Embed Size (px)
Citation preview

PEDIATRIC DENTISTRY/Copyright’9 1981 byThe American Academy of Pedodontics/Vol. 3, No. 3 CAS
Dental management of idiopathic aplasticanemia: report of a case
James E. Jones, DMD, MSThomas D. Coates, MDCharles Poland, DDS
AbstractAplastic anemia is a serious and often fatal hematological
disorder characterized by hypoplastic bone marrow andperipheral pancytopenia. Epistaxis, oral lesions and gingivalhemorrhage often necessitates multiple platelet transfusionsin these patients. The use of aminocaproic acid to controlhemorrhagic episodes has been especially beneficial inpatients with bone marrow hypoplasia as they often becomerefractory to repeated transfusions. In this casepresentation, a 15-year-old black female with idiopathicaplastic anemia was treated with a combination ofmodalities including initial platelet transfusion, oral hygiene
instruction, dental prophylaxis and systemic aminocaproicacid. The health of the oral tissues greatly improvedfollowing this regimen.
IntroductionAplastic anemia is a serious and often fatal hema-
tologic disorder characterized by hypoplastic bonemarrow and peripheral pancytopenia. Recently, theuse of systemic aminocaproic acida in these patientshas demonstrated positive results in the control oforal hemorrhagic episodes, thus reducing the need formultiple platelet transfusions.’ In this case presenta-tion, a 15-year-old black female with severe idiopathicaplastic anemia was treated with a combination ofmodalities, including initial platelet transfusion, oralhygiene instruction, dental prophylaxis and systemicaminocaproic acid. The oral tissues appeared clinicallyhealthy following this regimen.
Literature ReviewAplastic anemia was first described in 1888 by Ehr-
lich as a rapidly fatal hematologic disease seen inyoung adults between the ages of 15 and 30.2 Today,the concept of aplastic anemia has been broadened
Accepted: December 29, 1980
aNon-proprietary name and trademarks of drug: amniocaproic acid-- Amicar, Cuprocid.
since the disease has been known to occur at any age.Usually, the onset is gradual, but acute fulminatingcases have been reported?,4 The mortality in severecases is more than 50 percent during the first year andmay be greater than 70 percent at five years? Aplasticanemia is normochromic and normocytic, and mani-fests itself as a pancytopenia. The bone marrowis devoid of megakaryocytes, myeloid and erythroidprecursors?
Clinical signs and symptoms include: 1) severeweakness and dyspnea even after mild physical exer-tion, 2) pallor of the skin, 3) numbness and tingling the extremities, 4) decreased resistance to infection,and 5) petechiae of the skin and mucous membranes;These clinical manifestations are caused by the inabil-ity of the hematopoietic system to deliver enough redcells, white cells and platelets to the peripheral circu-lation. The specific clinical picture varies according tothe cell line predominantly affected. Oral signs in-clude: 1) spontaneous bleeding from the mucous mem-branes, 2) petechiae, 3) purpuric spots, and 4) frankhematomas of the mucosa, pharnyx and gingiva.
Aplastic anemia is generally recognized in twoforms: idiopathic and secondary. Idiopathic aplasticanemia affects young adults, progresses rapidly and isusually fatal. This form accounts for approximately 60percent of the reported cases? Secondary aplasticanemia is of known etiology and can affect individualsat any age. The prognosis, once again, is poor even ifthe causative agent is identified. Among the agents as-sociated with secondary aplastic anemia are: ionizingradiation, ~ Atabrine/° chloramphenicol/u2 benezene/TMgold compounds,’~ viral hepatitis, and miliary tubercu-losis?,~ Secondary aplastic anemia accounts for approxi-mately 40 percent of reported cases?
Report of CaseA 15-year-old black female was referred to the
James Whitcomb Riley Hospital for Children in
PEDIATRIC DENTISTRY: Volume 3, Number 3 267

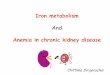
Figure 1. Initial intraoral view demonstrating gingivitis andspontaneous gingival hemorrhage.
March, 1979, with complaints of malaise and pro-longed epistaxis. The patient denied any episodes ofjaundice or hematuria. The family history was nega-tive for sickle cell anemia or Fanconi's anemia. Thepatient had been transfused with 5 units of randomdonor platelets and packed cells prior to arrival atRiley Hospital.
Physical examination revealed a well-developedblack female in no acute distress. Heart rate was 80,respiratory rate 18, weight 38.1 Kg. The examinationwas unremarkable with the exception of mucosal andpetechial hemorrhage. Specifically, there was no hepa-tosplenomegaly or lymphadenopathy. No abnormalityof the digits was noted. The patient was admitted tothe hospital for evaluation. Admission laboratory datawere as follows: Hemoglobin 7.6 gr.%, hematocrit 24%,white cell count 2,400/cu mm, platelets 10,000/cu mm,PT 11.5 seconds, PTT 23.0 seconds, SCOT 20, SPOT19, and Alkaline Phosphatase 91. Antinuclear anti-body was negative.
The patient was transfused with packed red cells,whole blood and five units of random donor plateletsshortly after admission. A repeat hemoglobin was 9.1gr.%. A bone aspiration and biopsy were performed.These demonstrated a marked decrease in precursorsof all cell lines. Prominent mast cells and plasma cellswere noted. There were no megaloblastic changes
noted. Subsequent normal 612 and folate levels weredocumented. A sucrose hemolysis test proved nega-tive. In the absence of historical evidence for marrowtoxins and the fact that the physical findings were notconsistent with familial aplastic anemia, the diagnosisof idiopathic aplastic anemia was made. A histo-compatible donor was unavailable for marrow trans-plantation. The patient was discharged from the hospi-tal to her parents five days after admission. Subsequentattempts at treatment with high dose corticosteroidsand antithymocyte globulin were unsuccessful.
At the request of the hematology service, the pa-tient was seen in the dental clinic of Riley Hospital onOctober 18, 1979 for evaluation of gingival hemor-rhage and oral lesions. Her oral temperature was 38.9°C, hematocrit 20%, and a platelet count of 1,000cu mm.Oral and Radiographic Examination
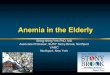
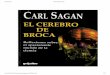
Oral examination demonstrated generalized gingivi-tis with spontaneous gingival hemorrhage (Figure 1).Periodontal examination demonstrated no pocket for-mation greater than three millimeters. Multipleround, raised lesions approximately 3 mm in diameterwere present on the anterior half of the tongue (Figure2). Bilateral lesions approximately 1 cm in diameterwere distal to the second permanent molars on thebuccal mucosa (Figure 3). There was no history of oraltrauma. Radiographic examination, including pano-rex, bite-wing and two maxillary anterior periapicalradiographs were negative for pathology.
The patient reported severe pain during tooth-brushing and had not been practicing regular oralhygiene in the past. At this time the patient was read-mitted to the hospital for dental evaluation and treat-ment of the oral condition.Initial Dental Treatment
The patient received two transfusions of 10 unitseach of platelets. The platelets were matched bymajor blood groups only. This brought her platelet
Figure 2. Multiple round,raised lesions on the anteriorhalf of the tongue (left).
Figure 3. Intraoral view oflesion on patient's left buccalmucosa (right).
268 IDIOPATHIC APLASTIC ANEMIA: Jones, Coates, and Poland

count to 190,000/cu mm. At this time, definitive den-tal treatment was initiated. Oral hygiene instructionswere given to the patient and her parents. The needfor daily oral care was stressed and the patientdemonstrated that she could remove plaque from allsurfaces of her teeth using a toothbrush and dentalfloss. A thorough debridement of the gingiva and aprophylaxis of the teeth were completed. Nitrousoxide-oxygen analgesia was used to reduce the pa-tient's anxiety concerning dental treatment. Thepatient was seen daily in the dental clinic for theremainder of her admission for evaluation and rein-forcement of her oral hygiene. Upon her release fromthe hospital, five days after initial dental treatment,the gingivitis had been reduced, although some spon-taneous gingival hemorrhage continued and the orallesions remained essentially unchanged. This wasthought to be secondary to her thrombocytopenia.
The patient was evaluated in the dental clinic onNovember 26, 1979. She was again admitted to thehospital for severe, prolonged epistaxis and gingivalhemorrhage. Her hematocrit was 30% and her plateletcount was 2,000/cu mm. She received 10 units ofplatelets. The patient complained of moderate intra-oral pain and was given two Tylenol #3b tablets onehour before dental treatment, which consisted of rein-forcing oral hygiene, gingival debridement and pro-phylaxis. Due to her anxiety concerning dental treat-ment, these procedures were accomplished usingnitrous oxide-oxygen analgesia. On the following day,the procedure was repeated without the use of Tylenol# 3. She was discharged later that same day after thegingival hemorrhage had been controlled.
The patient was seen every two weeks in the dentalclinic for observation of oral health and reinforcementof oral hygiene. She consistently demonstratedmeticulous oral home care, although gingival hemor-rhage and oral lesions were still present. This was pri-marily due to her thrombocytopenia. From her initialdiagnosis of idiopathic aplastic anemia in March, 1979to January, 1980, she had received approximately 190units of random donor platelets (approximately 17units per month) during 10 hospital admissions andnumerous out-patient visits for epistaxis and gingivalhemorrhage secondary to her thromobcytopenia.Systemic Use of Aminocaproic Acid
Due to the frequency and severity of epistaxis,chronic gingival hemorrhage and the subsequent needof multiple platelet transfusions, the hematology ser-vice elected to start the patient on oral aminocaproicacid. The initial dosage was 6 gm per day (1.5 gmq.i.d.) The maximal recommended dosage of amino-caproic acid is 30 gm per day. Epistaxis and gingivalhemorrhage ceased within 24 hours. Only 15 units ofplatelets were given over the next three months due tobMcNeil Laboratories, Fort Washington, Pennsylvania 19034.
persistent, severe thrombocytopenia (2,000/cu mm),and periodic epistaxis. The need for platelets had beenreduced to approximately 5 units per month. Gingivalinflammation and oral lesions decreased within twoweeks. The patient did experience a mild candidosisduring a three-day period (Figure 4-6). The patientmaintained meticulous oral hygiene and was followedregularly in the dental clinic for observation and recallexaminations. During the fourth month of amino-caproic acid therapy, the patient experienced signifi-cant episodes of nasopharyngeal hemorrhage requiringhospitalization. This was controlled by adjusting thedosage of aminocaproic acid to 20 gm/day (5.0 gmq.i.d.), nasal packing and platelet transfusions. She isbeing maintained at this dosage.
Figure 4. Intraoral view oi gingival health approximatelytwo weeks after aminocaproic acid therapy was initiated.
DiscussionAminocaproic acid is a monoaminocarboxylic acid
which inhibits fibrinolysis. The beneficial effectsappear to be principally via inhibition of the plas-minogen activator substances and through antiplas-min activity, although the exact mechanism is notknown.1-1617 The drug is absorbed rapidly following oraladministration. In dentistry, aminocaproic acid hasbeen especially useful to control patients with classichemophilia A.1* Some patients experience orthostatichypotension while undergoing animocaproic acid ther-apy,1 although this patient reports no such experience.Aminocaproic acid is also contraindicated in patientswith hematuria.
The use of aminocaproic acid in the management ofamegakaryocytic thrombocytopenia has been espe-cially beneficial by reducing the need for multipletransfusions to control hemorrhagic episodes.1 This isparticularly important since patients with bone mar-row hypoplasia often become refractory to repeatedtransfusions. It has been reported that aminocaproicacid therapy be discontinued when the platelet countconsistently exceeds 20,000/cu mm.1 In this patient,whose platelet count consistently remains 2,000/cumm, the need for platelet transfusion to control epis-taxis and gingival bleeding was reduced from approxi-mately 17 units of platelets per month prior to amino-caproic acid therapy to approximately 5 units ofplatelets per month following aminocaproic therapy.
PEDIATRIC DENTISTRY: Volume 3, Number 3 269

Figure 5. Clinical appearanceof the tongue approximatelytwo weeks after aminocaproicacid therapy was initiated.Note absence of lesions.
Figure 6. Intraoral view ofpatient's left buccal mucosaapproximately two weeksafter aminocaproic acid ther-apy was initiated. Note thehealing of the lesion.
SummaryIn this case presentation, a 15-year-old black
female with idiopathic aplastic anemia was treatedwith a combination of modalities including initialplatelet transfusion, oral hygiene instruction, dentalprophylaxis and systemic aminocaproic acid. Thehealth of the oral tissue greatly improved. Previousstudies have demonstrated the positive results ofmeticulous oral hygiene in these patients.6192° Althoughthis patient consistently demonstrated meticulousoral hygiene, gingival bleeding and oral lesions werestill evident during treatment. This suggests that inpatients with severe thrombocytopenia (2,000/cumm), meticulous oral hygiene can improve the oralenvironment but direct hematologic measures are es-sential for treatment. At this time, the patientremains stable and is continuing a relatively normaladolescence. She reports that her improved oralhealth has enhanced her sense of well-being.
AcknowledgmentsThe authors would like to thank Dr. David R. Avery, Dr. Ken-
neth D. Snawder, and Professor Paul Barton for their suggestionsduring the preparation of this manuscript.
Dr. Jones is in private practice at the Medical Arts Tower, 207Sparks Avenue, Suite 204, Jeffersonville, Indiana, 47130. He is alsoclinical instructor, department of pedodontics, University of Louis-ville, School of Dentistry. Dr. Coates is senior fellow in pediatrichematology-oncology, and Dr. Poland is associate professor of pedo-dontics & oral-facial genetics, Indiana University School of Den-tistry. Requests for reprints should be sent to Dr. Jones.
References1.Gardner, F. H. and Helmer, R. E.: Aminocaproic acid. Use in
control of hemorrhage in patients with amegakaryocyte throm-bocytopenia, JAMA, 243:1, 35-37, January 4,1980.
2. Ehrlich, P.: Uber einen fall von anaime mit bermerkungen uberregentzrative veranderungen des knochenmarys, Charite — Ann,13:300,1888.
3. Geary, C. G.: Blood and neoplastic disease: Acquired aplasticanemia, Brit Med J, 2:432-435, May 25, 1974.
4. Moffitt, M. and Cooley, R. O.: Aplastic anemia: A case report, JDent Child, Sept.-Oct, 379-381, 1970.
5. Wintrobe, M. M.: Clinical Hematology, Ed. 7. Philadelphia: Leeand Febiger, 1974, pp 1749-1769.
6. Stamps, J. T.: The role of oral hygiene in a patient with idio-pathic aplastic anemia, JADA, 88:1025-1027, 1974.
7. Shafer, W. G.; Hine, M. K.; and Levy, B. A.: A Textbook of OralPathology, Ed. 3, Philadelphia: W. B. Saunders Co., 1974, pp669-671.
S.Williams, W. J.: Hematology. New York: McGraw-Hill BookCompany, Inc., 1972, pp 207-227.
9. Davidson, S. (Sir): The Principles and Practice of Medicine, Ed.3. Edinburgh and London: E. and S. Livingston, Ltd., p 648,1956.
10. Custer, R. P.: Aplastic anemia in soldiers treated with atabrine,Am J M Se, 212:211, 1946.
11. Smiley, R. K.; Cartwright, G. E.; and Wintrobe, M. M.: Fatalaplastic anemia following chloratiphenicul (chloromycetin)administration, JAMA, 149: 914, 1952.
12. Scott, J. L.; Cartwright, G. E.; and Wintrobe, M. M.: Acquiredaplastic anemia: An analysis of thirty-nine cases and review ofthe pertinent literature, Medicine, 38:119, 1959.
13. Loge, J. P.: Aplastic anemia following exposure to benzene hex-achloride (lindane), JAMA, 193:110, 1965.
14. Powars, D.: Aplastic anemia secondary to glue sniffing, N Engl JMed, 273:700, 1965.
15. Wintrobe, M. M.; Stowell, A.; and Roll, R. M.: Report of a caseof aplastic anemia following gold injections in which recoveryoccurred, Am J M Se, 197:698, 1939.
16. Gaum, L. I.: Use of aminocaproic acid in oral surgery forhaemophiliacs: Report of case, J Can Dent Assoc, 35:599-602,November, 1969.
17. Nilsson, I. M.; Andersson, L.; and Bjoryman, S. E.: Epsilonaminocaproic acid (EACA) as a therapeutic agent: Based on fiveyears' clinical experience, Acta Med Scand, suppl. 448, 17, 1966.
18. Corrigan, Jr., J. J.: Oral bleeding in hemophilia: Treatment withepsilon aminocaproic and replacement therapy, J Pediatr,80:124-128, January, 1972.
19. Lasser, S. D.; Camitta, B. M.; and Needleman, H. L.: Dentalmanagement of patients undergoing bone marrow transplanta-tion for aplastic anemia, Oral Surg, 43, 2:181-189, 1977.
20. Mcllwain, J. E.: Dental support of severe metabolic disease:Aplastic anemia, J Dent Child, 43:54-55, July-August, 1976.
270 IDIOPATHIC APLASTIC ANEMIA: Jones, Coates, and Poland