-
Angioplasty and Stenting of the Great VesselsJ. Bayne Selby,
Jr., MDMedical University of South CarolinaInstitut fur
Diagnostische und Interventionelle RadiologieUniversitat Frankfurt
am MainJune 7, 2006
-
History1964 First angioplasty report by Dotter and Judkins1980
First subclavian angioplasty report by Bachman and Kim1991 Report
by Soulen for subclavian angioplasty proximal to LIMA coronary
bypass graft1993 First subclavian stent use reported by Mathias
-
OverviewStenoses/occlusion in the great vessels usually
represent difficult areas to access surgicallyResults with
angioplasty have been uniformly good in stenosesUse of stents has
resulted in similar results for complete occlusionsRole of distal
embolic protection devices unclear at this time
-
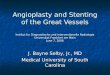
95% Left Subclavian StenosisPrePostPost Aortagram
-
Left Subclavian Stenosis Pre, Post, and 6 month
follow-upPreImmediate Post6 months post
-
Patient SelectionAs always, treatment should only be performed
in those patients who have both a hemodynamically significant
lesion and appropriate corresponding symptoms
-
Anatomic LocationsLeft Subclavian (most
common)BrachiocephalicLeft Common Carotid OriginRight Subclavian
(often in aberrant vessel)
-
IndicationsUpper Extremity IschemiaArm ClaudicationEmboli from
lesion to handCerebral IschemiaAnterior (carotid)
symptomsVertebro-basilar Insufficiency w/wo subclavian
stealDiminished Inflow to GraftAngina in patient with
LIMAClaudication in patient with Ax-fem
-
DiagnosisClinical HistoryBLOOD PRESSURES in both arms
simpleMRACTAConventional Angiography AP and LAO
-
Diagnostic AngiographyEvaluate for central lesion
(stenosis/occlusion)Evaluate for evidence of distal emboli (then do
echocardiography of heart)Evaluate for vasospastic disorder, e.g.,
Raynauds (do angio before and after vasodilator)Evaluate for
thoracic outlet syndrome (do abduction and adduction angio)
-
Great Vessel Angioplasty/Stent Technique
Do baseline neurological examInitial high quality diagnostic
thoracic aortagramArteriography of distal vascular beds as allowed
by degree of diseaseFirst attempt to cross lesion from belowUse
brachial approach if necessaryGive Heparin once lesion has been
crossed (2,000-3,000 units)
-
Great Vessel Angioplasty/Stent TechniqueHave nurse perform
neurological tests on patients at regular intervals (e.g., speak,
grip strength, smile, wiggle toes)Use guiding catheter or sheathTry
to use appropriate ballon size for initial dilatation, but
pre-dilate if lesion is too tight to get acrossLeave balloon up for
10 secondsStent for >30% residual stenosis, dissection,
recoilConsider primary stent based on appearance of lesion
-
Brachiocephalic (Innominate) Artery Angioplasty99% stenosis at
originof brachiocephalic arteryCross lesion from an axillary
approach
-
Brachiocephalic (Innominate) Artery Angioplasty10 mm balloon
with waist10 mm balloon fully inflated
- Brachiocephalic (Innominate) Artery AngioplastyInitial 99%
stenosisFinal with residual stenosis
-
Subclavian Stenosis proximal to LIMA coronary graft no
stentDiffuse stenosis poor fillingof the LIMA graftS/P Angioplasty
circa 1991
-
Stenosis in Single supra-aortic Vessel Now What?
-
Follow up MR? CT? Angio?Peloschek P., et al. The Role of
Multi-slice Spiral CT Angiography in Patient Management After
Endovascular Therapy. Cardiovascular and Interventional Radiology,
In Press
-
Subclavian Stenosis proximal to LIMA coronary graft with
stent
-
Stenosis within stent
-
Bifurcation LesionsCan occur at right subclavian right common
carotid bifurcationMust use RAO projection to evaluate
stenosisOptions include: 1) simple angioplasty2) kissing balloon
angioplasty3) simple stent4) kissing stents
-
Bifurcation LesionsSubclavian Steal95% stenosis in proximalright
subclavian artery
-
Bifurcation LesionsKissing balloon from femoral andright
axillary approachFinal ResultExcellent is the Enemy of Good!
-
Bifurcation LesionPulse Volume RecordingsRight ArmLeft
ArmFingers of Right Hand
-
Life Table Analysis30 Subclavian Angioplasty Patients University
of Virginia
-
Summary of Largest Series of PTA of Brachiocephalic Arterial
Stenoses
-
Summary of Series of Brachiocephalic Arterial Occlusions
-
ComplicationsPuncture site complications, femoral or
brachialRupture of vesselEmboli from angioplasty siteStent
misplacement
-
ComplicationsMathias, et al: 38 patients with total occlusions
No significant embolic occlusions
-
ComplicationsLiterature review by Kachel, et al: 774 supraaortic
lesions treated with PTA0.5% Major complications3.5% Minor
complications
-
Explanations20 second delay in restoration of antegrade flow in
vertebral artery following angioplasty Ringelstein, et al, Nuclear
Medicine dataLack of clinical significance of small emboli to
handPossible different response of large vessels to
angioplasty/stent (iliac vs. SFA emboli experience)
-
Still, now we have protection devices Landing zone for
protection device in supra-aortic angioplasty is often vessel too
largeProbably should use it when possible
-
Were not done yet!Articles to be published in 20066 articles on
results of simple angioplasty and/or stenting of great vessels3
articles on great vessel disease treatment in conjunction with
thoracic aortic stent graft2 articles on percutaneous treatment for
arteritis
-
ConclusionAngioplasty, with or without stenting is highly
effective for stenoses of the great vesselsOcclusive disease in the
great vessels should always be treated with stentLong term result
are excellent (70-90%), but follow up with CTA upon return of
symptoms may be necessaryConsider the use of distal embolic
protection, although rate of complications has been low without
it
-
SummaryAngioplasty of the Great Vessels can be a useful
treatment in a surgically difficult areaResults mimic those of the
common iliac arteries (>90% success) and have further improved
with the use of stents, particularly for occlusionsImprovements in
technology have increased the technical success in
occlusionsComplications are low, but remain a hazard consideration
should be given to the use of distal protection devices when
anatomy is suitable