, examples of shallow ACs in cold-climate mammals are not forthcoming. For example, it is notknown if polar bears have shallower ACs than Malayan sunbears. But, interestingly, the Samoyed breed of dog, origi-nally, from Siberia, has a strong tendency to develop PACGwith increasing age.80 Finally, it is possible that a shallow AC
first emerged more recently in the Inuit population and sub-sequently appeared in the Mongolian population because ofreverse migration back to Asia across the Bering Straits.
ANOTHER EVOLUTIONARY EXPLANATION?
Could there be another selection advantage in a shallow AC?In taxonomy, humans are grouped with the Anthropoidea, asuborder of primates including monkeys and apes. Charac-teristic features of the Anthropoidea are their high levelof visual acuity and the relatively low corneal diameter/posterior nodal distance ratio.81 An increased posterior nodaldistance (approximating the vitreous chamber length) meansthat the retinal image will be spread over more photorecep-tors, thus, improving the acuity. The relatively small cornealdiameter is attributed to an adaptation to diurnality,81
an anatomical modification which reduces the maximumamount of light entry into the eye in animals predominantlyactive during daylight. It is unclear why the pupil alone cannot serve this function or why a large corneal diameter and alarge posterior nodal distance can not coexist. Nevertheless,this morphology does exist in the Anthropoidea and prob-ably has selection advantages. Given that for a fixed cornealcurvature, a reducing corneal diameter produces a reducingACD, it is possible that these traits are an adaptationto optimize resolving power under certain illuminationconditions. Why conditions in north-east Asia during thelate Pleistocene would favour this adaptation is unknown,and this hypothesis must be viewed as considerably moretenuous than Alsbirk’s.
MORE TO PACG than a shallow ACAlthough the relationship between ACD and ITC does notaffect the validity of the hypothesis, there is clearly more toITC than a shallow AC. The relationship between ACD andITC is complex and involves poorly understood factors.Aung et al. assessed the risk of angle closure (indicated byPAS) and GON among Chinese Singaporeans and Mongo-lians for different levels of ACD.11 The highest rate and riskof developing these two pathological entities, in both popu-lations, occurred with the shallowest ACs. However, the‘dose–response’ relationship between ACD and angle-closurewas different between these two populations. The authorspropose that this difference may reflect the contribution ofdifferent mechanisms responsible for angle closure in thetwo populations: mainly pupillary-block in Mongolians andmainly non-pupillary block in Chinese Singaporeans.11
Furthermore, Congdon et al. have reported that the meanACD does not differ between white and Taiwanese Chinesepopulations.82 Later, using biometric gonioscopy, Congdonet al. found that there was no significant difference in theoverall biometric gonioscopic measurments between black,white and Chinese populations.83 However, at younger ages,Chinese had deeper angles than white or black people,whereas the angles of older Chinese were significantlynarrower, a fact that may relate to near-task-induced axial
74 Casson
© 2008 The AuthorJournal compilation © 2008 Royal Australian and New Zealand College of Ophthalmologists

myopia in younger Chinese (a cohort effect rather thanan age-related effect). Oh et al. reported racial differencesin gonioscopy findings among white, black and Asianpopulations.84 They found that the iris insertion was mostanterior in the Asian individuals.84 Hence, there is likely tobe a complex age–related interaction between genes and theenvironment which affects the angle anatomy overlaid onany effects of ACD.
In conclusion, a shallow AC remains an undisputed riskfactor for PACG. ACD is an inheritable trait which isaffected by variables such as age and gender, but, allowingfor this, certain populations, particularly Inuit and Mongo-lians have shallower ACs than others. The most parsimoni-ous explanation for the shallow AC found in certain peopleof Asian extraction is that this trait originated in H. sapiens innorth-east Asia 40 000–15 000 years ago as an anatomicaladaptation to resist corneal freezing and that their descen-dants possess the trait.
ACKNOWLEDGEMENTS
Acknowledgements to Paul Foster (Moorfields Eye Hospitaland Institute of Ophthalmology, London, UK) and Poul-Helge Alsbirk (Department of Ophthalmology, HillerødHospital, Denmark) for reading and taking an interest indrafts of this manuscript.
REFERENCES
1. Quigley HA, Broman AT. The number of people with glau-coma worldwide in 2010 and 2020. Br J Ophthalmol 2006; 90:262–7.
2. Foster PJ, Buhrmann R, Quigley HA, Johnson GJ. The defini-tion and classification of glaucoma in prevalence surveys. Br JOphthalmol 2002; 86: 238–42.
3. He M, Foster PJ, Johnson GJ, Khaw PT. Angle-closure glau-coma in East Asian and European people. Different diseases?Eye 2006; 20: 3–12.
4. Johnson GJ, Foster PJ. Can we prevent angle-closure glaucoma?Eye 2005; 19: 1119–24.
5. Thomas R, Parikh R, Muliyil J, Kumar RS. Five-year risk ofprogression of primary angle closure to primary angle closureglaucoma: a population-based study. Acta Ophthalmol Scand2003; 81: 480–5.
6. Vijaya L, George R, Arvind H et al. Prevalence of angle-closuredisease in a rural southern Indian population. Arch Ophthalmol2006; 124: 403–9.
7. Casson RJ, Newland HS, McGovern S et al. Gonioscopy find-ings and prevalence of occludable angles in a Burmese popula-tion: the Meiktila EyeStudy. Br J Ophthalmol 2007; 9: 856–9.
8. Salmon JF. Predisposing factors for chronic angle-closureglaucoma. Prog Retin Eye Res 1999; 18: 121–32.
9. Alsbirk PH. Primary angle-closure glaucoma. Oculometry,epidemiology, and genetics in a high risk population. ActaOphthalmol Suppl 1976; 127: 5–31.
10. Alsbirk PH. Anatomical risk factors in primary angle-closureglaucoma. A ten year follow up survey based on limbal and axialanterior chamber depths in a high risk population. Int Ophthal-mol 1992; 16: 265–72.
11. Aung T, Nolan WP, Machin D et al. Anterior chamber depthand the risk of primary angle closure in 2 East Asianpopulations. Arch Ophthalmol 2005; 123: 527–32.
12. Lowe RF. Aetiology of the anatomical basis for primary angle-closure glaucoma. Biometrical comparisons between normaleyes and eyes with primary angle-closure glaucoma. Br J Oph-thalmol 1970; 54: 161–9.
13. Foster PJ, Oen FT, Machin D et al. The prevalence of glaucomain Chinese residents of Singapore: a cross-sectional populationsurvey of the Tanjong Pagar district. Arch Ophthalmol 2000; 118:1105–11.
14. George R, Paul PG, Baskaran M et al. Ocular biometry inoccludable angles and angle closure glaucoma: a populationbased survey. Br J Ophthalmol 2003; 87: 399–402.
15. Lowe RF. Aetiology of the anatomical basis for primary angle-closure glaucoma. Biometrical comparisons between normaleyes and eyes with primary angle-closure glaucoma. Br J Oph-thalmol 1970; 54: 161–9.
16. Shufelt C, Fraser-Bell S, Ying-Lai M, Torres M, Varma R.Refractive error, ocular biometry, and lens opalescence in anadult population. the Los Angeles Latino Eye Study. InvestOphthalmol Vis Sci 2005; 46: 4450–60.
17. Collins FS. What we do and don’t know about ‘race’, ‘ethnicity’,genetics and health at the dawn of the genome era. Nat Genet2004; 36 (Suppl. 11): S13–5.
18. Schwartz RS. Racial profiling in medical research. N Engl J Med2001; 344: 1392–3.
19. Tishkoff SA, Kidd KK. Implications of biogeography of humanpopulations for ‘race’ and medicine. Nat Genet 2004; 36 (Suppl.11): S21–7.
20. Burchard EG, Ziv E, Coyle N et al. The importance of race andethnic background in biomedical research and clinical practice.N Engl J Med 2003; 348: 1170–5.
21. Cavalli-Sforza LL. Human evolution and its relevance forgenetic epidemiology. Annu Rev Genomics Hum Genet 2007; 8:1–15.
22. Quigley HA, West SK, Rodriguez J, Munoz B, Klein R, SnyderR. The prevalence of glaucoma in a population-based study ofHispanic subjects: proyecto VER. Arch Ophthalmol 2001; 119:1819–26.
23. Clemmesen V, Alsbirk PH. Primary angle-closure glaucoma(a.c.g.) in Greenland. Acta Ophthalmol (Copenh) 1971; 49: 47–58.
24. Drance SM. Angle closure glaucoma among Canadian Eskimos.Can J Ophthalmol 1973; 8: 252–4.
25. Wojciechowski R, Congdon N, Anninger W, Teo Broman A.Age, gender, biometry, refractive error, and the anteriorchamber angle among Alaskan Eskimos. Ophthalmology 2003;110: 365–75.
26. Arkell SM, Lightman DA, Sommer A, Taylor HR, KorshinOM, Tielsch JM. The prevalence of glaucoma amongEskimos of northwest Alaska. Arch Ophthalmol 1987; 105: 482–5.
27. Salmon JF, Mermoud A, Ivey A, Swanevelder SA, Hoffman M.The prevalence of primary angle closure glaucoma and openangle glaucoma in Mamre, western Cape, South Africa. ArchOphthalmol 1993; 111: 1263–9.
28. Foster PJ, Baasanhu J, Alsbirk PH, Munkhbayar D, UranchimegD, Johnson GJ. Glaucoma in Mongolia. A population-basedsurvey in Hovsgol province, northern Mongolia. Arch Ophthal-mol 1996; 114: 1235–41.
Anterior chamber depth 75
© 2008 The AuthorJournal compilation © 2008 Royal Australian and New Zealand College of Ophthalmologists

29. He M, Foster PJ, Ge J et al. Prevalence and clinical characteris-tics of glaucoma in adult Chinese: a population-based study inLiwan District, Guangzhou. Invest Ophthalmol Vis Sci 2006; 47:2782–8.
30. Rahman MM, Rahman N, Foster PJ et al. The prevalence ofglaucoma in Bangladesh: a population based survey in Dhakadivision. Br J Ophthalmol 2004; 88: 1493–7.
31. Bourne RR, Sukudom P, Foster PJ et al. Prevalence of glaucomain Thailand: a population based survey in Rom Klao District,Bangkok. Br J Ophthalmol 2003; 87: 1069–74.
32. Ramakrishnan R, Nirmalan PK, Krishnadas R et al. Glaucoma ina rural population of southern India: the Aravind comprehen-sive eye survey. Ophthalmology 2003; 110: 1484–90.
33. Raychaudhuri A, Lahiri SK, Bandyopadhyay M, Foster PJ,Reeves BC, Johnson GJ. A population based survey of theprevalence and types of glaucoma in rural West Bengal: the WestBengal Glaucoma Study. Br J Ophthalmol 2005; 89: 1559–64.
34. Casson RJ, Newland HS, Muecke J et al. Prevalence of glau-coma in rural Myanmar: the Meiktila Eye Study. Br J Ophthalmol2007; 91: 710–4.
35. Mitchell P, Smith W, Attebo K, Healey PR. Prevalence ofopen-angle glaucoma in Australia. The Blue Mountains EyeStudy. Ophthalmology 1996; 103: 1661–9.
36. Vijaya L, George R, Paul PG et al. Prevalence of open-angleglaucoma in a rural south Indian population. Invest OphthalmolVis Sci 2005; 46: 4461–7.
37. Wolpoff MH, Hawks J, Caspari R. Multiregional, not multipleorigins. Am J Phys Anthropol 2000; 112: 129–36.
38. Cann RL, Stoneking M, Wilson AC. Mitochondrial DNA andhuman evolution. Nature 1987; 325: 31–6.
39. Wilson AC, Cann RL. The recent African genesis of humans.Sci Am 1992; 266: 68–73.
40. Yu N, Zhao Z, Fu YX et al. Global patterns of human DNAsequence variation in a 10-kb region on chromosome 1. Mol BiolEvol 2001; 18: 214–22.
41. Stringer CB, Andrews P. Genetic and fossil evidence for theorigin of modern humans. Science (New York, N. Y.) 1988; 239:1263–8.
42. Stringer CB. Reconstructing recent human evolution. PhilosTrans R Soc Lond B Biol Sci 1992; 337: 217–24.
43. Stringer C. Modern human origins: progress and prospects.Philos Trans R Soc Lond B Biol Sci 2002; 357: 563–79.
44. Quintana-Murci L, Semino O, Bandelt HJ, Passarino G,McElreavey K, Santachiara-Benerecetti AS. Genetic evidenceof an early exit of Homo sapiens sapiens from Africa througheastern Africa. Nat Genet 1999; 23: 437–41.
45. Macaulay V, Hill C, Achilli A et al. Single, rapid coastal settle-ment of Asia revealed by analysis of complete mitochondrialgenomes. Science 2005; 308: 1034–6.
46. Su B, Xiao J, Underhill P et al. Y-Chromosome evidencefor a northward migration of modern humans into EasternAsia during the last Ice Age. Am J Hum Genet 1999; 65: 1718–24.
47. Ke Y, Su B, Song X et al. African origin of modern humans inEast Asia: a tale of 12,000 Y chromosomes. Science (New York)2001; 292: 1151–3.
48. Jin L, Su B. Natives or immigrants: modern human origin in eastAsia. Nat Rev 2000; 1: 126–33.
49. Goebel T, Anthropology. The missing years for modernhumans. Science (New York) 2007; 315: 194–6.
50. Pitulko VV, Nikolsky PA, Girya EY et al. The Yana RHS site:humans in the Arctic before the last glacial maximum. Science(New York) 2004; 303: 52–6.
51. Anikovich MV, Sinitsyn AA, Hoffecker JF et al. Early UpperPaleolithic in Eastern Europe and implications for the dispersalof modern humans. Science (New York) 2007; 315: 223–6.
52. Lee TD, Zhao TM, Mickey R et al. The polymorphism of HLAantigens in the Chinese. Tissue Antigens 1988; 32: 188–208.
53. Zhao TM, Lee TD. Gm and Km allotypes in 74 Chinesepopulations: a hypothesis of the origin of the Chinese nation.Hum Genet 1989; 83: 101–10.
54. Yao YG, Kong QP, Bandelt HJ, Kivisild T, Zhang YP. Phylo-geographic differentiation of mitochondrial DNA in HanChinese. Am J Hum Genet 2002; 70: 635–51.
55. Capelli C, Wilson JF, Richards M et al. A predominantly indig-enous paternal heritage for the Austronesian-speaking peoplesof insular Southeast Asia and Oceania. Am J Hum Genet 2001; 68:432–43.
56. Schurr TG, Sherry ST. Mitochondrial DNA and Y chromo-some diversity and the peopling of the Americas: evolutionaryand demographic evidence. Am J Human Biol 2004; 16: 420–39.
57. Greenberg J, Turner CG, Zegura SL. The settlement of theAmericas: a comparison of linguistic, dental, and geneticevidence. Curr Anthropol 1986; 4: 477–97.
58. Williams RC, Steinberg AG, Gershowitz H et al. GM allotypesin Native Americans: evidence for three distinct migrationsacross the Bering land bridge. Am J Phys Anthropol 1985; 66:1–19.
59. Forster P, Harding R, Torroni A, Bandelt HJ. Origin and evo-lution of Native American mtDNA variation: a reappraisal. AmJ Hum Genet 1996; 59: 935–45.
60. Torroni A, Schurr TG, Cabell MF et al. Asian affinities andcontinental radiation of the four founding Native AmericanmtDNAs. Am J Hum Genet 1993; 53: 563–90.
61. Rubicz R, Schurr TG, Babb PL, Crawford MH. MitochondrialDNA variation and the origins of the Aleuts. Hum Biol 2003; 75:809–35.
62. Starikovskaya EB, Sukernik RI, Derbeneva OA et al. Mitochon-drial DNA diversity in indigenous populations of the southernextent of Siberia, and the origins of Native Americanhaplogroups. Ann Hum Genet 2005; 69 (Pt 1): 67–89.
63. Darwin C. On the Origin of Species by Means of Natural Selection, or thePreservation of Favoured Races in the Struggle for Life, 1st edn. London:John Murray, 1859.
64. Jablonski NG, Chaplin G. The evolution of human skincoloration. J Hum Evol 2000; 39: 57–106.
65. So JK. Human biological adaptation to arctic and subarcticzones. Annu Rev Anthropol 1980; 9: 63–82.
66. Coon CS, Garn SM, Birdsell JB. Races – A Study of the Problems ofRace Formation in Man. Thomas, IL: Springfield, 1965.
67. Beals KL. Head form and climatic stress. Am J Phys Anthropol1972; 37: 85–92.
68. Bergmann C. Über die Verhältnisse der wärmeökonomie derThiere zu ihrer Grösse. Annual Review of Anthropology 1847; 3:595–708.
69. Steegmann AT Jr. Human cold adaptation: an unfinishedagenda. Am J Hum Biol 2007; 19: 218–27.
70. Steegmann AT Jr. Cold adaptation and the human face. Am JPhys Anthropol 1970; 32: 243–50.
76 Casson
© 2008 The AuthorJournal compilation © 2008 Royal Australian and New Zealand College of Ophthalmologists

71. Columbo GL. Bilateral changes in the corneae followingexposure to cold in an airman. Br J Ophthalmol 1921; 5: 553–8.
72. Gruppo L, Mader TH, Wedmore I. Ocular problems in militaryfree fall parachutists. Mil Med 2002; 167: 797–800.
73. Kolstad A, Opsahl R Jr. Cold injury to corneal epithelium. Acause of blurred vision in cross-country skiers. Acta Ophthalmol(Copenh) 1969; 47: 656–9.
74. Duke-Elder S, MacFaul PA. Hypothermal injuries. InDuke-Elder S, ed. System of Ophthalmology. London: Kimpton,1972; 776–99.
75. Tuljapurkar SD, Puleston CO, Gurven MD. Why men matter:mating patterns drive evolution of human lifespan. PloS ONE2007; 2: e785.
76. Rennie J. 15 answers to creationist nonsense. Sci Am 2002; 287:78–85.
77. Brown MD, Hosseini SH, Torroni A et al. mtDNA, haplogroupX: an ancient link between Europe/Western Asia and NorthAmerica? Am J Hum Genet 1998; 63: 1852–61.
78. Rysa P, Sarvaranta J. Thermography of the eye during coldstress. Acta Ophthalmol Suppl 1974; 123: 234–9.
79. Turner JD, Scrag JD, DeVries AL. Ocular freezing avoidance inAntarctic fish. J Exp Biol 1985; 118: 121–31.
80. Ekesten B, Torrang I. Age-related changes in ocular distances innormal eyes of Samoyeds. Am J Vet Res 1995; 56: 127–33.
81. Ross CF. Into the light: the origin of Anthropoidea. Annu RevAnthropol 2000; 29: 147–94.
82. Congdon NG, Youlin Q, Quigley H et al. Biometry and primaryangle-closure glaucoma among Chinese, white, and blackpopulations. Ophthalmology 1997; 104: 1489–95.
83. Congdon NG, Foster PJ, Wamsley S et al. Biometric gonioscopyand the effects of age, race, and sex on the anterior chamberangle. Br J Ophthalmol 2002; 86: 18–22.
84. Oh YG, Minelli S, Spaeth GL, Steinman WC. The anteriorchamber angle is different in different racial groups: a gonio-scopic study. Eye 1994; 8 (Pt 1): 104–8.
Anterior chamber depth 77
© 2008 The AuthorJournal compilation © 2008 Royal Australian and New Zealand College of Ophthalmologists







![FOR REVIEW 1 Angle-Closure Detection in Anterior Segment ...with primary angle-closure glaucoma (PACG) being a major cause of blindness in Asia [1], [2]. Since vision loss from PACG](https://img.pdfslide.us/doc/110x75/5f33ab761bf82b40104258f2/for-review-1-angle-closure-detection-in-anterior-segment-with-primary-angle-closure.jpg)