Embed Size (px)
Citation preview

Announcements

Stat’s Seminars UpdateRest of the Fall
• Nov 4: Competing Risks, Frailty, and Violations of Proportional Hazards Tom Greene
• Nov 11: Alternatives to Cox regression Tom Greene & Nan Hu
• Dec 2: Chasing Tail(s): Statistical Intuition for High-Throughput Studies Ken Rice, University of Washington
• Dec 9: Case Control Study Design Carroll Sweeney
• Dec 16: Analyses for case-control studies Greg Stoddard
Statistical Methods in Progress Meetings:(also in WB – usually 238A or B) Charlie Casper: Nov 8, 10 AMMary Slattery: Nov 22, 10 AMAndrew Redd: Dec 6, 10 AM
Causal Modeling Workgroup:3rd Friday of Each Month (3PM, Div. EPI conference room, WB)

Other Announcements• Slides sets for seminars to be archived at
http://www.ccts.utah.edu/biostats/• R User’s group forming– Andrew Redd

Competing Risks, Frailty, and Violations of Proportional Hazards
Tom Greene

References
• Aalen O, Borgan O, Gjessing H. Survival and Event History Analysis: A Process Point of View, Springer, 2008
• Martinussen T, Scheike T. Dynamic Regression Models for Survival Data. Springer, 2010

Issues for Today• Understanding what standard Kaplan-Meier
curves and competing risk cumulative incidence curves really estimate in competing risk situations
• Same issue for standard hazard ratios and competing risk hazard ratios for subdistributions
• When to use standard methods or competing risk methods?

Issues for Today
• What is the difference between individual-level hazard ratios and population hazard ratios?
• What are the implications of variation in frailty for population hazard ratios in Cox regression ?
• What are the implications of variation in frailty for standard survival analysis in clinical trials?
• What if there are also competing risks?

Questions for Today• How can one check for non-proportional
hazards in Cox regression? • How can Cox regression be modified to
account for non-proportional hazards?

Quantities in Survival AnalysisS(t) = Pr(T > t) for a survival time TT may be subject to right censoring time C: we observe X = min(T,C)
The hazard rate λ(t) = event rate in time interval (t, t+ε) for the subgroup still at risk at time t
)()( tHetS
The cumulative hazard H(t) is the area under the λ(u) vs. u curve up to time t:
Relationship of survival and cumulative hazard:
t
duutH0
)()(

Estimating S(t) and H(t)
Nelson-Aalen estimator (discrete version):
t
j
j
n
dtH
0)(ˆ )(ˆ)(ˆ tHetS
Kaplan-Meier estimator:
tt j
j
jn
dtS 1)(ˆ
dj = # events at time tj; nj = # at risk at time tj

Cox Modelλ(t|Z) = λ0 (t) × exp( β Z)Z : Covariate(s) of interest λ0 (t): Baseline hazard function when Z = 0β: Cox regression coefficientsexp(β): Hazard ratios under the Cox model
Two key assumptions:1) T and C are independent given Z2) Proportional hazards

Competing Risks Events• An event whose occurrence precludes
the occurrence of an event of interest • Usually a clinical event, possibly having a
direct or indirect relationship with the event being analyzed

Competing Risk Subdistribution• The subdistribution, or cumulative incidence
probability, corresponding to the fraction of all patients with the event of interest, after accounting for “true censoring”
• Estimated by )(ˆ)(ˆ1.
jtt j
jdistsub tS
n
dtF
j
• tj : Event times (all event types)• dj: Number of pts with event of interest at tj
• nj: Number at risk at tj
• : Kaplan-Meier Curve for the composite outcome T = min(T1,T2)
S

Cumulative Incidence of ESRD, Death as competing risk Traditional Kaplan-Meier, ESRD censoring death
Traditional Kaplan-Meier, Death censoring ESRDCumulative Incidence, Death as competing risk
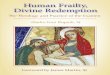
Traditional Kaplan Meier and Competing Risk Cumulative Incidence
Pts > 55 Years of Age
Months Follow-up
Example:Study of chronickidney disease;Death and End Stage Renal Disease(ESRD) are competing Risks

Interpretation of Kaplan Meier curves with competing risks
• The Kaplan Meier cumulative incidence curve indicates the event probability for a “virtual population” in which the competing risk does not occur, but which is linked to the studied population such that the target event occurs after a competing event at the same rate as for patients not experiencing the competing event.
• This virtual population is hard to fathom if the competing risk and target event are associated

Competing Risk Cumulative Incidence Curves for Time to ESRD or Death prior to ESRD
Age < 55 years Age > 55 years
Months Follow-up Months Follow-up

Alive without ESRD
Alive with ESRD prior to Death
Death prior to ESRD
Alive without ESRD
Alive with ESRD prior to Death
Death prior to ESRD
Competing Risk Formulation Decomposes Cohort Into 3 or More States
Age < 55 years Age > 55 years
Months Follow-up Months Follow-up

Conventional and Competing Risk Hazard Calculation
Competing Risk Calculation
Conventional Risk Calculation
nj(at risk)
nj(cmp.rsk)
nj(event)
nj(at risk)
nj(cmp.rsk)
nj(event)
Timetj- tj
Hazard Increment at time tj
).()( rskcmpnriskatn
d
jj
j
).()(
).()(
)( rskcmpnriskatn
rskcmpnriskatn
dd
riskatn
d
jj
jj
jj
j
j

Analysis of Subdistriubtion Hazard• Typically implemented using a proportional
model (Grey’s model), analogous to proportional Hazards Cox regression
• Implemented in R library cuminc• Can be viewed as assigning + infinity to
survival times for those with competing risks

What to do in practice?Example: RCT of effect of BP drug on CV composite; non-CV
death is competing risk. The trial’s focus is on the CV outcome, but the treatment may also affect non-CV death.
• Useful to display competing risk cumulative incidence• The standard analysis (using log rank or Cox) gives the correct
HR in the hypothetical “independent competing risk” universe– This remains true even if the treatment affects the competing risk
• This is not true of the HR under Gray’s competing risk model – Treatment can appear beneficial by increasing the competing risk
even if it has no effect on the target endpoint
• Hence, the “standard approach” is typically used to compare hazard rates in RCTs

A man is walking home one dark night when he sees a sage searching for something frantically under a streetlight.
“Teacher, what have you lost?” the man asks.
“I am searching for my key,” the sage says worriedly.
“I’ll help you look,” the man says and joins the search. Soon both are down on their knees under the streetlight, looking for the lost key. After some time, the man asks, “Tell me, teacher, do you remember where exactly you dropped the key?”
The sage waves his arm back toward the darkness and says, “Over there, in my house. I lost the key inside my house…” Shocked and exasperated, the man shouts, “Then why are you searching for the key out here in the street?”
“Because there is more light here than inside my house,” the teacher answers non-chalantly.
A Parable for Statisticians

Population and Individual Level Hazards
• The hazard in the Cox model
λ(t|Z) = λ0 (t) × exp( β Z) represents the “population hazard” given Z.
• The population hazard represents an average of individual level hazards among patients remaining at-risk
• The variation in individual level hazards, conditional on Z, is captured by the concept of frailty.

Proportional Frailty Model• Assume the hazard function for an subject
with frailty W is α(t|W) = W × α(t).• As before:• • The population hazard, λ(t) is related to the
standardized individual hazard α(t) by:
t
duutA0
)()(
))((}E{)( )( tAetS tWA L
))((
))(()()(
/
tA
tAtt
LL
Standardized individual hazard,
when W = 1

Proportional Frailty Model• Special Case: Assume W is gamma distributed
with mean 1 and variance δ• Then
)(1
)()(
tA
tt
Time
δ=0
δ=0.4
δ=1δ=3
Relationship of λ(t) with α(t) if α(t) = t2

Relationship of Population and Individual Hazard Ratios
• Suppose the proportional frailty model holds in two groups, with gamma frailties with mean 1 and variance δ within each group.
• If the individual hazards in 2 groups are W1rα(t) and W2α(t), so the individual HR is r, then
)(1
)(1
)(
)(
1
2
tAr
tAr
t
t
Attenuates towards 1 as t increases

Attenuation in Population HR Due to Frailty Variance
δ=0
δ=0.40
δ=1.00
δ=3.00
Assumes r = 4, α(t) = 0.5(i.e., ~40%with events in 1 yr)

Impact of Immediate Attenuation of Patient-Level HR to 1 Under Frailty
VariationAssumes 1)δ=12)r(t)=0.5 for
first year, r(t) = 1 after1 year
3) α(t) = 1

Competing Risks and False ProtectivityDifferential Survival Bias
Alive without
Event
Event B
Event C
WB αB(t)
WC αC(t)
WB= Y0 + Y2
WC= Y0 + Y3
Y0, Y2, Y3
independentgammas withmean 1 and variances δ0, δ2, and δ3
)()((42
1
)(42
1)()(
02 tAtAtAtt
CBBBB
Then
A treatment which has no effect on αB(t) but increases αC(t) will have lower λB, and thus appear protective for event B.

Practical Implications • Variation in population hazards ratio over
time depends both on variation in individual hazards ratio and to frailty selection
• It is often found that HRs attenuate towards 1 or reverse over time, or among “survivors” who reach an advance stage of a chronic disease (e.g., those with end stage renal disease)

Relative Mortality for Norwegian Men1901-1905 compared to 1991
Horizontal line indicates relative risk of 1
From “Statistics Norway” as reproduced in Aalen O, Survival and Event History Analysis

Practical Implications • Prevailing practice is to avoid covariate
adjustment for survival outcomes in RCTs.• But adjustment for strong prognostic factors
can:– Reduce conservative bias in estimated treatment
effect– Increase power – Reduce differential survival bias

Practical Implications • Three approaches to estimating effects on
individual hazards:– Analysis of repeat event data– Joint analysis of longitudinal and time-to-event
outcomes – Use background knowledge to posit assumptions for
frailty distribution and/or on the mathematical form of α(t)

Evaluation of Proportional Hazards
• Parametric models for change in hazard ratios over time
• Non-parametric smooths of Schoenfeld residuals
• Non-parametric models for multiplicative hazards

Parametric models for change in hazard ratios over time
Example: • Cox Regression of Effects of Dose Group
(Ktv_grp) and baseline serum albumin (Balb) in the HEMO Study
• RCT with 871 deaths in 1871 patients; planned follow-up 1.5 to 7 years.

Parametric models for change in hazard ratios over time
1) Test for linear interactions of predictors with follow-up time proc phreg data=demsum01 ; model fu_yr * ev_d(0) = ktv_grp balb ktv_grpt balbt; ktv_grpt = ktv_grp*fu_yr; balbt = balb*fu_yr;
Parameter Standard Parameter DF Estimate Error Chi-Square Pr > ChiSq
KTV_GRP 1 -0.06933 0.12112 0.3277 0.5670 BALB 1 -1.50469 0.17279 75.8320 <.0001 Ktv_grpt 1 0.00686 0.04406 0.0243 0.8762 Balbt 1 0.16874 0.06378 7.0001 0.0082
HR for baseline albumin (in g/dL) is 0.22 at time 0, but attenuates by a factor of exp(0.1687) = 1.184 per year

Parametric models for change in hazard ratios over time
2) Test for interactions of predictors with time period (> 1 yr vs. < 1yr) proc phreg data=demsum01 ; model fu_yr * ev_d(0) = Ktv_grp1 Balb1 Ktv_grp2 Balb2; if fu_yr > 1 then period =1; if . < fu_yr <= 1 then period = 0; Ktv_grp1 = ktv_grp*(1-period); Balb1 = balb*(1-period); Ktv_grp2 = ktv_grp*period; Balb2 = balb*period; PropHazKtv: test Ktv_grp1=Ktv_grp2; PropHazBalb: test Balb1 = Balb2;

Parametric models for change in hazard ratios over time
2) Test for interactions of predictors with time period (> 1 yr vs. < 1yr)
Parameter Standard Parameter DF Estimate Error Chi-Square Pr > ChiSq
Ktv_grp1 1 -0.07569 0.13413 0.3185 0.5725 Balb1 1 -1.58168 0.18855 70.3661 <.0001 Ktv_grp2 1 -0.04680 0.07861 0.3545 0.5516 Balb2 1 -0.95959 0.11553 68.9860 <.0001
Wald Label Chi-Square DF Pr > ChiSq
PropHazKtv 0.0345 1 0.8526 PropHazBalb 7.9139 1 0.0049

Plots of Schoenfeld ResidualsR Code:require(survival)HEMOCox<-coxph(Surv(fu_yr,EV_D) ~ KTV_GRP+BALB,data=hemodat)HEMOPropchk<-cox.zph(HEMOCox)HEMOPropchk
plot(HEMOPropchk,var="KTV_GRP")plot(HEMOPropchk,var="BALB")plot(HEMOPropchk,var=“KTV_GRP",resid=FALSE)plot(HEMOPropchk,var="BALB",resid=FALSE)
rho chisq pKTV_GRP 0.0049 0.0209 0.88510BALB 0.0968 8.2343 0.00411GLOBAL NA 8.2570 0.01611

Schoenfeld Residual Plots with Cubic Spline Smooths: R Output
For KTV_GRP For Baseline Albumin

Schoenfeld Residual Plots with Cubic Spline Smooths: R Output(Omitting the residuals)
For KTV_GRP For Baseline Albumin

Multiplicative Hazards with Time Varying Coefficients
• Standard Cox Proportional Hazards Model λ(t|Z) = λ0 (t) × exp(β Z)
• Cox Proportional Hazards Model with Time-Dependent Covariates λ(t|Z) = λ0 (t) × exp(β Z(t))
• Multiplicative Hazards Model with Fixed Covariates and Time-Varying Coefficients λ(t|Z) = λ0 (t) × exp(β(t) Z)
• Multiplicative Hazards Model with Time-Dependent Covariates and Time-Varying Coefficients λ(t|Z) = λ0 (t) × exp(β(t) Z(t))

Multiplicative Hazards Model with Fixed Covariates and Time-Varying Coefficients• Model
λ(t|Z) = λ0 (t) × exp(β(t) Z)
• Useful if proportional hazards assumption in doubt,and you don’t want to assume a particular parametric model for change in HR over time
• Estimands are cumulative Cox regression coefficients
• Can use timereg package in R (if you are careful to center predictor variables)
t
jj duutB0
)()(

Multiplicative Hazards Model with Fixed Covariates and Time-Varying Coefficients
summary(fit)
Multiplicative Hazard Model
Test for nonparametric terms
Test for non-significant effects Supremum-test of significance p-value H_0: B(t)=0cKTV_GRP 1.38 0.931cBALB 11.30 0.000
Test for time invariant effects Kolmogorov-Smirnov test p-value H_0:constant effectcKTV_GRP 0.163 0.986cBALB 0.833 0.038 Cramer von Mises test p-value H_0:constant effectcKTV_GRP 0.015 0.993cBALB 1.040 0.026

Multiplicative Hazards Model with Fixed Covariates and Time-Varying Coefficients
> cBALB<-BALB – mean(BALB)> cKTV_GRP <- KTV_GRP – mean(KTV_GRP) > require(timereg)> fit<-timecox(Surv(fu_yr,EV_D)~KTV_GRP+cBALB,max.time=5)> summary(fit)> par(mfrow(1,2)> plot(fit,c(2,3))
R Code:

Multiplicative Hazards Model with Fixed Covariates and Time-Varying Coefficients

Next WeekAlternatives to the Cox Model• Aalen’s Additive Hazards Model• Accelerated Failure Time Models• Proportional Odds Models for Survival Data


















![Frailty pathway [970kb]](https://img.pdfslide.us/doc/110x75/588da5761a28ab737b8b4e2c/frailty-pathway-970kb.jpg)