Embed Size (px)
Citation preview

lable at ScienceDirect
Journal of Cancer Research and Practice 3 (2016) 132e135
Contents lists avai
Journal of Cancer Research and Practicejournal homepage: http: / /www.journals .e lsevier .com/journal-of-cancer-
research-and-pract ice
Case report
Antecedent presentation of aplastic anemia in a patient with diffuselarge B cell lymphoma
Chien-Ting Chen a, c, *, Yuan-Bin Yu a, c, Chun-Yu Liu b, c
a Division of Hematology, Department of Internal Medicine, Taipei Veterans General Hospital, Taipei, Taiwanb Division of Medical Oncology, Department of Oncology, Taipei Veterans General Hospital, Taipei, Taiwanc School of Medicine, National Yang-Ming University, Taipei, Taiwan
a r t i c l e i n f o
Article history:Received 12 January 2016Accepted 22 April 2016Available online 6 May 2016
Keywords:Aplastic anemiaLymphomaImmunogenic prodrome
* Corresponding author. Division of HematologMedicine, Taipei Veterans General Hospital, No.201, Strict, Taipei 11217, Taiwan.
E-mail address: [email protected] (C.-T. ChPeer review under responsibility of The Chinese O
http://dx.doi.org/10.1016/j.jcrpr.2016.04.0022311-3006/Copyright © 2016, The Chinese Oncolog(http://creativecommons.org/licenses/by-nc-nd/4.0/
a b s t r a c t
Immunological manifestation occasionally develops concurrently with lymphoid neoplasms, includingimmune thrombocytopenia and autoimmune hemolytic anemia, but rarely reported acquired aplasticanemia (AA). Here we present a female case of diffuse large B cell lymphoma (DLBCL) with antecedentpresentation of AA. Recovery of AA was noted after complete response to lymphoma treatment. Liter-ature regarding this issue was reviewed.Copyright © 2016, The Chinese Oncology Society. Production and hosting by Elsevier B.V. This is an open
access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Acquired aplastic anemia (AA) is an idiopathic disease man-ifested as unexplained bonemarrow hypocellularity and peripheralcytopenia. Clinical response to immuno-suppressive therapy (IST)1
and HLA-DR15 restriction2,3 manner both support an immunepathogenesis of idiopathic AA. It is caused by T-cell mediatedautoimmune response against immature HLA-DR (þ) hematopoi-etic progenitor cells. Rising evidence has shown that AA can also bea para-neoplastic phenomenon of lymphoid neoplasms.2,4,5
Lymphoid neoplasms may precede AA, or occur concomitantly ormetachronously with AA. While some cases with AA and lym-phoma can be para-neoplastic AA, some others may also be treat-ment related. Physicians might have dilemma in treatingsimultaneous AA and lymphoid neoplasms.5,6 For example, what isthe aim of therapy? Would the marrow hematopoiesis recover orget worse after chemotherapy for lymphoid neoplasms? Here wepresent a female case of diffuse large B cell lymphoma (DLBCL) withantecedent presentation of AA. Recovery of AA was noted after
y, Department of Internalec. 2, Shipai Rd., Beitou Dis-
en).ncology Society.
y Society. Production and hosting).
complete response to lymphoma treatment. We also reviewed theliterature regarding this issue.
2. Case report
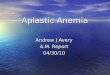
A 50-year-old female presented with splenomegaly (24 cm) andpancytopenia in Mar. 2014. A bone marrow biopsy revealed hypo-cellular marrow (<5%). Biochemistry tests including ANA and anti-Ds-DNA were normal. Flow cytometry revealed no CD59/CD55deficient clones. Aplastic anemia was diagnosed after serial work-ups. She initially received low dose prednisolone (10 mg/day).The hemogram improved but worsened again in Dec. 2014. Onexaminations showed white cell count (WBC) 810/ul; hemoglobin7.0 g/dl; platelet count 64,000/ul, and lactate dehydrogenase1041 U/L. An abdominal computed tomography revealed extensivelymphadenopathies mainly at retroperitoneum and massivesplenomegaly, with biopsy proved DLBCL (Fig. 1).
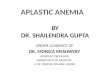
Repeated bone marrow biopsy again showed remarkablehypocellularity (Fig. 2). Concerning for profound myelosup-pression, we delivered chemotherapy with standard dose R-COPregimen (rituximab; cyclophosphamide; vincistine, and oral pred-nisolone), and we skipped anthracycline for the first 3 cycles due toconcern for profound marrow suppression. Long-acting filgrastim(pegylated granulocyte colony stimulating factor, [G-CSF]) wasgiven 24 h after chemotherapy. The patient stood 3 cycles of R-COPvery well and there was no occurrence of neutropenia. Interest-ingly, her WBC recovered shortly after the 1st cycle of R-COP
by Elsevier B.V. This is an open access article under the CC BY-NC-ND license

Fig. 1. (A) DLBCL diagnosed 9 months after diagnosis of aplastic anemia (HE stain, 1000X). (B) Strong CD20 positive (IHC stain for CD20, 1000X). (C) Massive splenomegaly atdiagnosis by abdominal CT.
Fig. 2. (A) Hypocellular marrow at initial presentation and (B) at diagnosis of DLBCL 9 months later, neither marrow involvement (both HE stain, 200X).
Fig. 3. Trends of white blood cell and platelet counts: transient response after IST usage but rapid recovery of hematopoiesis after 1st cycle of cytotoxic therapy.
C.-T. Chen et al. / Journal of Cancer Research and Practice 3 (2016) 132e135 133
(Fig. 3). Further 5 cycles of cytotoxic therapy with standard dose R-CEOP (rituximab; cyclophosphamide; epirubicin; vincistine, andoral prednisolone) regimen were given, and a follow-up abdomenCT showed marked decreased spleen size and resolution of previ-ous lymphadenopathy (Fig. 4). PET-CT confirmed complete meta-bolic response (Fig. 5). We accomplished successful stem cellharvest after documented recovery of hematopoiesis (Fig. 6). HerHLA-DR typing revealed DRB1*12.
3. Discussion
Immunological manifestations occasionally develop concur-rently with lymphoid neoplasms, including immune thrombocy-topenia and autoimmune hemolytic anemia, but rarely acquiredAA. Since Keisu et al notified one third of patients with initialdiagnosis of acquired idiopathic AA developed myelodysplasticsyndrome (MDS) or Non-Hodgkin lymphoma (NHL),7 there havebeen more and more studies finding chronological associationsbetween AA and NHL: some cases developed NHL during IST forinitially diagnosed AA.8e11 In literature review, NHL tends to occurshortly after IST for antecedent AA, predominantly 2e4 months

Fig. 4. Spleen involvement and lymphadenopathy at diagnosis of DLBCL (A); remarkable remission after 6 cycles of chemotherapy (B).
Fig. 5. Complete metabolic response by PET-CT.
Fig. 6. Recovery of hematopoiesis after complete remission of lymphoma, obtainedbefore stem cell harvest (HE stain, 200X).
C.-T. Chen et al. / Journal of Cancer Research and Practice 3 (2016) 132e135134
after IST.8,12,13 B-cell lymphomas are more likely. Dorr et al8 foundwithdrawal of IST plus radiotherapy attain complete remission.Suzuki et al13 used anthracycline-based chemotherapy to achieve apartial remission; while Saitoh et al reported a case that followed a
more fulminant course and showed no response to IST withdrawalor chemotherapy, which might be the nature of a late stage re-lapsing lymphoma.12 On the other hand, NHL could also developedafter a protracted use of IST, often 1.5 years later, in which T-cell14,15
or B-cell13,16 neoplasms evolved equally, and responded poorly tochemotherapy, carrying a grim prognosis.
HLA-DR15 might account for the paraneoplastic relationshipbetween lymphoproliferative disease (LPD) and preceding AA:Nissen et al reported a case of NHL with tumor regressioncompletely 10 days after diagnosis, accompanied with progressivepancytopenia, without treatment. The patient was positive for HLA-DR152; Jerez et al found a higher frequency of HLA-DR15 positivity(75% vs 44%, P ¼ 0.02) in patient with concomitant AA and T largegranular lymphocyte leukemia (T-LGL) than those who had no T-LGL clone.4 Though it is not HLA-DR15 in our case, whether otherimmunogenic HLA subtypes could predispose to both AA and LPDremains unclear. However, these evidences explained the para-neoplastic nature of AA as a collateral damage to hematopoieticprogenitor cell while launching immune attack toward occultlymphoma cells.6 As occult lymphoma cells tolerate, escape im-mune surveillance mainly via IST, and re-expand as clonal evolu-tion, it might be more aggressive than de novo lymphoma cells.2
Reviewing the literature, we knew that in cases of AA, use of ISTshould be cautious, as IST might accelerate occult lymphoma

C.-T. Chen et al. / Journal of Cancer Research and Practice 3 (2016) 132e135 135
escaping immune surveillance and evolving as a refractory lym-phoma. Second, in cases of AA and concomitant NHL, to choosecytotoxic chemotherapy or IST is an art. Depending on the intensityof immunogenic cytopenia and aggressiveness of NHL, physicianmight decide which aims should be treated first. In this case,splenomegaly at her first presentation is difficult to prove it lym-phoma. However, lately lymphadenopathy and worsening spleno-megaly confirmed lymphoma involvement. Her presentation of AAmight be an immunogenic prodrome of DLBCL rather than hyper-splenism related. It should be noted that splenomegaly are notfeatures of aplastic anemia; such findings suggest an alternativediagnosis such as a clonal myeloid or lymphoid disease,17 althoughthere has been a rare case report of splenomegaly associated withAA.18 There is also a possibility that this patient had both aplasticanemia and diffuse large B-cell lymphoma. Aplastic anemia wasrefractory to steroid but responsive to rituximab.19,20 Medinger et aldescribed two cases of concomitant AA and NHL,6 one case ofmultiple myeloma and concomitant AA. All of their hematopoiesisfailed recovery after short course of chemotherapy, despite allattaining complete remission. The former two received ISTand allo-HSCT respectively. Both restored hematopoiesis; the last onereceiving IST, having temporary recovery, but still died of aplasiaand infection. According to literature, hematopoiesis seldom re-covers in cases of NHL with antecedent or concomitant AA despiteremission of lymphoma. Nevertheless, here we provided a casereport of DLBCL with initial presentation of AA. Hematopoiesisrecovered after first cycle of chemotherapy, and later a successfulstem cell harvest after complete remission of lymphoma.
Author contributions
All authors performed and/or designed the research study,analysed the data, contributed to the development and revision ofthe manuscript and approved the final version for submission.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgements
This work was partially supported from the Taipei VeteransGeneral Hospital (V104C-182), and National Yang-Ming University.
References
1. Maciejewski JP, Steensma DP. Marrow Failure Syndromes. ASH-SEP. 14th ed.:450e452.
2. Nissen C, Stern M. Acquired immune mediated aplastic anemia: is it antineo-plastic? Autoimmun Rev. 2009;9:11e16.
3. Stern M, Buser AS, Lohri A, et al. Autoimmunity and malignancy in hema-tologyemore than an association. Crit Rev Oncol Hematol. 2007;63:100e110.
4. Jerez A, Clemente MJ, Makishima H, et al. STAT3 mutations indicate the pres-ence of subclinical T-cell clones in a subset of aplastic anemia and myelodys-plastic syndrome patients. Blood. 2013;122:2453e2459.
5. Tzankov A, Medinger M. Aplastic anemia: possible associations with lympho-proliferative neoplasms. Int J Lab Hematol. 2014;36:382e387.
6. Medinger M, Buser A, Stern M, et al. Aplastic anemia in association with alymphoproliferative neoplasm: coincidence or causality? Leuk Res. 2012;36:250e251.
7. Keisu M, Ost A. Diagnoses in patients with severe pancytopenia suspected ofhaving aplastic anemia. Eur J Haematol. 1990;45:11e14.
8. Dorr V, Doolittle G, Woodroof J. First report of a B cell lymphoproliferativedisorder arising in a patient treated with immune suppressants for severeaplastic anemia. Am J Hematol. 1996;52:108e113.
9. Paquette RL, Tebyani N, Frane M, et al. Long-term outcome of aplastic anemia inadults treated with antithymocyte globulin: comparison with bone marrowtransplantation. Blood. 1995;85:283e290.
10. Ruiz-Arguelles GJ, Gomez-Rangel JD. Long-term results of the immunosup-pressive treatment of patients with severe acquired aplastic anemia: a singleinstitution study. Acta Haematol. 2003;110:184e187.
11. Socie G, Henry-Amar M, Bacigalupo A, et al. Malignant tumors occurring aftertreatment of aplastic anemia. European Bone Marrow Transplantation-SevereAplastic Anaemia Working Party. N Engl J Med. 1993;329:1152e1157.
12. Saitoh T, Matsushima T, Yamane A, et al. Hodgkin lymphoma accompanied byaplastic anemia and polyclonal expansion of large granular lymphocytes. ActaHaematol. 2007;117:238e241.
13. Suzuki Y, Niitsu N, Hayama M, et al. Lymphoproliferative disorders afterimmunosuppressive therapy for aplastic anemia: a case report and literaturereview. Acta Haematol. 2009;121:21e26.
14. Hirose Y, Masaki Y, Ebata K, et al. T-Cell type acute lymphoblastic leukemiafollowing cyclosporin A therapy for aplastic anemia. Int J Hematol. 2001;73:226e229.
15. Sarangi JN, Kashyap R, Choudhry VP, et al. Severe aplastic anemia evolving intoT cell acute lymphoblastic leukemia. Eur J Haematol. 1999;63:269e271.
16. Takeuchi M, Soda R, Takahashi K, et al. Philadelphia chromosome positive acutelymphocytic leukemia arising from aplastic anemia. Am J Hematol. 2000;63:161e162.
17. Segel GB, Lichtman MA. Chapter 34: aplastic anemia: acquired and inherited.In: Williams Hematology. vol. 8. 2010:463e483.
18. Kaito K, Otsubo H, Ogasawara Y, et al. Aplastic anemia with giant splenomegalyand myelofibrosis successfully treated with antilymphocyte globulin. [Rinshoketsueki] Jpn J Clin Hematol. 1995;36:786e791.
19. Takamatsu H, Yagasaki H, Takahashi Y, et al. Aplastic anemia successfullytreated with rituximab: the possible role of aplastic anemia-associated auto-antibodies as a marker for response. Eur J Haematol. 2011;86:541e545.
20. Hansen PB, Lauritzen AM. Aplastic anemia successfully treated with rituximab.Am J Hematol. 2005;80:292e294.