Embed Size (px)
Citation preview

Angioplasty and Stenting of Angioplasty and Stenting of the Great Vesselsthe Great Vessels
J. Bayne Selby, Jr., MDJ. Bayne Selby, Jr., MD
Medical University of South Medical University of South CarolinaCarolina
Institut fur Diagnostische und Interventionelle RadiologieUniversitat Frankfurt am Main
June 7, 2006

HistoryHistory
1964 First angioplasty report by Dotter and 1964 First angioplasty report by Dotter and JudkinsJudkins
1980 First subclavian angioplasty report by 1980 First subclavian angioplasty report by Bachman and KimBachman and Kim
1991 Report by Soulen for subclavian 1991 Report by Soulen for subclavian angioplasty proximal to LIMA coronary bypass angioplasty proximal to LIMA coronary bypass graftgraft
1993 First subclavian stent use reported by 1993 First subclavian stent use reported by MathiasMathias

OverviewOverview
Stenoses/occlusion in the great vessels Stenoses/occlusion in the great vessels usually represent difficult areas to access usually represent difficult areas to access surgicallysurgically
Results with angioplasty have been Results with angioplasty have been uniformly good in stenosesuniformly good in stenoses
Use of stents has resulted in similar results Use of stents has resulted in similar results for complete occlusionsfor complete occlusions
Role of distal embolic protection devices Role of distal embolic protection devices unclear at this timeunclear at this time

95% Left Subclavian Stenosis95% Left Subclavian Stenosis
Pre Post Post Aortagram

Left Subclavian Stenosis – Pre, Left Subclavian Stenosis – Pre, Post, and 6 month follow-upPost, and 6 month follow-up
Pre Immediate Post 6 months post
Patient SelectionPatient Selection
As always, treatment should only be As always, treatment should only be performed in those patients who have performed in those patients who have both a hemodynamically significant lesion both a hemodynamically significant lesion and appropriate corresponding symptomsand appropriate corresponding symptoms

Anatomic LocationsAnatomic Locations
Left Subclavian (most common)Left Subclavian (most common) BrachiocephalicBrachiocephalic Left Common Carotid OriginLeft Common Carotid Origin Right Subclavian (often in aberrant vessel)Right Subclavian (often in aberrant vessel)

IndicationsIndications
Upper Extremity IschemiaUpper Extremity Ischemia Arm ClaudicationArm Claudication Emboli from lesion to handEmboli from lesion to hand
Cerebral IschemiaCerebral Ischemia Anterior (carotid) symptomsAnterior (carotid) symptoms Vertebro-basilar Insufficiency w/wo subclavian stealVertebro-basilar Insufficiency w/wo subclavian steal
Diminished Inflow to GraftDiminished Inflow to Graft Angina in patient with LIMAAngina in patient with LIMA Claudication in patient with Ax-femClaudication in patient with Ax-fem

DiagnosisDiagnosis
Clinical HistoryClinical History BLOOD PRESSURES in both arms – simpleBLOOD PRESSURES in both arms – simple MRAMRA CTACTA Conventional Angiography – AP and LAOConventional Angiography – AP and LAO

Diagnostic AngiographyDiagnostic Angiography
Evaluate for central lesion (stenosis/occlusion)Evaluate for central lesion (stenosis/occlusion) Evaluate for evidence of distal emboli (then do Evaluate for evidence of distal emboli (then do
echocardiography of heart)echocardiography of heart) Evaluate for vasospastic disorder, e.g., Evaluate for vasospastic disorder, e.g.,
Raynaud’s (do angio before and after Raynaud’s (do angio before and after vasodilator)vasodilator)
Evaluate for thoracic outlet syndrome (do Evaluate for thoracic outlet syndrome (do abduction and adduction angio)abduction and adduction angio)

Great Vessel Angioplasty/Stent Great Vessel Angioplasty/Stent TechniqueTechnique
Do baseline neurological examDo baseline neurological exam Initial high quality diagnostic thoracic aortagramInitial high quality diagnostic thoracic aortagram Arteriography of distal vascular beds as allowed Arteriography of distal vascular beds as allowed
by degree of diseaseby degree of disease First attempt to cross lesion from belowFirst attempt to cross lesion from below Use brachial approach if necessaryUse brachial approach if necessary Give Heparin once lesion has been crossed Give Heparin once lesion has been crossed
(2,000-3,000 units)(2,000-3,000 units)

Great Vessel Angioplasty/Stent Great Vessel Angioplasty/Stent TechniqueTechnique
Have nurse perform neurological tests on patients at Have nurse perform neurological tests on patients at regular intervals (e.g., speak, grip strength, smile, regular intervals (e.g., speak, grip strength, smile, wiggle toes)wiggle toes)
Use guiding catheter or sheathUse guiding catheter or sheath Try to use appropriate ballon size for initial dilatation, Try to use appropriate ballon size for initial dilatation,
but pre-dilate if lesion is too tight to get acrossbut pre-dilate if lesion is too tight to get across Leave balloon up for 10 secondsLeave balloon up for 10 seconds Stent for >30% residual stenosis, dissection, recoilStent for >30% residual stenosis, dissection, recoil Consider primary stent based on appearance of lesionConsider primary stent based on appearance of lesion

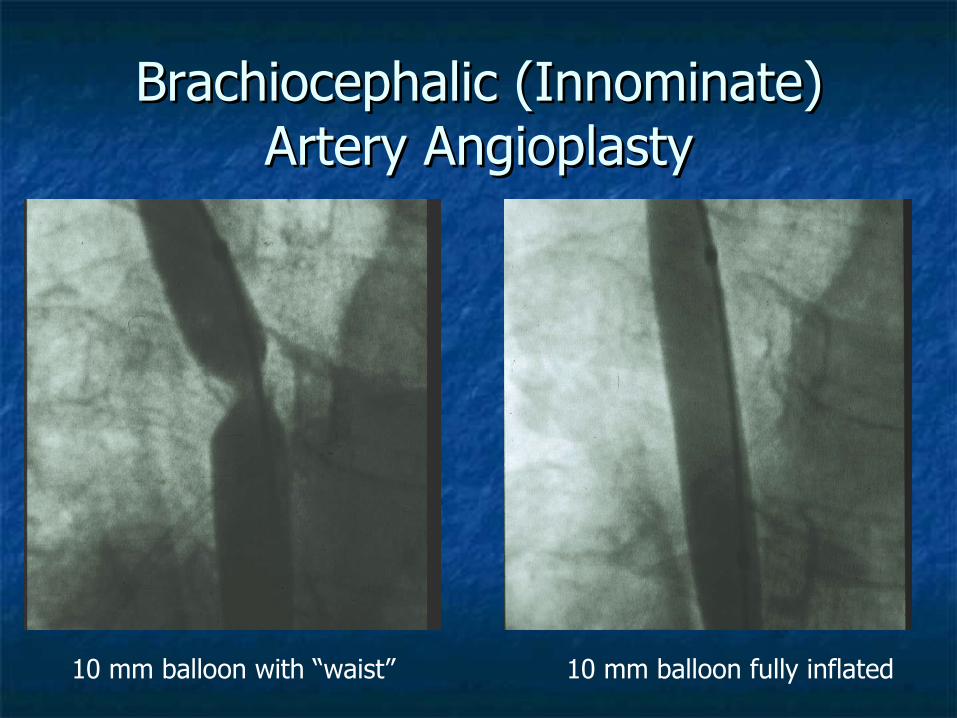
Brachiocephalic (Innominate) Brachiocephalic (Innominate) Artery AngioplastyArtery Angioplasty
99% stenosis at originof brachiocephalic artery
Cross lesion from an axillary approach
Brachiocephalic (Innominate) Brachiocephalic (Innominate) Artery AngioplastyArtery Angioplasty
10 mm balloon with “waist” 10 mm balloon fully inflated

Brachiocephalic (Innominate) Brachiocephalic (Innominate) Artery AngioplastyArtery Angioplasty
Initial 99% stenosis Final with residual stenosis <30%Note post stenotic dilatation
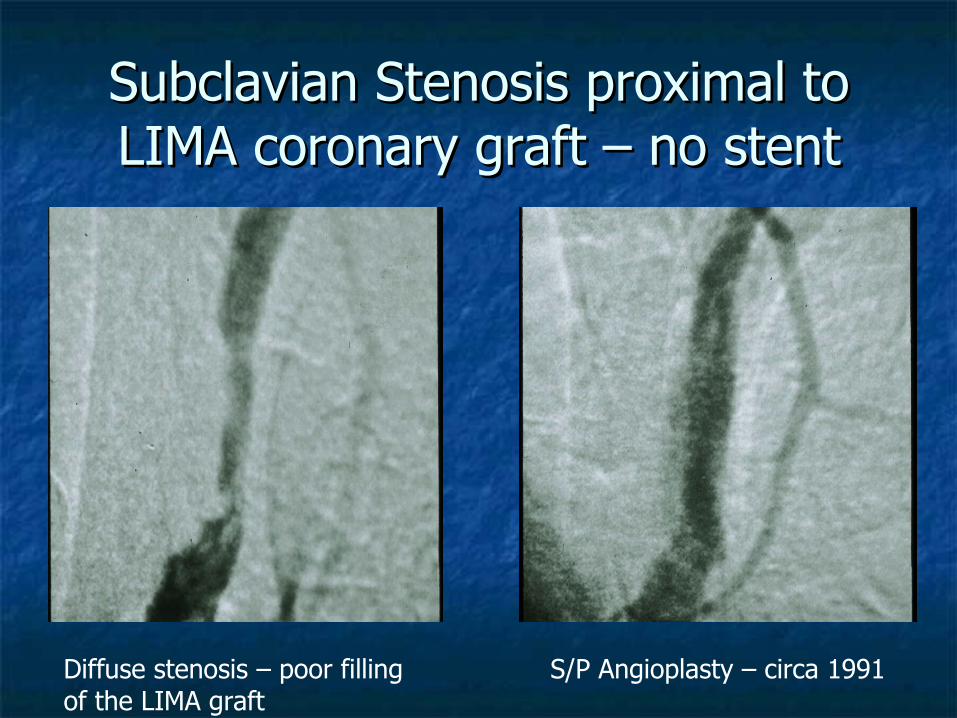
Subclavian Stenosis proximal to Subclavian Stenosis proximal to LIMA coronary graft – no stentLIMA coronary graft – no stent
Diffuse stenosis – poor fillingof the LIMA graft
S/P Angioplasty – circa 1991

Stenosis in Single supra-aortic Stenosis in Single supra-aortic Vessel – Now What?Vessel – Now What?

Follow up – MR? CT? Angio?Follow up – MR? CT? Angio?
Peloschek P., et al. The Role of Multi-slice Peloschek P., et al. The Role of Multi-slice Spiral CT Angiography in Patient Spiral CT Angiography in Patient Management After Endovascular Therapy. Management After Endovascular Therapy. Cardiovascular and Interventional Cardiovascular and Interventional Radiology, In PressRadiology, In Press

Subclavian Stenosis proximal to Subclavian Stenosis proximal to LIMA coronary graft – with stentLIMA coronary graft – with stent

Stenosis within stentStenosis within stent

Bifurcation LesionsBifurcation Lesions
Can occur at right subclavian – right Can occur at right subclavian – right common carotid bifurcationcommon carotid bifurcation
Must use RAO projection to evaluate Must use RAO projection to evaluate stenosisstenosis
Options include: Options include: 1) simple angioplasty1) simple angioplasty 2) kissing balloon angioplasty2) kissing balloon angioplasty 3) simple stent3) simple stent 4) kissing stents4) kissing stents

Bifurcation LesionsBifurcation Lesions
Subclavian Steal95% stenosis in proximalright subclavian artery

Bifurcation LesionsBifurcation Lesions
Kissing balloon from femoral andright axillary approach
Final ResultExcellent is the Enemy of Good!

Bifurcation LesionBifurcation LesionPulse Volume RecordingsPulse Volume Recordings
Right Arm Left ArmFingers of Right Hand

Life Table AnalysisLife Table Analysis30 Subclavian Angioplasty Patients 30 Subclavian Angioplasty Patients
University of VirginiaUniversity of Virginia

Summary of Largest Series of PTA of Summary of Largest Series of PTA of Brachiocephalic Arterial StenosesBrachiocephalic Arterial Stenoses
-164239/305 (78%)
380/396 (96%)
396OVERALL
(30)1-(54%)21/23 (91%)23Farina et al
6-60 (25)2118/21 (86%)21/23 (91%)23Wilms et al
9-101 (41)4137/44 (84%)45/46 (98%)46Millaire et al
18-26--17/21 (81%)18/21 (86%)21Erbstein et al
8-111 (50)0017/25 (68%)23/25 (92%)25Romanowshi et al
2-90 (26)2130/34 (89%)34/34 (100%)34Insall et al
(37)11-26/29 (90%)29Burke et al
-00-35/35 (100%)35Vitek et al
8-60 (27)0016/16 (100%)16/16 (100%)16Motarjeme et al
2-73 (28)2021/22 (95%)22/22 (100%)22Dorros et al
6-48 (29)0034/43 (79%)40/43 (93%)43Hebrang et al
3-109 (58)2045/47 (96%)47/47 (100%)47Kachel et al
4-88 (36)2031/32 (97%)32/32 (100%)32Selby et al
Months Follow-up (mean)
Complications - Other
Complications – Neurologic
Clinical SuccessTechnical Success
No. of LesionsAuthors

Summary of Series of Brachiocephalic Summary of Series of Brachiocephalic Arterial OcclusionsArterial Occlusions
1936/46 (78%)68/93 (73%)93Overall
5-5/5 (100/5)5Bates
73/7 (43%)7/8 (88%)8Duber et al
732/38 (84%)38/46 (83%)46Mathias et al
01/1 (100%)1/7 (15%)7Motarjeme et al
0-11/11 (100%)11Dorros et al
0-5/9 (56%)9Hebrang et al
0-1/7 (15%)7Kachel et al
No. of Patients Receiving Stents
Clinical SuccessTechnical SuccessNo. of OcclusionsAuthors

ComplicationsComplications
Puncture site complications, femoral or Puncture site complications, femoral or brachialbrachial
Rupture of vesselRupture of vessel Emboli from angioplasty siteEmboli from angioplasty site Stent misplacementStent misplacement

ComplicationsComplications
Mathias, et al: 38 patients with total Mathias, et al: 38 patients with total occlusions – No significant embolic occlusions – No significant embolic occlusionsocclusions

ComplicationsComplications
Literature review by Kachel, et al: Literature review by Kachel, et al: 774 supraaortic lesions treated with PTA774 supraaortic lesions treated with PTA 0.5% Major complications0.5% Major complications 3.5% Minor complications3.5% Minor complications

ExplanationsExplanations
20 second delay in restoration of antegrade flow 20 second delay in restoration of antegrade flow in vertebral artery following angioplasty – in vertebral artery following angioplasty – Ringelstein, et al, Nuclear Medicine dataRingelstein, et al, Nuclear Medicine data
Lack of clinical significance of small emboli to Lack of clinical significance of small emboli to handhand
Possible different response of large vessels to Possible different response of large vessels to angioplasty/stent (iliac vs. SFA emboli angioplasty/stent (iliac vs. SFA emboli experience)experience)

Still, now we have protection Still, now we have protection devices …devices …
Landing zone for protection device in Landing zone for protection device in supra-aortic angioplasty is often vessel too supra-aortic angioplasty is often vessel too largelarge
Probably should use it when possibleProbably should use it when possible

We’re not done yet!We’re not done yet!Articles to be published in 2006Articles to be published in 2006
6 articles on results of simple angioplasty 6 articles on results of simple angioplasty and/or stenting of great vesselsand/or stenting of great vessels
3 articles on great vessel disease 3 articles on great vessel disease treatment in conjunction with thoracic treatment in conjunction with thoracic aortic stent graftaortic stent graft
2 articles on percutaneous treatment for 2 articles on percutaneous treatment for arteritisarteritis

ConclusionConclusion
Angioplasty, with or without stenting is highly Angioplasty, with or without stenting is highly effective for stenoses of the great vesselseffective for stenoses of the great vessels
Occlusive disease in the great vessels should Occlusive disease in the great vessels should always be treated with stentalways be treated with stent
Long term result are excellent (70-90%), but Long term result are excellent (70-90%), but follow –up with CTA upon return of symptoms follow –up with CTA upon return of symptoms may be necessarymay be necessary
Consider the use of distal embolic protection, Consider the use of distal embolic protection, although rate of complications has been low although rate of complications has been low without itwithout it

SummarySummary
Angioplasty of the Great Vessels can be a useful Angioplasty of the Great Vessels can be a useful treatment in a surgically difficult areatreatment in a surgically difficult area
Results mimic those of the common iliac arteries Results mimic those of the common iliac arteries (>90% success) and have further improved with (>90% success) and have further improved with the use of stents, particularly for occlusionsthe use of stents, particularly for occlusions
Improvements in technology have increased the Improvements in technology have increased the technical success in occlusionstechnical success in occlusions
Complications are low, but remain a hazard – Complications are low, but remain a hazard – consideration should be given to the use of consideration should be given to the use of distal protection devices when anatomy is distal protection devices when anatomy is suitablesuitable





























