Embed Size (px)
Citation preview
Anaemia in the ICU: Is there an alternative to using blood
transfusion?
Tim Walsh
Professor of Critical Care, Edinburgh University
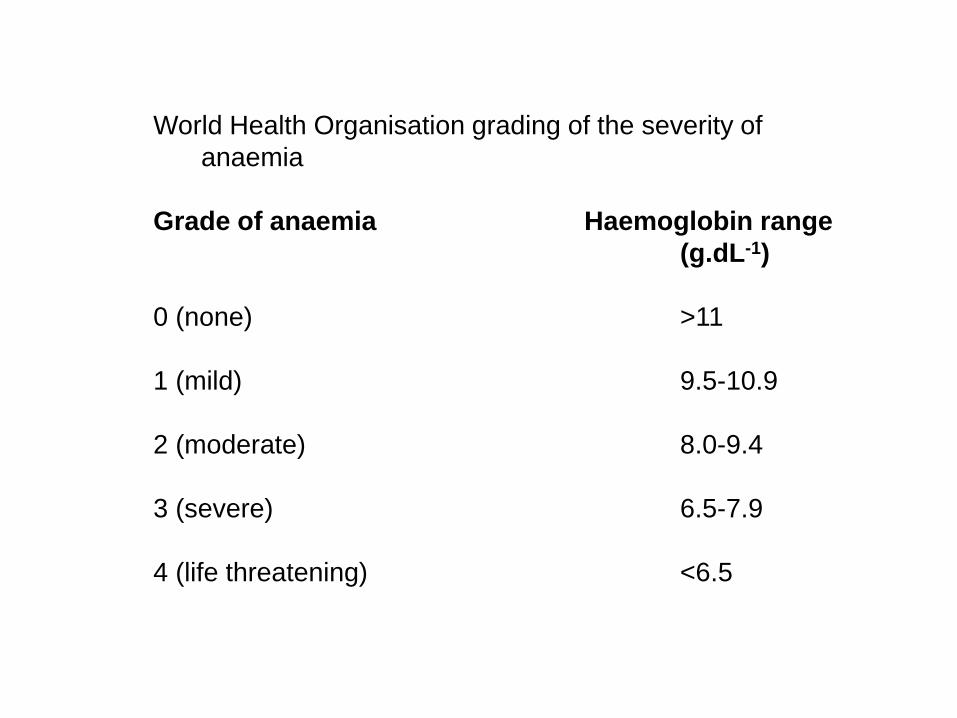
World Health Organisation grading of the severity of
anaemia
Grade of anaemia Haemoglobin range
(g.dL-1)
0 (none) >11
1 (mild) 9.5-10.9
2 (moderate) 8.0-9.4
3 (severe) 6.5-7.9
4 (life threatening) <6.5
“No question!”
“Not sure”
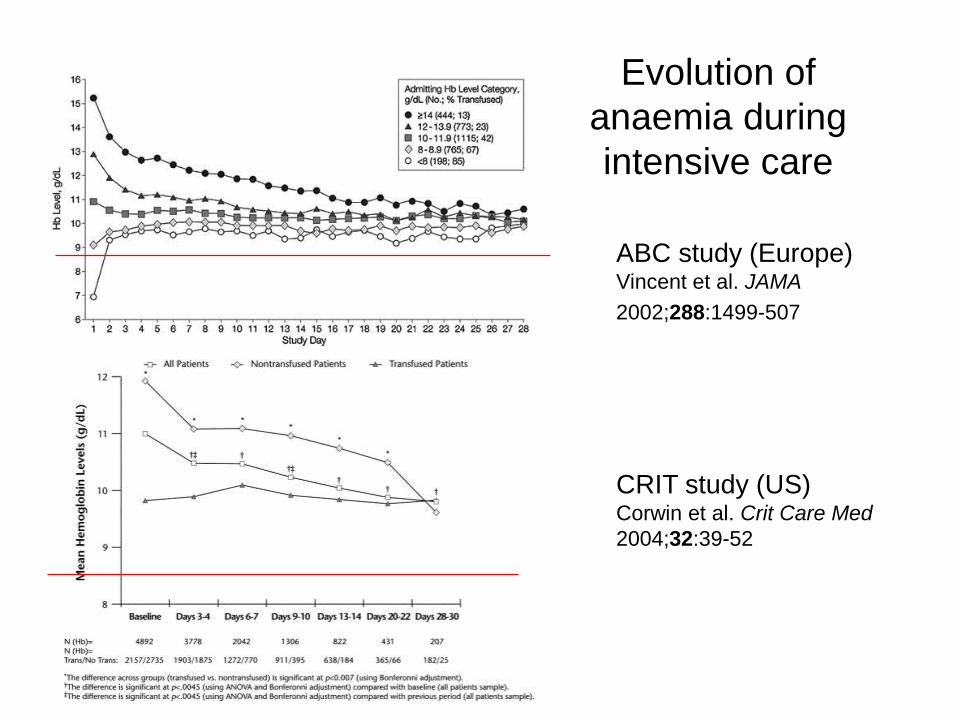
Evolution of
anaemia during
intensive care
ABC study (Europe) Vincent et al. JAMA
2002;288:1499-507
CRIT study (US) Corwin et al. Crit Care Med
2004;32:39-52
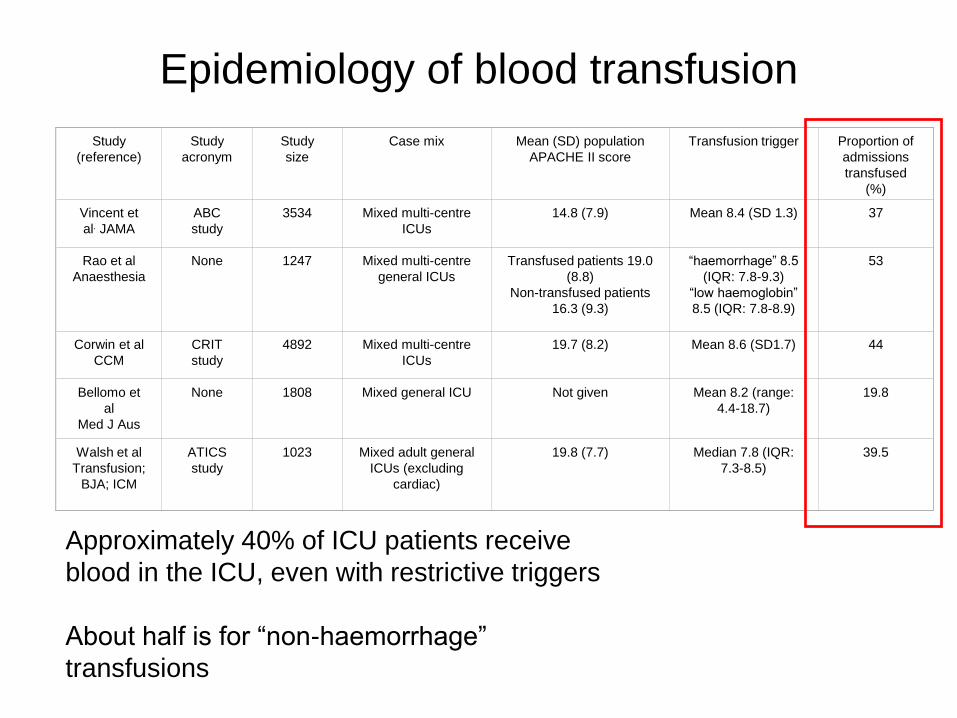
Epidemiology of blood transfusion
Study
(reference)
Study
acronym
Study
size
Case mix
Mean (SD) population
APACHE II score
Transfusion trigger
Proportion of
admissions
transfused
(%)
Vincent et
al. JAMA
ABC
study
3534
Mixed multi-centre
ICUs
14.8 (7.9)
Mean 8.4 (SD 1.3)
37
Rao et al
Anaesthesia
None
1247
Mixed multi-centre
general ICUs
Transfused patients 19.0
(8.8)
Non-transfused patients
16.3 (9.3)
“haemorrhage” 8.5
(IQR: 7.8-9.3)
“low haemoglobin”
8.5 (IQR: 7.8-8.9)
53
Corwin et al
CCM
CRIT
study
4892
Mixed multi-centre
ICUs
19.7 (8.2)
Mean 8.6 (SD1.7)
44
Bellomo et
al
Med J Aus
None
1808
Mixed general ICU
Not given
Mean 8.2 (range:
4.4-18.7)
19.8
Walsh et al
Transfusion;
BJA; ICM
ATICS
study
1023
Mixed adult general
ICUs (excluding
cardiac)
19.8 (7.7)
Median 7.8 (IQR:
7.3-8.5)
39.5
Approximately 40% of ICU patients receive
blood in the ICU, even with restrictive triggers
About half is for “non-haemorrhage”
transfusions
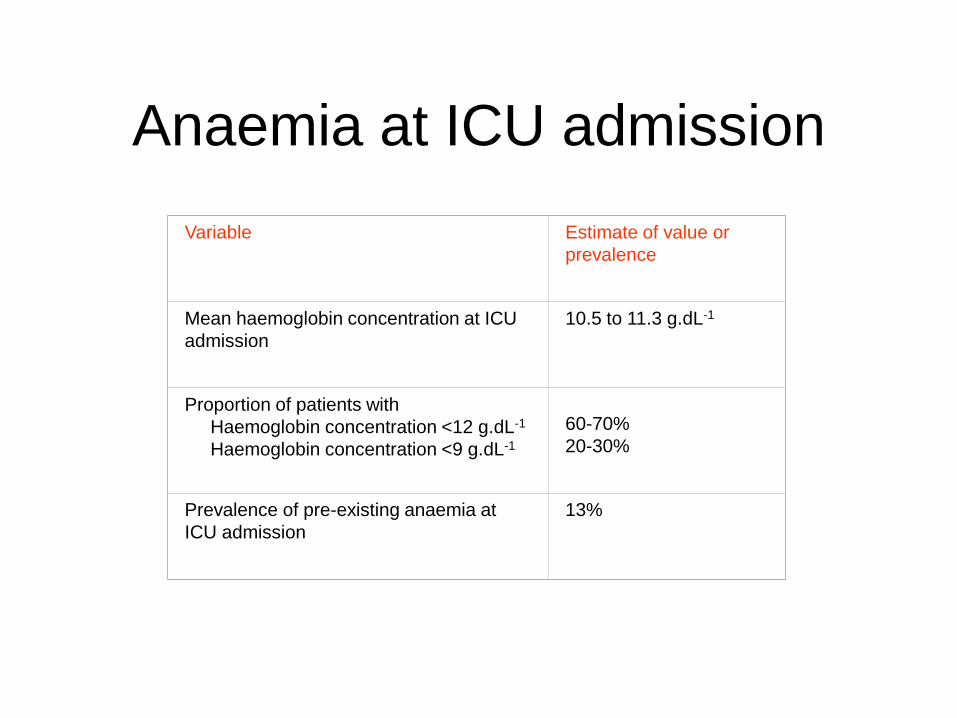
Anaemia at ICU admission
Variable
Estimate of value or
prevalence
Mean haemoglobin concentration at ICU
admission
10.5 to 11.3 g.dL-1
Proportion of patients with
Haemoglobin concentration <12 g.dL-1
Haemoglobin concentration <9 g.dL-1
60-70%
20-30%
Prevalence of pre-existing anaemia at
ICU admission
13%
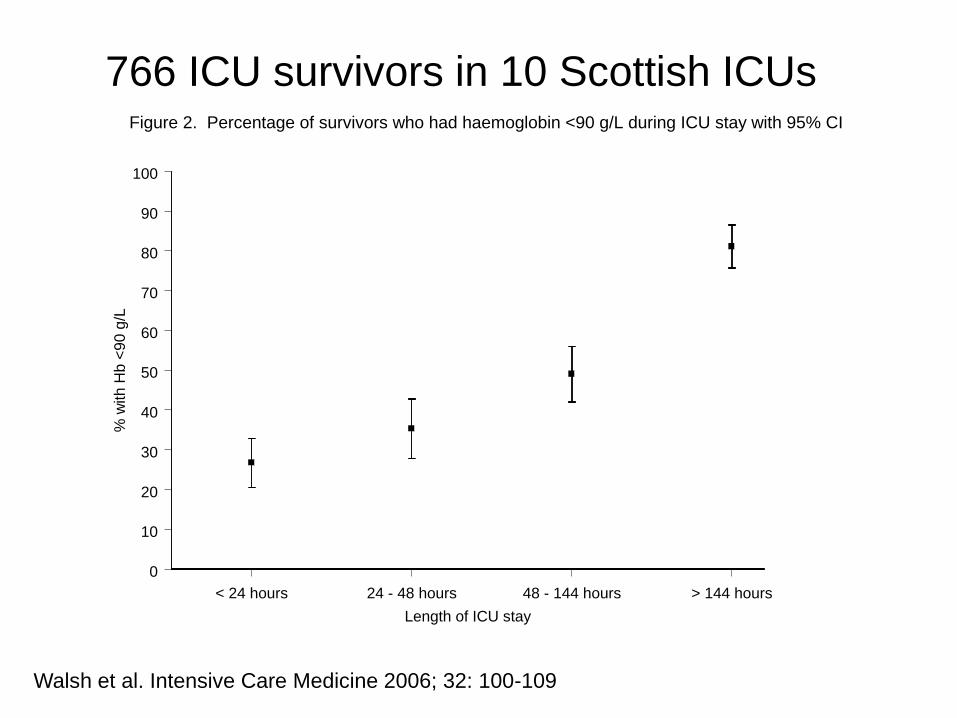
< 24 hours 24 - 48 hours 48 - 144 hours > 144 hours
Length of ICU stay
0
10
20
30
40
50
60
70
80
90
100
% w
ith H
b <
90 g
/LFigure 2. Percentage of survivors who had haemoglobin <90 g/L during ICU stay with 95% CI
766 ICU survivors in 10 Scottish ICUs
Walsh et al. Intensive Care Medicine 2006; 32: 100-109
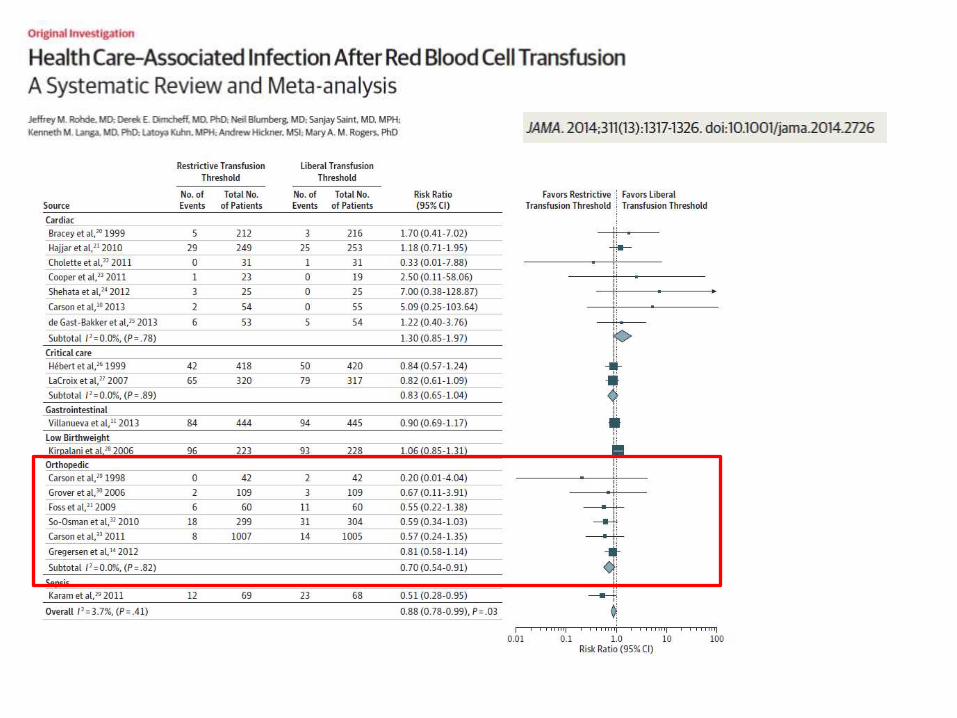
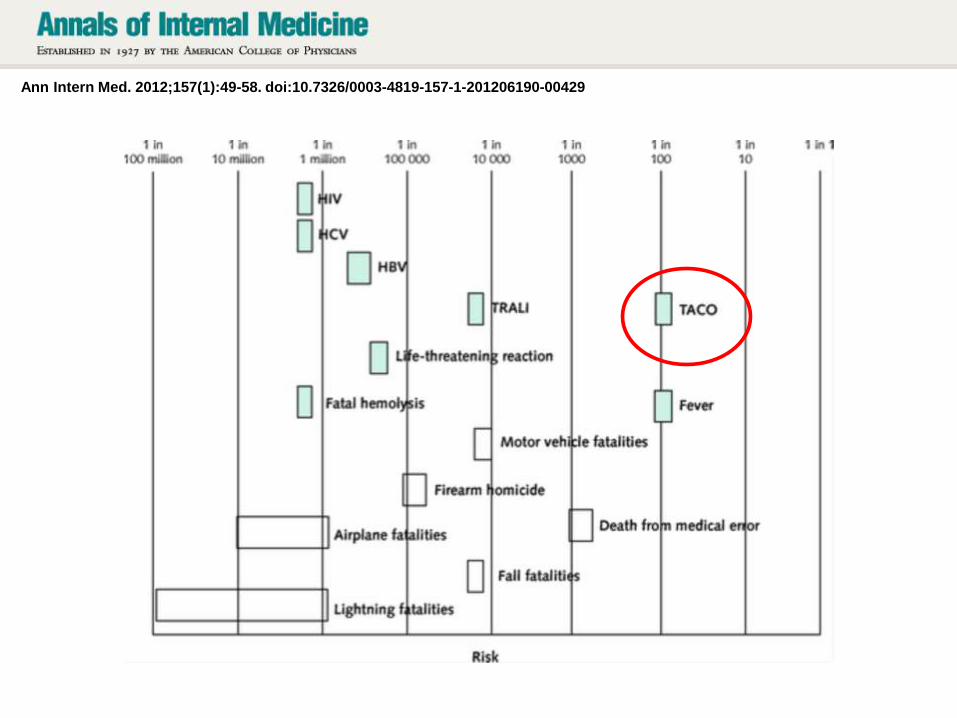
Ann Intern Med. 2012;157(1):49-58. doi:10.7326/0003-4819-157-1-201206190-00429
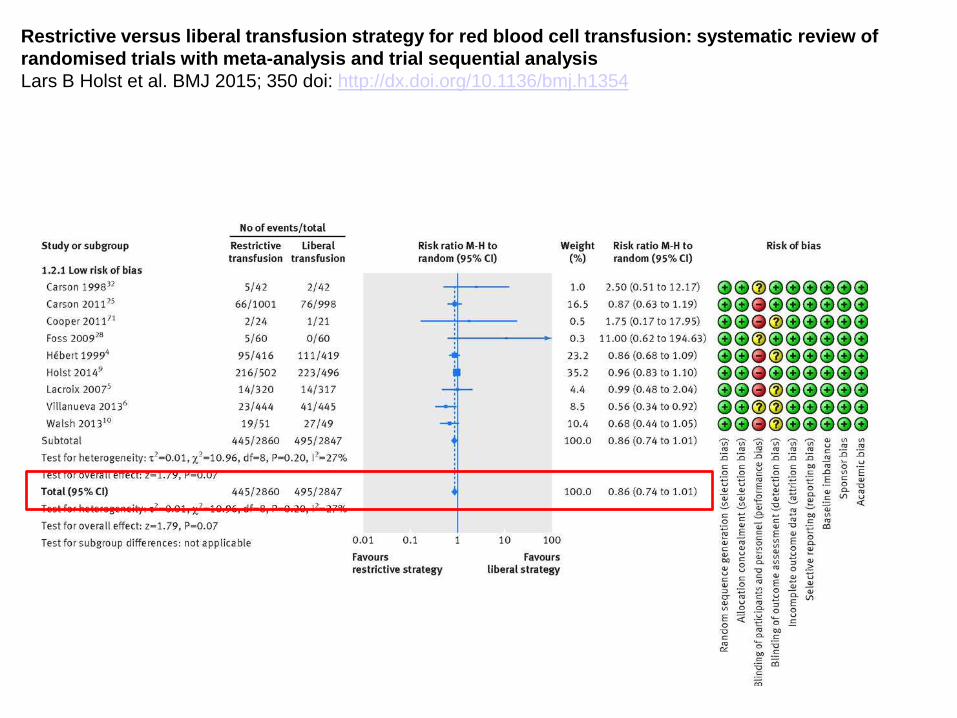
Restrictive versus liberal transfusion strategy for red blood cell transfusion: systematic review of
randomised trials with meta-analysis and trial sequential analysis
Lars B Holst et al. BMJ 2015; 350 doi: http://dx.doi.org/10.1136/bmj.h1354
Lecture plan
• Review the aetiology of anaemia during
critical illness
• Consider the evidence for 3 non-
transfusion interventions – Minimisation of blood loss
– Iron therapy
– Erythropoietin therapy (with iron)

Lecture plan
• Review the aetiology of anaemia during
critical illness
• Consider the evidence for 3 non-
transfusion interventions – Minimisation of blood loss
– Iron therapy
– Erythropoietin therapy (with iron)
Causes of anaemia during critical
illness
Pre-existing anaemia
Acquired anaemia Haemodilution
Blood loss
Blood sampling
Haemorrhage
Reduced red cell survival
Reduced red cell production
Abnormal iron metabolism
Nutritional deficiencies
Inappropriate erythropoietin production
Abnormal red cell production
Causes of anaemia during critical
illness
Pre-existing anaemia
Acquired anaemia Haemodilution
Blood loss
Blood sampling
Haemorrhage
Reduced red cell survival
Reduced red cell production
Abnormal iron metabolism
Nutritional deficiencies
Inappropriate erythropoietin production
Abnormal red cell production
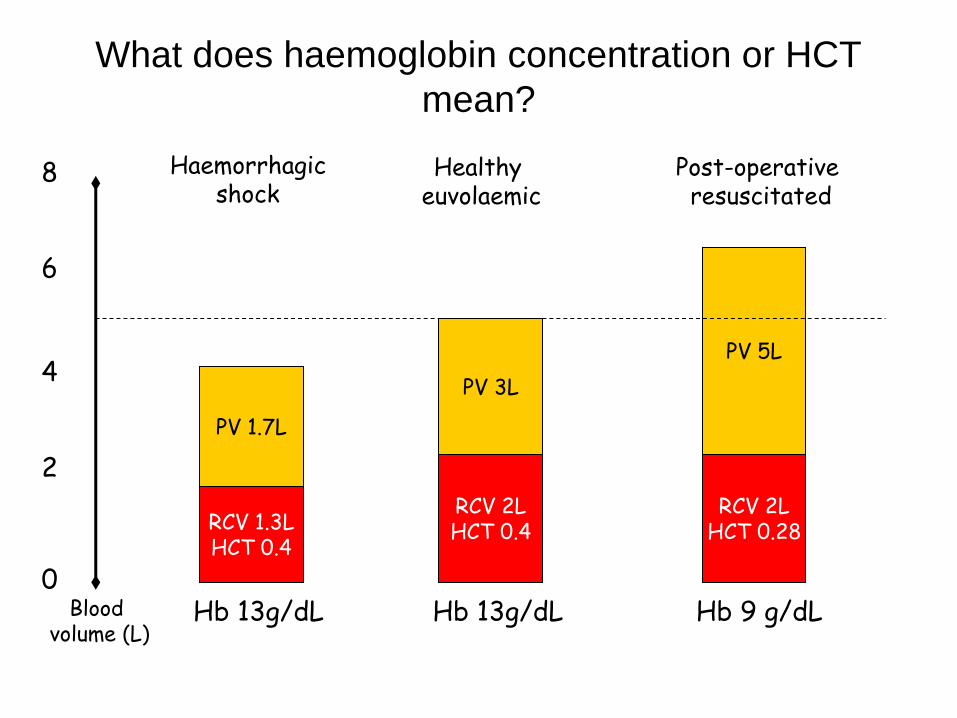
What does haemoglobin concentration or HCT
mean?
RCV 2L HCT 0.4
PV 3L
RCV 1.3L HCT 0.4
PV 1.7L
PV 5L
RCV 2L HCT 0.28
Haemorrhagic shock
2
4
6
0
8
Blood volume (L)
Healthy euvolaemic
Post-operative resuscitated
Hb 13g/dL Hb 13g/dL Hb 9 g/dL
Causes of anaemia during critical
illness
Pre-existing anaemia
Acquired anaemia Haemodilution
Blood loss
Blood sampling
Haemorrhage
Reduced red cell survival
Reduced red cell production
Abnormal iron metabolism
Nutritional deficiencies
Inappropriate erythropoietin production
Abnormal red cell production
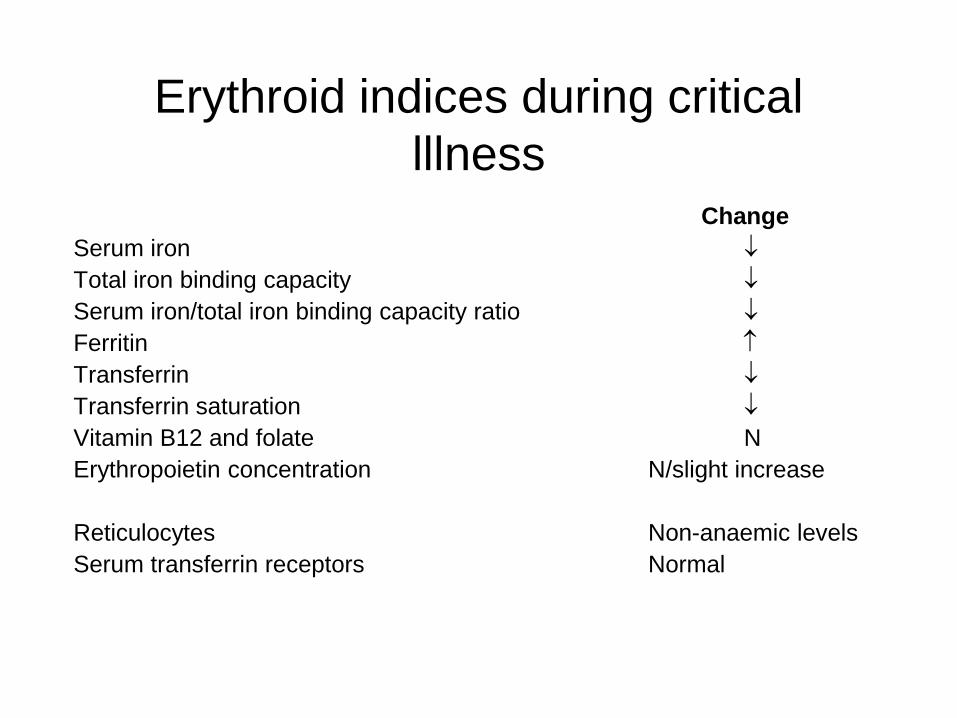
Erythroid indices during critical
lllness Change Serum iron
Total iron binding capacity
Serum iron/total iron binding capacity ratio
Ferritin
Transferrin
Transferrin saturation
Vitamin B12 and folate N
Erythropoietin concentration N/slight increase
Reticulocytes Non-anaemic levels
Serum transferrin receptors Normal
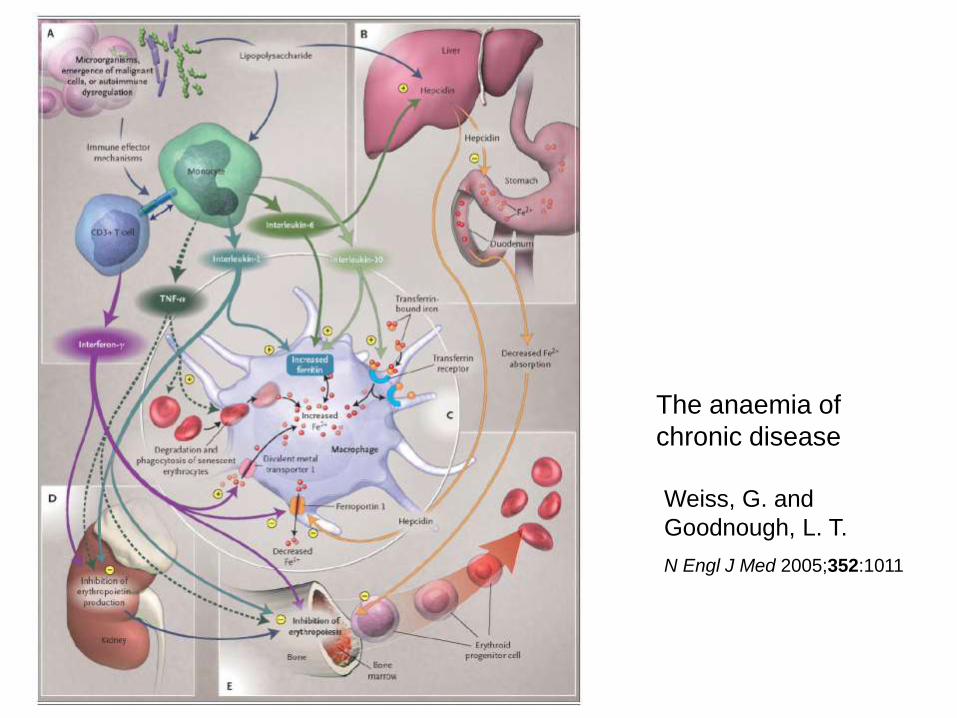
Weiss, G. and
Goodnough, L. T.
N Engl J Med 2005;352:1011
The anaemia of
chronic disease
Weiss, G. and
Goodnough, L. T.
N Engl J Med 2005;352:1011
The anaemia of
chronic disease
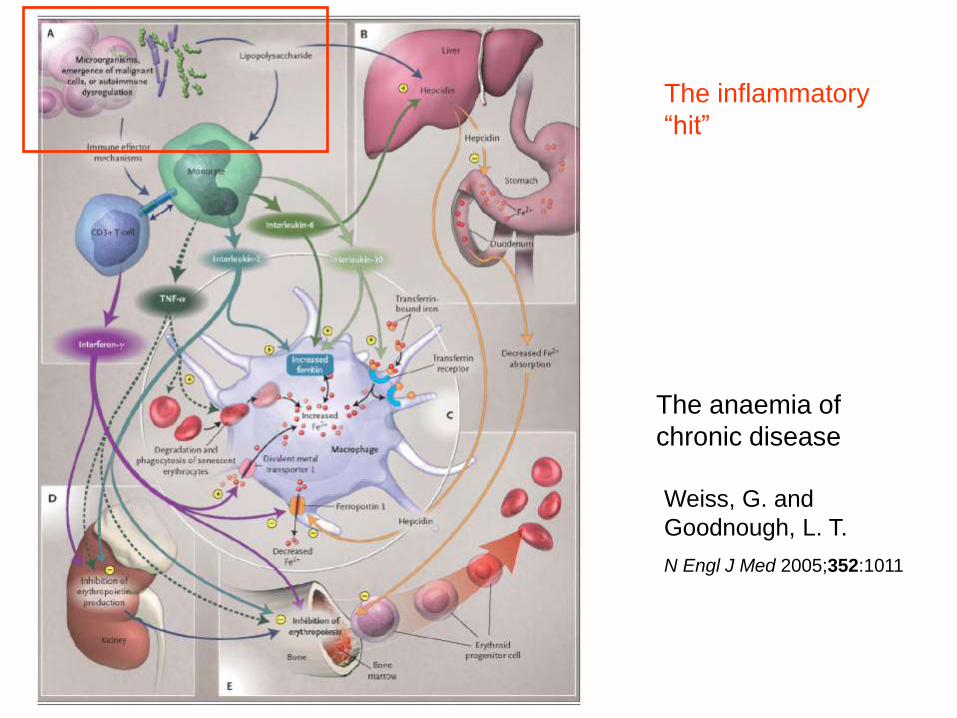
The inflammatory
“hit”
Effects of inflammation
• Inhibition of renal erythropoietin
production
– Blunted “inappropriate” response to
anaemia
• Direct effects on erythropoiesis in bone
marrow
• Effects on acute phase proteins
Weiss, G. and
Goodnough, L. T.
N Engl J Med 2005;352:1011
The anaemia of
chronic disease
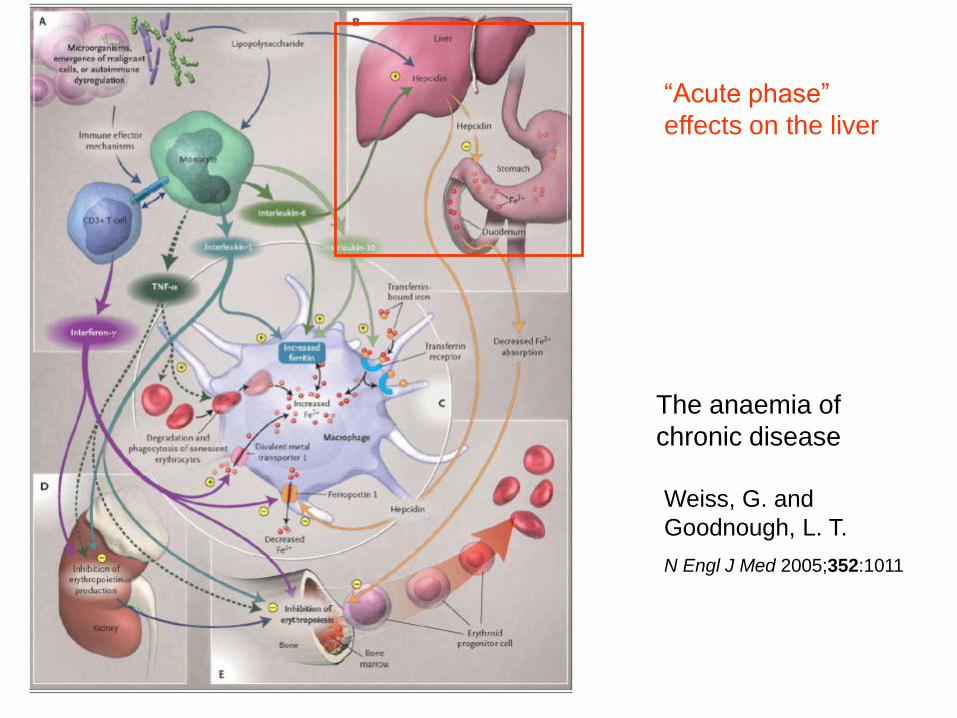
“Acute phase”
effects on the liver
Acute phase effects on the liver
• Up-regulation of ferritin production
– Increased storage iron
• Down-regulation of transferrin production
– Decreased iron availability for erythropoiesis
• Up-regulation of hepcidin production
– Decreased duodenal iron absorption
Weiss, G. and
Goodnough, L. T.
N Engl J Med 2005;352:1011
The anaemia of
chronic disease
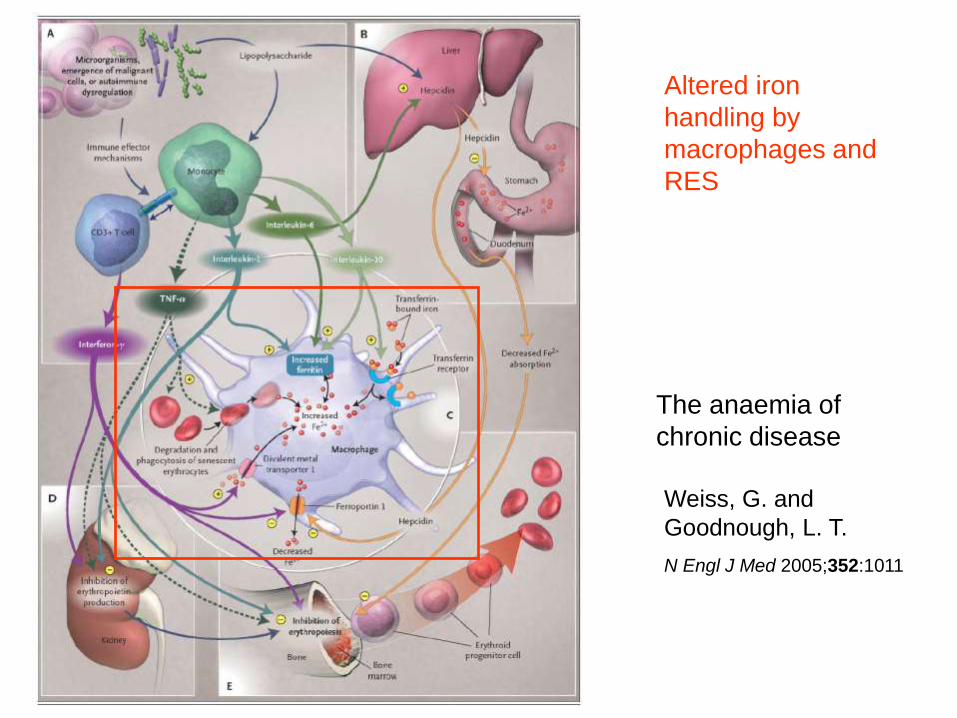
Altered iron
handling by
macrophages and
RES
Effects on macrophage and RES
• Increased iron uptake – Increased ferritin
– Opening of divalent metal transported protein
– Closure of ferroportin 1
– Hepcidin mediated
• Increased phagocytosis of senescent red cells by activated macrophages
• Increased uptake of transferrin bound iron
• Functional iron deficiency
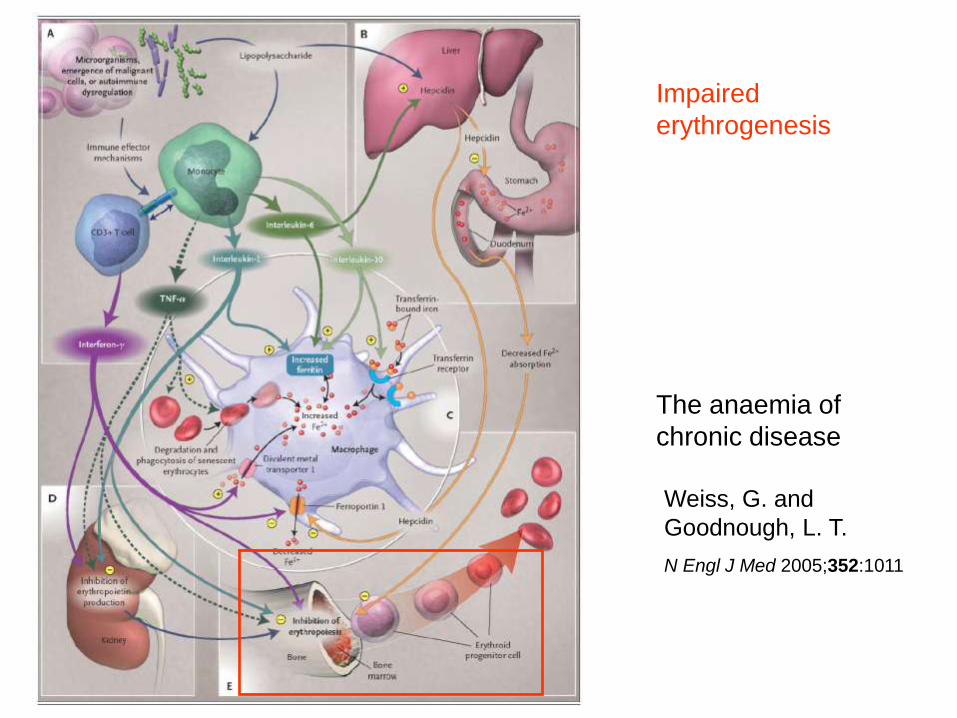
Weiss, G. and
Goodnough, L. T.
N Engl J Med 2005;352:1011
The anaemia of
chronic disease
Impaired
erythrogenesis
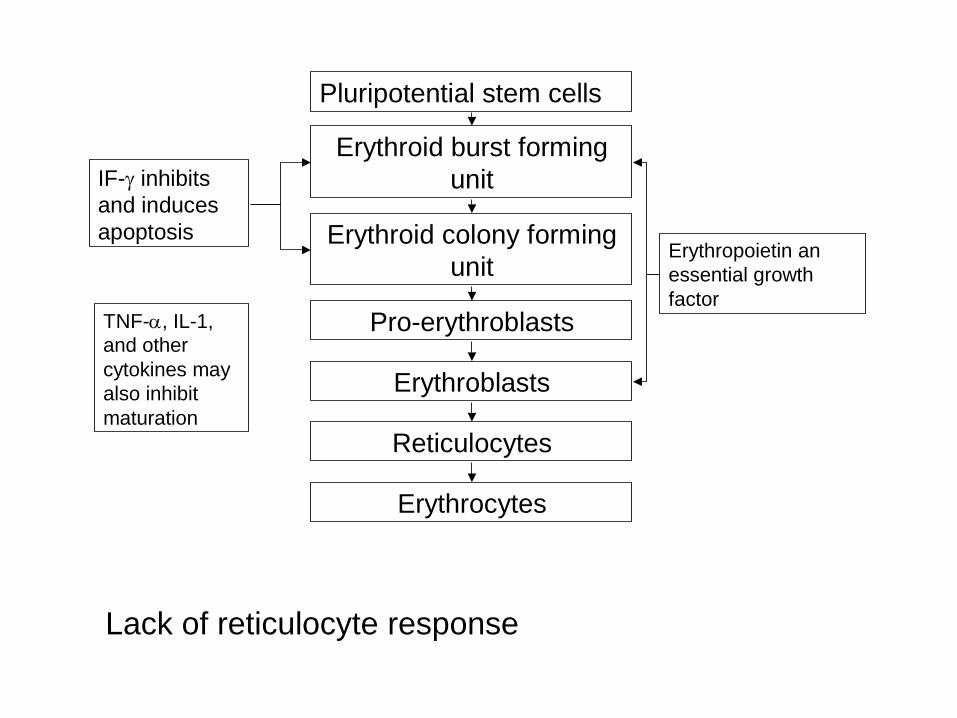
Pluripotential stem cells
Erythroid burst forming
unit
Pro-erythroblasts
Erythroblasts
Reticulocytes
Erythrocytes
Erythropoietin an
essential growth
factor
Erythroid colony forming
unit
IF- inhibits
and induces
apoptosis
TNF-, IL-1,
and other
cytokines may
also inhibit
maturation
Lack of reticulocyte response
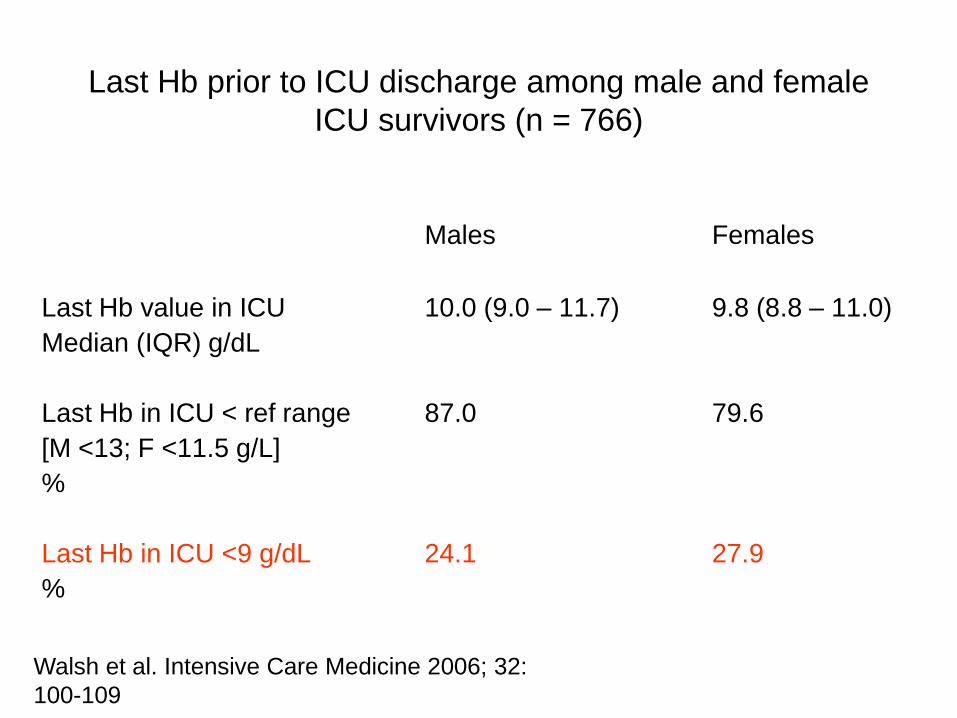
Last Hb prior to ICU discharge among male and female
ICU survivors (n = 766)
Males Females
Last Hb value in ICU 10.0 (9.0 – 11.7) 9.8 (8.8 – 11.0)
Median (IQR) g/dL
Last Hb in ICU < ref range 87.0 79.6
[M <13; F <11.5 g/L]
%
Last Hb in ICU <9 g/dL 24.1 27.9
%
Walsh et al. Intensive Care Medicine 2006; 32:
100-109
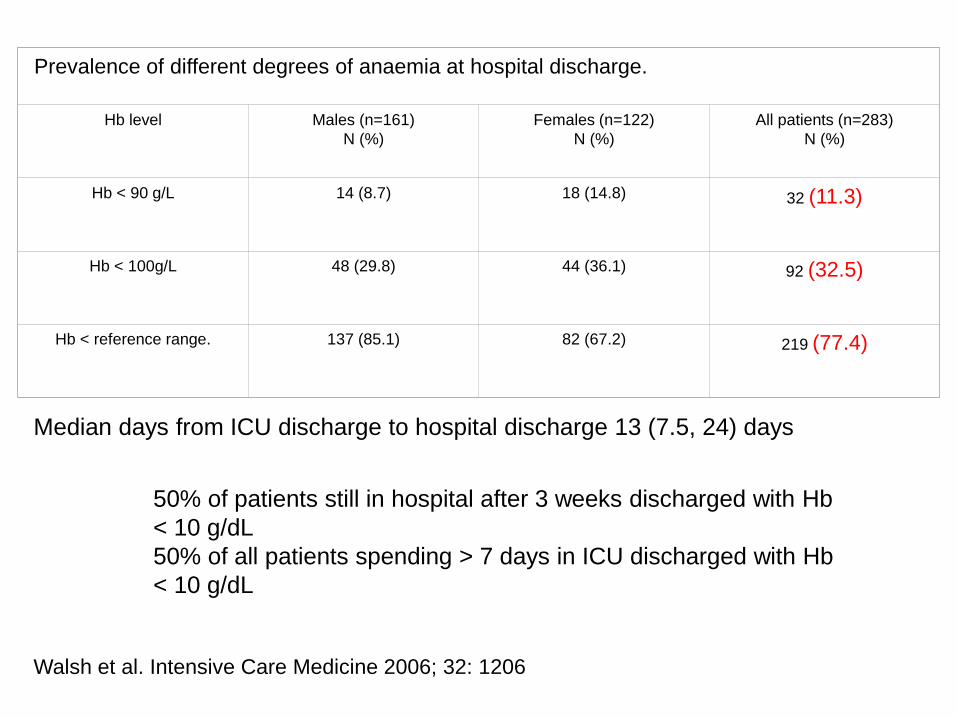
Prevalence of different degrees of anaemia at hospital discharge.
Hb level
Males (n=161)
N (%)
Females (n=122)
N (%)
All patients (n=283)
N (%)
Hb < 90 g/L
14 (8.7)
18 (14.8)
32 (11.3)
Hb < 100g/L
48 (29.8)
44 (36.1)
92 (32.5)
Hb < reference range.
137 (85.1)
82 (67.2)
219 (77.4)
Median days from ICU discharge to hospital discharge 13 (7.5, 24) days
50% of patients still in hospital after 3 weeks discharged with Hb
< 10 g/dL
50% of all patients spending > 7 days in ICU discharged with Hb
< 10 g/dL
Walsh et al. Intensive Care Medicine 2006; 32: 1206
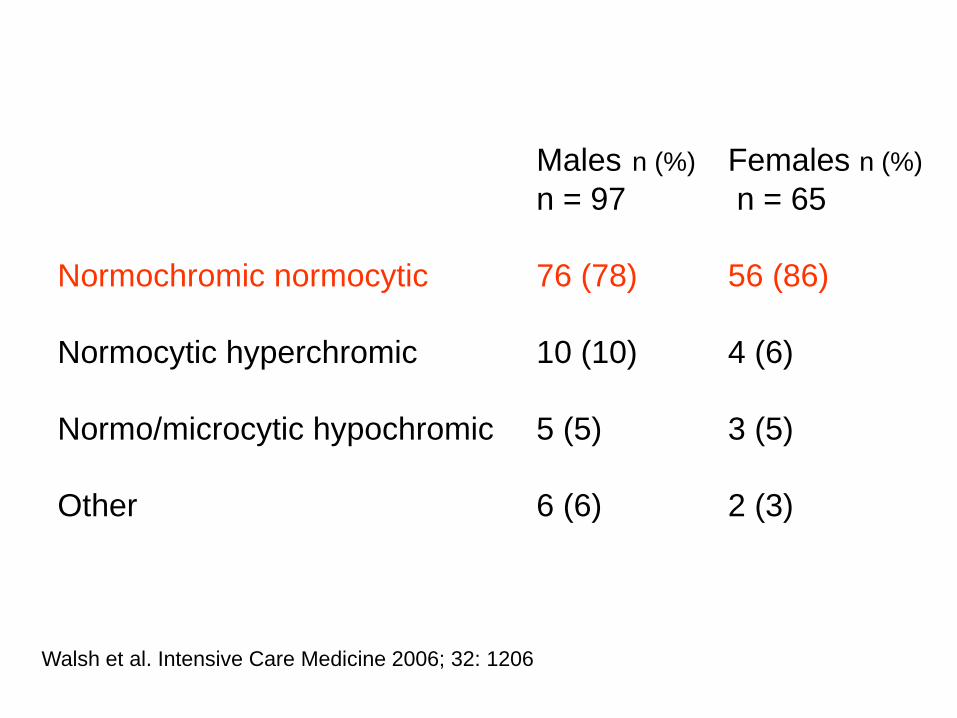
Characteristics of anaemia at hospital discharge
Males n (%) Females n (%)
n = 97 n = 65
Normochromic normocytic 76 (78) 56 (86)
Normocytic hyperchromic 10 (10) 4 (6)
Normo/microcytic hypochromic 5 (5) 3 (5)
Other 6 (6) 2 (3)
Walsh et al. Intensive Care Medicine 2006; 32: 1206
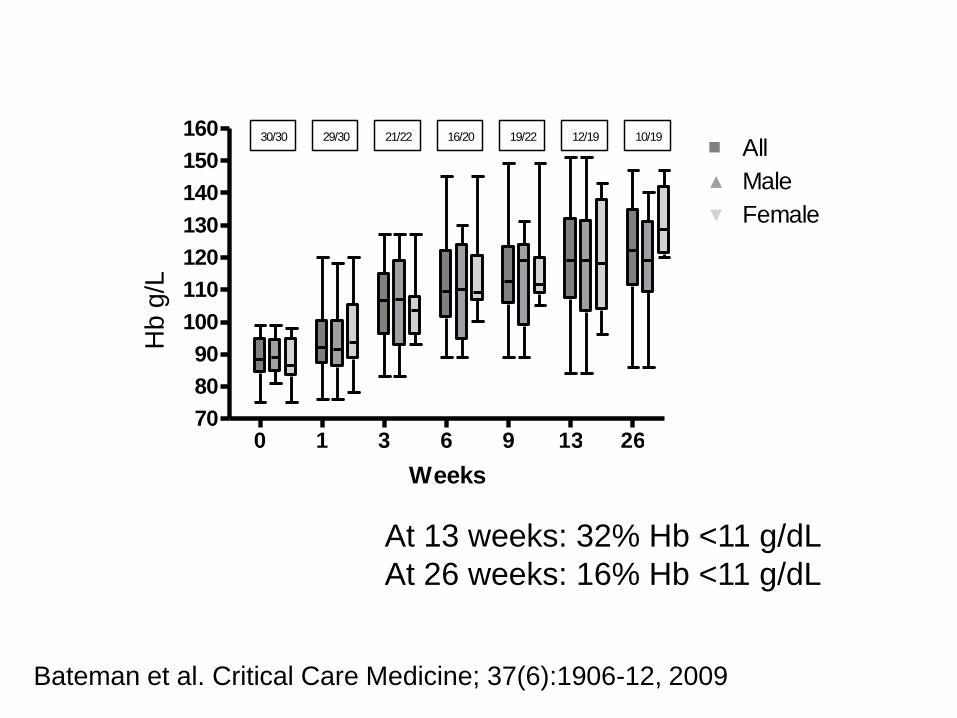
0 1 3 6 9 13 2670
80
90
100
110
120
130
140
150
160All
Male
Female
30/30 29/30 21/22 16/20 12/19 10/1919/22
Weeks
Hb
g/L
Hb
g/L
Bateman et al. Critical Care Medicine; 37(6):1906-12, 2009
At 13 weeks: 32% Hb <11 g/dL
At 26 weeks: 16% Hb <11 g/dL
Factors associated with slow or failure to
recover
• Higher circulating inflammatory markers following
discharge (IL-6 and CRP)
• Lack of reticulocyte response
• Erythropoietin concentrations inappropriately low in
all patients
• No evidence of nutritional deficiency
• “Inflammatory” anaemia
Summary • With restrictive transfusion anaemia is highly
prevalent in the ICU
• Anaemia is multifactorial, but inflammation is an important mechanism
• About 25% of patients are discharged with Hb <90 g/L
• Recovery is slow; anaemia is frequently moderate at hospital discharge
• In many patients anaemia persists for months
• The importance of anaemia to recovery after critical illness is unknown
Lecture plan
• Review the aetiology of anaemia during
critical illness
• Consider the evidence for 3 non-
transfusion interventions – Minimisation of blood loss
– Iron therapy
– Erythropoietin therapy (with iron)
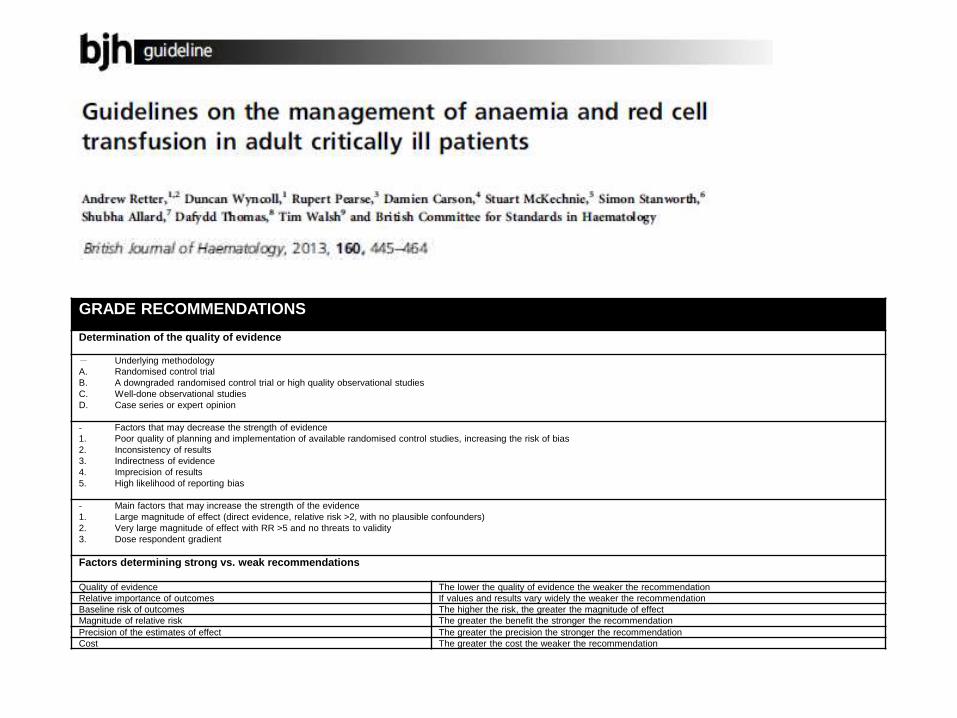
GRADE RECOMMENDATIONS 1: Summary of the Grade Recommendations
Determination of the quality of evidence
- Underlying methodology
A. Randomised control trial
B. A downgraded randomised control trial or high quality observational studies
C. Well-done observational studies
D. Case series or expert opinion
- Factors that may decrease the strength of evidence
1. Poor quality of planning and implementation of available randomised control studies, increasing the risk of bias
2. Inconsistency of results
3. Indirectness of evidence
4. Imprecision of results
5. High likelihood of reporting bias
- Main factors that may increase the strength of the evidence
1. Large magnitude of effect (direct evidence, relative risk >2, with no plausible confounders)
2. Very large magnitude of effect with RR >5 and no threats to validity
3. Dose respondent gradient
Factors determining strong vs. weak recommendations
Quality of evidence The lower the quality of evidence the weaker the recommendation
Relative importance of outcomes If values and results vary widely the weaker the recommendation
Baseline risk of outcomes The higher the risk, the greater the magnitude of effect
Magnitude of relative risk The greater the benefit the stronger the recommendation
Precision of the estimates of effect The greater the precision the stronger the recommendation
Cost The greater the cost the weaker the recommendation
Lecture plan
• Review the aetiology of anaemia during
critical illness
• Consider the evidence for 3 non-
transfusion interventions – Minimisation of blood loss
– Iron therapy
– Erythropoietin therapy (with iron)
Minimisation of blood loss
• Reducing phlebotomy frequency
• Reducing phlebotomy volumes
• “Reinfusion” devices for blood discards
• Low quality evidence
• Likely to decrease transfusion requirement and other
costs
• Specific re-infusion devices available
• Needs system level change
Lecture plan
• Review the aetiology of anaemia during
critical illness
• Consider the evidence for 3 non-
transfusion interventions – Minimisation of blood loss
– Iron therapy
– Erythropoietin therapy (with iron)
Iron therapy • Most critically ill patients have a functional iron deficiency
• Oral iron unlikely to be absorbed and has risk of GI
complications
Few studies during critical illness
– Iron therapy does not increase reticulocyte counts
– No high quality studies showing benefit for important clinical outcomes,
including blood transfusion
Intravenous iron
– No high quality trials showing benefit during general critical illness
– No benefit in trauma critical care Crit Care Med 2014; 42:2048–2057
– Concern in sepsis from risk of infection
– Association between IV iron and increased infection in non-critical care
settings Systematic review BMJ 2013;347:f4822 doi: 10.1136/bmj.f4822
Lecture plan
• Review the aetiology of anaemia during
critical illness
• Consider the evidence for 3 non-
transfusion interventions – Minimisation of blood loss
– Iron therapy
– Erythropoietin therapy (with iron)
Erythropoietin therapy
Corwin, H. L., et al (2002) “Efficacy of recombinant human erythropoietin in critically ill
patients: a randomized controlled trial (EPO Critical Care Trials)” JAMA, 288:2827-2835
MC DB RCT; n = 1302
weekly recombinant EPO (40,000IU) vs placebo
• 20% reduction in RBC transfusion in the treatment group
• Mean Hb transfusion trigger 90g/L
Corwin, H. L, et al (2007) “Efficacy and Safety of Epoetin Alfa in Critically Ill Patients”
NEJM, 357:10 pages 965-76
MC DB RCT; n = 1460
medical, surgical and trauma patients (high proportion trauma patients)
EPO vs placebo for 3 weeks
• no change in RBC transfusion
• mean haemoglobin transfusion trigger 80g/L
• higher Hb
• trend towards mortality advantage (more pronounced in trauma patients)
• significant increase in thrombotic events (especially among patients not receiving
thromboprophylaxis)
Interpreting the erythropoietin literature
• Trial populations of interest; low risk of transfusion
• Balance of early therapy versus enrolment of patients with low
transfusion requirements
• Transfusion practice; most did not use restrictive haemoglobin
triggers close to 70g/L
• Uncertain benefit for long term patients at risk of chronic
anaemia
• Variable dose and use of iron therapy
• Uncertain safety profile (especially thrombotic events)
• Uncertain cost-effectiveness
Summary
• Anaemia during critical illness is multifactorial
• Inflammation is a major mechanism resulting
in functional iron deficiency and marrow
suppression
• Minimising blood loss through sampling is
simple and effective
• Based on current evidence routine use of oral
or intravenous iron is not indicated
• Erythropoietin has unproven clinical-
effectiveness and safety and is not indicated