Embed Size (px)
Citation preview

Integrative Nursing Intervention to Reduce Patients’ Pain
Barriers to Nurse- Facilitated Patient Mobility in the ICU
Mobilization Therapy in the PICU
Early Blood Transfusions in Sepsis
Critical Care Nurses’ Experiences With Spiritual Care
Survival of Patients With Severe ARDS Treated Without ECMO
Fluid Response to Passive Leg Raising
Early Warning Score Communication Bundle
Effect of Dynamic Light on Nurses
May 2018 • Volume 27, Number 3
American Journal ofCritical Care

LEADER IN NASAL DECOLONIZATION™
LEADER IN NASAL DECOLONIZATION™
Nozin.com 877-669-4648
Ask a Nozin advisor for a savings analysis and professional samples.
• Safely Reduce MRSA Contact Precautions
• 30 Bed ICU Could Save $600,000 Per Year*
• Improve Patient Care and Satisfaction
1. Huang SS et al. Targeted versus universal. N Engl J Med, 2013: 368(24): 2255-65. Mupirocin and CHG used in study. 2. Huang SS et al. Cost Savings of Universal Decolonization
to Prevent Intensive Care Unit Infection. ICHE, 2014: 35 (S3): S23-S31. 3. Steed L, et al. Reduction of nasal Staphylococcus aureus carriage. AJIC, 2014: 42(8): 841-846. ©2018 Global
Life Technologies Corp. All rights reserved. Made in USA. Nozin®, Nasal Sanitizer®, Leader in Nasal Decolonization™ are trademarks of Global Life Technologies Corp. Nozin® Nasal
Sanitizer® antiseptic is an OTC topical drug. No claim is made that it has an effect on any specific disease. * Savings estimates are for example only. Any actual savings may vary.
Nasal Decolonization is The Key to Reduce CP
Contact isolation precautions (CP) can adversely affect patient care, utilization of staff and costs. Research shows that universal skin and nasal decolonization can help.1, 2
Nozin ICU programs use universal patient decolonization to safely reduce screening and CP for MRSA colonization.
With the Nozin program, healthcare facilities are able to lessen CP burdens on patients, address staff isolation fatigue, and support antibiotic stewardship.
Nozin® Nasal Sanitizer® antiseptic is clinically proven to decolonize nasal S. aureus day one without antibiotics.3 Learn how a Nozin program can be the key to safely reducing CP in critical care at your facility.
NTI 2018 - Visit Nozin Booth 2973 - Earn ExpoEd CERPs

www.ajcconline.org
Evidence-based interdisciplinary knowledge for high acuity and critical care
AMERICAN ASSOCIATION OF CRITICAL-CARE NURSESPresident, CHRISTINE SCHULMAN, RN, MS, CNS, CCRN-K; President-elect, LISA RIGGS, RN, MSN, APRN-BC, CCRN-K; Secre-tary, MICHELLE KIDD, RN, MS, ACNS-BC, CCRN-K; Trea surer, LOUISE SALADINO, RN, DNP, MHA, CCRN-K; Directors, ELIZABETH BRIDGES, RN, PhD, CCNS; KIMBERLY CURTIN, RN, DNP, APRN, ACNS-BC, CCRN, CEN, CNL; JUSTIN DiLIBERO, RN,
DNP, CCRN, CCNS, ACCNS-AG; NIKKI DOTSON-LORELLO, RN, BSN,
CCRN, CPTC; WENDI FROEDGE, RN-BC, MSN, CCRN-K; DEBORAH JONES, RN, MS, PhD; MARY BETH FLYNN MAKIC, RN, PhD, CNS,
CCNS, CCRN-K; ROSEMARY TIMMERMAN, RN, DNP, CCNS,
CCRN-CSC-CMC; BETH WATHEN, RN, MSN, APRN, CCRN; Chief Executive Officer, DANA WOODS, MBA
EDITORIAL OFFICEAmerican Association of Critical-Care Nurses, 101 Columbia, Aliso Viejo, CA 92656. (800) 899-1712, (949) 362-2000. E-mail address: [email protected]. Web address: www.ajcconline.org Publishing Manager, MICHAEL MUSCAT; Managing Editor, KATIE L. SPILLER, MS; Art and Production Director, LeROY HINTON; Copy Editors, JANE CALAYAG, BA; BARBARA HALLIBURTON, PhD; JULIE HENDERSON, RN, MS, ELS; LAURIE ANNE WALDEN, DVM,
ELS; Graph ics Specialist, MATT EDENS; Peer-Review Coor-dinator, DENISE GOTTWALD; Publishing Assistant, SAM MARSELLA
ADVERTISING SALES OFFICESLACK Incorporated, 6900 Grove Rd, Thorofare, NJ 08086. (800) 257-8290, (856) 848-1000. National Account Manager, NICOLE RUTTER; Recruit ment Sales Representative BERNADETTE HAMILTON; Admin-is trator, JOANN CAMPISI
AMERICAN JOURNAL OF CRITICAL CARE® Telephone: (949) 362-2000. Fax: (949) 362-2049. Copyright 2018 by AACN. All rights reserved. The AMERICAN JOURNAL OF CRITICAL CARE is an official peer-reviewed publication of AACN. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mech an ical, including photo copying, recording or by any information storage retrieval system, without per mission of AACN. For all permission requests, please contact the Copyright Clearance Center, Customer Ser-vice, 222 Rosewood Dr, Danvers, MA 01923. (978) 750-8400. Prices on bulk reprints of articles available on request from AACN at (800) 899-1712. Printed on acid-free paper. The AMERICAN JOURNAL OF CRITI-CAL CARE is indexed in MEDLINE/PubMed, Psy-cINFO, Cum u lative Index to Nursing & Allied Health Literature (CINAHL), Science Citation Index Expanded, ISI Alerting Services, Current Contents/Clinical Medi-cine, EBSCO collections, Ovid collections, and Scopus.
Annual individual subscriptions: US and possessions, $59; Canada and Mexico, $120 (US); all other countries, $120 (US). Institutional rates: US, print and online, $640; print only, $465; online only, $440. Institutional rates for all countries outside the US: print and online, $780; print only, $605; online only, $440. Single copies: US, $50; all other countries, $60 (US). For subscription questions: AACN members, please call toll-free (800) 899-2226 or (949) 362-2000; nonmembers, please call toll-free (800) 336-6348 or (818) 487-2075. Change of ad dress: Send notices to AMERICAN JOURNAL OF CRITICAL CARE, Subscrip-tion Service Depart ment, 101 Columbia, Aliso Viejo, CA 92656. Allow 4 to 6 weeks for change to take effect.
The statements and opinions contained in the articles in the AMERICAN JOURNAL OF CRITICAL CARE are solely those of the individual contributors and not of the editors or the American Association of Critical-Care Nurses. The edi-tors and the American Association of Critical-Care Nurses assume that articles emanating from a particular institu-tion are submitted with the approval of the requisite authority, including all matters pertaining to human stud-ies and patient privacy requirements. Advertisements in this journal are not a warranty, endorsement, or approval of the products by the editors of this journal or the Amer-ican Association of Critical-Care Nurses, who disclaim all responsibility for any injury to persons or property result-ing from any ideas or products referred to in the articles or advertisements.
Editors in Chief
CINDY L. MUNRO, RN, PhD, ANP
Dean and Professor, School of Nursing and Health Studies, University of Miami, Coral Gables, Florida
RICHARD H. SAVEL, MD
Adjunct Professor of Clinical Medicine and Neurology, SUNY Downstate College of Medicine, New York, New York
Clinical Advisers
LINDA BELL, RN, MSN
American Association of Critical-Care Nurses Aliso Viejo, California
Founding Coeditors
CHRISTOPHER W. BRYAN-BROWN, MD, and KATHLEEN DRACUP, RN, DNSc
Editorial Board
SARAH A. DELGADO, RN, MSN, ACNP-BC
American Association of Critical-Care NursesAliso Viejo, California
MICHAEL H. ACKERMAN, RN, DNS
Rochester, New York
THOMAS AHRENS, RN, DNS, CCRN
St Louis, Missouri
JOANN GRIF ALSPACH, RN, MSN, EdD
Annapolis, Maryland
JUDY L. BEZANSON, RN, DSN
Dallas, Texas
STIJN I. BLOT, RN, PhD
Ghent, Belgium
ELIZABETH J. BRIDGES, RN, PhD, CCNS, CCRN
Seattle, Washington
TIMOTHY G. BUCHMAN, PhD, MD, MCCM
Atlanta, Georgia
LINDA L. CHLAN, RN, PhD
Rochester, Minnesota
MARIANNE CHULAY, RN, DNSc
Southern Pines, North Carolina
MARTHA A. Q. CURLEY, RN, PhD
Boston, Massachusetts
RHONDA D’AGOSTINO, ACNP-BC
New York, New York
LYNN DOERING, RN, DNSc Los Angeles, California
BARBARA DREW, RN, PhD San Francisco, California
LEWIS A. EISEN, MD
Bronx, New York
DOUG ELLIOTT, RN, PhD
Sydney, New South Wales, Australia
SUSAN K. FRAZIER, RN, PhD Lexington, Kentucky
DORRIE K. FONTAINE, RN, DNSc
Charlottesville, Virginia
MARJORIE FUNK, RN, PhD
New Haven, Connecticut
MICHAEL A. GROPPER, MD, PhD
San Francisco, California
SANDRA HANNEMAN, RN, PhD
Houston, Texas
KATHRYN HAUGH, RN, PhD
Charlottesville, Virginia
STEVEN HOLLENBERG, MD
Camden, New Jersey
CONNIE JASTREMSKI, RN, MS, CNAA
Syracuse, New York
RUTH KLEINPELL, RN, PhD
Chicago, Illinois
CONSTANTINE MANTHOUS, MD
Bridgeport, Connecticut
PETER E. MORRIS, MD
Winston Salem, North Carolina
DEBRA K. MOSER, RN, DNSc Lexington, Kentucky
JANET D. PIERCE, DSN, ARNP Kansas City, Kansas
KATHLEEN PUNTILLO, RN, PhD
San Francisco, California
MARY LOU SOLE, RN, PhD
Orlando, Florida
THEODORE A. STERN, MD
Boston, Massachusetts
M. CHRISTINE STOCK, MD
Chicago, Illinois
KATHLEEN M. VOLLMAN, RN, MSN, CCNS, CCRN
Detroit, Michigan
DOUGLAS WHITE, MD, MAS
Pittsburgh, Pennsylvania
SUSAN WOODS, RN, PhD
Seattle, Washington
Printed in the USA.
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 165

AMERICAN JOURNAL OF CRITICAL CARE® (Print ISSN 1062-3264, Online ISSN 1937-710X) is published bi monthly (January, March, May, July, September, Nov ember) by the American Association of Critical-Care Nurses (AACN), 101 Columbia, Aliso Viejo, CA 92656. Periodicals postage paid at Laguna Beach, CA, and additional mailing office(s). Postmaster: Send address changes to the AMER ICAN JOURNAL OF CRITICAL CARE, Subscription Service Depart ment, 101 Columbia, Aliso Viejo, CA 92656.
Coming in July …Distinguished Research Lecturer Margaret L.
Campbell addresses the role of critical care
nurses in ensuring breathing comfort in pa-
tients at the end of life.
On the Cover
Detail from “Yeon-gyel (coupling) 1507”
Jeong Han Yun & Choon-Hyang Yun
16.5'' x 16.5''
Mixed media
2015
To view other works by
Jeong Han & Choon-Hyang Yun,
visit their website at
www.jeonghan.net
Critical Care Evaluation
Early Mobility in Critical Care
Critical Care Management
172 Effects of an Integrative Nursing Intervention on Pain in Critically Ill Patients: A Pilot Clinical TrialElizabeth D. E. Papathanassoglou, Maria Hadjibalassi,
Panagiota Miltiadous, Ekaterini Lambrinou, Evridiki Papastavrou,
Lefkios Paikousis, and Theodoros Kyprianou
186 Identifying Barriers to Nurse-Facilitated Patient Mobility in the Intensive Care UnitDaniel L. Young, Jason Seltzer, Mary Glover, Caroline Outten, Annette Lavezza,
Earl Mantheiy, Ann M. Parker, and Dale M. Needham
194 Mobilization Therapy in the Pediatric Intensive Care Unit: A Multidisciplinary Quality Improvement Initiative Blair R. L. Colwell, Cydni N. Williams, Serena P. Kelly, and Laura M. Ibsen
205 Early Blood Transfusions in Sepsis: Unchanged Survival and Increased CostsKarthik Raghunathan, Mandeep Singh, Brian H. Nathanson, Elliott Bennett-Guerrero,
and Peter K. Lindenauer
166 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
252 Abstracts of articles available exclusively online at www.ajcconline.org
e1 2018 National Teaching Institute Research Abstracts
May 2018, Volume 27, No. 3

212 Critical Care Nurses' Experiences With Spiritual Care: The SPIRIT StudyNigel Bone, Marilyn Swinton, Neala Hoad, Feli Toledo, and Deborah Cook
220 Survival of Patients With Severe Acute Respiratory Distress Syndrome Treated Without Extracorporeal Membrane OxygenationSarina K. Sahetya, Roy G. Brower, and R. Scott Stephens
228 Noninvasive Blood Pressure Monitoring and Prediction of Fluid Responsiveness to Passive Leg RaisingJoya D. Pickett, Elizabeth Bridges, Patricia A. Kritek, and JoAnne D. Whitney
238 Early Warning Score Communication Bundle: A Pilot StudyCheryl Gagne and Susan Fetzer
245 Effect of Dynamic Light Application on Cognitive Performance and Well-being of Intensive Care NursesKoen S. Simons, Enzio R. K. Boeijen, Marlies C. Mertens, Paul Rood, Cornelis
P.C. de Jager, and Mark van den Boogaard
End-of-Life Care
Pulmonary Critical Care
Cardiovascular Critical Care
Brief Report
168 Editorial Celebrating May—and Nursing!
Cindy L. Munro and
Richard H. Savel
170 Clinical Pearls Rhonda Board
171 Distinguished Research Lecture Abstract
Ensuring Breathing Comfort at
the End of Life: The Integral
Role of the Critical Care Nurse
Margaret L. Campbell
204 Patient Care Page No Time for Early Mobility?
Cindy Cain
243 Evidence-Based Review and Discussion Points
Ronald L. Hickman
249 ECG Puzzler The Value of Lead aVR:
A Frequently Neglected Lead
Salah S. Al-Zaiti, Teri M. Kozik,
Michele M. Pelter, and Mary G. Carey
252 Education Directory
Visit AJCC’s website, www.ajcconline.org, to submit a manuscript or for author guidelines, full text of selected articles, OnlineNOW articles, digital edition access, links to AACN’s online continuing education tests, and more.
An Official Publication of the American Association of Critical-Care Nurses
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 167

168 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
CELEBRATING MAY—AND NURSING! By Cindy L. Munro, RN, PhD, ANP, and Richard H. Savel, MD
Editorial
Comedian Robin Williams said, “Spring is
nature’s way of saying, ‘Let’s party!’”1 May is
the last month of spring, and it is a month
of celebration. Holidays include May Day (May 1st),
Cinco de Mayo (May 5th), Mother’s Day (the second
Sunday in May), and Memorial Day (the last Monday
in May). May is also a special time of celebration for
nursing. National Nurses Week traditionally begins
on May 6th with National Nurses Day and concludes
on May 12th with International Nurses Day, which is
also Florence Nightingale’s birthday. National Student
Nurses Day is May 8th, and School Nurses Day falls
on the Wednesday of Nurses Week. The American
Association of Critical-Care Nurses (AACN) National
Teaching Institute (NTI)—the premier gathering of
critical care nurses—is held in May of every year.
Recognition and celebration of the contributions of
nurses are appropriate all year long, but the special
emphasis in May is appreciated.
A new global initiative to recognize and celebrate
nursing was launched in February 2018. Nursing
Now is a 3-year campaign focused on acknowledg-
ing and expanding the worldwide involvement of
nursing in health.2 Key components of the campaign
are improving public perceptions of nurses, enhanc-
ing the infl uence of nurses, and maximizing nursing’s
contributions to health and access to health care.
Nursing Now is a collaborative effort with the Inter-
national Council of Nurses and the World Health
Organization. Nursing Now already has star power
on board; Her Royal Highness Catherine The Duch-
ess of Cambridge (née Kate Middleton) is the cam-
paign’s patron. The campaign will conclude in 2020,
coinciding with the 200th anniversary of Nightin-
gale’s birth.
The Nursing Now website ambitiously states,
“We work to empower nurses to take their place at
the heart of tackling 21st Century health challenges.”2
This statement affi rms that nurses are central to improv-
ing the health care system. The active involvement
of nurses in advancing health care in all settings is
crucial; nurses have both the capacity and the num-
bers to make a real difference.
Nurses’ capacity to drive change is centered in
extraordinary knowledge and patient care skills. Crit-
ical care nurses are grounded by their initial nursing
education, which enables them to care for patients
and families throughout the life span and in a vari-
ety of settings. Additional specialty education is built
upon this foundation, giving nurses who work in
critical care the tools they need to care for the highly
vulnerable patients and families entrusted to their care.
Some nurses will pursue graduate nursing education
at the master’s and doctoral level to expand their exper-
tise and to contribute to the scientifi c base of critical
care nursing. Many nurses pursue and achieve certifi -
cation in critical care, as a visible recognition of their
commitment to excellence. AACN offers certifi cation
in multiple specialties and subspecialties relevant to
critical care practice for bedside nurses, nurse manag-
ers, educators, and advanced practice nurses.
Nurses are well positioned to advance change
in the health care system because they are the largest ©2018American Association of Critical-Care Nursesdoi:https://doi.org/10.4037/ajcc2018206

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 169
group of health care clinicians worldwide, and they
are integral to every aspect of health care. The United
States has nearly 3 million registered nurses,3 and
registered nurses are the largest group of health care
providers. Registered nurses are also the largest com-
ponent of the critical care workforce. In the United
States alone, more than 500 000 critical care regis-
tered nurses work together with their colleagues
(15 000 acute care nurse practitioners, 10 000 physi-
cian intensivists, and many other members of the
critical care team) to meet the needs of critically
ill patients and their families.4
Leveraging the power of nursing’s capacity and
numbers should be an overarching goal of any cam-
paign to improve health. Particularly in critical care,
nursing exemplifies both leadership and collabora-
tive effort. Nursing Now will provide important
opportunities to advance the role of nursing world-
wide. We encourage nurses and other health profes-
sionals to follow the activities of Nursing Now as
the campaign matures and to contribute to advanc-
ing its important goals.
Every May, AACN’s NTI “offers learning, inspi-
ration and celebration for high-acuity and critical
care nurses.”5 This year’s conference in Boston will
bring an estimated 7000 critical care nurses and
their colleagues together for 4 days of celebration,
mentoring, education, and companionship. NTI
sessions offer up-to-date information about new
research and evidence-based practice that invigo-
rates patient care. Supersessions and interactions
with colleagues provide inspiration. Recognition
and celebration are central to NTI. Visionary
Leadership Awards are presented to nurses and
other critical care leaders for lifetime achievements.
Individual and AACN Chapter Circle of Excellence
Awards are celebrated. The AACN Distinguished
Research Lecture is a celebration of outstanding
critical care research. Units that have received Gold,
Silver, and Bronze Beacon Awards along a journey
for excellence are recognized during NTI. Attendees
leave NTI energized and empowered to improve
their units and their care of patients and families.
Of course, nurses are not the only critical care
professionals who deserve recognition and celebra-
tion! Meaningful recognition is one of 6 essential
standards underpinning the AACN Healthy Work
Environment Initiative. That standard is based on
the idea that, “Nurses must be recognized and must
recognize others for the value each brings to the work
of the organization.”6(p29) A sampling of upcoming
events relevant to recognizing the contributions of
critical care team members includes
National Physician Assistants Day: October 6,
2018
National Physical Therapy Month: October 2018
National Radiologic Technology Week: Novem-
ber 4-10, 2018
National Pharmacists Day: January 12, 2019
National Women Physicians Day: February 3,
2019
Certified Nurses Day: March 19, 2019
National Doctors Day: March 30, 2019
Recognition is not a zero-sum game, where a
win for one party can come only at the expense
of a loss for others. Rather, recognition should be a
“win-win.” The celebrations of nursing that occur
in May are a spring party that we can all enjoy!
The statements and opinions contained in this editorial are solely those of the coeditors in chief.
FINANCIAL DISCLOSURESNone reported.
REFERENCES1. Brainy Quotes. Robin Williams. https://www.brainyquote
.com/quotes/robin_williams_107638. Accessed March 3, 2018.2. Nursing Now. http://www.nursingnow.org/. Accessed
March 3, 2018.3. Bureau of Labor Statistics, US Department of Labor. Occu-
pational Outlook Handbook, Registered Nurses. https://www.bls.gov/ooh/healthcare/registered-nurses.htm. Accessed March 4, 2018.
4. Society of Critical Care Medicine. Critical Care Statistics, Staffing/Salary. http://www.sccm.org/Communications/Pages /CriticalCareStats.aspx. Accessed March 4, 2018.
5. American Association of Critical-Care Nurses. NTI 2018. https://www.aacn.org/conferences-and-events/nti. Accessed March 8, 2018.
6. American Association of Critical-Care Nurses. 2016. AACN Standards for Establishing and Sustaining Health Work Envi-ronments: A Journey to Excellence. 2nd ed. Aliso Viejo, CA: AACN; 2016.
To purchase electronic or print reprints, contact American Association of Critical-Care Nurses, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; e-mail, [email protected].
Nurses must be recognized and must recognize others for the value each brings to the work of the organization.
About the AuthorsCindy L. Munro is coeditor in chief of the American Journal of Critical Care. She is dean and professor, School of Nursing and Health Studies, University of Miami, Coral Gables, Florida. Richard H. Savel is coeditor in chief of the American Journal of Critical Care. He is director, Adult Critical Care Services, Maimonides Medical Center and adjunct professor of clinical medicine and neurology, SUNY Down state College of Medicine, both in New York City.

Clinical Pearls Rhonda Board, RN, PhD, CCRN, Section Editor
Clinical Pearls is designed to help implement evidence-based care at the bedside by summarizing some of the most clinically useful material from select articles in each issue. Readers are encouraged to photocopy this ready-to-post page and share it with colleagues. Please be advised, however, that any substantive change in patient care protocols should be carefully reviewed and approved by the policy-setting authorities at your institution.
Nurse-Facilitated Patient Mobility
Early movement can improve the muscle weakness commonly
experienced by patients in the intensive care unit and prevent potential long-term impairments. Nurse-facilitated mobility improves patient out-comes and decreases length of hospital stay. However, a commonly named barrier to nurse-facilitated mobilization is nurses’ lack of time. To understand time-related barriers, Young and colleagues designed a multidisciplinary team process to directly observe the work performed by nurses and clinical care technicians. They found the following: • Four categories of nurse work: patient care (47%), provider com-munication (25%), documentation (18%), and down time (10%). • The best times for potential mobility events occurred during direct patient care or down time. • Nursing team members noted that when mobility could be possible, it was not necessarily thought about. Direct observation of nursing care activities is a process that could be replicated by other institutions to provide insight in identifying missed opportunities for nurse-facilitated patient mobility.
See Article, pp 186-193
Patient Early Warning Scores
About half of adults admitted to intensive care units (ICUs) are patients whose condition has deteriorated while on a medical-surgical
unit. Patients’ early warning scores (EWSs) are based on physiological measures and were developed as a decision tool to help bedside nurses identify and take action when a patient decompensates. Fetzer and colleagues created an EWS bundle of interventions, including alerting an experienced ICU nurse, to improve communication and patient outcomes related to patient deterioration. After testing the bundle, they found the following: • The number of medical-surgical transfers to the ICU decreased. • The percentage of patients admitted to the ICU after a rapid response team (RRT) call decreased. • RRT calls increased in general but decreased for patients with an EWS greater than 4 (indicat-ing clinical deterioration), suggesting earlier identification and intervention occurred with deteriorating patients. Findings suggest that use of an electronically embedded EWS and a communication bundle with experienced ICU nurse collaboration can improve patient care and preserve health care costs.
See Article, pp 238-242
©2018 American Association of Critical-Care Nurses, doi:https://doi.org/10.4037/ajcc2018970
Nurses’ Experiences With Spiritual Care
Patients and families in the critical care setting often experience spiritual distress. Although most nurses do not receive education in how to provide spiritual
care to patients, most recognize it as part of holistic nurs-ing practice. Bone and colleagues interviewed nurses in an intensive care unit (ICU) to understand their experiences when making a referral for spiritual care for a dying patient and/or the patient’s family. They found the following 3 categories related to spiritual presence: 1. The value and role of chaplains: Chaplains were con-sidered an essential part of the ICU team and provided sup-port to both families and nurses. 2. Nurses’ experiences with chaplains: Nurses appreciated sharing care with chaplains and made referrals to them throughout a patient’s stay. 3. How ICU nurses provide spiritual care: Although nurses stated that compassion came naturally to them, providing spir-itual care was not always intentional or recognized as such. Nurses considered spiritual care important and valued chaplain support in the holistic care they provide to patients and their families.
See Article, pp 212-219
170 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
Putting Evidence-Based
Care in Your Hands
Effects of an Integrative Nursing Intervention on Pain in ICU Patients
Pain is a common symptom for many patients in the inten-sive care unit (ICU). Unrelieved pain can contribute to physical and psychological complications such as hemo-
dynamic instability, infections, anxiety, delirium, and post-ICU syndrome. The complex nature of pain management requires both pharmacological and nonpharmacological interventions. Papathanassoglou and colleagues examined the effects of a multimodal integrative intervention that included relax-ation and guided imagery, moderate pressure massage, and music listening. They found that patients receiving the inter-vention had • Decreased incidence of pain • Lower systolic blood pressure • Reduced fear • Decreased anxiety levels • Improved quality of sleep Although many of the patients had low acuity of illness, the authors suggest use of a multimodal daily intervention to reduce pain and improve pain-related outcomes in critically ill adults.
See Article, pp 172-185

Distinguished Research Lecture AbstractPresented May 21, 2018, at the AACN National Teaching Institute in Boston, Massachusetts
©2018 American Association of Critical-Care Nursesdoi:https://doi.org/10.4037/ajcc2018487
About the AuthorMargaret L. Campbell is a professor in the College of Nursing at Wayne State University, Detroit, Michigan.
Dyspnea is one of the worst symptoms experi-
enced by patients in the intensive care unit
and patients approaching the end of life.
The patients in the intensive care unit who are at the
highest risk include those with underlying cardiopul-
monary conditions and those with respiratory failure.
Critical care nurses are integral to assessing and treat-
ing dyspnea during the trajectory of critical care illness,
especially when a patient is not expected to survive
and care goals are shifted to focus on comfort. Para-
doxically, cognitive impairment develops along with
worsening dyspnea in dying patients, preventing
patients from reporting their distress while they
may still be able to experience it. Inability to report
distressing symptoms can lead to undertreatment or
overtreatment. The Respiratory Distress Observation
Scale (RDOS), developed by the author, is the only
known valid, reliable tool for assessing respiratory
distress when the patient cannot self- report dyspnea,
as typifies many critically ill patients. An evidence-
based approach to dyspnea assessment by patient
report and RDOS and treatment is addressed in this
lecture. Interventions are categorized into those that
are effective, interventions with limited effectiveness,
and interventions whose effectiveness has not been
established. In addition, a nurse-led, respiratory
therapist–supported ventilator withdrawal algorithm
guided by the RDOS is introduced.
Margaret L. Campbell’s presentation will be published in its
entirety in the July 2018 issue of AJCC.
ENSURING BREATHING COMFORT AT THE END OF LIFE: THE INTEGRAL ROLE OF THE CRITICAL CARE NURSEBy Margaret L. Campbell, RN, PhD
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 171

Critical Care Evaluation
©2018 American Association of Critical-Care Nursesdoi:https://doi.org/10.4037/ajcc2018271
Background Pain, a persistent problem in critically ill patients, adversely affects outcomes. Despite recom-mendations, no evidence-based nonpharmacological approaches for pain treatment in critically ill patients have been developed.Objectives To investigate the effects of a multimodal integrative intervention on the incidence of pain and on secondary outcomes: intensity of pain, hemodynamic indices (systolic and mean arterial pressure, heart rate), anxiety, fear, relaxation, optimism, and sleep quality.Methods A randomized, controlled, double-blinded repeated-measures trial with predetermined eligibility criteria was conducted. The intervention included relax-ation, guided imagery, moderate pressure massage, and listening to music. The primary outcome was incidence of pain (score on Critical Care Pain Observation Tool > 2). Other outcomes included pain ratings, hemodynamic measurements, self-reported psychological outcomes, and quality of sleep. Repeated-measures models with adjustments (baseline levels, confounders) were used.Results Among the 60 randomized critically ill adults in the sample, the intervention group experienced signifi-cant decreases in the incidence (P = .003) and ratings of pain (P < .001). Adjusted models revealed a significant trend for lower incidence (P = .002) and ratings (P < .001) of pain, systolic arterial pressure (P < .001), anxiety (P = .01), and improved quality of sleep (P = .02).Conclusion A multimodal integrative intervention may be effective in decreasing pain and improving pain- related outcomes in critically ill patients. (American Journal of Critical Care. 2018; 27:172-185)
EFFECTS OF AN INTEGRATIVE NURSING INTERVENTION ON PAIN IN CRITICALLY ILL PATIENTS: A PILOT CLINICAL TRIAL By Elizabeth D. E. Papathanassoglou, RN, MSc, PhD, Maria Hadjibalassi, RN, MSc,
PhD, Panagiota Miltiadous, PhD, Ekaterini Lambrinou, RN, MSc, PhD, Evridiki Papastavrou, RN, MSc, PhD, Lefkios Paikousis, and Theodoros Kyprianou, PhD, MD
1.0 HourC EThis article has been designated for CE contact
hour(s). See more CE information at the end of
this article.
172 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org

Intensive care unit (ICU) patients experience pain at rest and during procedures.1 Unre-lieved pain is common among ICU patients and may compromise outcomes, by contrib-uting to unstable hemodynamic parameters, hypercatabolism, hyperglycemia, infections, delirium, and posttraumatic stress.2 Pain in ICU patients may also be part of a vicious circle implicating anxiety3 and insomnia.4 Moreover, pain has been linked to the post-ICU
syndrome5 and may become chronic in survivors, a situation associated with poor quality of life and poor psychological and physiological outcomes.6
Management of pain in patients with a critical
illness is challenging.7 Opioids, the drug class of
choice, are associated with marked side effects, includ-
ing respiratory depression, hypotension, decreased
gastrointestinal motility, delirium, and higher costs
due to increased use of resources and prolonged stay
in the ICU.8 Nociception, the perception of painful
stimuli, entails a complex interaction among sensory,
affective, and social components.9 Moreover, anxiety,
fear, and negative expectations are common in criti-
cally ill patients and may contribute to heightened
perception of pain.10 Thus, the multifactorial nature
of ICU pain calls for approaches that address both
physiological and psychosocial responses to pain.
Current guidelines highlight the need to test and
implement nonpharmacological strategies for pain
treatment in critically ill patients.2 Interventions
that elicit a relaxation response, via parasympathetic
activation, appear to influence a some patients’
outcomes.11 For example, the authors of a recent
review12 concluded that guided imagery can decrease
pain and anxiety in critically ill patients. However,
studies on nonpharmacological interventions for
ICU pain and related outcomes are scarce. The
physiological pathway involved in decreasing pain
via relaxation-inducing interventions is unclear.13
Multiple synergistic mechanisms may be involved,
including distraction of attention, diminished
transmission of nociceptive signals due to descending
impulses from the brain during processing of relax-
ation cues, downregulation of the affective nociceptive
pathway, and perception of social connectedness.14-18
Objectives Our aim was to investigate measures of the effect
of a multimodal integrative intervention on the inci-
dence of pain (primary outcome) and several second-
ary outcomes: intensity of pain; hemodynamic indices
(systolic arterial pressure [SAP], mean arterial pressure
[MAP]), and heart rate); psychological outcomes (anxi-
ety, fear, feeling of relaxation, optimism); quality of
sleep; patient outcomes (complications, mortality);
and daily analgesic doses. Measures of effect were tested
before and after the intervention and longitudinally.
Literature Review and Definitions Relaxation, guided imagery, and music therapy
are categorized as mind-body interventions, whereas
touch and massage are con-
sidered body-based prac-
tices.19 Relaxation promotes a
sense of calmness often asso-
ciated with parasympathetic
activation.20 Guided imagery
involves focusing one’s imag-
ination on pleasurable cir-
cumstances in a way that
elicits emotion.19 Interper-
sonal touch or massage is a powerful means of mod-
ulating emotion, triggering neuroendocrine and
immune effects, vagal stimulation, and a reduction
in stress, pain, and depression.21
Recent evidence22 suggests that nonpharmaco-
logical interventions for pain, such as hand massage,
may be feasible and acceptable in critical care settings.
Moreover, both families of ICU patients and nurses
seem to regard nonpharmacological interventions
as relevant and feasible approaches for relief of ICU
pain.23 However, despite reports of increased effec-
tiveness of multimodal integrative interventions,24
few studies have addressed the impact of combining
About the AuthorsElizabeth D. E. Papathanassoglou is an associate profes-sor, Faculty of Nursing, University of Alberta, Edmonton, Alberta, Canada. Maria Hadjibalassi is an assistant pro-fessor Panagiota Miltiadous is special teaching staff, and Ekaterini Lambrinou and Evridiki Papastavrou are associate professors, Department of Nursing, Cyprus University of Technology, Limassol, Cyprus. Lefkios Paikousis is an analyst, Improvast Analytical Services Company, Nicosia, Cyprus. Theodoros Kyprianou is an associate professor, St Georges University of London Medical Program, Uni-versity of Nicosia Medical School, Nicosia, Cyprus.
Corresponding author: Elizabeth D. E. Papathanassoglou, RN, MSc, PhD, Faculty of Nursing, University of Alberta, Edmonton, Alberta, Canada, 5-262 Edmonton Clinic Health Academy, 11405-87th Ave, Edmonton, Alberta, Canada T6G 1C9 (email:[email protected]).
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 173
Perception of pain entails a complex interaction among sensory, affective, and social components.

174 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
integrative approaches in critically ill patients. In
most instances, relaxation was combined with guided
imagery25-27; in 1 study,28 relaxation and guided imag-
ery were combined with gentle massage. Anxiety, pain,
and sleep were the most common outcomes addressed,
and the results varied. However, little attention was
given to confounders and the effect and interactions
with time in previous studies.12
Methods The study has been registered at ClinicalTrials.gov
(Identifier: NCT02423252).
Ethical approval was obtained from the Cyprus
National Bioethics Committee, Republic of Cyprus.
Written informed consent was obtained from all
patients or their surrogates before recruitment. Each
participant’s assent was acquired when the partici-
pant regained capacity.
DesignWe conducted a randomized, controlled, double-
blinded (clinicians, outcome assessors) repeated-
measures pilot trial with 2 parallel groups (intervention
and standard care groups; Figure 1). The sample con-
sisted of patients admitted to a 17-bed academic
teaching general systems ICU in Cyprus. Patients
were eligible for the study if they were more than 18
years old, understood Greek, had a score of -2 to +2
on the Richmond Agitation-Sedation Scale, had a score
greater than 9 on the Glasgow Coma Scale (GCS) at
Figure 1 Schematic of study design.
Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; CPOT, Critical Care Pain Observation Tool; ICU, intensive care unit; MODS, multiple organ dysfunction syndrome; NRS, Numeric Rating Scale; RASS, Richmond Agitation-Sedation Scale; SOFA, Sequen-tial Organ Failure Assessment.
Before enrollment
Visit 1: time point 1 (day 1)
Visit 2-5: time point 2-5 (day 2-5) or until transfer
At ICU discharge
60 participants: Obtain informed consent, screen potential participants by inclusion and exclusion criteria, obtain history, document
Arm 1 (n = 30), study groupStandard care + intervention
Perform once-daily measurementsSleep NRS, APACHE II, SOFA, and MODS scores, daily dose of opioid and nonopioid analgesic agents
Perform preintervention measurementsVital signs; sleep NRS, APACHE II, SOFA, MODS, CPOT, pain NRS, anxiety NRS, relaxation NRS,
fear level NRS, and optimism NRS scoresRepeat study intervention
Perform postintervention assessmentsVital signs; CPOT, pain NRS, anxiety NRS, relaxation NRS, fear level NRS, and optimism NRS scores
Perform baseline assessmentsAge, sex, admission diagnosis, history of alcohol use, depression, baseline clinical data, intravenous sedation, anal-
gesia, vasoactive medication dose, and baseline RASS, CPOT (or pain NRS), APACHE II, MODS, and SOFA scoresAdminister study intervention
Randomize
Final follow-upsRate of complications: hospital-acquired infections, thromboembolism,
stress-related gastrointestinal bleeding, deliriumICU length of stay
Survival
Arm 2 (n = 30), control groupStandard care only

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 175
the time of inclusion, and had an arterial catheter
in place.
Patients were excluded if they had an expected
ICU length of stay less than 48 hours, had a current
history of severe mental health problems or demen-
tia, had a hearing impairment or conditions that
did not permit the use of headphones, were receiv-
ing neuromuscular blockers, were confused at the
time of screening (according to the assessment of
an expert research nurse; no formal tool for confu-
sion was used in the unit at the time), or required,
at the time of screening, special contact or isolation
precautions for any reason.
The size of the sample was predefined as 30
patients per arm. This pilot study was not powered to
determine a difference in a primary outcome, because
our aim was to assess estimates of effect and to
attain high probability of equivalence at baseline.29
Consecutive patients were screened daily (March
2013-March 2015) and were recruited for the study
by a research nurse (Figure 2). For patients who were
uncommunicative or incapable for any reason of
providing informed consent, the patients’ families
were approached to obtain written informed consent.
Participants were randomized (http://www
.randomization.com/) to an intervention (n = 30)
or a control (n = 30) group. Patients in the interven-
tion group received, in addition to standard care,
the daily 55-min intervention. Randomization blocks
of 4 allocations were based on participants’ age (≤ 45
years, > 45 years), sex (men, women), and systemic
inflammatory response syndrome (SIRS) status (SIRS,
no SIRS). Concealment during the intervention was
maintained by drawing the curtains around a partic-
ipant’s bed and by the presence of an intervention
nurse at the bedside for the set amount of time in
both the intervention and control groups. Before
the intervention, the intervention nurse negotiated a
time at which the participant (in either group: inter-
vention or control) could remain uninterrupted for
55 minutes with the bedside nurse and the partici-
pant’s family. However, if a clinical need arose, clini-
cians were free to enter the room. Clinicians and
all study personnel had no knowledge of the group
allocations. Outcomes were assessed by persons not
involved in patient care or in other aspects of the
trial and with no knowledge of the study. Allocation
was disclosed to the intervention nurse only. Partici-
pants were not blinded to the allocation.
InterventionThe intervention was delivered once daily
(between 9:30 AM and 11:30 AM) by a trained
intervention nurse not involved in patient care, for
up to 5 days during the ICU stay, starting the day after
ICU admission. The multimodal intervention, with a
duration of approximately 55 minutes, was based on
a literature review; recommendations of the American
Holistic Nurses Association30; recommendations of a
group of experts, including academics and clinicians
(n = 5); results of a small feasibility pilot test (n = 10);
and feedback of patients and patients’ families. The
selection of music (Mozart piano sonata KV 283)
was based on previous evidence of physiological
effects in the critically ill.31 The intervention included
relaxation and guided imagery (40 minutes) and
moderate-pressure massage (15 minutes). The seg-
ment of relaxation and guided imagery included
guided relaxation, a use of a structured guided
imagery script, and listening to music through head-
phones for 15 minutes. Moderate-pressure, low-
velocity (4 N, 1-5 cm/s) massage consisted of
squeezing movements with a wide area of contact
over the head, neck, trapezius muscles, and fore-
arms. Moderate-pressure massage was used because
Figure 2 Flowchart of enrollment of participants in the study.
Excluded (n = 552) Did not meet inclusion criteria (n = 337) Met exclusion criteria (n = 215)
Refused consent (n = 13)No timely access to family for consent (n = 14)
Patients screened for eligibility (n = 639)
Randomized (n = 60)
Allocated to standard-care group (n = 30)
Analyzed (n = 30)
Allocated to intervention group (n = 30)
Analyzed (n = 30)
Eligible for participation (n = 87)

176 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
After the intervention, participants in the intervention group
had 44% less chance of having indications
of pain than did the control participants.
it elicits parasympathetic activation, which light-
pressure massage does not.32 The efficacy of multi-
modal integrative interventions is superior to that of
1-dimensional ones.24
OutcomesThe primary outcome was incidence of pain as
indicated by a score greater than 2 on the Critical
Care Pain Observation Tool (CPOT). Secondary
outcomes were the CPOT score, self-reported pain
intensity according to a numeric rating scale (NRS),
observer-reported pain (NRS), systolic arterial pres-
sure (SAP), heart rate, respiratory rate, anxiety,
fear, relaxation, optimism, quality of sleep (self-
reported NRS scales), length of ICU stay (hours),
ICU survival, score on the
Sequential Organ Failure
Assessment (SOFA), multiple-
organ dysfunction syndrome
(MODS) score, and daily doses
of opioid (morphine equiva-
lents)33 and nonopioid (mg/
kg per 24 hour) analgesics.34
The aim of the interven-
tion was to elicit a relaxation
response, which, despite lack
of any pertinent evidence,
could in theory cause
increased parasympathetic tone and a decrease in
mean arterial pressure (MAP). Thus, MAP measure-
ments were used as a safety outcome for
intervention-induced impairment of tissue perfusion
(lower cutoff: 65 mm Hg).35 Physiological and
behavioral alterations and incidence of complica-
tions were reported (infections, thromboembolism,
organ dysfunction, delirium). Adverse events, irre-
spective of causal relationship, were noted for all
participants.
Data Collected. All clinical assessment scales
we used are routinely used in clinical practice with
established psychometrics, with the exception of
the NRS scale for the assessment of psychological
responses, which had been tested during the pre-
liminary pilot phase during which we pilot tested
use of the instruments. Measurements were col-
lected by trained data collectors with no knowledge
of the study. Interrater reliability was established
during the pilot phase ( > 0.80).
Three pain assessment scales were used: CPOT,
the 0 to 10 NRS, and the 0 to 10 observer-rated NRS.
The Greek CPOT has reliability and validity similar
to those of the original version.36,37 Although a CPOT
score greater than 2 indicates presence of pain, the
CPOT value has also been used as a pain score.38 We
used CPOT to assess both presence and intensity of
pain, because of the lack of tools for uncommunicative
patients.39 Communicative patients also indicated their
pain on the NRS. Following the recommendation of
the panel of experts, we used an observer NRS as an
indicator of nurses’ assessment of patients’ pain that
can be a basis for clinical judgments. Observers’ NRS
ratings correlate highly with patients’ NRS values, but
observers tend to underestimate pain when a patient’s
NRS score is greater than 4.40 We also collected val-
ues for clinical variables to use as control variables in
the analysis: age, sex, vital signs, SOFA score, MODS
score, presence of SIRS, score on the Acute Physiology
and Chronic Health Evaluation (APACHE) II, use of
analgesics, and use of vasoactive medications.
Data AnalysisWe checked variables for normality and used
transformations as needed. We did baseline and
cross-sectional comparisons between the interven-
tion and control groups by using an independent t
test or the Fisher exact test. We analyzed the pri-
mary outcome by using a logistic regression model
and the binary logistic link function41 based on
generalized estimating equations with autoregres-
sive first-order correlation structure. We used the
quasi-likelihood under independence model crite-
rion to compare model fit across covariance struc-
tures. To assess the effect of the intervention, we
used the adjusted estimated marginal means of
the proportions at each time measurement. These
proportions were adjusted for within participant
“time,” taking into account the correlation of pain
incidents between time points. The odds ratio (OR)
was calculated at each time point.
For effects on continuous variables, we used a
linear mixed models approach with autoregressive
or unstructured covariance structure for parsimony.
The best model fit was selected on the basis of the
Akaike Information Criterion. We calculated effect
sizes by using estimated marginal means and calcu-
lating the Cohen d. For effects at discrete time points,
analysis of covariance (ANCOVA) was performed to
control for pretreatment measurements and a num-
ber of confounders. The Cohen f was calculated as a
measure of effect size.42
Not all participants were able to self-report
NRS scores, especially after day 2, when most
communicative participants would be discharged.
The effect of the intervention on self-reported NRS
scores was assessed by using a linear mixed model
for the first 2 days only and ANCOVA for the first

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 177
Within the first 2 days of interven-tion, anxiety levels in the intervention group decreased, whereas those in the control group remained stable.
day of intervention. Linear mixed models for self-
reported psychological responses were fit for the
first 2 days under the unstructured covariance matrix,
with 1 covariate at a time, because adding more
covariates resulted in nonconvergence. ORs and
95% CIs were calculated for rates of complications.
We used SPSS, version 21, software (IBM SPSS) for
analysis; with an of .05.
Results Participants and Baseline Characteristics
In the final sample of 60 participants, the 2
groups had no statistically significant differences
(Table 1). No losses in the number of participants
occurred after randomization, and no participants
skipped a session. Only a small proportion of partici-
pants completed 5 days of intervention (6 in the
intervention group and 2 in the control group)
because of earlier discharge from the unit. No
adverse events were reported.
Primary Outcome: Presence of PainIncidence of pain (CPOT > 2) had a downward
trend in both groups, with a clear trend for postin-
tervention decreases in the intervention group (Table
2A). Analysis with generalized estimating equations
revealed that the trend for decreased pain incidence
was significantly greater in the intervention group
than in the control group: Wald 21 = 18.0; P = .003;
(Table 2B). After adjustment (sex and age), the
effect of the intervention remained significant
(P = .002).
At the first preintervention measurement, 43%
of participants in the control group and 57% in the
intervention group had indications of pain (CPOT > 2;
OR = 1.76). After the intervention, participants in
the intervention group had 44% less chance of
having indications of pain than did participants
in the control group (OR = 0.42; Table 3C).
Secondary OutcomesCPOT Scores. Mean CPOT scores on day 1 before
the intervention were equivalent (P = .52) in the con-
trol (2.7; SD, 1.2) and the intervention (2.5; SD, 1.1)
groups. On day 1 after the intervention, mean CPOT
scores were 1.44 (SD, 1.26) in the intervention
group and 2.5 (SD, 1.29) in the control group, a
finding that suggests a large effect size (P = .004;
Cohen d = 0.83; Table 3A). Over time, mean CPOT
scores in both groups showed a downward trend,
with a consistent trend for decreased CPOT values
after the intervention in the intervention group.
Adjusted linear mixed models (age, sex) indicated
a significant interaction effect of the intervention
group (P < .001). When only postintervention mea-
surements were used, the intervention effect over
time remained significant, with a large effect size
(P < .001; Cohen d = 0.77-1.10; Table 3A).
An ANCOVA for CPOT scores 1 day after the
intervention (adjustments: preintervention scores
for pain, SOFA, MODS, SIRS, and APACHE II; doses
of analgesics), showed a significant difference in
postintervention pain in the intervention group
(P < .001). The study group explained 30% of the
variation of postintervention CPOT scores (partial 2 = 0.3; Table 2C).
Self-reported Pain NRS. Preintervention self-
reported pain did not differ between the 2 groups
(P = .30, Table 1). On day 1 after the intervention,
pain NRS scores were lower in the intervention
group than in the control group, with a large effect
size (P < .001; Cohen d = 1.21; Table 3B).
The effect of the intervention over time was sig-
nificant, with a large effect size (adjustments for age,
sex; linear mixed model; P < .01; Tables 3B and 4B).
An ANCOVA of self-reported pain
NRS scores 1 day after the interven-
tion (adjustments for preinterven-
tion scores of self-reported pain
NRS, SOFA, SIRS, and APACHE II
and doses of analgesics), indicated
a significant decrease in pain in the
intervention group (P < .001; partial 2 = 0.353).
Hemodynamic Measurements. On
day 1 after the intervention, partici-
pants in the intervention group had
a decrease in SAP, with a moderate
to large effect size (P = .02; Cohen
d = 0.63; Table 3G). The interven-
tion effect over time was significant, even after
adjustment for confounders, with a moderate
effect size (P = .008; Cohen d = 0.63-0.89; Table 4).
An ANCOVA for mean SAP on day 1 after the
intervention (adjustments: preintervention scores
for SAP, SOFA, SIRS, APACHE II; doses of vasoactive
medication) indicated a significant decrease in SAP
in the intervention group (P < .04).
Before the intervention, MAP levels did not
differ significantly (P = .81) between the 2 groups or
in linear mixed model and ANCOVA analyses. No
statistically significant differences in heart rate and
respiratory rate were evident (Table 1). Both adjusted
and unadjusted linear models and ANCOVA analyses
indicated no significant differences (P > .06; Cohen
d = 0.21-0.52; relative risk = 0.59-0.71).

178 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
Variable
Variable
Variable
Variable
Table 1Baseline clinical data of the intervention and control groups
Demographic and clinical data Female sex, No. (%) Age, mean (SD), y Body mass index,c mean (SD) SIRS, No. (%) Mechanical ventilation (intubated), No. (%)
Clinical assessment score, mean (SD) RASS GCS APACHE II SOFA MODS
Vital signs, mean (SD) SAP DAP MAP Heart rate Respiratory rate Body temperature
Pain score, mean (SD) CPOT NRS self-reported NRS observer
Subjective baseline assessment score, mean (SD) Anxiety Fear Relaxation Optimism Sleep quality
Diagnostic categories, No. (%) Neurosurgical Heart surgery Burns Medical Coronary Surgical Pulmonary
Comorbid conditions, No. (%) CAD Hyperlipidemia Hypertension Diabetes COPD/respiratory failure Renal failure
Vasoactive medication, day 1, No. (%) Any type Dobutamine Dopamine Norepinephrine Nitroglycerin Esmolol
11 (37) 63.9 (12.7) 30.7 (7.1) 7 (23) 4 (13)
-0.1 (0.5) 14.1 (3.0) 17.0 (5.9) 4.2 (1.2) 3.4 (1.8)
125.7 (18.6) 62.4 (15.1) 82.1 (14.0) 84.8 (15.5) 21.1 (5.9) 36.7 (0.6)
2.7 (1.2) 3.7 (2.1) 4.9 (1.5)
4.0 (1.7) 3.2 (2.2) 5.5 (1.6) 5.8 (1.5) 4.2 (2.1)
2 (7) 25 (83) 0 (0) 0 (0) 0 (0) 1 (3) 2 (7)
12 (40) 3 (10) 22 (73) 11 (37) 3 (10) 1 (3)
15 (50) 4 (13) 12 (40) 1 (3) 3 (10) 0 (0)
9 (30) 62.4 (12.9) 28.7 (5.7) 12 (40) 3 (10)
-0.5 (0.5) 13.4 (2.6) 15.1 (6.2) 4.7 (2.0) 3.3 (1.6)
128.9 (22.2) 60.1 (10.5) 81.3 (12.1) 90.8 (15.6) 23.0 (4.4) 36.6 (0.6)
2.5 (1.1) 4.4 (2.4) 5.0 (1.6)
4.7 (2.4) 4.4 (3.1) 5.0 (1.4) 6.1 (1.9) 4.4 (2.4)
5 (17) 15 (50) 1 (3) 2 (7) 2 (7) 2 (7) 3 (10)
13 (43) 0 (0) 19 (63) 11 (37) 3 (10) 1 (3)
8 (27) 1 (3) 6 (20) 0 (0) 2 (7) 1 (3)
.39a
.66b
.23b
.27a
>.99a
.11 .35 .23 .25 .87
.55 .48 .81 .14 .16 .82
.52 .30 .74
.23 .23 .18 .69 .79
.16
>.99 .24 .58 .79>.99>.99
.06 .35 .16>.99>.99>.99
-1.667-0.942-1.207 1.169-0.160
0.600-0.706-0.241 1.488 1.440-0.234
-0.640 1.042 0.338
1.212 1.228-1.344 0.403 0.274
7 (12)40 (67) 1 (2) 2 (3) 2 (3) 3 (5) 5 (8)
25 (42) 3 (5)41 (68)20 (33) 6 (10) 2 (3)
23 (38) 5 (8)18 (30) 1 (2) 5 (8) 1 (2)
Intervention (n = 30)
Intervention (n = 30)
Control (n = 30)
Control (n = 30)
TotalControl (n = 30)Intervention (n = 30)
TotalControl (n = 30)Intervention (n = 30)
P
Pb
Pa
Pd
t
Continued

Variable
Table 1Continued
Analgesics, day 1, No. (%) Any type Paracetamol Morphine ASA Fentanyl Pethidine
26 (87)18 (60) 6 (20)13 (43) 5 (17) 0 (0)
20 (67)17 (57) 4 (13) 5 (17) 5 (17) 2 (7)
.12>.99 .73 .05>.99 .49
46 (77)35 (58)10 (17)18 (50)10 (17) 2 (3)
Intervention (n = 30) Control (n = 30) Total Pd
Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; ASA, acetylsalicylic acid; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; CPOT, Critical Care Pain Observation Tool; DAP, diastolic arterial blood pressure; GCS, Glasgow Coma Scale; ICU, intensive care unit; MAP, mean arterial blood pressure; MODS, multiple organ dysfunction syndrome; NRS, Numeric Rating Scale; RASS, Richmond Agitation-Sedation Scale; RGI, relaxation and guided imagery; SAP, systolic arterial blood pressure; SIRS, systemic inflammatory response syndrome; SOFA: Sequential Organ Failure Assessment.
a From 2 test. b From t test. c Calculated as weight in kilograms divided by height in meters squared.d Fisher exact test.
Day
Source
Source
Table 2Effects of the intervention on the presence of pain (CPOT score > 2) and CPOT pain ratings
First Before intervention After interventionSecond Before intervention After interventionThird Before intervention After intervention
Corrected modelInterceptInterventionSexPain at baselineAgeAnalgesicsAPACHE II scoreSIRS scoreSOFA scoreMODS score
Intercept Group Time Group x Time, QIC = 233. AR(1) covariance structure.
57 (9)24 (8)
38 (14) 9 (9)
23 (16)12 (12)
5.084 0.10611.798 0.81119.360 1.153 0.249 0.118<0.001 1.650 1.551
15.6 0.024.718.0
43 (9)43 (9)
18 (7)13 (7)
23 (13)18 (12)
0.6240.0040.3000.0290.4130.0400.0090.0040.0000.0570.053
6.834 0.14215.861 1.09026.026 1.550 0.335 0.159 0.000 2.218 2.085
91111111111
1155
1.76 0.42
2.790.66
1.000.62
<.001.71
<.001.30
<.001.22.57.69
>.99.14.16
<.001.94
<.001 .003
Intervention
Mean square F df
Wald 2
A. Adjusted prevalence of paina
Mean percentage (SE)
C. ANCOVA (dependent variable: first day postintervention CPOT scores)c
B. GEE for repeated measurements (dependent variable: CPOT score > 2)b
Control
Partial 2
df
Odds ratio (intervention vs control)
P
P
Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; AR (1), autoregressive first order; CPOT, Critical Care Pain Observation Tool; MODS, multiple organ dysfunction syndrome; QIC, quasi-information criterion; SIRS, systemic inflammatory response syndrome; SOFA: Sequential Organ Failure Assessment. a Adjusted (for the within-subject correlation across time) prevalence of pain (CPOT > 2) during the first 3 days of observation and related odds ratios for pain.b Generalized estimating equations (GEE) accounting for repeated measurements.c Analysis of covariance (ANCOVA) for first day postintervention CPOT scores.

Continued
Content
Table 3Point estimates of repeated measurements and differences in pain, psychological outcomes, and sleep quality from before to after the intervention for the 5 days of the interventiona
A. CPOTIntervention N Mean SDControl N Mean SDAdjusted Cohen d
B. Self-reported NRS pain ratingsIntervention N Mean SDControl N Mean SDAdjusted Cohen d
C. AnxietyIntervention N Mean SDControl N Mean SDAdjusted Cohen d
D. FearIntervention N Mean SDControl N Mean SDAdjusted Cohen d
E. Relaxation Intervention N Mean SDControl N Mean SDAdjusted Cohen d
F. OptimismIntervention N Mean SDControl N Mean SDAdjusted Cohen d
29 2.50 1.14
30 2.70 1.24 0.16
24 3.71 2.14
22 4.41 2.42 0.01
264.01.7
22 4.7 2.4 0.42
183.22.2
114.43.1
0.43
265.51.6
225.01.4
0.35
11 6.090.50
18 5.91 0.39 0.11
25 1.44 1.26
28 2.50 1.29 0.88
20 2.35 1.63
20 4.55 1.99 1.37
22 2.9 1.7
16 4.3 2.5 1.05
131.91.9
83.93.41.14
22 6.6 2.3
16 4.8 1.6 1.21
95.740.52
146.920.400.79
12 2.00 1.13
12 1.67 1.61 0.03
82.252.55
63.001.790.82
82.62.3
74.02.60.78
72.02.2
53.02.80.74
86.41.8
75.41.30.66
46.530.68
76.940.520.29
11 1.18 0.98
11 1.73 1.68 0.77
82.382.07
53.201.921.83
62.31.9
54.22.61.25
52.22.0
33.02.61.12
66.22.6
55.00.70.80
36.860.83
56.970.620.16
81.751.04
91.781.300.44
42.001.63
43.252.221.41
51.02.2
53.82.21.62
50.81.8
33.02.62.20
58.01.0
55.40.91.16
36.860.80
56.860.680.01
81.500.76
71.571.400.60
40.250.50
24.500.712.26
41.82.1
33.02.61.18
41.82.1
22.02.81.44
47.81.7
35.71.21.22
28.340.87
46.810.650.20
61.170.41
52.201.641.10
30.6671.154
15.000.00
42.02.4
22.53.5
41.82.1
22.53.5
48.30.5
26.01.4
60.830.41
41.500.581.50
200
15.000.00
32.32.1
10.00.0
32.32.1
10.00.0
38.70.6
17.00.0
41.250.50
21.000.00
32.3302.516
31.32.3
10.00.0
30.71.2
10.00.0
38.30.6
16.00.0
41.000.82
21.000.00
20.5000.707
31.01.7
10.00.0
30.71.2
10.00.0
38.31.2
16.00.0
BeforeBeforeBeforeBeforeBefore AfterAfterAfterAfterAfter
First day Second day Third day Fourth day Fifth day

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 181
Psychological Responses. Within the first 2 days,
anxiety levels in the intervention group decreased,
whereas those in the control group were stable
(Table 3C). The intervention had a significant effect
over time, even after adjustments for heart rate or
SAP (Cohen d = 1.04-1.24; Table 4). An adjusted
ANCOVA for anxiety 1 day after the intervention
indicated a significant decrease in the intervention
group (P = .01; f = 0.506).
Fear was moderate with a general downward
trend in both groups (Table 3D). Analysis with lin-
ear models indicated a nonstatistically significant
effect of the intervention (over a 2-day period;
P = .05; Cohen d = 1.13-1.44; Table 4). An adjusted
ANCOVA for fear on day 1 after the intervention
decreased significantly in the intervention group
(P = .04; f = 0.562).
Relaxation NRS ratings indicated a trend for
improvement in both groups (Table 3E). Linear
mixed models showed a significant effect of the
intervention in a 2-day observation period (P < .001;
Cohen d = 0.79-1.22; Table 4). An unadjusted
ANCOVA for ratings obtained 1 day after the inter-
vention indicated a significant increase in relaxation
in the intervention group (P = .004; f = 0.517); how-
ever, the adjusted model showed no statistical signif-
icance (P = .07; f = 0.352).
Optimism ratings fluctuated and had a moder-
ate upward trend in both groups (Table 3F). Linear
mixed models indicated that the effect of the inter-
vention during a 3-day observation period was sig-
nificant (P = .01; Cohen d = 0.76-1.97; Table 4). An
unadjusted ANCOVA showed a significant increase
in optimism in the intervention group (P = .02;
f = 0.574); however, after adjustments, the increase
was not significant (P = .16; f = 0.348).
Quality of Sleep. Self-reported quality of sleep
showed a trend toward gradual improvement in
both groups (Table 3G). During the first 2 days,
changes in sleep quality did not differ significantly
between the 2 groups (P = .98). Nevertheless, during
a 4-day observation period, sleep quality improved
significantly in the intervention group (P = .02,) with
a progressively increasing effect size (Cohen d = 0.1-
3.5). The effect of the intervention over time was sig-
nificant (linear models P = .02; Table 4).
Participants’ Outcomes. Incidence of respiratory
complications (atelectasis and pneumonia) was
higher in the control group (7) than in intervention
group (3): 2 = 1.9; P = .16; OR = 0.36; 95% CI = 0.08-
1.57). The incidence of delirium was also higher in
the control group: ( 2 = 3.2; P = .08). Renal failure
developed in 1 participant in the intervention group
and in none of the participants in the control group.
Content
Table 3Continued
G. Sleep qualityIntervention N Mean SDControl N Mean SDAdjusted Cohen d
H. SAPIntervention N Mean SDControl N Mean SDAdjusted Cohen d
254.22.1
214.62.40.22
30125.7 18.6
30128.9 22.20.16
30120.8 17.5
30133.3 21.50.63
75.33.4
66.31.20.06
13133.4 22.9
14130.5 19.30.03
13127.2 19.8
14138.6 24.10.80
66.81.7
55.01.21.09
9122.7 16.1
11131.9 20.00.87
9122.2 19.2
10133.6 20.70.88
48.01.2
25.50.71.60
7124.7 22.2
7141.4 16.91.39
7125.9 21.1
5134.8 25.10.89
38.71.5
16.00.0
6126.5 12.0
2118.5 21.9
5121.2 14.5
2108.5 12.0
Before BeforeBeforeBeforeBeforeAfter AfterAfterAfterAfter
First day Second day Third day Fourth day Fifth day
Abbreviations: CPOT, Critical Care Pain Observation Tool; N, number of participants; NRS, Numeric Rating Scale; SAP, systolic arterial blood pressure.
a Adjusted Cohen d effect sizes are based on estimated marginal means and are shown for those days for which linear mixed models could converge.
182 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
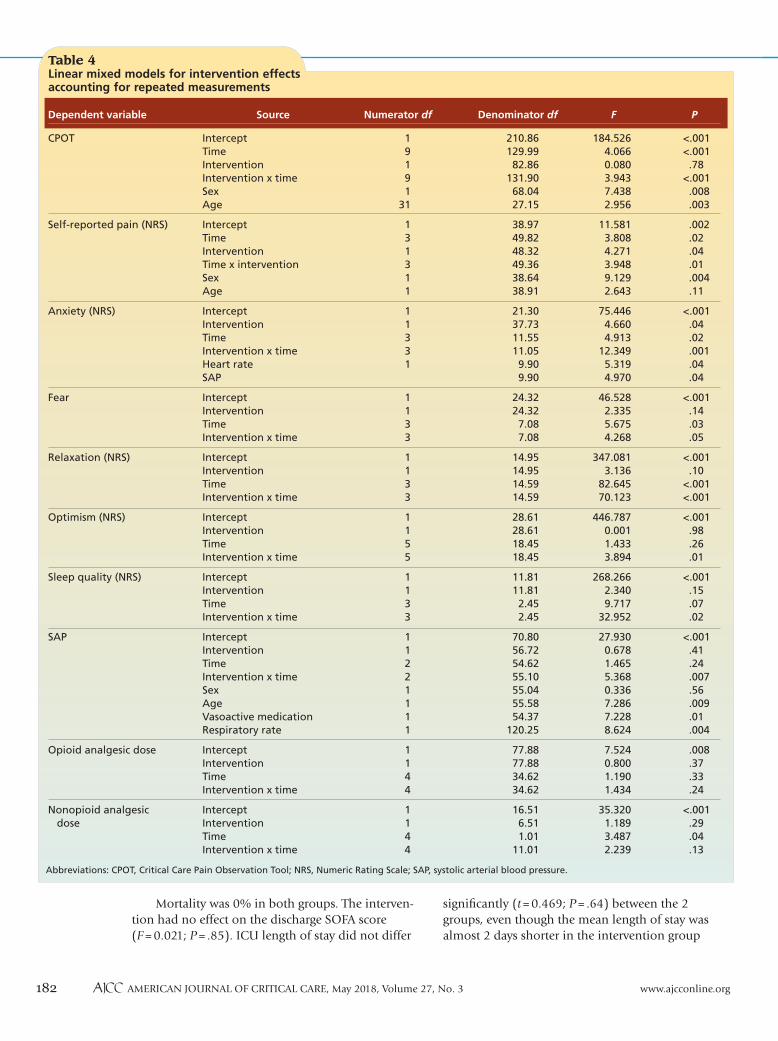
Mortality was 0% in both groups. The interven-
tion had no effect on the discharge SOFA score
(F = 0.021; P = .85). ICU length of stay did not differ
significantly (t = 0.469; P = .64) between the 2
groups, even though the mean length of stay was
almost 2 days shorter in the intervention group
Dependent variable
Table 4Linear mixed models for intervention effects accounting for repeated measurements
CPOT
Self-reported pain (NRS)
Anxiety (NRS)
Fear
Relaxation (NRS)
Optimism (NRS)
Sleep quality (NRS)
SAP
Opioid analgesic dose
Nonopioid analgesic dose
<.001<.001 .78<.001 .008 .003
.002 .02 .04 .01 .004 .11
<.001 .04 .02 .001 .04 .04
<.001 .14 .03 .05
<.001 .10<.001<.001
<.001 .98 .26 .01
<.001 .15 .07 .02
<.001 .41 .24 .007 .56 .009 .01 .004
.008 .37 .33 .24
<.001 .29 .04 .13
184.526 4.066 0.080 3.943 7.438 2.956
11.581 3.808 4.271 3.948 9.129 2.643
75.446 4.660 4.913 12.349 5.319 4.970
46.528 2.335 5.675 4.268
347.081 3.136 82.645 70.123
446.787 0.001 1.433 3.894
268.266 2.340 9.717 32.952
27.930 0.678 1.465 5.368 0.336 7.286 7.228 8.624
7.524 0.800 1.190 1.434
35.320 1.189 3.487 2.239
210.86129.99 82.86131.90 68.04 27.15
38.97 49.82 48.32 49.36 38.64 38.91
21.30 37.73 11.55 11.05 9.90 9.90
24.32 24.32 7.08 7.08
14.95 14.95 14.59 14.59
28.61 28.61 18.45 18.45
11.81 11.81 2.45 2.45
70.80 56.72 54.62 55.10 55.04 55.58 54.37120.25
77.88 77.88 34.62 34.62
16.51 6.51 1.01 11.01
1 9 1 9 131
1 3 1 3 1 1
1 1 3 3 1
1 1 3 3
1 1 3 3
1 1 5 5
1 1 3 3
1 1 2 2 1 1 1 1
1 1 4 4
1 1 4 4
InterceptTimeInterventionIntervention x time SexAge
InterceptTimeInterventionTime x interventionSexAge
InterceptInterventionTimeIntervention x timeHeart rateSAP
InterceptInterventionTimeIntervention x time
InterceptInterventionTimeIntervention x time
InterceptInterventionTimeIntervention x time
InterceptInterventionTimeIntervention x time
InterceptInterventionTimeIntervention x timeSexAgeVasoactive medicationRespiratory rate
InterceptInterventionTimeIntervention x time
InterceptInterventionTimeIntervention x time
PFDenominator dfNumerator dfSource
Abbreviations: CPOT, Critical Care Pain Observation Tool; NRS, Numeric Rating Scale; SAP, systolic arterial blood pressure.

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 183
(mean, 7.6; SD, 13.8) than in the control group
(mean, 9.4; SD, 14).
Use of Analgesics. The intervention had no sig-
nificant effect on the use of opioid (P = .24) or
nonopioid (P = .13) analgesics (Table 4), despite a
nonstatistically significant trend for decreased use
of nonopioids in the intervention group. Over time,
use of opioid analgesics remained approximately
constant in both groups.
Discussion We used a multimodal intervention and com-
prehensively assessed its effects on participants’
pain via subjective and behavioral assessments,
analgesic use, and related physiological and psy-
chological measures. We included a longer term
intervention, and, for the first time, we used
repeated-measures modeling. Our main findings
included a moderate to large effect size in decreas-
ing pain incidence and subjective, objective, and
behavioral pain ratings; a moderate effect size in
lowering SAP; a moderate to progressively large
effect size on the quality of sleep; and a moderate
effect size on anxiety, fear, and relaxation.
The intervention-associated decrease in pain is
consistent with previous reports28,43-45 of relaxation-
inducing interventions in critical and noncritical care
settings. The decrease in pain did not correspond to
use of analgesics, which remained almost stable, in
line with previous results.46 This finding may be under-
standable on the basis of clinical practices, because at
the time of the study, pain assessment tools were not
used in the unit, and, therefore, prescription of
analgesics was not based on valid assessments.
The multifactorial physiology of nociception
may favor multimodal rather than unimodal inter-
ventions, and this physiological context may be a
reason for the large effect sizes we observed.
Although the difference in complication rates may
reflect the bias of using a small sample, increased
atelectasis or pneumonia and delirium in the con-
trol group may be commensurate with higher pain.
The decrease in SAP is in accordance with
reports47-53 of interventions consisting of music or
massage. The intervention did not evoke unfavorable
hemodynamic effects; SAP and MAP were maintained
within the normal reference range. Although the tim-
ing of the effect may indicate parasympathetic trig-
gering, this notion is not commensurate with the
lack of effect on heart rate. Future research needs
to address the underlying mechanisms.
Anxiety and fear interfere with perception of
pain.9 The intervention-associated decrease in
anxiety is in line with previous reports on relax-
ation,28,44-46,54 music,48,49,55 and touch-massage.21,55,56
We also found some effect of the intervention on
patients’ fear, which is an important outcome
because fear is involved in pain perception.57 No
previous studies have addressed fear responses.
The effect of the intervention on relaxation agrees
with findings of a small pretest-posttest trial58 and is
important because anxiety can initiate a neuroendo-
crine cascade that interferes with recovery.59,60 The
moderate effect on optimism is noteworthy, because
optimism may modulate anxiety responses.61 The
improvement in self-reported quality of sleep is an
important finding, because lack of sleep may elicit
feedback to anxiety and pain.62 Previous research
with unimodal interventions did not show signifi-
cant effects on sleep54; multimodal interventions can
be more effective.25,26 Although testing the mediating
effect of sedation on relaxation and anxiety outcomes
would be interesting, only a few patients in our
study (1 participant per arm) continued to receive
sedation after day 1. Therefore such an investiga-
tion was not possible.
LimitationsLimitations include the small number of partic-
ipants and the progressive loss of participants, and
thus the loss of statistical power, as ICU patients were
discharged. Although we used block randomization
and adjustment, a larger study is needed to confirm
our results. On the basis of the eligibility criteria,
participants had overall low acuity and sedation
levels; therefore our conclusions may not be extrap-
olated to more severely ill patients. In the future, a
thorough assessment of the effect of sedation on
the effectiveness of the intervention is warranted.
The progressive loss of participants as they got better
and were discharged might have introduced type II
error and bias (either overestimation or underesti-
mation of the effects of the intervention) because
only the most severely ill participants remained in
the study. Moreover, the self-reporting nature of
many of the outcome variables contributed to miss-
ing values if participants were unable to self-report.
To mitigate the loss of statistical power as ICU patients
were discharged, we confirmed analyses by applying
longer and shorter term follow-up periods. However,
our results need to be tested in a larger sample with
inclusion criteria that would allow for longer follow-up.
Another limitation might be due to incom-
plete concealment; clinicians might have entered a
participant’s space at the time of intervention. We
tried to mitigate this risk by having independent

184 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
assessors, not employed in the unit, perform assess-
ments before and after the intervention. Although evi-
dence63 indicates the merits of allowing patients to
self-select music, for this pilot study we decided to
keep all aspects of the intervention constant. How-
ever, not allowing patients to self-select music might
have resulted in underestimation of the usefulness
of the intervention, especially in participants who
did not enjoy classical music.
Conclusions A multimodal integrative intervention delivered
once daily may be effective and safe in decreasing
pain and in improving pain-related outcomes in
critically ill patients. Cost-effectiveness associated
with costs for use of resources by personnel must be
addressed in the future. Moreover, in future attempts
to replicate our results with similar eligibility crite-
ria, a 2-day intervention would be more appropriate
to avoid postintervention attrition.
Financial DisclosuresThis research was supported by a Cyprus University of Technology faculty grant and a University of Alberta establishment grant to Dr Papathanassoglou.
REFERENCES1. Puntillo KA, Max A, Timsit JF, et al. Determinants of proce-
dural pain intensity in the intensive care unit: the Europain study. Am J Respir Crit Care Med. 2014;189(1):39-47.
2. Barr J, Fraser GL, Puntillo K et al; American College of Criti-cal Care Medicine. Clinical practice guidelines for the man-agement of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med. 2013;70(1):263-306.
3. Oh J, Sohn JH, Shin CS, et al. Mutual relationship between anxiety and pain in the intensive care unit and its effect on medications. J Crit Care. 2015;30(5):1043-1048.
4. Jaiswal SJ, Malhotra A, Owens RL. Sleep and critical illness: bridging the two pillars at the ATS 2016. J Thorac Dis. 2016; 8(suppl 7):S536-S538.
5. Davidson JE, Harvey MA, Bemis-Dougherty A, Smith JM, Hopkins RO. Implementation of the pain, agitation, and delirium clinical practice guidelines and promoting patient mobility to prevent post-intensive care syndrome. Crit Care Med. 2013;41(9)(suppl 1):136-145.
6. Battle CE, Lovett S, Hutchings H. Chronic pain in survivors of critical illness: a retrospective analysis of incidence and risk factors. Crit Care. 2013;17(1): R101.
7. Georgiou E, Hadjibalassi M, Lambrinou E, Andreou P, Papa-thanassoglou ED. The impact of pain assessment on criti-cally ill patients’ outcomes: a systematic review. Biomed Res Int. 2015;2015:503830. doi:10.1155/2015/503830.
8. Hughes CG, McGrane S, Pandharipande PP. Sedation in the intensive care setting. Clin Pharmacol. 2012;4:53-63.
9. Papathanassoglou E. Recent advances in understanding pain: what lies ahead for critical care? Nurs Crit Care. 2014; 19(3):110-113. doi: 10.1111/nicc.12097
10. Peris A, Bonizzoli M, Iozzelli D, et al. Early intra-intensive care unit psychological intervention promotes recovery from post traumatic stress disorders, anxiety and depression symptoms in critically ill patients. Crit Care. 2011; 15(1):R41.
11. Oke SL, Tracey KJ. The inflammatory reflex and the role of complementary and alternative medical therapies. Ann N Y Acad Sci. 2009;1172:172-180.
12. Hadjibalassi M, Lambrinou E, Papastavrou E, Papathanas-soglou E. The effect of guided imagery on physiological and psychological outcomes of adult ICU patients: a sys-tematic literature review and methodological implica-tions [published online March 29, 2017]. Aust Crit Care. doi:10.1016/j.aucc.2017.03.001.
13. Papathanassoglou E, Park T. To put the patient in the best condition: integrating integrative therapies in critical care. Nurs Crit Care. 2016;21(3):123-126.
14. Umezawa S, Higurashi T, Uchiyama S, et al. Visual distraction alone for the improvement of colonoscopy-related pain and satisfaction. World J Gastroenterol. 2015; 21(15):4707-4714.
15. Volz MS, Suarez-Contreras V, Portilla AL, Fregni F. Mental imagery-induced attention modulates pain perception and cortical excitability. BMC Neurosci. 2015;16:15.
16. Bonapace J, Chaillet N, Gaumond I, Paul-Savoie E, March-and S. Evaluation of the Bonapace Method: a specific edu-cational intervention to reduce pain during childbirth. J Pain Res. 2013;6:653-661.
17. Eisenberger NI. The neural bases of social pain: evidence for shared representations with physical pain. Psychosom Med. 2012;74(2):126-135.
18. Kross E, Berman MG, Mischel W, Smith EE, Wager TD. Social rejection shares somatosensory representations with phys-ical pain. Proc Natl Acad Sci U S A. 2011;108(15):6270-6275.
19. Complementary, alternative, or integrative health: what’s in a name? National Center for Complementary and Integra-tive Health. NCCIH publication D347. https://nccih.nih.gov /health/integrative-health. Updated June 2016. Accessed January 22, 2017.
20. Sanders S, reviewer. Am J Clin Hypn. 1981;24(1):65-66. Review of: Edmonston WE Jr. Hypnosis and Relaxation: Modern Verification of an Old Equation.
21. Papathanassoglou ED, Mpouzika MD. Interpersonal touch: physiological effects in critical care. Biol Res Nurs. 2012; 14(4):431-443.
22. Martorella G, Boitor M, Michaud C, Gélinas C. Feasibility and acceptability of hand massage therapy for pain man-agement of postoperative cardiac surgery patients in the intensive care unit. Heart Lung. 2014;43(5):437-444.
23. Gélinas C, Arbour C, Michaud C, Robar L, Côté J. Patients and ICU nurses’ perspectives of non-pharmacological inter-ventions for pain management. Nurs Crit Care. 2013; 18(6):307-318.
24. Hermann C. Psychological interventions for chronic pediat-ric pain: state of the art, current developments and open questions. Pain Manag. 2011;1(5):473-483.
25. Richards KC. Effect of a back massage and relaxation inter-vention on sleep in critically ill patients. Am J Crit Care. 1998;7(4):288-299.
26. Richardson S. Effects of relaxation and imagery on the sleep of critically ill adults. Dimens Crit Care Nurs. 2003; 22(4): 182-190.
27. Stein T, Olivo E, Grand S, Namerow P, Costa J, Oz M. A pilot study to assess the effects of a guided imagery audiotape intervention on psychological outcomes in patients under-going coronary artery bypass graft surgery. Holist Nurs Pract. 2010;24(4):213-222.
28. Kshettry V, Carole L, Henly S, Sendelbach S, Kummer B. Complementary alternative medical therapies for heart surgery patients: feasibility, safety, and impact. Ann Thorac Surg. 2006;81(1):201-205.
29. Moore CG, Carter RE, Nietert PJ, Stewart PW. Recommen-dations for planning pilot studies in clinical and translational research. Clin Transl Sci. 2011;4(5):332-337.
30. Dossey BM, Keegan L. Holistic Nursing: A Handbook for Practice. 5th ed. Boston MA: Jones & Bartlett Learning; 2009.
31. Conrad C, Niess H, Jauch KW, Bruns CJ, Hartl W, Welker L. Overture for growth hormone: requiem for interleukin-6? Crit Care Med. 2007;35(12):2709-2713.
32. Diego MA, Field T. Moderate pressure massage elicits a parasympathetic nervous system response. Int J Neurosci. 2009;119(5):630-638.
33. Faculty of Medicine and Dentistry, University of Alberta. Opioid conversion guide. https://www.ualberta.ca/medicine /institutes-centres-groups/multidisciplinary-pain-clinic/for -healthcare-professionals/opioid-conversion-guide. Accessed January 22, 2018.
34. Koh W, Nguyen KP, Jahr JS. Intravenous non-opioid analge-sia for peri- and postoperative pain management: a scientific review of intravenous acetaminophen and ibuprofen. Korean J Anesthesiol. 2015;68(1):3-12.
35. Callaway CW, Donnino MW, Fink EL, et al. Part 8: Post-cardiac arrest care: 2015 American Heart Association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care [published correction appears in Circulation. 2017;136(10):e197]. Circulation. 2015; 132(18)(suppl 2):S465-S482.

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 185
36. Mamoura K. Validation of the Greek Version of the Critical Care Pain Observation Tool [master’s thesis]. Athens, Greece: National and Kapodistrian University of Athens; 2017.
37. Gélinas C, Fillion L, Puntillo KA, Viens C, Fortier M. Valida-tion of the Critical-Care Pain Observation Tool in adult patients. Am J Crit Care. 2006;15(4):420-427.
38. Li Q, Wan X, Gu C, et al. Pain assessment using the Critical-Care Pain Observation Tool in Chinese critically ill ventilated adults. J Pain Symptom Manage. 2014;8(5):975-982.
39. Chanques G, Viel E, Constantin JM, et al. The measurement of pain in intensive care unit: comparison of 5 self-report intensity scales. Pain. 2010;151(3):711-721.
40. Ahlers SJ, van Gulik L, van der Veen AM, et al. Comparison of different pain scoring systems in critically ill patients in a general ICU. Crit Care. 2008;12(1):R15.
41. Twisk J. Applied Longitudinal Data Analysis for Epidemiology. 2nd ed. Cambridge, UK: Cambridge University Press; 2013.
42. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Associates; 1988.
43. Deisch P, Soukup SM, Adams P, Wild MC. Guided imagery: replication study using coronary artery bypass graft patients. Nurs Clin North Am. 2000;35(2):417-425.
44. Tusek D L, Cwynar R, Cosgrove DM. Effect of guided imag-ery on length of stay, pain and anxiety in cardiac surgery patients. J Cardiovasc Manag. 1999;10(2):22-28.
45. Kuo B, Bhasin M, Jacquart J, et al. Genomic and clinical effects associated with a relaxation response mind-body interven-tion in patients with irritable bowel syndrome and inflam-matory bowel disease [published correction appears in PLos One. 2017;12(2):e0172872]. PLoS One. 2015; 10(4): e0123861.
46. Ashton C Jr, Whitworth GC, Seldomridge JA, et al. Self-hypnosis reduces anxiety following coronary artery bypass surgery: a prospective, randomized trial. J Cardiovasc Surg (Torino). 1997;38(1):69-75.
47. Mofredj A, Alaya S, Tassaioust K, Bahloul H, Mrabet A. Music therapy, a review of the potential therapeutic benefits for the critically ill. J Crit Care. 2016;35:195-199.
48. Wong HL, Lopez-Nahas V, Molassiotis A. Effects of music therapy on anxiety in ventilator-dependent patients. Heart Lung. 2001;30(5):376-387.
49. Han L, Li JP, Sit JW, Chung L, Jiao ZY, Ma WG. Effects of music intervention on physiological stress response and anxiety level of mechanically ventilated patients in China: a ran-domised controlled trial. J Clin Nurs. 2010;19(7-8):978-987.
50. Dijkstra BM, Gamel C, van der Bijl JJ, Bots ML, Kesecioglu J. The effects of music on physiological responses and sedation scores in sedated, mechanically ventilated patients. J Clin Nurs. 2010;19(7-8):1030-1039.
51. Albert NM, Gillinov AM, Lytle BW, Feng J, Cwynar R, Black-stone EH. A randomized trial of massage therapy after heart surgery. Heart Lung. 2009;38(6):480-490.
52. Vahedian-Azimi A, Ebadi A, Asghari Jafarabadi M, Saadat S,
Ahmadi F. Effect of massage therapy on vital signs and GCS scores of ICU patients: a randomized controlled clinical trial. Trauma Mon. 2014;19(3):e17031.
53. Adib-Hajbaghery M, Abasi A, Rajabi-Beheshtabad R. Whole body massage for reducing anxiety and stabilizing vital signs of patients in cardiac care unit. Med J Islam Repub Iran. 2014;28:47.
54. Casida JM, Yaremchuk KL, Shpakoff L, Marrocco A, Babicz G, Yarandi H. The effects of guided imagery on sleep and inflam-matory response in cardiac surgery: a pilot randomized con-trolled trial. J Cardiovasc Surg (Torino). 2013;54(2):269-279.
55. Lee OK, Chung YF, Chan MF, Chan WM. Music and its effect on the physiological responses and anxiety levels of patients receiving mechanical ventilation: a pilot study. J Clin Nurs. 2005;14(5):609-620.
56. Henricson M, Ersson A, Määttä S, Segesten K, Berglund AL. The outcome of tactile touch on stress parameters in inten-sive care: a randomized controlled trial. Complement Ther Clin Pract. 2008;14(4):244-254.
57. Palstam A, Larsson A, Löfgren M, et al. Decrease of fear avoid-ance beliefs following person-centered progressive resistance exercise contributes to reduced pain disability in women with fibromyalgia: secondary exploratory analyses from a random-ized controlled trial. Arthritis Res Ther. 2016; 18(1): 116.
58. Hattan J, King L, Griffiths P. The impact of foot massage and guided relaxation following cardiac surgery: a randomized controlled trial. J Adv Nurs. 2002;37(2):199-207.
59. Lusk B, Lash AA. The stress response, psychoneuroimmunol-ogy, and stress among ICU patients. Dimens Crit Care Nurs. 2005;24(1):25-31.
60. Papathanassoglou ED, Giannakopoulou M, Mpouzika M, Bozas E, Karabinis A. Potential effects of stress in critical illness through the role of stress neuropeptides. Nurs Crit Care. 2010;15(4):204-216.
61. Castillo MI, Cooke M, Macfarlane B, Aitken LM. Factors asso-ciated with anxiety in critically ill patients: a prospective observational cohort study. Int J Nurs Stud. 2016;60:225-233.
62. Stewart JA, Green C, Stewart J, Tiruvoipati R. Factors influencing quality of sleep among non-mechanically ventilated patients in the intensive care unit. Aust Crit Care. 2017; 30(2):85-90.
63. Heiderscheit A, Chlan L, Donley K. Instituting a music listen-ing intervention for critically ill patients receiving mechani-cal ventilation: exemplars from two patient cases. Music Med. 2011;3(4):239-246.
To purchase electronic or print reprints, contact American Association of Critical-Care Nurses, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; email, [email protected].
1.0 Hour Category BC ENotice to CE enrollees:
This article has been designated for CE contact hour(s). The evaluation demonstrates your knowledge of the
following objectives:
1. Identify factors implicated in the perception of pain in the critically ill.
2. Describe the role of nonpharmacological therapies in the treatment of critical illness pain.
3. Discuss the research design issues for studies examining the effectiveness of integrative interventions in criti-
cal care.
To complete the evaluation for CE contact hour(s) for this article #A1827033, visit www.ajcconline.org and
click the “CE Articles” button. No CE evaluation fee for AACN members. This expires on May 1, 2021.
The American Association of Critical-Care Nurses is an accredited provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. AACN has been approved as a provider of continuing education in nursing by the State Boards of Registered Nursing of California (#01036) and Louisiana (#LSBN12).

Early Mobility in Critical Care
©2018 American Association of Critical-Care Nursesdoi:https://doi.org/10.4037/ajcc2018368
Background Nurse-facilitated mobility of patients in the intensive care unit can improve outcomes. However, a gap exists between research findings and their implemen-tation as part of routine clinical practice. Such a gap is often attributed, in part, to the barrier of lack of time. The Translating Evidence Into Practice model provides a framework for research implementation, including rec-ommendations for identifying barriers to implementa-tion via direct observation of clinical care.Objectives To report on design, implementation, and outcomes of an approach to identify and understand lack of time as a barrier to nurse-facilitated mobility in the intensive care unit.Methods An interprofessional team designed the obser-vational process and evaluated the resulting data by using qualitative content analysis. Results During three 4-hour observations of 2 nurses and 1 nursing technician, 194 distinct tasks were per-formed (ie, events). A total of 4 categories of nurses’ work were identified: patient care (47% of observation time), provider communication (25%), documentation (18%), and down time (10%). In addition, 3 types of potential mobility events were identified: in bed, edge of bed, and out of bed. The 194 observed events included 34 instances (18%) of potential mobility events that could be implemented: in bed (53%), edge of bed (6%), and out of bed (41%). Conclusions Nurses have limited time for additional clinical activities but may miss potentially important opportunities for facilitating patient mobility during existing patient care. The proposed method is feasible and helpful in empirically investigating barriers to nurse-facilitated patient mobility in the intensive care unit. (American Journal of Critical Care. 2018; 27:186-193)
IDENTIFYING BARRIERS TO NURSE-FACILITATED PATIENT MOBILITY IN THE INTENSIVE CARE UNITBy Daniel L. Young, PT, DPT, PhD, Jason Seltzer, PT, DPT, Mary Glover, RN, Caroline Outten, RN, BSN, CCRN, Annette Lavezza, OTR/L, Earl Mantheiy, BA, Ann M. Parker, MD, and Dale M. Needham, MD, PhD, FCPA
186 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
This article is followed by an AJCC Patient Care Page on page 204.

The muscle weakness commonly experienced by survivors of critical illness is a potentially modifiable risk factor for long-term functional impairment, mortality, and use of health care resources.1-12 Facilitating early mobility of patients in the intensive care unit (ICU) can reduce such muscle weakness13,14 and can be done safely and feasibly, even in patients receiving mechanical ventilation who have an
endotracheal tube in place.15-21 Many ICU mobilization efforts have engaged physical and occupational therapists (PTs and OTs), but successfully changing an ICU culture of bed rest requires the involvement of all clinicians.13,19,22
Engaging ICU nurses to mobilize patients can
have positive outcomes.23-25 In an international, mul-
ticentered, blinded randomized controlled trial,8,26
a multidisciplinary team set a daily mobility goal for
each patient, and ICU nurses worked with the patient
to meet that goal. The results indicated that such
nurse-facilitated mobility improved patients’ mobil-
ity status and decreased length of stay.8 However, a
gap exists between research evidence and its imple-
mentation as part of routine clinical practice in the
ICU.17,27,28 Structured quality improvement projects
play a critical role in bridging that gap.29,30
One framework for designing and executing
structured quality improvement projects is the
Translating Evidence Into Practice (TRIP) model.31
The model has 4 stages: summarize the evidence,
identify local barriers, measure performance, and
ensure patients receive the intervention via an itera-
tive process of engaging, educating, executing, and
evaluating. Within the TRIP model, stage 2 high-
lights the need to identify local barriers to imple-
mentation and recommends direct observation of
clinicians as a successful approach to inform quality
improvement efforts. For nurse-facilitated mobiliza-
tion in the ICU, a commonly cited barrier is lack of
time.17,20,32,33 However, to our knowledge, design
and implementation of a method to understand
this specific barrier have not been undertaken. Hence,
our objective was to report on the design, imple-
mentation, and outcomes of an approach to identi-
fying and understanding the barrier of lack of time
for nurse-facilitated mobility in the ICU.
Methods Background
An early rehabilitation quality improvement
project with the TRIP model was previously con-
ducted in the Johns Hopkins Hospital medical ICU
(MICU).29,34 This project increased early rehabilita-
tion, with interventions primarily
performed by PTs and OTs. However,
lighter sedation35 and a growing cul-
ture of mobility clearly indicated
that MICU patients have the poten-
tial for mobility and activity via inter-
ventions facilitated by nurses and
clinical technicians in addition to
interventions performed by PTs and
OTs. To understand time-related bar-
riers to performing such interventions in our MICU,
we directly observed the work carried out by nurses
and a clinical technician and measured the time
required for that work in order to understand the
feasibility of integrating mobility interventions into
the daily activities of nurses and technicians.
Interprofessional Generation of IdeasThe first step in this project involved interpro-
fessional discussions and planning by members of
the quality improvement team, including physi-
cians (D.M.N., A.M.P.), nurses (M.G., C.O.), physical
About the AuthorsDaniel L. Young is an associate professor, Department of Physical Therapy, University of Nevada Las Vegas, Las Vegas, Nevada, and a visiting scientist, Department of Physical Medicine and Rehabilitation, and Outcomes After Critical Illness and Surgery (OACIS) Group, Johns Hopkins University, Baltimore, Maryland. Jason Seltzer is intensive care unit rehabilitation team coordinator, Department of Physical Medicine and Rehabilitation, and OACIS Group, Johns Hopkins Hospital, Baltimore, Maryland. Annette Lavezza is therapy manager, Depart-ment of Physical Medicine and Rehabilitation, and OACIS Group, Johns Hopkins Hospital. Mary Glover is a nurse clinician, medical intensive care unit, Johns Hopkins Hospital. Caroline Outten is a nurse clinician, Department of Medicine, Johns Hopkins Hospital. Earl Mantheiy is senior clinical coordinator, Division of Pulmonary and Critical Care Medicine, and OACIS Group, Johns Hopkins University. Ann M. Parker is an assistant professor, Divi-sion of Pulmonary and Critical Care Medicine, and OACIS Group, Johns Hopkins University. Dale M. Needham is a professor, Division of Pulmonary and Critical Care Medi-cine, Department of Physical Medicine and Rehabilitation, and OACIS Group, Johns Hopkins University.
Corresponding author: Dale M. Needham, MD, 5th Floor, 1830 E Monument St, Baltimore, MD 21205 (e-mail: dale .needham @jhmi.edu).
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 187
Understanding of barriers to nurse-facilitated patient mobility needs to improve.

188 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
We directly observed nurses and measured
the time required for their work.
therapists (J.S., A.T.), an occupational therapist (A.L.),
and a senior clinical coordinator for the ICU clinical
rehabilitation program (E.M.). In these meetings,
team members discussed the idea of directly observ-
ing and recording work-related activities of nurses
and clinical technicians. Including clinical techni-
cians was suggested because they are delegated
certain tasks to perform by MICU nurses, including
mobility-related interventions. The quality improve-
ment team decided that direct observation would be
a valuable way to “walk the process” of nurses’ work
activities and clarify the lack-of-time barrier. The Johns
Hopkins University institutional review board deemed
the project quality improvement, under the US Office
for Human Research Protections guidance, with no
need for consent of patients or clinicians.
Planning the ObservationsWithin the framework of typical case sampling,36
a type of purposive sampling, representative days,
times of day, and personnel for the observations
were determined via discussions with nurses on
the quality improvement team. The quality improve-
ment team wanted to observe times that included
typical responsibilities of nurses, such as morning
report, initial patient assess-
ment, routine patient assess-
ments, and MICU team rounds,
because these routine nursing
events were generalizable to
most patients. The quality
improvement team wanted to
avoid observations of times when
nonroutine events occur more
frequently or when mobility may be less feasible. In
our MICU, such times include 11:30 AM to 3:30 PM,
when tests and procedures unique to individual
patients occur more frequently, and during the
night shift. Hence, observations were planned for 3
consecutive days: day 1, from 3 PM to 7:30 PM; day 2,
from 7 AM to 10 AM; and day 3, from 7 AM to 11 AM.
The nurse or technician to be observed was selected
to achieve variability in staff experience and
patient characteristics. In the MICU, 1 nurse with
more than 5 years of experience and 1 with less
than 2 years of experience were chosen. One nurse
had a 2-patient assignment; the other, a 1-patient
assignment. The third observation was designated
for a clinical technician, as previously explained.
The quality improvement team thought that this
mix of days, times, and personnel was representa-
tive and feasible for this project.
Executing Direct ObservationsA physical therapist (J.S.), the rehabilitation
team coordinator for the hospital’s adult ICUs,
performed all observations, for a total of 10 hours.
During these times, the observer’s goal was to watch
the designated nurse or clinical technician and record
all of their activities and the time spent on each activ-
ity. Using a paper-based logbook, the observer chrono-
logically recorded a description of each task performed
by the nurse or technician (eg, assessments, admin-
istering medications) with the associated starting and
ending time for each event. In order to reduce the
potential for modifying staff attitudes or behaviors,
the specific purpose of the observation was described
as better understanding nurses’ workflow, without
mentioning the specific focus on understanding
barriers to patient mobilization.
Review of the Observation Logbook Four members of the project team, 2 nurses
(M.G., C.O.) and 2 physical therapists (J.S., D.L.Y),
met in person to receive a brief orientation (by
J.S.) to the observation logbook, including defini-
tion of abbreviations, and to receive a copy of the
logbook for their individual reviews. These 4 team
members used qualitative content analysis37 to
evaluate the logbooks. First, each of the 4 mem-
bers independently read the logbook to become
familiar with its content, identify “meaning units,”
and categorize those meaning units into codes.37
For example, 1 activity logbook entry reads, “Addi-
tional family member calls to talk to RN. On
phone discusses social aspects of pt care, too many
family members involved asking for updates. RN
arranges specific family members who are identi-
fied by current family member (P.O.A.) who can
receive info.” The meaning unit here would be
family member calls to talk to RN, and the code
created was family-centered care. D.L.Y. then reviewed
all 4 coded logbooks and identified 4 categories37
into which all codes fit: patient care (eg, measur-
ing blood pressure, administering medication,
talking to a patient’s family), documentation (eg,
keying in the electronic medical record), provider
communication (eg, talking with the patient’s
physician, taking report from another nurse),
and down time (eg, time during which the nurse
or technician had no active demands). The catego-
ries assigned to each event were then reviewed by
the other 3 members of the research team in a
group meeting, and discrepancies were resolved
by consensus.

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 189
More mobility opportunities were identified for in-bed activities than out-of-bed or edge-of-bed activities.
Review of Potential for Mobility Using the analyses of the logbooks, the 4 mem-
bers of the project team (M.G., C.O., J.S., D.L.Y.)
met and collectively discussed potential for nurse-
facilitated mobility events, what those activities might
have been, and when the activities could have
occurred. For example, when the logbook stated,
“Bed laid flat, bed elevated to begin clean up. Chang-
ing chucks [disposable bed pads], linens that are
soiled, places new brief down,” the 4 members
thought that the nurse could have encouraged the
patient to “roll and bridge actively” (1 example of
a code from this process) as the linens, chuck, and
brief were changed. Another example that was noted
several times in the logbook was meals being served
in bed, and the 4 members identified the opportu-
nity for the nurse to help the patient sit at the edge
of bed, or get out of bed to a chair, to eat the meal
(“out of bed for meals” was the code used). When
the logbook indicated that time was spent in work
away from the patient (eg, documentation), the 4
members thought that mobility was not possible.
On the basis of these group discussions, 4 categories
of potential mobility events emerged: not possible,
in bed, edge of bed, and out of bed. These categories
for potential mobility events, along with the codes
from which they were created, were added to the
logbook. As a result of this process, each event in
the logbook was assigned 2 categories, 1 for general
workload (patient care, documentation, provider
communication, down time) and 1 for potential
mobility (not determined, in bed, edge of bed, out
of bed).
Results Design
The first step in the design process was assem-
bling the interdisciplinary quality improvement
team. This process was an iterative one, conducted
during 3 MICU quality improvement group meet-
ings, devoted to identifying appropriate personnel
needed for this specific project. Once the team
members to execute this specific project were identi-
fied, two 1-hour meetings were needed to outline
the plan for the observations and discuss questions
about those specific methods. One of the more
time-consuming items on the agenda of those 2
meetings was discussing who and when to observe.
Selecting the right person to perform the observa-
tions was also discussed in detail. The final issue
was creating the logbook. Attention was given to
create adequate space for detailed descriptions of
desired elements for the observed work and for
notation of potential mobility activities. The origi-
nal logbooks were created and implemented in
paper form, but for analysis, they were transcribed
into an electronic document.
ImplementationAs planned, the observations took approximately
11 hours (655 minutes). We found no indication that
the observations created disruption or concern for the
clinicians being observed, the
patient, or anyone else coming
into a patient’s room. Transcrip-
tion of the observation log into
an electronic document took 1.5
hours. The qualitative analysis
involved three 1-hour meetings
with 4 of the team members
(M.G., C.O., J.S., D.L.Y.), 1 hour
for each person to identify the
meaning units and codes inde-
pendently, and another 2 hours
for D.L.Y. to apply categories to the logs. Total time
for this part of the project was approximately 11 hours
for observation and 20 person-hours for analysis.
OutcomesThe results of the qualitative content analysis
of activities and time revealed 194 distinct events
observed during a period of 655 total minutes (Table
1). As expected, patient care accounted for the larg-
est part of observed time (47%) among the 4 defined
categories. The second largest time commitment
(25%) was communication with other health care
providers. Documentation accounted for 18% and
down time for 10%. Table 2 provides examples of
logbook entries and the codes and categories that
were assigned to those entries during the qualitative
content analysis.
The final step in completing the qualitative
content analysis of the logbook data was identifying
potential mobility events. The number of logbook
entries during which mobility could have been
Activity observed
Table 1Direct observation of nurse and clinical technician activity, by category
Patient care
Provider communication
Documentation
Down time
Total
305 (47)
166 (25)
116 (18)
68 (10)
655 (100)
115 (59)
47 (24)
27 (14)
5 (3)
194 (100)
Time required, min (%)
Distinct tasks observed, No. (%)

190 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
facilitated is reported in Table 3. As expected, all
potential mobility events were identified during
times of direct patient care or down time. The not
possible category for mobility events had the most
events (82%) and time (79% of observed minutes)
and included all time spent in communication
with other providers and in documentation. More
opportunities were identified for in-bed activities
(9%) and out-of-bed activities (7%) than for edge-
of-bed activities (1%). However, in-bed activities
were the third largest category in terms of minutes
(6%), after not possible (79%) and out of bed
(15%). Table 4 provides examples of logbook
entries, codes, and categories that were assigned to
those entries during the qualitative content analysis.
Discussion We devised a process to investigate the lack-of-
time barrier that nurses often express when asked
about facilitating mobility of their patients. Using
the TRIP model31 as a guide, we explored this barrier
by using a direct observation approach. Herein we
have provided the design, implementation, and out-
comes of the approach. This approach was feasible
and provided valuable insight into how nurses and
clinical technicians spend their time and where
potential mobility could occur. We observed that
nurses and clinical technicians working with nurses
have relatively little time not already filled with
patient care and related tasks. However, coincid-
ing with direct patient care, we detected important
opportunities for patient mobility that could be
facilitated by a nurse or a technician.
Our observations confirm that nurses are
busy.38-41 The nurses and clinician technician were
completely free from work tasks for only 10% of the
observed time, and most of that time was attributed
to the clinical technician, rather than nurses. This
Logbook observation
Table 2Examples of logbook observations of clinician activities with assigned codes and categories
Performing assessment
Face-to-face communication
Comfort and safety
Facilitating ADLs/IADLs
NA
Communication with patient
Getting supplies/medications
Documentation
Facilitating ADLs/IADLsPerforming assessment
Documentation
Patient safety and comfort
Face-to-face communication
Enters room 58, checks blood pressure to assess vitals prior to giving BP meds
Approached by buddy to take report on 2 patients (room 59 and…) while buddy is on lunch break
Pillows replaced under both arms, pt assists with placement of pillows, demonstrating shoulder AROM
Prepare to enter room 60 where pt is delirious, asking to go to bathroom. Pt is put on bedpan
Done charting
Pt spontaneously moving, RN addressing pt directly at eye level to attempt to calm down
Gathers supplies from supply room for 58: chucks, briefs, wipes, linens
Starts filing out rounding template (update to provide to team since last report, issues, concerns, drips pt has been started on)
Breakfast arrives, sets pt up to eat in bed and takes dexi
Updates and rereads notes from multi D rounds for better understanding of pt social issues
Checks on pt to see if he wants or needs anything
Reviews CT scan with RN for pt who was scheduled for level 1 to OR
Patient care
Provider communication
Patient care
Patient care
Down time
Patient care
Patient care
Documentation
Patient care
Documentation
Patient care
Provider communication
CategoryCode
Abbreviations: ADL, activities of daily living; AROM, active range of motion; BP, blood pressure; chucks, disposable bed pads; CT, computed tomography; dexi, Dextrostix (reagent strip for estimating blood sugar levels); drips, infusions; D rounds, multidisciplinary rounds; IADL, instrumental activities of daily liv-ing; meds, medications; NA, not applicable; OR, operating room; pt, patient; RN, nurse.
Table 3Potential mobility events during observed clinician activities
a Because of rounding, percentages do not total 100.
Mobility event category
Not possible
In bed
Out of bed
Edge of bed
Total
518 (79)
39 (6)
95 (15)
3 (< 1)
655 (100)
160 (82)
18 (9)
14 (7)
2 (1)
194 (100)
Minutes (%)aNo. (%)a

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 191
Coinciding with direct patient care are opportunities for nurse-facilitated patient mobility.
down time may be a target for increasing patient
mobility. Documentation was a major time require-
ment; nearly 20% of all time observed was devoted
to this task. Other reports of the proportion of nurses’
time spent documenting range from 7%38 to 35%.42
In 2 studies of critical care nurses, values were rela-
tively similar to ours: 24%39 and 30%.40 These results
support efforts to streamline documentation to allow
more time for direct patient care.43,44 Despite the
relative lack of down time among the nurses in our
project, we observed opportunities to facilitate
patient mobility concurrently with other tasks of
direct patient care.
During the logbook review, when searching
for potential mobility opportunities, the nursing
members of the project team repeatedly commented
that, in retrospect, mobility was possible, but not
performed, because nurses “just don’t think to do
it.” In order for nurses to think more about mobil-
ity and to facilitate mobility, a shift in culture and
behavior must occur.19,29,45-51 In a systematic review,
Coquhoun et al52 highlighted 4 key components:
identifying barriers, selecting intervention compo-
nents, using theory, and engaging end users. Direct
observation is a potentially important component
of identifying barriers and engaging end users. The
results from direct observation could be effectively
used as a starting point for discussions about the
what and when of nurse-facilitated patient mobility.
Another strategy to help detect missed mobility
opportunities could be setting specific mobility
goals for a nursing shift, facilitated by using a sim-
ple and clear mobility scale, as successfully done in
a recent randomized controlled trial.8,53,54
Our project has potential limitations. First, this
project was conducted in a single MICU in which 2
nurses and 1 clinical technician were observed by
only 1 physical therapist. Observing other providers,
at different times, in different
units or hospitals, could change
the findings. The observer also may
not have been completely objective
regarding documentation of obser-
vations in the logbook, and a dif-
ferent physical therapist or a nurse
might have differed in documen-
tation. Although qualitative evalua-
tions have this type of limitation,
they offer an important framework
for other researchers to replicate and obtain results
specific to other institutions.55 Finally, because the
potential mobility events were not actually
observed, but inferred from post hoc review of log-
books, the number of those potential mobility events
and the time required may contain measurement
error.
Conclusion We have described a process for better under-
standing the lack-of-time barrier to nurse-facilitated
Logbook observation
Table 4Examples of logbook observations of potential mobility events with assigned codes and categories
Ask pt to sit at side of bed for assessment
In-bed exercise
Have patient get out of bed to chair for oral medication
Have patient get out of bed to chair for meals
Face-to-face communication
Ambulate with patient
Help patient stand at sink in room
In-bed exercise: rolling, bridging, scooting
In-bed exercise: scooting, bridging
Assessment: lung/abdominal sounds, pain, pulses, strength by assessing resisted DF/hip flexion via heel slide, orientation questions mixed in throughout; asks pt what he would like for breakfast
Gets up to check on rm 58 who is agitated, vent alarming
Prepares to give meds to pt. Pt is mobile in bed, moves into long sitting in bed to take oral meds, RN raises HOB to support pt while pt is sitting upright. Pt returns to resting against support of bed
Breakfast arrives, sets pt up to eat in bed and takes dexi
Talks to providers about labs requested
Walk past rm 56 and pt now in chair at bedside, with assistance of son
Gives pt his toothbrush while pt seated in chair. Tech gets TB from table on opposite side of room, prepares it with water cup, gives in to pt while pt is seated in chair
BP did not record, needs retake—asks pt how he does moving around in bed
Pt asks to be boosted/moved to HOB
Edge of bed
In bed
Out of bed
Out of bed
Not possible
Out of bed
Out of bed
In bed
In bed
CategoryCode
Abbreviations: BP, blood pressure; dexi, Dextrostix (reagent strip for estimating blood sugar levels); DF, dorsiflexion; HOB, head of bed; labs, laboratory tests; meds, medications; pt, patient; rm, room; RN, nurse; TB, toothbrush; tech, technologist; vent, ventilator.

192 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
patient mobility. The design and implementation
of this process were feasible and provided valuable
insights for our quality improvement project. We
observed that nurses have relatively little available
time for additional clinical activities, but they may
miss opportunities to facilitate patient mobility as
part of existing patient care activities. Using our
observational process, other researchers can begin
to better understand barriers to nurse-facilitated
patient mobility in other clinical settings.
ACKNOWLEDGMENTThis work was performed at Johns Hopkins Hospital.
FINANCIAL DISCLOSURESDr Young was supported by the Foundation for Physical Therapy’s Center of Excellence in Physical Therapy Health Services and Health Policy Research and Training Grant. Dr Parker was supported by award 1K23HL138206-01 from the National Institutes of Health and received an honorarium for a presentation for Vizient.
SEE ALSO For more about patient mobility, visit the Critical Care Nurse website, www.ccnonline.org, and read the article by Messer et al, “Implementation of a Progressive Mobilization Program in a Medical-Surgical Intensive Care Unit” (October 2015).
REFERENCES 1. Herridge MS, Cheung AM, Tansey CM, et al; Canadian Critical
Care Trials Group. One-year outcomes in survivors of the acute respiratory distress syndrome. N Engl J Med. 2003; 348(8):683-693.
2. Herridge MS, Tansey CM, Matté A, et al; Canadian Critical Care Trials Group. Functional disability 5 years after acute respira-tory distress syndrome. N Engl J Med. 2011; 364(14): 1293-1304.
3. Mueller N, Murthy S, Tainter CR, et al. Can sarcopenia quan-tified by ultrasound of the rectus femoris muscle predict adverse outcome of surgical intensive care unit patients as well as frailty? A prospective, observational cohort study. Ann Surg. 2016;264(6):1116-1124.
4. Heyland DK, Stapleton RD, Mourtzakis M, et al. Combining nutrition and exercise to optimize survival and recovery from critical illness: conceptual and methodological issues. Clin Nutr. 2016;35(5):1196-1206.
5. Fan E, Dowdy DW, Colantuoni E, et al. Physical complications in acute lung injury survivors: a two-year longitudinal pro-spective study. Crit Care Med. 2014;42(4):849-859.
6. Dinglas VD, Aronson Friedman L, Colantuoni E, et al. Muscle weakness and 5-year survival in acute respiratory distress syndrome survivors. Crit Care Med. 2017;45(3):446-453.
7. Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically venti-lated, critically ill patients: a randomised controlled trial. Lancet. 2009;373(9678):1874-1882.
8. Schaller SJS, Anstey M, Blobner M, et al; International Early SOMS-guided Mobilization Research Initiative. Early, goal-directed mobilisation in the surgical intensive care unit: a randomised controlled trial. Lancet. 2016;388(10052):1377-1388.
9. Ruhl AP, Huang M, Colantuoni E, et al; with the National Insti-tutes of Health, National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome Network. Healthcare utilization and costs in ARDS survivors: a 1-year longitudinal national US multicenter study. Intensive Care Med. 2017;43(7):980-991.
10. Ruhl AP, Lord RK, Panek JA, et al. Health care resource use and costs of two-year survivors of acute lung injury: an observational cohort study. Ann Am Thorac Soc. 2015; 12(3): 392-401.
11. Ruhl AP, Huang M, Colantuoni E, et al. Healthcare resource use and costs in long-term survivors of acute respiratory distress syndrome: a 5-year longitudinal cohort study. Crit Care Med. 2017;45(2):196-204.
12. Hermans G, Van Mechelen H, Clerckx B, et al. Acute outcomes and 1-year mortality of intensive care unit-acquired weakness. A cohort study and propensity-matched analysis. Am J Respir Crit Care Med. 2014;190(4):410-420.
13. Hashem MD, Parker AM, Needham DM. Early mobilization and rehabilitation of patients who are critically ill. Chest. 2016; 150(3):722-731.
14. Tipping CJ, Harrold M, Holland A, Romero L, Nisbet T, Hodgson CL. The effects of active mobilisation and rehabilitation in ICU on mortality and function: a system-atic review. Intensive Care Med. 2017;43(2):171-183.
15. Wahab R, Yip NH, Chandra S, et al. The implementation of an early rehabilitation program is associated with reduced length of stay: a multi-ICU study. J Intensive Care Soc. 2016;17(1):2-11.
16. Perme C, Nalty T, Winkelman C, Kenji Nawa R, Masud F. Safety and efficacy of mobility interventions in patients with femoral catheters in the ICU: a prospective observa-tional study. Cardiopulm Phys Ther J. 2013;24(2):12-17.
17. Nydahl P, Sricharoenchai T, Chandra S, et al. Safety of patient mobilization and rehabilitation in the intensive care unit: systematic review with meta-analysis. Ann Am Thorac Soc. 2017;14(5):766-777.
18. Bailey P, Thomsen GE, Spuhler VJ, et al. Early activity is feasible and safe in respiratory failure patients. Crit Care Med. 2007;35(1):139-145.
19. Dubb R, Nydahl P, Hermes C, et al. Barriers and strategies for early mobilization of patients in intensive care units. Ann Am Thorac Soc. 2016;13(5):724-730.
20. Parry SM, Knight LD, Connolly B, et al. Factors influencing physical activity and rehabilitation in survivors of critical ill-ness: a systematic review of quantitative and qualitative studies. Intensive Care Med. 2017;43(4):531-542.
21. Sricharoenchai T, Parker AM, Zanni JM, Nelliot A, Dinglas VD, Needham DM. Safety of physical therapy interventions in critically ill patients: a single-center prospective evaluation of 1110 intensive care unit admissions. J Crit Care. 2014;29(3): 395-400.
22. Parry SM, Nydahl P, Needham DM. Implementing early physical rehabilitation and mobilisation in the ICU: institu-tional, clinician, and patient considerations [published online ahead of print August 2017]. Intensive Care Med. doi:10.1007/s00134-017-4908-8.
23. Titsworth WL, Hester J, Correia T, et al. The effect of increased mobility on morbidity in the neurointensive care unit. J Neu-rosurg. 2012;116(6):1379-1388.
24. Piva S, Dora G, Minelli C, et al. The Surgical Optimal Mobility Score predicts mortality and length of stay in an Italian pop-ulation of medical, surgical, and neurologic intensive care unit patients. J Crit Care. 2015;30(6):1251-1257.
25. Dong ZH, Yu BX, Sun YB, Fang W, Li L. Effects of early rehabili-tation therapy on patients with mechanical ventilation. World J Emerg Med. 2014;5(1):48-52.
26. Meyer MJ, Stanislaus AB, Lee J, et al. Surgical Intensive Care Unit Optimal Mobilisation Score (SOMS) trial: a proto-col for an international, multicentre, randomised controlled trial focused on goal-directed early mobilisation of surgical ICU patients. BMJ Open. 2013;3(8):e003262.
27. Sibilla A, Nydahl P, Greco N, et al. Mobilization of mechan-ically ventilated patients in Switzerland [published online ahead of print August 2017]. J Intensive Care Med. doi: 10.1177/0885066617728486.
28. Jolley SE, Moss M, Needham DM, et al. Point prevalence study of mobilization practices for acute respiratory failure patients in the United States. Crit Care Med. 2017;45(2):205-215. doi:10.1097/CCM.0000000000002058.
29. Needham DM, Korupolu R. Rehabilitation quality improvement in an intensive care unit setting: implementation of a quality improvement model. Top Stroke Rehabil. 2010;17(4):271-281.
30. Hashem MD, Nelliot A, Needham DM. Early mobilization and rehabilitation in the ICU: moving back to the future. Respir Care. 2016;61(7):971-979.
31. Pronovost PJ, Berenholtz SM, Needham DM. Translating evidence into practice: a model for large scale knowledge translation. BMJ. 2008;337(6):963-965.
32. Zanni JM, Korupolu R, Fan E, et al. Rehabilitation therapy and outcomes in acute respiratory failure: an observational pilot project. J Crit Care. 2010;25(2):254-262.
33. Anekwe DE, Koo KK-Y, de Marchie M, Goldberg P, Jayara-man D, Spahija J. Interprofessional survey of perceived barriers and facilitators to early mobilization of critically ill patients in Montreal, Canada [published online ahead

of print January 1, 2017]. J Intensive Care Med. doi: 10.1177/0885066617696846.
34. Needham DM, Korupolu R, Zanni JM, et al. Early physical medicine and rehabilitation for patients with acute respira-tory failure: a quality improvement project. Arch Phys Med Rehabil. 2010;91(4):536-542.
35. Hager DN, Dinglas VD, Subhas S, et al. Reducing deep seda-tion and delirium in acute lung injury patients: a quality improvement project. Crit Care Med. 2013;41(6):1435-1442.
36. Suri H. Purposeful sampling in qualitative research synthe-sis. Qual Res J. 2011;11(2):63-75.
37. Erlingsson C, Brysiewicz P. A hands-on guide to doingcontent analysis. Afr J Emerg Med. 2017;7(3):93-99.doi:10.1016/j.afjem.2017.08.001.
38. Westbrook JI, Duffield C, Li L, Creswick NJ. How much time do nurses have for patients? A longitudinal study quantify-ing hospital nurses’ patterns of task time distribution and interactions with health professionals. BMC Health Serv Res. 2011;11:319.
39. Douglas S, Cartmill R, Brown R, et al. The work of adultand pediatric intensive care unit nurses. Nurs Res. 2013; 62(1): 50-58.
40. Ballermann MA, Shaw NT, Mayes DC, Gibney RT, West-brook JI. Validation of the Work Observation Method By Activity Timing (WOMBAT) method of conducting time-motion observations in critical care settings: an observa-tional study. BMC Med Inform Decis Mak. 2011;11(1):32.
41. Farquharson B, Bell C, Johnston D, et al. Frequency of nursing tasks in medical and surgical wards. J Nurs Manag. 2013;21(6):860-866.
42. Hendrich A, Chow MP, Skierczynski BA, Lu Z. A 36-hospital time and motion study: how do medical-surgical nurses spend their time? Perm J. 2008;12(3):25-34. http://www.ncbi.nlm.nih.gov/pubmed/21331207. Accessed February 6, 2018.
43. Freeman R, Maley K. Mobilization of intensive care cardiac surgery patients on mechanical circulatory support. Crit CareNurs Q. 2013;36(1):73-88.
44. Cheevakasemsook A, Chapman Y, Francis K, Davies C. The study of nursing documentation complexities. Int J Nurs Pract. 2006;12(6):366-374.
45. Parker AM, Sricharoenchai T, Needham DM. Early rehabilita-tion in the intensive care unit: preventing impairment of physical and mental health. Curr Phys Med Rehabil Rep.2013;1(4):307-314.
46. Drolet A, DeJuilio P, Harkless S, et al. Move to improve: the feasibility of using an early mobility protocol to increase ambulation in the intensive and intermediate care settings. Phys Ther. 2013;93(2):197-207.
47. Engel HJ, Needham DM, Morris PE, Gropper MA. ICU early mobilization: from recommendation to implementation at three medical centers. Crit Care Med. 2013;41(9)(suppl 1): S69-S80.
48. Hopkins RO, Spuhler VJ, Thomsen GE. Transforming ICU cul-ture to facilitate early mobility. Crit Care Clin. 2007; 23(1): 81-96.
49. Cameron S, Ball I, Cepinskas G, et al. Early mobilization in the critical care unit: a review of adult and pediatric litera-ture. J Crit Care. 2015;30(4):664-672.
50. Hester JM, Guin PR, Danek GD, et al. The economic and clini-cal impact of sustained use of a progressive mobility program in a neuro-ICU. Crit Care Med. 2017;45(6):1037-1044.
51. Messer A, Comer L, Forst S. Implementation of a progres-sive mobilization program in a medical-surgical intensive care unit. Crit Care Nurse. 2015;35(5):28-42.
52. Colquhoun HL, Squires JE, Kolehmainen N, Fraser C, Grim-shaw JM. Methods for designing interventions to change healthcare professionals’ behaviour: a systematic review. Implement Sci. 2017;12(1):30.
53. Hodgson CL, Bailey M, Bellomo R, et al; Trial of Early Activ-ity and Mobilization Study Investigators. A binational multi-center pilot feasibility randomized controlled trial of early goal-directed mobilization in the ICU. Crit Care Med. 2016; 44(6):1145-1152.
54. Tipping CJ, Bailey MJ, Bellomo R, et al. The ICU MobilityScale has construct and predictive validity and is respon-sive: a multicenter observational study. Ann Am Thorac Soc. 2016;13(6):887-893.
55. Portela MC, Pronovost PJ, Woodcock T, Carter P, Dixon-Woods M. How to study improvement interventions: a brief overview of possible study types. BMJ Qual Saf. 2015; 24(5):325-336.
To purchase electronic or print reprints, contact American Association of Critical-Care Nurses, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; email, [email protected].
TemporalScanner™
The Exergen TemporalScanner Temporal Artery Thermometer
More than 70 published studies - supporting accuracy from preemies to geriatrics in all areas of care.
• Patients love the TemporalScanner!
• Cost savings of 90% over other thermometry methods
• Lifetime Warranty – unique to thermometry
• Chemical resistant materials stand up to harsh disinfectants
• On-demand, innovative, inservicing results in successful usage for all levels of nursing skills
To evaluate, email: [email protected]
For general information: www.exergen.com
For clinical information, visit: www.TAThermometry.org
For educational videos, clinical studies, and manuals: www.exergen.com/ww
Exergen Corporation 400 Pleasant Street Watertown MA 02472 Tel 617-923-9900 Fax 617-923-9911
www.exergen.com/s
Invented, designed, assembled, tested, & packaged in the U.S.A. by Exergen

Early Mobility in Critical Care
©2018 American Association of Critical-Care Nursesdoi:https://doi.org/10.4037/ajcc2018193
Background Mobilization is safe and associated with improved outcomes in critically ill adults, but little is known about mobilization of critically ill children. Objective To implement a standardized mobilization therapy protocol in a pediatric intensive care unit and improve mobilization of patients.Methods A goal-directed mobilization protocol was instituted as a quality improvement project in a 20-bed cardiac and medical-surgical pediatric intensive care unit within an academic tertiary care center. The mobilization goal was based on age and severity of illness. Data on severity of illness, ordered activity limitations, baseline functioning, mobilization level, complications of mobili-zation, and mobilization barriers were collected. Goal mobilization was defined as a ratio of mobilization level to severity of illness of 1 or greater.Results In 9 months, 567 patient encounters were ana-lyzed, 294 (52%) of which achieved goal mobilization. The mean ratio of mobilization level to severity of illness improved slightly but nonsignificantly. Encounters that met mobilization goals were in younger (P = .04) and more ill (P < .001) patients and were less likely to have barriers (P < .001) than encounters not meeting the goals. Compli-cation rate was 2.5%, with no difference between groups (P = .18). No serious adverse events occurred.Conclusions A multidisciplinary, multiprofessional, goal-directed mobilization protocol achieved goal mobilization in more than 50% of patients in this pediatric intensive care unit. Undermobilized patients were older, less ill, and more likely to have mobilization barriers at the patient and provider level. (American Journal of Critical Care. 2018; 27:194-203)
MOBILIZATION THERAPY IN THE PEDIATRIC
INTENSIVE CARE UNIT: A MULTIDISCIPLINARY QUALITY
IMPROVEMENT INITIATIVEBy Blair R. L. Colwell, MD, Cydni N. Williams, MD, Serena P. Kelly, CPNP-AC, and Laura M. Ibsen, MD
1.0 HourC EThis article has been designated for CE contact
hour(s). See more CE information at the end of
this article.
This article is followed by an AJCC Patient Care Page on page 204.
194 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org

Mobilization therapy is safe and beneficial in critically ill adults and is associated with decreased length of stay, improved physical function at discharge, and reduced hospital costs,1,2 but little is known about mobilization therapies in the pediatric intensive care unit (PICU). The definition of mobilization therapy and the timing of mobilization vary widely in the literature.3-5 Mobilization
therapy in the intensive care unit (ICU) is rehabilitating physical activity that escalates from passive range of motion exercises to standing and walking.
A variety of adverse effects, including ICU-
acquired weakness, delirium, and poor quality of
life and functional outcomes, have been associated
with adult ICU admission6 and are supported in
limited pediatric studies.7-11 Functional impairment
may persist in children after PICU admission, with
up to one-third of children displaying impairment
upon discharge and up to 13% showing
impairment at 2-year follow-up.12 Studies in
adults have shown that mobilization therapy may
mitigate some of these long-term adverse effects of
ICU admission. A recent prospective quality
improvement (QI) study in a tertiary PICU by
Wieczorek et al13 demonstrated that implementa-
tion of a mobilization bundle in children admitted for
more than 3 days doubled the frequency of mobili-
zation events and was safe; the main barrier to
mobilization was a lack of appropriate equipment.
Another study showed that about half of children
admitted to a PICU in Canada received some type of
physical therapy.14 A survey of pediatric critical care
physicians and physical therapists in Canada
showed that most clinicians believe mobilization is
important but that a major barrier to early mobili-
zation is lack of established guidelines, in addi-
tion to safety concerns and lack of physician orders
for mobilization.4 After the implementation of a
nurse-led, progressive early mobilization protocol (in
conjunction with a delirium bundle and sedation
protocol) in a mixed PICU, the prevalence of delirium
dropped from 19% to 12%.15 Because of improvements
in outcomes in adult ICU patients who receive
mobilization therapy, we developed a mobilization
protocol designed to improve PICU patient care
through nurse-driven mobilization interventions.
We implemented a unique goal-directed multi-
disciplinary and multiprofessional mobilization
protocol for critically ill infants and children admit-
ted to the PICU. Our pro-
tocol defined a minimum
goal for mobility, with
adjusted goals based on
patients' severity of illness
(SOI) and age. We tailored
mobilization activities on
the basis of minimum
goals to be completed
primarily by the bedside
nurse. We tracked proto-
col adherence, adverse events, and perceived barriers
to goal mobilization. In this article, we report our
preliminary experience with a focus on safety and
identifying areas to target for continued improve-
ment in mobilizing critically ill children.
Methods Ethical Issues
We implemented this project as a QI protocol
that applied to all PICU patients and designed it to
improve patient care by standardization of mobility
practices without comparison to other interventions.
It was therefore exempt from institutional review
board approval. Dissemination of results was also
deemed exempt. We tracked adverse events closely
to ensure that no additional patient risk occurred as
a result of practice change.
SettingOur hospital is an urban, academic tertiary care
children’s hospital and a referral center for several
states. The PICU has 20 beds and is a combined
About the AuthorsBlair R. L. Colwell is a pediatric critical care physician at University of California Davis, Sacramento, California. Cydni N. Williams is an assistant professor of pediatrics at Oregon Health and Science University, Portland, Oregon. Serena P. Kelly is an assistant professor of pediatrics at Oregon Health and Science University. Laura M. Ibsen is a professor of pediatrics and anesthesiology at Oregon Health and Science University.
Corresponding author: Blair R. L. Colwell, MD, University of California Davis, Department of Pediatrics, Division of Critical Care, 2516 Stockton Blvd, Sacramento, CA 95817 (email: [email protected]).
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 195
A goal-directed multidis-ciplinary mobilization protocol for critically ill infants and children was implemented in a PICU.

196 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
cardiac and medical-surgical unit with a typical
nurse to patient ratio of 1 to 1 or 1 to 2. There are
approximately 1300 admissions and approximately
200 cardiac surgery cases per year. The PICU uses
nurse-driven sedation protocols for most intubated
patients, as published in the RESTORE (Randomized
Evaluation of Sedation Titration for Respiratory Fail-
ure) trial.16 Physical and occupational therapists are
available for consultation in our PICU 8 hours per
day (9 AM to 5 PM), 6 days per week. Before implemen-
tation of the goal-directed mobilization protocol,
no guidelines were in place for initiation of rehabili-
tation or physical or occupational therapy in the
PICU, and mobilization practices depended on care
providers and bedside nurses.
Planning the InterventionWe first conducted a survey of nursing staff in
the PICU, focusing on perceptions of and barriers
to mobilization. The most significant preimple-
mentation barriers were perception of physiologic
instability and lack of additional staff to help with
mobilization activities. We formed a multidisci-
plinary, multiprofessional group including bedside
nurses, a PICU nurse practitioner, nursing leaders,
PICU physicians, and physical, occupational, and
respiratory therapists, and we created a goal-directed
mobilization protocol. Goal minimum mobilization
was based on age and SOI (Table 1). The protocol
applied to all PICU patients upon admission, includ-
ing patients supported by vasoactive infusions, inva-
sive respiratory support, and extracorporeal membrane
oxygenation, but it did not supersede practitioner-
ordered activity limitations. To simplify the protocol,
we did not specifically address patients with primary
neurologic disease (eg, elevated intracranial pressure).
However, these patients have activity orders in place
to limit elevations in intracranial pressure. Addition-
ally, children with developmental delays are addressed
in the special considerations section of the protocol
(see Appendix).
The protocol was embedded into the electronic
medical record's admission order sets and was also
available as a stand-alone order, allowing the
Description
Age 0-12 months
1-4 years
>4 years
Mobilization level
No invasive respi-ratory or inotro-pic support
Add:Up to chair, seat,
or swing 2-3 times per day; floor time
Add:Sit in chair; stand
side of bed; ambulate 3 times per day
Add:Sit in chair; stand
side of bed; ambulate 3 times per day
4
PEEP < 10 cm H2O, FIO2 < 60%, stable dopamine < 10 μg/kg/min
Add:Parent hold in chair; active
positioning; up to chair, seat, or swing
Add:Sit on edge of bed, in
chair, or in pediatric positioning chair; twice daily ambulation; con-sider physical and/or occupational therapy consultation
Add:Sit on edge of bed, in
large pediatric position-ing chair, or cardiac chair; active assist with transfer; twice daily ambulation; consider physical and/or occupational therapy consultation
3
PEEP 10 cm H2O, dopamine 10 μg/kg/min, any epinephrine or norepinephrine
Add:Active range of motion; use of
bumper or nesting for supported flexion, supine, side-lying, and prone positioning; use of towel roll to support hip flexion
Add:Active range of motion; supine,
side-lying, and prone positioning; use of towel roll to support hip flexion; resting hand/foot splints if prolonged intubation
Add:Active range of motion; supine,
side-lying, and prone positioning; use of towel roll to support hip flexion; resting hand/foot splints if prolonged intubation
2
Vital sign lability requiring titration of interventions
Turn; gentle passive range of motion of all 4 extrem-ities and neck; alternate position of ventilator tubing
Turn; gentle passive range of motion of all 4 extrem-ities and neck; alternate position of ventilator tub-ing; float heels
Turn; gentle passive range of motion of all 4 extrem-ities and neck; alternate position of ventilator tub-ing; float heels
1
4: Most stable3: Stable2: Somewhat unstable1: Very unstable
Abbreviations: FIO2, fraction of inspired oxygen; PEEP, positive end-expiratory pressure. a For long-stay, chronically critically ill patients, consider more active exercise when still in acute phase of illness, as tolerated (see Appendix).
Severity of illness
Feature
Table 1Goal-directed mobilization protocola

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 197
Goal minimum mobiliza-tion was based on age and severity of illness for all PICU patients.
protocol to be initiated on the first hospital day
and continue throughout PICU hospitalization.
Mobilization activities could be initiated immedi-
ately after arrival in the PICU because most activi-
ties were structured to be performed by the bedside
nurse with or without additional support staff. A
laminated copy of the protocol was placed at each
patient’s bedside for review by staff as necessary.
An additional order for supplemental support from
a respiratory therapist could also be placed to allow
for extra support personnel when mobilizing intu-
bated patients.
We educated all PICU staff regarding the safety
and importance of mobilization therapy by presen-
tations on educational days, access to references,
and email updates. Attending physicians on service
in the PICU conducted biweekly rounds with bed-
side nurses to collect data on all patients and solicit
perceived barriers to mobilization (as reported by
bedside nurses). A multiprofessional team conducted
additional “mobilization rounds” on weekday
mornings. During these rounds, the charge nurse,
PICU nurse practitioner, and physical, occupational,
and respiratory therapists discussed each patient.
Discussion during mobilization rounds allowed
appropriate allocation of staff and facilitated earlier
mobilization by identifying patients who might
benefit from the assistance of additional support
staff, such as physical, occupational, or respiratory
therapists or a more experienced additional bed-
side nurse, to achieve mobilization goals.
Planning the Study of the InterventionWe chose protocol adherence as the primary
outcome because there is no gold standard for type
or timing of mobilization therapy in pediatric patients.
We quantified protocol adherence as a mobilization
ratio (level of mobilization to SOI) using the defini-
tions contained in Table 1. A ratio of 1 or greater
defined protocol adherence. Secondary outcome
measures included adverse events and barriers to
mobilization. We grouped perceived barriers to
mobilization by category. We defined serious adverse
events as desaturation requiring escalation of ther-
apy, unplanned extubation, removal of other medi-
cal equipment (eg, arterial catheter, central venous
catheter), and falls. We included all children admit-
ted to the PICU, and we excluded adult patients who
were boarding in the PICU solely for management
of extracorporeal membrane oxygenation because
these patients were primarily cared for by other
services. We ensured data accuracy by having only
PICU attending physicians collect data.
Methods of EvaluationData collection began in August 2014 and
included patients' age, SOI level from 1 to 4 (with
1 indicating the most ill patients), ordered activity
limitations, preadmission pediatric overall perfor-
mance category, mobilization level from 1 to 4 (see
Table 1), and complications of and barriers to mobi-
lization. Attending physicians collected data in real
time during biweekly rounds with bedside nurses.
We tracked the mean mobilization ratio every 2
weeks from all included encounters (defined as
admissions during time points at which data were
collected) and reviewed progress at monthly QI
meetings. We also reviewed adverse events, the data
collection process, and barriers to mobilization at
monthly meetings. We distributed summaries from
monthly meetings to all PICU staff to relay the cur-
rent status of the mobilization project and to pro-
mote continued improvement.
AnalysisThe first 3 months of data defined the implemen-
tation period. We used standard statistical process
control charts to plot mean mobilization ratio over
time and the proportion of patients not adherent to
the protocol (mobilization ratio < 1) over time to
account for skew related to
mobilization ratios greater
than 1 when calculating
means. Three limits were
used to set the upper and
lower control limits. Some
patients were present during
multiple data collection
encounters, but because the
primary outcome was adherence to the mobiliza-
tion protocol within the PICU, we analyzed data by
encounter and not by individual patient. Continuous
variables were reported as medians with interquartile
ranges; categorical variables, as counts with percent-
ages. We used the Mann-Whitney U (continuous)
and 2 (categorical) tests to compare variables
between encounters achieving goal mobilization
(mobilization ratio ≥1) and encounters not achiev-
ing goal mobilization (mobilization ratio <1). We
analyzed the data by using statistics software (SPSS
version 22, IBM, and Minitab 16.2.4, Minitab Inc).
Results During the first 9 months, we analyzed 567
encounters. We designated the initial 3 months as
the implementation period, during which the roll-
out of the protocol occurred with extensive staff

198 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
education. We designated the following 6 months
as the postintervention period. The implementation
and postintervention period populations are com-
pared in Table 2. Patients in the implementation
period were less ill (SOI, 3-4) than patients in the
postintervention period (P = .009) but were otherwise
similar. Notably, 18% of patients in the postinter-
vention period were classified as SOI 1 to 2 (intu-
bated with positive end-expiratory pressure ≥ 10 cm
H2O and/or receiving moderate amounts of vasoac-
tive infusions).
Of the 567 encounters, 294 (52%) achieved
the goal mobilization ratio (level of mobilization
to SOI ratio of ≥ 1). Figure 1 displays the study’s
mean mobilization ratio over time. The mean mobi-
lization ratio was slightly higher in the postinterven-
tion period (0.86) than in the implementation period
(0.84), but this difference was not statistically signif-
icant. The proportion of encounters meeting mobili-
zation goals remained stable over time (Figure 2).
In the postintervention period, some patients were
able to mobilize well beyond their minimum goals,
skewing some data points toward a higher mean
mobilization ratio. For instance, some patients ven-
tilated on high positive end-expiratory pressure
(> 10 cm H2O) were able to walk. This variability
accounts for the small increase in the postintervention
mean mobilization ratio among a stable proportion
of patients meeting mobilization goals.
Comparing goal-mobilized versus undermobi-
lized encounters revealed improved adherence to
mobilization goals in patients who were younger
(P = .04), more ill (P < .001), and less likely to have
barriers (P < .001) than in patients not meeting mobi-
lization goals, as displayed in Table 3. The compli-
cation rate was 2.5% (n = 14), with no difference
between groups (P = .18, Table 3). No complications
prevented mobility activities. Transient desatura-
tion was the most common complication (Table 4).
Characteristic of patients
Table 2Implementation versus postintervention period
Age, median (IQR), y
Pediatric overall performance category, No. (%)
Normal/mild disability Moderate disability or worse
Severity of illness, No. (%) Most ill (level 1-2) Less ill (level 3-4)
.94
.35
.009
1.3 (0.3-9.4)
291 (67)143 (33)
77 (18)357 (82)
2.5 (0.4-9.1)
83 (62)50 (38)
11 (8)122 (92)
P valuePostintervention period (n = 434)
Implementation period (n = 133)
Abbreviation: IQR, interquartile range.
Figure 1 Mean mobilization ratios (level of mobilization to severity of illness) of all encounters during the 3-month implementation period and the 6-month postintervention period. A mean value of 1 or greater on the y-axis describes a patient meeting the minimum mobilization goal. The mean mobilization ratio over time was 0.86 (represented by the horizontal green line). Data points represent 2-week intervals. The process remained in control during the study period.
Abbreviations: LCL, lower control limit; UCL, upper control limit.
Implementation
Implementation
1.0
0.9
0.8
0.7
0.6
0.20
0.15
0.10
0.00
0.05
1
1
4
4
7
7
10
10
13
13
16
16
19
19
22
22
25
25
28
28
LCL = 0.7279
LCL = 0
UCL = 1.0016
UCL = 0.1681
Mean = 0.8648
Mean = 0.0514
Ind
ivid
ual
val
ue
Mo
vin
g r
ang
e
Observation number
Observation number
Postintervention
Postintervention

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 199
No serious adverse events, such as hemodynamic
instability or unintended extubation, occurred. Bed-
side nursing staff identified barriers in 104 encoun-
ters not achieving goal mobilization. These barriers
are displayed in Table 5.
Discussion We implemented a unique multidisciplinary
and multiprofessional goal-directed mobilization
protocol based on SOI and age in our PICU as a
QI initiative, achieving goal mobilization in more
than 50% of encounters. The mean mobilization
ratio improved over time as staff seemed to become
more comfortable mobilizing the most critically ill
patients, although this improvement was not statis-
tically significant. However, we continue to have a
proportion of patients, mostly older and less ill,
who do not achieve the minimum mobilization
goals, most likely because of the increasing mobili-
zation requirements needed to achieve goal levels
in these children. The protocol was safe during this
period of preliminary implementation, with no seri-
ous adverse events even in the most severely ill
patients. We identified potentially modifiable bar-
riers to mobilization, including parent and patient
refusal. In addition, we found that staff sometimes
perceived patients to be too physiologically unsta-
ble for mobilization and that patients' families per-
ceived medical equipment to be a barrier. This study
was a collaborative effort among multidisciplinary
Figure 2 Proportion of encounters not achieving minimum mobility goals (on y-axis) during the 3-month implementa-tion period and the 6-month postintervention period. The mean proportion of patients not achieving the minimum mobility goal was 0.52 (represented by the horizontal green line). Data points represent 2-week intervals. The process remained in control during the study period.
Abbreviations: LCL, lower control limit; UCL, upper control limit.
Implementation
1 4 7 10 13 16 19 22 25 28
LCL = 0.358
UCL = 0.691
Mean = 0.525
Observation number
Postintervention
1.0
0.6
0.8
0.4
0.2
0.0
Pro
po
rtio
n
Characteristic of patients
Table 3Goal-mobilized versus undermobilized encounters
Age, median (IQR), y
Pediatric overall performance category, No. (%)
Normal/mild disability Moderate disability or worse
Severity of illness, No. (%) Most ill (level 1-2) Less ill (level 3-4)
Complications, No. (%)
Perceived barriers, No. (%)
.04
.86
< .001
.18
< .001
2.6 (0.5-9.1)
179 (66) 94 (34)
19 (7)254 (93)
4 (1)
139 (51)
1.1 (0.4-9.6)
195 (66) 99 (34)
69 (23)225 (77)
10 (3)
85 (29)
P valueUndermobilized
(n = 273)Goal-mobilizeda
(n = 294)
Abbreviation: IQR, interquartile range.a Mobilization ratio 1.

200 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
Goal mobilization was achieved in
52% of encounters.
providers in the PICU and resulted in a novel
goal-directed mobilization protocol.
PICU mobilization protocols are innovative;
however, few studies on this topic are available.
A recent report showed that implementation of a
mobilization bundle for children in a tertiary PICU
led to a significant increase in mobilization events,
although the study included only 100 postimple-
mentation patients admitted to the PICU for more
than 3 days.13 Our study was larger and included all
admissions but similarly showed improvement in
mobilization activities and no serious adverse events.
Choong et al14 noted that early mobilization within
48 hours of admission occurred in only 9.5% of
patients and was more common
in older patients. In contrast, our
results demonstrate a goal mobiliza-
tion of 52% of patients and easier
mobilization of younger children,
possibly because of our specific
age-based protocol goals and a
primarily nurse-driven protocol. Choong et al did
not use a mobilization protocol, which most likely
accounts for the higher proportion of patients
mobilized in our study. We chose to describe our
protocol as a goal-directed protocol rather than as
an early mobilization protocol, although the dis-
tinction is unclear in the literature, and timing of
mobilization activities in the 2 studies may account
for some differences.
The incidence of adverse events during early
mobilization in adult patients varies from 0% to
4% of all mobilization sessions.3,17-20 Studies in
children also support a very low rate of adverse
events,13,21,22 consistent with the 2.5% rate of adverse
events in our study. We were able to track adverse
events in a prospective manner, which most likely
allowed us to accurately estimate the number of
adverse events because mild events may be missed
during retrospective chart review. The most common
complications in our study were transient desaturation
and tachypnea (93% of all adverse events), similar
to studies of adults in which approximately half of
all adverse events were respiratory complications.23
Studies in adults have shown that barriers to
mobilization therapy are multifaceted and include
unit culture, perceived lack of resources, and factors
intrinsic to patients.24 Pediatric barriers to mobiliza-
tion therapy may include institutional barriers, such
as the absence of practice guidelines or an order for
mobilization, in addition to unit culture, safety, and
resource concerns.4,13,22 Our data indicate that disease
severity (or the perception thereof) represents a sub-
stantial barrier to mobilization, as this accounted
for almost half of identified barriers in our study.
In addition, a substantial number of patients or
their families refused to participate, providing a new
target to improve mobilization in our unit. Interest-
ingly, nurse refusal was not identified as a barrier in
our study, in contrast to a study by Cui et al22 in
which nurses deferred physical or occupational ther-
apy sessions in 50% of cases. This finding suggests
that the mobilization protocol was well received
by the bedside nursing staff in our study. Medical
equipment barriers, such as access to wheelchairs at
home, were also identified as potentially modifiable
barriers to mobilization. Notably, lack of an order to
proceed with mobilization and lack of practice
guidelines were not barriers in our study because
strategies to overcome institutional barriers were
built into this QI project. Because we collected our
data in real time, our study most likely reveals more
barriers to mobilization than did the study by
Wieczorek et al,13 which identified barriers only
through a retrospective chart review.
Our study has several limitations, including
implementation in a single setting and lack of
assessment of outcome measures because the pri-
mary goals were protocol adherence and safety
monitoring. The preliminary data are underpow-
ered to detect changes in important outcomes such
as incidence of delirium, duration of mechanical
respiratory support, and length of stay. We adjusted
the mobilization protocol on the basis of SOI pri-
marily according to patients’ respiratory and cardio-
vascular requirements by administering invasive
Complication
Table 4Complications among all encounters during mobilization therapy
Transient desaturation
Tachypnea
Emesis
11 (79)
2 (14)
1 (7)
No. (%) of 14 complications
Barrier
Table 5Barriers among patients not achieving minimum mobilization goals
Diagnosis or severity-of-illness concerns
Medical equipment–related concerns
Parent’s refusal
Patient’s refusal
Timing of admission
48 (47)
31 (30)
10 (10)
3 (3)
11 (11)
No. (%) of 103 encounters

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 201
mechanical ventilation and vasoactive infusions as
needed. However, the protocol did not specifically
address patients with primary neurological disease.
Although the protocol applied to all patients with
neurological disease, orders for management of ele-
vated intracranial pressure and spinal precautions
superseded the protocol. The omission of neuro-
logical criteria was intended to simplify the proto-
col and is a limitation of the study. Patients with
primary neurological disease can be challenging to
mobilize, which could have contributed to the
inability of some patients to adhere to the mobiliza-
tion protocol and meet mobilization goals, thereby
decreasing the mean mobilization ratio. We plan to
modify the protocol for this population of patients
by including active management of elevated intra-
cranial pressure in SOI category 1.
We chose to analyze data by the mean mobili-
zation ratio instead of analyzing the number of
mobilization activities per patient to set a minimum
mobilization goal for our patients. By choosing this
strategy, we aimed to have each patient meet a spe-
cific mobilization goal and to identify barriers to
early mobilization at the individual patient level.
We analyzed data by encounter, not by individual
patient. Therefore, some patients were counted mul-
tiple times in the data set, potentially causing P val-
ues to be falsely elevated or skewing the mean
mobilization ratio over time.
As this QI project continues, we are targeting
patients who are older and less critically ill for
improved adherence to the mobilization protocol.
We are also making efforts to ensure the availabil-
ity of equipment needed to mobilize patients,
such as encouraging parents to bring wheelchairs
from home upon hospital admission. We are cur-
rently surveying families to better understand
their response to mobilization, hoping to learn
how we can decrease parents' and patients' refusal
of mobilization therapies. In the future, we intend
to collect data on outcome measures such as length
of stay, duration of mechanical ventilation, and
incidence of delirium.
Conclusions Implementation of a novel multidisciplinary
and multiprofessional goal-directed mobilization
protocol adjusted for patients' age and SOI as a QI
initiative has improved patient mobility in children
admitted to our PICU. We have observed no serious
adverse events related to our protocol. During this
preliminary period, we identified barriers at both
the patient and staff levels to target for future
improvements, and we seek to improve protocol
adherence with ongoing educational interventions.
Appendix: Special Considerations of Goal-Directed Mobilization ProtocolFractures
Pelvic fractures • Range of motion as tolerated to 90° of hip flexionAcetabular fractures • Range of motion through functional mobility, no
repetitive range of motionIntramedullary nailing of lower extremity fractures • Range of motion as toleratedUpper extremity fractures • Require orthopedic clarification for range of motion
restrictions
BracesCervical collar • Follow cervical spine precautions Cervical thoracic orthosis • Follow cervical and thoracic spine precautionsThoracolumbosacral orthosis • Follow lumbar spine precautions Knee immobilizer • Ankle and hip range of motion only Hinged knee brace • Range of motion within locked parameters of brace
Spines Not ClearedCollar or braces must be worn at all times unless
otherwise ordered.Cervical spine precautions • Logroll to sitting position: Do not let them sit
straight up • Avoid neck rotation • No shoulder range of motion greater than 90° • No lifting elbow above shoulders • No lifting, pushing, pulling, or carrying more
than 5 pounds (2.25 kg) • Do not use walker or crutches to assist with
ambulation or transfersThoracic spine precautions • Logroll: No twisting or bending • No lifting, pushing, pulling, or carrying more
than 5 pounds (2.25 kg) • No head-of-bed elevation greater than 30°
(unless brace is on or otherwise indicated) • If upper thoracic injury, avoid repetitive overhead
activitiesLumbar spine precautions • Logroll: No twisting or bending • No excessive hip flexion
Spines ClearedAll activities acceptable unless otherwise specifically
orderedSpinal Fusion
Logroll, side-lie, sitNo lifting, pushing, pulling, or carrying more than 5
pounds (2.25 kg)No twisting or bendingAvoid lengthy overhead activity
CraniotomyNo head below heartAvoid anything that will increase intracranial pressure,
for example

202 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
• Stifling a sneeze • Plugging nose to “pop” ears • Holding breath • Lifting anything heavier than 10 pounds (4.5 kg)
Bone Flap OutHelmet must be worn with • Edge-of-bed or out-of-bed activity • Head-of-bed elevation greater than 30° • During transportNo head below heart No lifting, pushing, pulling, or carrying more than 5
pounds (2.25 kg)Sternal Precautions
Logroll, side-lie, sitNo lifting, pushing, pulling, or carrying more than 5
pounds (2.25 kg)No pushing up with arms to get out of bed/chairNo twisting or bendingNo shoulder range of motion greater than 90°No lifting from under shouldersScoop patient
Cardiac PrecautionsWarm up and cool down: • For at least 2 minutes • Before and after any change of position • Ankle pumps/hand squeezesNo head below heart No bending down
Abdominal Surgery PrecautionsLogroll, side-lie, sitNo lifting, pushing, pulling, or carrying more than 5
pounds (2.25 kg)Avoid Valsalva maneuver and bearing down
Developmental DelayHave parents bring patient’s personal equipment, for
example, wheelchair, chair, etcIncorporate home occupational/physical therapy
regimen if possibleChronically Critically Ill Patients (Length of Stay > 7 Days)
Consider more active exercise program to avoid critical illness myopathy
Use sedation/muscle relaxation holds to encourage activity as tolerated
Exercise upper and/or lower extremities as catheters,
wires, tubes, etc allow
ACKNOWLEDGMENTSWe sincerely thank all the physicians, nurses, and respir a-tory, physical, and occupational therapists for their help.
FINANCIAL DISCLOSURESDr Williams is supported by grant number K12HS022981 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.
SEE ALSO For more about mobilization of patients, visit the Critical Care Nurse website, www.ccnonline.org, and read the article by Messer et al, “Implementation of a Progressive Mobilization Program in a Medical-Surgical Intensive Care Unit” (October 2015).
REFERENCES
1. Adler J, Malone D. Early mobilization in the intensive care unit: a systematic review. Cardiopulm Phys Ther J. 2012; 23(1):5-13.
2. Cameron S, Ball I, Cepinskas G, et al. Early mobilization in the critical care unit: a review of adult and pediatric literature. J Crit Care. 2015;30(4):664-672.
3. Bailey P, Thomsen GE, Spuhler VJ, et al. Early activity is feasible and safe in respiratory failure patients. Crit Care Med. 2007;35(1):139-145.
4. Choong K, Koo KK, Clark H, et al. Early mobilization in critically ill children: a survey of Canadian practice. Crit Care Med. 2013;41(7):1745-1753.
5. Kayambu G, Boots R, Paratz J. Physical therapy for the critically ill in the ICU: a systematic review and meta-analysis. Crit Care Med. 2013;41(6):1543-1554.
6. Herridge MS, Cheung AM, Tansey CM, et al; Canadian Critical Care Trials Group. One-year outcomes in survivors of the acute respiratory distress syndrome. N Engl J Med. 2003;3 48(8):683-693.
7. Choong K, Al-Harbi S, Siu K, et al; Canadian Critical Care Trials Group. Functional recovery following critical illness in children: the “wee-cover” pilot study. Pediatr Crit Care Med. 2015;16(4):310-318.
8. Daoud A, Duff JP, Joffe AR; Alberta Sepsis Network. Diagnostic accuracy of delirium diagnosis in pediatric intensive care: a systematic review. Crit Care. 2014;18(5):489.
9. Field-Ridley A, Dharmar M, Steinhorn D, McDonald C, Marcin JP. ICU-acquired weakness is associated with differences in clinical outcomes in critically ill children. Pediatr Crit Care Med. 2016;17(1):53-57.
10. Silver G, Traube C, Kearney J, et al. Detecting pediatric delirium: development of a rapid observational assessment tool. Intensive Care Med. 2012;38(6):1025-1031.
11. Wieczorek B, Burke C, Al-Harbi A, Kudchadkar SR. Early mobilization in the pediatric intensive care unit: a systematic review. J Pediatr Intensive Care. 2015;2015:129-170.
12. Ong C, Lee JH, Leow MK, Puthucheary ZA. Functional outcomes and physical impairments in pediatric critical care survivors: a scoping review. Pediatr Crit Care Med. 2016;17(5):e247-259.
13. Wieczorek B, Ascenzi J, Kim Y, et al. PICU up!: impact of a quality improvement intervention to promote early mobi-lization in critically ill children. Pediatr Crit Care Med. 2016; 17(12):e559-566.
14. Choong K, Foster G, Fraser DD, et al; Canadian Critical Care Trials Group. Acute rehabilitation practices in critically ill children: a multicenter study. Pediatr Crit Care Med. 2014; 15(6):e270-279.
15. Simone S, Edwards S, Lardieri A, et al. Implementation of an ICU bundle: an interprofessional quality improvement project to enhance delirium management and monitor delirium prevalence in a single PICU. Pediatr Crit Care Med. 2017;18(6):531-540.
16. Curley MA, Wypij D, Watson RS, et al; RESTORE Study Investigators and the Pediatric Acute Lung Injury and Sep-sis Investigators Network. Protocolized sedation vs usual care in pediatric patients mechanically ventilated for acute respiratory failure: a randomized clinical trial. JAMA. 2015;313(4):379-389.
17. Bourdin G, Barbier J, Burle JF, et al. The feasibility of early physical activity in intensive care unit patients: a prospec-tive observational one-center study. Respir Care. 2010; 55(4):400-407.
18. Sricharoenchai T, Parker AM, Zanni JM, Nelliot A, Dinglas VD, Needham DM. Safety of physical therapy interventions in critically ill patients: a single-center prospective evalua-tion of 1110 intensive care unit admissions. J Crit Care. 2014; 29(3):395-400.
19. Burtin C, Clerckx B, Robbeets C, et al. Early exercise in criti-cally ill patients enhances short-term functional recovery. Crit Care Med. 2009;37(9):2499-2505.
20. Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet. 2009;373(9678):1874-1882.

21. Abdulsatar F, Walker RG, Timmons BW, Choong K. “Wii-hab” in critically ill children: a pilot trial. J Pediatr Rehabil Med. 2013;6(4):193-204.
22. Cui LR, LaPorte M, Civitello M, et al. Physical and occupational therapy utilization in a pediatric intensive care unit. J Crit Care. 2017;40:15-20.
23. Nydahl P, Ewers A, Brodda D. Complications related to early mobilization of mechanically ventilated patients on intensive care units [published online November 7, 2014]. Nurs Crit Care. 2016;21(6):323-333. doi:10.1111/nicc.12134.
1.0 Hour Category AC E Notice to CE enrollees:
This article has been designated for CE contact hour(s). The evaluation demonstrates your knowledge of the
following objectives:
1. Collaborate to implement a multiprofessional and multidisciplinary quality improvement project.
2. Design a protocol for early mobilization of PICU patients.
3. Identify barriers to early mobilization in critically ill pediatric patients.
To complete the evaluation for CE contact hour(s) for this article #A1827031, visit www.ajcconline.org and
click the “CE Articles” button. No CE evaluation fee for AACN members. This expires on May 1, 2021.
The American Association of Critical-Care Nurses is an accredited provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. AACN has been approved as a provider of continuing education in nursing by the State Boards of Registered Nursing of California (#01036) and Louisiana (#LSBN12).
24. Dubb R, Nydahl P, Hermes C, et al. Barriers and strategies for early mobilization of patients in intensive care units. Ann Am Thorac Soc. 2016;13(5):724-730.
To purchase electronic or print reprints, contact American Association of Critical-Care Nurses, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; email, [email protected].
THE NEXT STEP IN PROVIDING EXCELLENT CARE to your critical care patients in any practice settingNew to the 2nd Edition• Updated information throughout reflects the latest evidence-based knowledgeplus national and international treatment guidelines• Streamlined content places a greater focus on need-to-know information for nurses in today’s high acuity, progressive, and critical care settings• Expanded coverage of the most topical emerging and infectious diseases including Zika virus and multidrug-resistant infections• Additional content on alternative settings including the eICU and remotemonitoringThe book is organized by body systems with synthesis chapters addressing patient conditions involving multiple body systemsEndorsed by the American Association of Critical-Care Nurses, this comprehensive, nursing-focused text underscores clinical reasoning skills as it helpsreaders comprehend, analyze, synthesize, and apply advanced critical care knowledgeand conceptsAdvanced Critical Care Nursing, 2nd edition, is a must-have resource dedicated to helping you oversee or care for critical care patients in any practice setting
Edited by Vicki S. Good and Peggy L. KirkwoodMarch 2017, 912 pagesISBN: 978-1455758753 VISIT aacn.org/store to get your copy today!
NEW EDITION!

NO TIME FOR EARLY MOBILITY?By Cindy Cain, RN, DNP, CNS, CCRN
AJCC Patient Care Page The AJCC Patient Care Page is a service of the American Journal of Critical Care and the American Association of Critical-Care Nurses.
Designed to elaborate on AACN practice guidelines based on content in select articles, this page may be photocopied noncommer-
cially for use by readers in their workplace, in continuing education programs, or for distribution to colleagues, patients, or
patients’ families. To purchase bulk reprints, call (800) 899-1712.
Based on material from and published as a supplement to the article by Young et al, “Identifying Barriers
to Nurse-Facilitated Patient Mobility in the Intensive Care Unit” (American Journal of Critical Care.
2018;27:186-193) and the article by Colwell et al, “Mobilization Therapy in the Pediatric Intensive
Care Unit: A Multidisciplinary Quality Improvement Initiative” (American Journal of Critical Care.
2018;27:194-203).
We know that early mobility has many
benefits. Nurse-facilitated early mobility
reduces incidence of delirium, improves
muscle strength, increases independent
functional status after discharge, and
improves overall quality of life.1 Early mobility also decreases
health care costs with fewer days of mechanical ventilation
and shorter stays in the intensive care unit.1 The question
then becomes, how do I fit one more task into my shift?
That is the question that Young et al and Colwell et al
seek to answer in their respective studies “Identifying Barri-
ers to Nurse-Facilitated Patient Mobility in the Intensive Care
Unit” and “Mobilization Therapy in the Pediatric Intensive
Care Unit: A Multidisciplinary Quality Improvement Initia-
tive.” Although early mobility is an interprofessional respon-
sibility, nurses have the unique distinction of being present
with the patient more than any other member of the health
care team. Thus nurses have the opportunity to assist patients
with passive range of motion exercises, dangling legs at the
bedside, or other types of early mobility at times that are
convenient to both the patient and the nurse.
Here’s what you can do:• Use the minimum required sedation for your patients
receiving mechanical ventilation.
• Consider using an early progressive mobility tool to
determine when it is safe for a patient to participate in early
mobility and the type of early mobility that is appropriate
for your patient.
• Look for opportunities to incorporate patients’ mobil-
ity activities such as passive range of motion exercises, dan-
gling legs at the bedside, or sitting/standing at the bedside
during times of routine nursing care.
• Assess your patient daily for readiness to mobilize or
advancement to the next level of a progressive mobility plan.
Other helpful resources:• View the AACN webinar “Executing Evidence-Based
Progressive Mobility in the ICU” and download the accom-
panying Tools and Tactics resources, https://www.aacn.org
/education/webinar-series/wb0007/executing-evidencebased
-progressive-mobility-in-the-icu. Share the tools with your team.
• Review CSI Mobility Projects: “Walk This Way: Early
Progressive Mobility in the ICU,” “Don't Be a Bedhead: Help
Your Head, Get Out of Bed,” and “Keep the Beat, Move Your
Feet” at https://www.aacn.org/nursing-excellence/csi-academy
/projects?page=1&topic=Pulmonary.
• Review early mobility and exercise information from
the ICU Delirium and Cognitive Impairment Study Group
at http://www.icudelirium.org/earlymobility.html.
• Review the Society of Critical Care Medicine’s ICU
Liberation web page on early mobility at http://www
.iculiberation.org /Mobility/Pages/early-mobility.aspx.
REFERENCE1. Parker A, Needham DM. The importance of early rehabilitation and
mobility in the ICU. Crit Connect. Society of Critical Care Medicine web-site. Published August 4, 2013. http://www.sccm.org/Communications /Critical-Connections/Archives/Pages/Importance-Early-Rehabilitation -Mobility-ICU.aspx. Accessed February 26, 2018.
©2018 American Association of Critical-Care Nursesdoi:https://doi.org/10.4037/ajcc2018441
204 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
Illustration by Steve Oh

Critical Care Management
©2018 American Association of Critical-Care Nursesdoi:https://doi.org/10.4037/ajcc2018303
Background Early red blood cell transfusions are a common treatment for adults hospitalized for sepsis without shock. However, their utility and association with mortality and costs have not been well studied.Objectives To examine early transfusion rates for patients with sepsis treated outside intensive care units, and to find a correlation between transfusion rates and survival rates and costs. Methods Data were obtained from hospital members of the Premier Healthcare Alliance that admitted at least 50 adults with sepsis between January 1, 2006, and December 31, 2010. Early transfusion rates at each hos-pital were calculated as the observed incidence of allo-geneic red blood cells administered by hospital day 2. A multivariable logistic regression model was constructed to estimate the expected or risk-adjusted transfusion rates, mortality rates, and costs.Results A total of 256 396 adults were hospitalized with sepsis without major bleeding or surgery at 364 US hospitals. Approximately 84% of all patients admitted with sepsis, without vasopressor therapy, were treated outside the intensive care unit (by day 2). The mean insti-tutional early transfusion rate was 6.9%. After risk stan-dardization, the median (interquartile range) transfusion rate was 6.7% (5.8%-7.6%), mortality rate was 15.5% (13.1%-18.1%), and costs were $13 333 ($11 939-$14 986). Early transfusion rates were not correlated with mortal-ity but were modestly positively correlated with costs (Spearman = 0.157; P = .003). Conclusions Early transfusion rates during hospitaliza-tion for sepsis without shock varied widely across the hospitals. Transfusion rates were associated with increased costs but not with mortality rates. (American Journal of Critical Care. 2018; 27:205-211)
EARLY BLOOD TRANSFUSIONS IN SEPSIS:UNCHANGED SURVIVAL AND INCREASED COSTSBy Karthik Raghunathan, MD, MPH, Mandeep Singh, MD, Brian H. Nathanson, PhD, DSHS, Elliott Bennett-Guerrero, MD, and Peter K. Lindenauer, MD, MSc
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 205

Between 1997 and 2011, the rate of hospitalization for sepsis increased more rapidly than that for any other condition in adults older than 45 years in the United States.1,2 During such hospitalization, allogeneic red blood cell (RBC) transfusions are often ordered by internists in the general medicine service.3,4 Although the Surviving Sep-sis Campaign recommends a generally restrictive approach to RBC transfusions, it
also endorses early goal-directed therapy for patients with tissue hypoperfusion, including a hemoglobin level lower than 10 g/dL (to convert hemoglobin to g/L, multiply by 10.0).5,6
Efforts to reduce medical resource
waste are increas-ingly relevant.
206 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
The benefit of such transfusions in septic shock
with central venous desaturation was recently called
into question by 4 large randomized controlled tri-
als.7-10 However, unlike septic shock, sepsis is treated
mostly outside of intensive care units (ICUs) by
internists.2 The utility of RBC transfusion in patients
with sepsis and the association of such transfusion
with survival and costs remain unknown. Efforts to
reduce medical resource waste (eg, the Choosing
Wisely campaign) may be especially
relevant because of the large num-
ber of adults with sepsis admitted
to US hospitals each year.11 There-
fore, in this study, we aimed to eval-
uate the institutional variations in
transfusion practices and their asso-
ciation with the institutional varia-
tions in mortality and costs. We hypothesized that
early RBC transfusions are a common treatment for
sepsis without shock and do not improve survival.
Methods After obtaining approval for this study from
the institutional review board at Baystate Medical
Center, we collected retrospective data on a cohort
of adult patients with sepsis admitted between Janu-
ary 1, 2006, and December 31, 2010, to hospitals
that are members of the Premier Healthcare Alliance.
Most hospital members of Premier are small (< 200
beds) to medium-sized (200-399 beds) institutions
in urban locations and without teaching affiliations.
The details of this voluntary, fee-supported, admin-
istrative and financial data set are described in previous
studies on sepsis and other hospital-based condi-
tions.12,13 In addition to the International Classifica-
tion of Diseases, Ninth Revision, Clinical Modification
(ICD-9-CM) diagnosis and procedure codes, item-
ized charges for diagnostic and therapeutic interven-
tions (eg, laboratory, radiology, and microbiology
tests; transfusions; mechanical ventilation; dialysis;
medications) as well as for other billable services for
each patient at each hospital are included in the data
set in a standardized format for each hospital day.
Study PopulationOur study focused on early RBC transfusions,
defined as the administration of allogeneic RBCs on
the day of hospital admission (day 1) or on the next
day (day 2), because such therapy was likely to be
associated with the admitting diagnosis. The patients
in our study population had a principal diagnosis
of sepsis14 (with ICD-9-CM codes including 038 and
995.91; see Supplement 1, available online only at
www.ajcconline.org, for a list of the ICD-9-CM codes
included) and had charges for blood cultures and
intravenous antibiotics initiated by day 2 and con-
tinued for at least 3 consecutive days. We excluded
patients who were discharged alive or died by day
2. To focus on transfusions for sepsis, we excluded
patients with charges for gastrointestinal bleeding
therapy (eg, colonoscopy, endoscopy, infusions of
proton pump inhibitors of histamine-2 receptor
blockers) or with a diagnosis or treatment for gas-
trointestinal hemorrhage (ICD-9-CM code 578) at
any time during hospitalization as well as patients
who had any all-patient refined diagnosis-related
group (APR-DRG) codes signifying major surgical
About the AuthorsKarthik Raghunathan is an associate professor, Department of Anesthesiology, Duke University Medical Center and Durham Veterans Affairs Medical Center, Durham, North Carolina. Mandeep Singh is an assistant professor, Depart-ment of Anesthesiology, University of Southern Califor-nia, Los Angeles, California. Brian H. Nathanson is chief executive officer, OptiStatim, LLC, Longmeadow, Massa-chusetts. Elliott Bennett-Guerrero is a professor, Depart-ment of Anesthesiology, Stony Brook University Medical Center, Stony Brook, New York. Peter K. Lindenauer is director, Institute for Healthcare Delivery and Population Science, and professor of medicine, University of Mas-sachusetts–Baystate; professor of quantitative health sciences, University of Massachusetts Medical School, Worcester; and an adjunct professor, Tufts University School of Medicine, and Tufts Clinical and Translational Science Institute, Boston, Massachusetts.
Corresponding author: Karthik Raghunathan, MD, MPH, Department of Anesthesiology, Duke University Medical Center/Durham VAMC, DUMC 3094, Durham, NC 27710 (email: [email protected]).

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 207
A multivariable logistic regression model predicting early RBC transfusions on the basis of patient charac-teristics was constructed and applied at each hospital.
procedures (APR-DRG codes 005, 444, and 710).
In addition, we excluded patients who were likely
to have ongoing blood loss (ie, those with charges
for more than 3 units of RBCs on any single hospital
day, for blood products other than RBCs at any time
during hospitalization, or for more than 2 labora-
tory tests for hematocrit or hemoglobin levels on
any single hospital day). We also excluded patients
who were transferred between hospitals, as they were
not tracked within Premier and thus might have had
missing early exposure and late outcomes data. See
Supplement 1 (available online only) for the list of
inclusion and exclusion criteria.
Exposures, Outcomes, and Analyses To avoid bias inherent in patient-level analyses,
we conducted all analyses at the hospital level.15 At
each hospital, exposure was defined as the observed
rate of early transfusions or the proportion of patients
who received RBC transfusions by day 2, whereas the
expected rate was the proportion of patients predicted
to receive RBC transfusions by day 2. Mortality out-
come was defined as the proportion of patients who
died in the hospital after day 2. Costs were defined
as the mean of total charges for each patient.
To estimate the expected rate of early transfu-
sions, we constructed a multivariable logistic regres-
sion model that predicted early transfusions solely
on the basis of patient characteristics, and then
we applied the model at each hospital. This model
included the following predictors: patient demograph-
ics; chronic comorbidities, grouped using Healthcare
Cost and Utilization Project software (Agency for
Healthcare Research and Quality [AHRQ]); and
interventions received by day 2. Using date-stamped
charge codes (see Supplement 2, available online
only), we identified the early interventions admin-
istered such as intravenous fluid, vasopressor drug,
inotropic agent, central venous catheterization,
mechanical ventilation, and dialysis. Because large
volumes of crystalloid solution may result in
hemodilution and consequent RBC transfusion,
we accounted for the proportion of patients who
had received 5 L or more of crystalloid solution
by day 2.16 We ensured the accuracy of the model
by using the area under the receiver operating char-
acteristic curve, Hosmer-Lemeshow statistic, and
adjusted Brier score17 (see Supplement 3, available
online only).
We calculated risk-standardized rates at each
institution using ratios of observed and expected
transfusion rates, and we examined institutional
variations in transfusion practices (independent of
the underlying differences in patient populations)
by comparing these
rates. Using similar
methods, we com-
puted standardized
mortality ratios and
adjusted cost ratios at
the institutional level.
Then, we correlated
risk-standardized early
transfusion rates with
the adjusted mortality
rates and costs using Spearman rank correlations.
We repeated all analyses to conduct sensitivity analy-
ses for our subset of patients with septic shock.
This subset was defined by the patients’ admission
to an intensive care unit (ICU) and receipt of vaso-
pressors by hospital day 2 (see Supplements 1 and
4, available online only).
Results The study cohort consisted of 256 396 adults
with sepsis admitted to 364 US hospitals (Figure 1)
Figure 1 The study cohort.
n = 36 235 did NOT receive any
red blood cells
n = 4840received at least 1
unit of red blood cells
n = 238 581 did NOT receive any red blood
cells early
n = 17 815 received red blood cells early
Transfusion by day 2 Transfusion by day 2No transfusion by day 2 No transfusion by day 2
Excluded patients with any possibility of active bleeding, any major surgery, incomplete data or admission to low-volume hospitals (< 50 cases)
(n = 320 437)
Adults with valid sepsis codes, charges for intravenous antibiotics and blood cultures by day 2, and
a known mortality outcome (n = 576 833)
Study cohort of adults with sepsis
(n = 256 396 across 364 hospitals)
Septic shock subsetPatients who were admitted to an intensive care unit and receiving
vasopressors by day 2(n = 41 075 across 254 intensive
care units)

208 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
between January 1, 2006, and December 31, 2010.
The overall rate of early RBC transfusions was 6.9%,
representing 17 815 patients who received 34 898
units of RBCs by day 2 at a median dose of 2 units.
These early transfusions represented 42.0% (17 815)
of all patients receiving a transfusion (42 390) and
32.7% (34 898 of 106 783) of all units transfused
during hospitalization for sepsis. When compared
with patients who did not receive early transfusions,
those who did were more likely to have a history
of anemia, malignant neoplasms, and weight loss.
Conversely, early transfusions were less likely in
patients with chronic pulmonary disease, obesity,
hypertension, and neurological comorbidities (Table
1 and Supplement 2). Patients who received early
transfusions, compared with those who did not,
had higher mortality rates (22.7% [4038] vs 14.9%
[35 548])and greater hospital costs (US $18 030 vs
$13 268; Table 1). At the hospital level, the median
(interquartile range [IQR]) early transfusion rate was
6.4% (4.5%-8.4%), the median (IQR) mortality rate
was 15.3% (12.6%-18.0%), and the median (IQR)
costs were $12 783 ($11 151-$15 194).
The multivariable model used for risk standard-
ization of early transfusion practices had an area under
the receiver operating characteristic curve of 0.78
(Supplement 3). Applying this model, we computed
and compared the risk-standardized rates across 364
hospitals. The median (IQR) risk-standardized early
transfusion rate was 6.7% (5.8%-7.6%) (Figure 2).
Rates varied widely across hospitals. Thirty-eight of
the 364 hospitals (10.4%) had early transfusion rates
greater than 10. The median (IQR) risk-standardized
mortality rate was 15.5% (13.1%-18.1%), and the
median (IQR) adjusted costs were $13 333 ($11 939-
$14 986). We found a modest positive correlation
between transfusion rates and costs (Spearman
= 0.157; P = .003; Figure 3). We did not find any
Variable
Table 1Selected characteristics and outcomes of adults with sepsis admitted to the hospitala
Admission via emergency department
Comorbid condition Smoking (current) Hypertension Obesity Weight loss Other neurological disorders Chronic blood loss anemia Deficiency anemias
Treatments by day 2 Vasopressors 0 1 2 3
Admission to intensive care unit Mechanical ventilation Sodium bicarbonate Hydrocortisone Central venous pressure monitoring Arterial catheterization Supplemental iron administration Ferritin test Colloids Volume of crystalloid solution, mean (SD), mL 5 L of crystalloid solution
Outcomes Mortality Costs, $
0.103 0.149 0.144-0.1940.141-0.130-0.494
0.280-0.169-0.141-0.121
-0.340-0.203-0.212-0.192-0.258-0.137-0.303-0.284-0.202-0.158-0.134
-0.185-0.299
72.9
2.830.6 6.819.613.6 2.855.7
68.518.5 8.4 4.7
48.819.016.512.126.4 6.014.812.510.9341826.4
22.718 030
76.0
4.537.510.411.918.4 0.731.1
81.511.9 4.5 2.1
31.811.0 8.7 5.815.0 2.7 4.1 3.1 4.6
2599 (2939)20.5
14.913 268
Standardized differencec
Patients who received early transfusionb
(n = 17 815)
Patients who did not receive early transfusionb
(n = 238 581)
a See Supplement 1 (available online only, at www.ajcconline.org) for the complete list of variables compared. b Numbers in this column are percentage of total number of patients in the group unless otherwise indicated in the first column.c Standardized differences are shown, rather than P values, because standardized differences measure the differences between groups independent of sam-
ple size. Although there is no accepted threshold to determine the significance of standardized differences, we elected to display characteristics with a standardized difference greater than 0.1 or less than -0.1.

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 209
correlation between transfusion and mortality rates
(Spearman = 0.078; P = .14; Figure 3). After risk
standardization, mortality rates were statistically
similar at hospitals in the highest and the lowest
transfusion quintiles. Hospitals with 400 or more
beds and hospitals with teaching affi liations had
signifi cantly higher transfusion rates (Table 2). We
did not observe any geographic differences.
In sensitivity analyses, which were restricted to
41 075 patients with septic shock who were admitted
to the ICU and received vasopressors by day 2, risk-
standardized rates of early transfusion varied between
0% and 30.4% with a median rate of 10.5% (Sup-
plement 4 and Figure 2). Analyses at the ICU level
were consistent with hospital-level analyses, as trans-
fusion rates were associated with costs but not with
mortality rates. The ICUs in larger hospitals (≥400
beds) with teaching affi liations and in urban loca-
tions had higher transfusion rates.
Discussion Our main fi nding was that early RBC transfusions
for sepsis—the single most expensive reason for hos-
pitalization1,2—were associated with increased costs
but not with survival. This fi nding is an extension
of or similar to fi ndings in studies on patients with
septic shock.7-10 We examined the institutional rates
of early transfusion in adults with sepsis without
Figure 2 Variations in risk-standardized rates of red blood cell transfusion across 364 hospitals (left) and intensive care units in 254 hospitals (right).
Percentage of patients with sepsis receiving at least 1 unit of red blood cells by day 2 at hospital level
Percentage of patients with septic shock receiving at least 1 unit of red blood cells by day 2 at hospital level
1515
1010
55
000 105 2010 3015
0
Perc
enta
ge
of
ho
spit
als
(n =
364
)
Perc
enta
ge
of
ho
spit
als
(n =
254
)
Figure 3 At the hospital level, early red blood cell (RBC) transfusions were not correlated with mortality (left panel) but were positively correlated with costs (right panel).
Standardized transfusion ratio
Ris
k-st
and
ard
ized
mo
rtal
ity
rate
, %
Ad
just
ed c
ost
s, $
Standardized transfusion ratio
2.5 2.52.0 2.01.5 1.51.0 1.00.5 0.50
0
10
20
30
40
50
60
0
5 000
10 000
15 000
20 000
25 000
30 000
0
Restrictive RBC transfusions
Low
mo
rtal
ity
Bel
ow
-ave
rag
e co
sts
Ab
ove
-ave
rag
e co
sts
Hig
h m
ort
alit
y
Restrictive RBC transfusionsLiberal RBC transfusions Liberal RBC transfusions

210 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
Early RBC transfu-sions, common in
patients without sep-tic shock and usually
given outside the ICU, are associated with increased costs but
no better survival.
major bleeding or surgery. After adjusting for inter-
hospital differences in patient characteristics, we
found that early transfusion rates varied significantly
among the 256 396 adults treated at 364 hospitals.
By hospital day 2, approximately 84% of patients
with sepsis, without shock (no vasopressor therapy),
had been treated outside the ICU, with approximately
1 in 15 (6.7%) receiving RBC
transfusions. Such early trans-
fusion rates were not associ-
ated with mortality rates,
but higher transfusion rates
meant greater costs.
Our finding that transfu-
sions were a common treat-
ment for sepsis was confirmed
in an AHRQ report18 indicat-
ing that the RBC transfusion
rate during hospitalization
for sepsis increased from
9.3% in 2000 to 13.7% in
2013.Our cohort of patients
represented the largest number of adults at risk for
receiving transfusions in US hospitals.1,2
We observed a lack of association between
hospital-level transfusion rates and mortality rates,
and this finding is consistent with the results of sev-
eral patient-level randomized controlled trials but
has not been described previously.7-10,19 Similar
variations in transfusion practices were found in
patients who were admitted to ICUs or undergoing
surgical procedures.19,20 Patients in our cohort were
under the care of internists in the general medicine
service, who order more RBC transfusions than do
physicians in any other hospital service. Therefore,
efforts to improve cost-effectiveness should also be
focused on these clinicians.3,4 Direct and indirect
costs of RBC transfusion have been estimated at $761
per unit administered,21 and the number of patients
receiving this costly and potentially unnecessary treat-
ment is large. Internists may help reduce such waste
by ordering fewer transfusions and routine laboratory
tests of hemoglobin level as well as by promoting the
use of pediatric blood-collection tubes (which mini-
mize phlebotomy-related blood loss).20,21
Strengths and LimitationsThe strengths of this study include the involve-
ment of a large sample of hospitals, which represented
approximately 15% to 20% of all hospitalizations
for sepsis in the United States during the study
period, and the use of reliable definitions of sepsis,
exposure to RBCs, and the mortality and cost out-
comes. The Premier data set was well suited for
examining costs as it contained detailed billing
records, and clerical errors in the attribution of
charges were less likely because allogeneic RBC
transfusions were carefully audited for ABO and Rh
compatibility. By conducting analyses at the hos-
pital level, we minimized bias that may threaten the
validity of observational patient-level studies.15,17
We confirmed our hospital-level results in ICU-level
sensitivity analyses.
Our study has several limitations, the most sig-
nificant of which is the lack of data on hemoglobin
levels. Hence we were unable to define an optimal
threshold for clinically beneficial RBC transfusion.
Although we examined a homogeneous patient
cohort, we still observed variations in transfusion
practices, but such variations might have been due
to hospital-level differences in hemoglobin levels.
We accounted for interhospital differences in patient
mix, including differences in rates of diagnoses of
chronic blood loss anemia and deficiency anemias
as well as in rates of other treatments for anemia
(eg, supplemental iron), further minimizing the
alternative explanations for the observed institu-
tional variation in practice.
Another limitation is our use of data from 2006
through 2010. However, our findings were confirmed
by a report18 that RBC transfusions during hospital-
ization for sepsis increased from 2000 to 2013. Last,
our hospital-level analyses are subject to the ecological
Hospital characteristic
Table 2Variation in standardized transfusion ratios across 364 hospitals
.04
.02
.99
.13
0.87 (0.60-1.15)0.97 (0.71-1.16)0.94 (0.77-1.15)1.04 (0.78-1.28)1.08 (0.92-1.30)
1.00 (0.81-1.26)0.94 (0.67-1.16)
0.98 (0.70-1.17)0.96 (0.73-1.23)
1.01 (0.79-1.27)0.92 (0.66-1.18)0.93 (0.68-1.13)0.99 (0.75-1.19)
115 (31.6) 79 (21.7) 71 (19.5) 45 (12.4) 54 (14.8)
101 (27.7)263 (72.3)
296 (81.3) 68 (18.7)
82 (22.5) 60 (16.5)153 (42.0) 69 (19.0)
No. of beds < 200 200-299 300-399 400-499 500
Teaching status Teaching Nonteaching
Location Urban Rural
Region Midwest Northeast South West
P valuebStandardized
transfusion ratioaNo. (%) of hospitals
a Median (interquartile range: 25th-75th percentile).b From Kruskal-Wallis test.

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 211
fallacy, wherein correlations at an aggregate level
may not exist at the patient level and residual con-
founding due to unmeasured factors is possible.
Conclusion We studied early RBC transfusions during hos-
pitalization for sepsis and found that approximately
1 in every 15 adults with sepsis without major bleed-
ing or surgery received this therapy during the epi-
sode of care. Transfusion rates varied widely across
the hospitals in our study, and a comparable group
of patients with sepsis received transfusions as fre-
quently as 1 in every 10 patients or as rarely as 1 in
every 25 patients without any differences in mortal-
ity rates. Such variation was associated with increased
costs. A practical strategy for reducing costs without
decreasing the quality of care may be for internists
to limit early RBC transfusions following admission
for sepsis.22-25
FINANCIAL DISCLOSUREDr Nathanson reported receiving a consulting fee for statistical analysis from Duke University School of Medicine. No other disclosures were reported.
SEE ALSO For more about sepsis, visit the Critical Care Nurse web-site, www.ccnonline.org, and read the article by Droege et al, “Application of Antibiotic Pharmacodynamics and Dosing Principles in Patients With Sepsis” (April 2016).
REFERENCES1. Pfuntner A, Wier LM, Stocks C. Most frequent conditions in
U.S. hospitals, 2011. http://www.hcup-us.ahrq.gov/reports /statbriefs/sb162.jsp. Healthcare Cost and Utilization Project Statistical Brief number 162. Published September 2013. Accessed January 26, 2016.
2. Torio CM, Moore BJ. National inpatient hospital costs: the most expensive conditions by payer, 2013. http://www.hcup -us.ahrq.gov/reports/statbriefs/sb204-Most-Expensive -Hospital-Conditions.jsp. Healthcare Cost and Utilization Project Statistical Brief number 204. Published May 2016. Accessed September 14, 2016.
3. Whitaker BI, Hinkins S, US Department of Health and Human Services. The 2011 National Blood Collection and Utilization Survey report. http://www.hhs.gov/ash/bloodsafety/2011 -nbcus.pdf. Accessed January 26, 2016.
4. US Department of Health and Human Services Advisory Committee for Blood Safety and Availability. 40th meeting minutes. Advisory Committee for Blood Safety and Avail-ability; June 8, 2011; Baltimore, MD. http://nih.granicus.com /DocumentViewer.php?file=nih_279c20e5-c8ef-4e28-b457 -d86995ff40fa.pdf. Accessed January 26, 2016.
5. Surviving Sepsis Campaign. Recommendations: other sup-portive therapy of severe sepsis. http://survivingsepsis.org /Guidelines/Documents/Other%20supportive%20therapy .pdf. Accessed January 26, 2016.
6. Dellinger RP, Levy MM, Rhodes A, et al; Surviving Sepsis Campaign Guidelines Committee including the Pediatric Subgroup. Surviving Sepsis Campaign: international guide-lines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580-637.
7. Holst LB, Haase N, Wetterslev J, et al; TRISS Trial Group; Scandinavian Critical Care Trials Group. Lower versus higher haemoglobin threshold for transfusion in septic shock. N Engl J Med. 2014;371:1381-1391.
8. ProCESS Investigators, Yealy DM, Kellum JA, et al. A ran-domized trial of protocol-based care for early septic shock. N Engl J Med. 2014;370(18):1683-1693.
9. ARISE Investigators; ANZICS Clinical Trials Group, Peake SL, et al. Goal-directed resuscitation for patients with early septic shock. N Engl J Med. 2014;371(16):1496-1506.
10. Mouncey PR, Osborn TM, Power GS, et al.; ProMISe Trial Investigators. Trial of early, goal-directed resuscitation for septic shock. N Engl J Med. 2015;372(14):1301-1311.
11. Bulger J, Nickel W, Messler J, et al; Choosing wisely in adult hospital medicine: five opportunities for improved healthcare value. J Hosp Med. 2013;8(9):486-492.
12. Raghunathan K, Shaw A, Nathanson B, et al. Association between the choice of IV crystalloid and in-hospital mortal-ity among critically ill adults with sepsis. Crit Care Med. 2014;42(7):1585-1591.
13. Lindenauer PK, Pekow PS, Lahti MC, Lee Y, Benjamin EM, Rothberg MB. Association of corticosteroid dose and route of administration with risk of treatment failure in acute exacerbation of chronic obstructive pulmonary disease. JAMA. 2010;303(23):2359-2367.
14. Martin GS, Mannino DM, Eaton S, Moss M. The epidemiol-ogy of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348(16):1546-1554.
15. Sjoding MW, Luo K, Miller MA, Iwashyna TJ. When do con-founding by indication and inadequate risk adjustment bias critical care studies? A simulation study. Crit Care. 2015; 19(1):195.
16. Tsui AK, Dattani ND, Marsden PA, et al. Reassessing the risk of hemodilutional anemia: some new pieces to an old puz-zle. Can J Anaesth. 2010;57(8):779-791.
17. Reade MC, Delaney A, Bailey MJ, Angus DC. Bench-to-bedside review: avoiding pitfalls in critical care meta-analysis—funnel plots, risk estimates, types of heterogeneity, baseline risk and the ecologic fallacy. Crit Care. 2008;12(4):220.
18. West KA, Barrett ML, Moore BJ, Miller JL, Steiner CA. Trends in hospitalizations with a red blood cell transfusion, 2000-2013. http://www.hcup-us.ahrq.gov/reports/statbriefs /sb215-Red-Blood-Cell-Transfusions.pdf. Healthcare Cost and Utilization Project Statistical Brief number 215. Pub-lished December 2016. Accessed January 14, 2017.
19. Salpeter SR, Buckley JS, Chatterjee S. Impact of more restrictive blood transfusion strategies on clinical out-comes: a meta-analysis and systematic review. Am J Med. 2014;127(2): 124-131.
20. Bennett-Guerrero E, Zhao Y, O’Brien SM, et al. Variation in use of blood transfusion in coronary artery bypass graft surgery. JAMA. 2010;304(14):1568-1575.
21. Shander A, Hofmann A, Ozawa S, Theusinger OM, Gombotz H, Spahn DR. Activity-based costs of blood transfusions in surgi-cal patients at four hospitals. Transfusion. 2010;50(4): 753-765.
22. Scott BH, Seifert FC, Grimson R. Blood transfusion is associ-ated with increased resource utilisation, morbidity and mor-tality in cardiac surgery. Ann Card Anaesth. 2008; 11(1): 15-19.
23. Rogers MA, Blumberg N, Saint S, Langa KM, Nallamothu BK. Hospital variation in transfusion and infection after car-diac surgery: a cohort study. BMC Med. 2009;7:37.
24. Lagu T, Rothberg MB, Nathanson BH, Pekow PS, Steingrub JS, Lindenauer PK. Variation in the care of septic shock: the impact of patient and hospital characteristics. J Crit Care. 2012;27(4):329-336.
25. Abdelsattar ZM, Hendren S, Wong SL, Campbell DA Jr, Henke P. Variation in transfusion practices and the effect on out-comes after noncardiac surgery. Ann Surg. 2015;262(1):1-6.
To purchase electronic or print reprints, contact American Association of Critical-Care Nurses, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; email, [email protected].

End-of-Life Care
©2018 American Association of Critical-Care Nursesdoi:https://doi.org/10.4037/ajcc2018300
Background Little is known about the effect of chaplains on critical care nurses who are caring for critically ill patients and their families.Objective To understand nurses’ experiences when they make a referral to the Spiritual Care Department for a patient or the family of a patient who is dying or deceased. Specific aims were to explore spiritual care’s effect on nurses and how nurses understand the role of spiritual care in practice.Methods A qualitative descriptive study using in-person, semistructured interviews in a 21-bed medical-surgical intensive care unit in a teaching hospital. Purposeful sampling identified nurses who had at least 5 years of experience and had cared for at least 5 patients who died on their shift and at least 5 patients for whom they initiated a spiritual care referral. Interviews were digitally recorded and anonymized; conventional content analysis was used to analyze transcripts. Three investigators inde-pendently coded 5 transcripts and developed the prelimi-nary coding list. As analysis proceeded, investigators organized codes into categories and themes.Results A total of 25 nurses were interviewed. The central theme that emerged was presence, described through 3 main categories: the value of having chap-lains present in the intensive care unit and their role, nurses’ experiences working with chaplains, and nurses’ experiences providing spiritual care.Conclusion Nurses considered spiritual care essential to holistic care and valued the support chaplains provide to patients, families, and staff in today’s spiritually diverse soci-ety. (American Journal of Critical Care. 2018; 27:212-219)
CRITICAL CARE NURSES’ EXPERIENCES WITH SPIRITUAL CARE:THE SPIRIT STUDYBy Nigel Bone, MDiv, RP, Marilyn Swinton, MSc, Neala Hoad, RN, Feli Toledo, MDiv, RP, and Deborah Cook, MD
1.0 HourC EThis article has been designated for CE contact
hour(s). See more CE information at the end of
this article.
212 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org

Although providing spiritual care has important meaning for nurses and enhances professional satisfaction,1 a “crisis of spirituality” has been identified within the nursing profession related to nurses’ preparedness to identify, assess, and provide spiritual care.1-4 This crisis may have evolved as modern nursing practice has been distanced from its original spiritual tradition through a more task-focused, problem-
solving approach to care.4 Another contributing factor may be technologic advances, which may have “led to a disconnect between caring for the body and caring for the soul.”5
Nurses report that attending to the spiritual care
of their patients is part of their scope of practice and
is rooted in holistic care.2-10 In 1988, the North Amer-
ican Nursing Diagnostic Association’s inclusion of
spiritual distress as a nursing diagnostic category
officially recognized the role of spiritual care in
nursing practice.11 However, according to several
studies,2,5,7-9,12 nurses do not receive education about
how to provide spiritual care.Some curricula “virtu-
ally ignore spiritual distress”9 despite recognition
that “spirituality is a way of being and experiencing
that shapes and impacts nursing presence.”13
According to results of a nursing survey, percep-
tions about the need for spiritual care differ depend-
ing on the care area; for example, in the operating
room, patients are usually unconscious and families
are not present, possibly attenuating the need for
spiritual care.12 In the intensive care unit (ICU), spir-
itual distress frequently is experienced by critically
ill patients requiring life support, their family mem-
bers, and staff.14 Referrals to professionals with
specialized knowledge and skills in spiritual care
are often made in this setting,15 because nurses may
lack the training to provide spiritual care and may be
uncomfortable with this aspect of practice.6-9,11,16-18
The role of spirituality in health care may be
assigned higher importance today than in the past,19
perhaps reflecting the growing societal interest in
spirituality.20 In a review of spirituality across disci-
plines, Swinton21 concluded that “it is clear that
people are trying to name and draw attention to
something that is missing from current ways of prac-
ticing.” The objective of our
study was to understand the
experiences of ICU nurses
when they make a referral to
spiritual care services for a
patient or the family of a
patient who is dying or is
deceased. Specific aims were to explore the effect of
spiritual care on nurses and how nurses understand
the role of spiritual care in the ICU.
Methods We used purposive sampling to identify ICU
nurses who had at least 5 years of experience, cared
for at least 5 patients who died on their shift, and
cared for at least 5 patients for whom they initiated
a referral to a chaplain (in this article, spiritual care
clinicians are referred to as chaplains). Nurses were
recruited through an email invitation.
Data were collected through semistructured
qualitative interviews. To frame a context for the
interview, we provided the following definition of
spirituality to participants:
Spirituality can mean different things
to different people and can be thought
of in terms of the ways that individuals
seek and express meaning and purpose,
and how they experience connections
with the moment, with themselves, with
others, with nature and with other things
that to them are significant or sacred. Reli-
gion is one way of expressing spirituality.15
Interviews were digitally recorded, transcribed verba-
tim, and anonymized.
AnalysisWe used qualitative description to produce a
descriptive summary of the findings.22 Conventional
About the AuthorsNigel Bone is a fellow in spiritual care and a registered psychotherapist, Spiritual Care Department, St Joseph’s Healthcare, Hamilton, Ontario, Canada. Marilyn Swinton is a research coordinator, Department of Health Research Methods, Evidence and Impact, McMaster University, Hamilton, Ontario, Canada. Neala Hoad is a registered nurse and research coordinator, Department of Critical Care, St Joseph’s Healthcare. Feli Toledo is a chaplain and registered psychotherapist, Spiritual Care Department, St Joseph’s Healthcare. Deborah Cook is a professor and intensivist, Department of Health Research Methods, Evidence and Impact and Department of Medicine, McMaster University; and Department of Critical Care, St Joseph’s Healthcare.
Corresponding author: Nigel Bone, MDiv, RP, St Joseph’s Healthcare Hamilton, 50 Charlton Ave, E, Hamilton, ON, Canada L8N 4A6 (e-mail: [email protected]).
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 213
“Most nursing pro-grams virtually ignore spiritual distress.”9

214 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
content analysis was used to analyze transcripts.
This is a coding approach whereby codes are derived
directly from the data without imposing precon-
ceived categories or theoretical perspectives.23 Three
investigators independently completed line-by-line
coding of 5 interview transcripts and, through a
consensus, developed the preliminary coding list.
The remaining transcripts were coded by 1 investiga-
tor, who recorded the evolution of the coding list
in an audit trail.24 The research team reviewed cod-
ing reports and organized the codes into categories.
We held a member checking event with 6 nurses to
assess the extent to which our findings resonated with
their experiences. N’Vivo (version 11.0; QSR Interna-
tional) was used for data management. Quantita-
tive data were summarized using descriptive statistics.
Results A total of 25 ICU nurses (22 women, 3 men) were
interviewed (Table 1). The following 3 main categories
emerged from the data, all related to the central theme
of presence: (1) the value of having chaplains present
in the ICU and their role, (2) nurses’ experiences work-
ing with chaplains in the ICU, and (3) ICU nurses’
experiences of providing spiritual care through their
own practice (Table 2).
Characteristica
Table 1Demographic characteristics of the 25 nurse participants
Age, y
Years worked as a nurse anywhere
Years worked as a nurse in an ICU
Years worked as a nurse in this hospital’s ICU
No. of patients in past year that nurses cared for who died during their shift in this hospital’s ICU
No. of referrals nurses made to spiritual care services for patients who died in the past year in this hospital’s ICU
43.7 (11.5)
21.0 (11.2)
17.5 (10.1)
17.1 (9.8)
14.6 (13.4)
8.6 (4.7)
Mean (SD)
Abbreviation: ICU, intensive care unit.
The value and role of having chaplains present in the ICU
Table 2Examples of 3 main themes found
“I can provide physical care but [spir-itual care] . . . it’s almost like round-ing out the care that we provide and it’s . . . that’s a good feeling for me. It’s almost a feeling of completeness of care, like, holistic. We’ve kind of come full circle and, you know, we’ve . . . we’ve addressed everything.”
“Spiritual care isn’t just for the patient . . . spiritual care, I think, pro-vides support to clinicians who are going through the process of, you know, losing a patient.”
“I’m there for the patient and the fam-ily, but often in situations, my respon-sibility goes to the patient first and foremost, so it’s nice to have some-body that’s there to take care of the family—the family is their primary focus, so that we work together, but I know that the family is looked after.”
“I find spiritual care clinicians not only deal with the spiritual aspect of things, like they have been kind of good at sorting out, like, even fam-ily dynamics and kind of calming the waters between family members that [are] at odds.”
“We had one instance, actually, if I can share that. It happened last fall . . . [a] very sick patient going to the OR. The surgeon said, ‘We’re not sure if he’s going to make it back.’ And spiritual care couldn’t make it here in time and I could feel from the family that they wanted prayers said before he went to the OR, so I prayed with them.”
“If the patient has died, I make sure their hands are out so that the family can hold their hands . . . I just allow them the opportunity to do what-ever they feel is right in the moment. If they just want to cry for an hour, I’ll just get boxes of [tis-sues] and make sure [there are] chairs around and [a] glass of water—just to make them more comfortable.”
“I remember him [patient’s family member] com-ing and me just sitting with him and chatting about how he was feeling and what was going on and, you know, kind of reassuring him, too, like, we’re looking after her and, you know, now you can do a little bit for yourself, too, which I think he [found] kind of like, eye opening. Kind of like, you know, ‘I can actually do something for myself right now.’”
“Hear the stories . . . because often they’ll speak of the patient, and the stories and, ‘Remember Dad did this,’ and ‘Remember Mum did that.’ And it’s nice, we’ll often, you know, go in and look at the photos that they have up.”
“A lot of times what we do is we brief the spiritual care personnel overall, [about] what’s going on with the indi-vidual, with the patient and with the families, because sometimes families are really stressed and they have difficulty dealing with diagnosis and prognosis.”
“When spiritual care is there with me in the room . . . it makes me feel less guilty that I have these tasks to do when some-one is dying in front of me and their family is there watching them pass away.”
“The more recent referrals I’ve made are not about dying. They’ve been more about comfort for patients or family . . . somebody just needs someone who has 30 minutes of their undivided attention to do nothing but listen to them.”
“It’s a shared experience and kind of unspoken support. It’s a bit intangible at times, but there’s comfort in seeing spiri-tual care staff . . . in some unspoken way, I’m feeling supported. . . . I’m not going through this alone. . . . There’s a sense of comfort because that person is there to experience it with me.”
How ICU nurses provide spiritual care through their practice
Nurses’ experiences working with chaplains on the unit
Abbreviation: ICU, intensive care unit; OR, operating room.

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 215
Value of Having Chaplains Present in the ICU and Their Role
Based on interview findings, we determined the
nurses viewed chaplains as an essential part of the
multidisciplinary team who were valued for their
supportive presence in 3 contexts: with patients and
families, with ICU staff, and in the ICU in general.
Chaplain’s Presence Supports Patients and Families.
We found that chaplains are considered by nurses to
have the optimal language and approach to support
patients and their families, regardless of the patient’s
or family’s faith or belief system:
Talking about the patient and who they
are, and acknowledging them as a per-
son—just reflecting on their life [is] some-
thing I’m pretty comfortable doing with
families. But there’s something about
the spiritual care person [who] has the
right language and has the ability to . . .
elicit that kind of reflection.
Nurses affirmed that chaplains can ease the pain
associated with the dying experience for patients and
families. They attributed this to the presence and indi-
vidualized approach of the chaplain:
When pastoral care is involved . . .it makes
the death more like it should be. It’s an
important event and it should be personal.
Chaplains’ Presence Supports Staff. In addition
to the support for patients and their families, nurses
shared how they often feel a sense of relief after call-
ing chaplains, knowing they will jointly help support
the patient and the patient’s family:
Relieved would be a good word. Just
that there is 1 more member of the
team that can help support the family.
I feel relieved that perhaps they already
have a relationship with the spiritual
care worker, so it’s another familiar
face, someone who knows their jour-
ney, someone who knows the patient
and the family and so there’s some-
thing familiar . . . It’s comforting for the
family and I feel comforted that they’re
feeling . . . better about the situation.
Nurses described how the presence of a chap-
lain personally supported nurses caring for dying
patients. They valued the opportunity to debrief,
which usually was done informally:
Sometimes they come around after an
event . . .and say “How are you doing?
That was a difficult situation.” . . . Then
we might debrief a bit . . . Even though
we go through a really difficult or tragic
experience, sometimes it’s over and then
we move on to the next patient. So I
always appreciate it when someone
comes along and says, “So, how are
things going? How did you find that?”
Chaplains Educate Through Their Presence in the
ICU. The important role for chaplains educating
nurses was underscored during the interviews, as
indicated by the following:
There’s great knowledge and experience
that could be transferred to some of our
more inexperienced nurses from spiri-
tual care. It would be great if that rela-
tionship was nurtured from the very
beginning and just became . . . part of
our culture here.
I think we learned from them . . . the
compassion part . . . You watch how they
work and we learn ourselves.
Nurses’ Experiences Working With Chaplains in the Unit
Nurses make referrals to chaplains through
all phases of a patient’s critical illness, sometimes
immediately after ICU admission. Through early
engagement of chaplains, patients and their families
can develop relationships that facilitate access to
spiritual support during the patient’s stay. Nurses
described a shared-care model when working with
chaplains, which was articulated in the following
3 ways: (1) why nurses call spiritual chaplains, (2)
how nurses introduce the idea of spiritual care to
patients and families, and (3) the shared experi-
ence of nurses working with chaplains.
Why Nurses Call Chaplains. Nurses reflected
on how the presence of chaplains help provide an
essential aspect of holistic care at the end of life:
It’s the more holistic, humanistic
approach to dying than what we deal
with, which is more of the medical . . .
messy kind of things.
I always want to try and make sure the
family feels supported and that, if they are
religious or spiritual, they feel like we took
care of them from that perspective as well.
Nurses believed that the support delivered by
chaplains was a reflection of their own caring. Even
though they wanted to care for patients and their
families in every domain, nurses were sometimes
unable to do so because they were busy attending
to technical aspects of practice:

216 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
Sometimes we can’t spend as much
time at the bedside as we want to. And
so our spiritual care team just steps in
and they . . . just carry on that caring
that we always want the family to know
[is there] even though we can’t be there
all the time.
Some nurses were uncomfortable identifying
or addressing spiritual needs, preferring to have
chaplains involved:
I don’t always have the ability to find
comforting words. . . . I’m too intimi-
dated that I might say the wrong
thing . . . so I just find [the chaplain],
when they’re there, they deal with that
aspect, which is relieving [for] me.
How Nurses Introduce the Idea of Spiritual Care
Support to Patients and Families. Nurses talked about
different ways of introducing the service of spiri-
tual care to patients and families, depending on
the context:
Someone to be there if you need someone
to talk to because this is a hard time. That’s
pretty much how I say it.
Nurses sometimes guide hesitant families to
consider the potential role for chaplains by affirm-
ing their frequent involvement:
I also tell them that we use them often. I
do make sure that they know that because
I don’t want them to think that someone
will come into the room who really doesn’t
have much experience with that situation
or with someone becoming palliative or
someone dying.
Nurses’ Shared Experience of Working With Chap-
lains. Nurses appreciated sharing the caring experi-
ence with chaplains. They talked about wanting to
have chaplains present more often, not only at the
end of life:
I think we work really cooperatively. I
really appreciate and trust their ability
and their gifts. . . . Personally, I like to
have the presence of the spiritual care
team in the unit even when we don’t have
a dying patient at that very moment.
Dialogue between nurses and chaplains was
identified as helping to share information about the
patient, the patient’s family, and their circumstances,
particularly when people are experiencing difficulty
accepting a patient’s prognosis. Nurses described
that chaplains often forge an intimate relationship
with the patient and family, which facilitates sharing
important aspects of personhood with the interpro-
fessional team:
Spiritual care will come to us to ask us
about the family and we’ll ask them
what things they found out, because
sometimes the family will talk differ-
ently . . . to someone like [the chaplain,
saying some different than] what they
would tell the nurse or the doctor.
How ICU Nurses Provide Spiritual Care Through Their Practice
All of the nurses that we interviewed shared
examples of providing spiritual care to patients and
families through their presence, but not all of them
cited this presence as being part of providing spiri-
tual care. We learned about the intentional provision
of spiritual care from some nurses, and the unarticu-
lated, if not unrecognized, provision of spiritual care
by others. From these data, 3 ways that nurses pro-
vide spiritual care through presence in their practice
were identified: (1) intention, (2) being with the
patient and/or family, and (3) compassion.
Intention. One of the most common motivators
for nurses to provide the best end-of-life experience
possible was intention:
I don’t want to miss an opportunity when
somebody’s going to pass away that they
would have liked some spiritual advice,
prayers, or calling your own pastor.
Yeah, it’s just 1 of those things. It’s . . .
someone’s last moment and . . you
have to make it the best for them.
Being With the Patient and/or Family. Given the
large amount of time that nurses spend at the bed-
side with their patients, their presence was consid-
ered to be a manifestation of their provision of
spiritual care:
We’re not necessarily invited, but I auto-
matically go in and shut the door, and
I like to be part of it because I think it’s
nice for the families to see that and it
makes them feel like their loved one . .
they’re not just a patient.
Nurses often disclosed being unaware of when
they were providing spiritual care. One nurse said,
“I think we all do it; we just don’t realize that we’re
doing it.” Nurses gave examples, such as the follow-
ing, of unknowingly providing spiritual care through
their presence:

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 217
Nurses valued informal, immediate debriefing with chaplains after challenging clinical situations.
We had a young lady in our unit . . . the
parents were in the room and I wasn’t
even aware I was doing it, and the mom
said to the daughter, who was in the
bed, “This must be so reassuring for
you because this is what your Grandma
would do. She would hum for you.” . . .
So I do things like that without even
being aware, and it brings them some
peace and comfort.
Compassion. Nurses claimed compassion as
something that comes naturally to them, citing it
as a core component of nursing practice that posi-
tively affects nurses themselves:
I think I’d only been with the patient
maybe a few hours that day. And the
family member pulled me aside and
said, “I can see that you really, really
love your work by your actions.”
It’s not always what you say . . . but your
actions . . . you know . . . whether it be a
touch of their forehead as you are talking
to them or holding their hand or . . . get-
ting a glass of water.
One of the things that is most powerful
for me is when you have a patient [who]
doesn’t have any family and they don’t
really have anyone there when they’re
passing away. It’s kind of a peaceful
thing to go be with a patient and even
just hold their hand while they’re dying.
I think that’s kind of a spiritual thing.
Discussion We identified the presence of spiritual care to be
the central theme when nurses refer to chaplains for
dying or deceased patients in their care. Hailed as
“the most essential element of spiritual care,”25
“based on a healing relationship,”13 elements of
presence include a reciprocal relationship to the
whole person extending beyond the technical and
attending to their needs.26-29 Like spirituality, pres-
ence takes many forms and is challenging to define.
Spiritual care presence has been described as
being accompanying and comforting30—elements
that were identified by nurses in this study. Nurs-
ing presence has been described as reflecting
“uniqueness, connecting with the patient’s experi-
ence, sensing, going beyond the scientific data, know-
ing what will work and when to act, and being with
the patient.”27 The uniqueness of each nurse’s spiri-
tuality gives nursing presence its unique style.31,32
We identified a need for more guided discus-
sions by chaplains for nurses to learn how to pro-
vide spiritual care and make appropriate referrals.
This is an actionable item that could be imple-
mented through the integration of spiritual care
education into ICU orientation for new learners
and could lead to an overall decrease in the amount
of spiritual distress experienced by patients, fami-
lies, and unit staff. Lack of nursing preparation may
lead to hesitation inquiring about the spiritual needs
of patients and their families.1 Experienced nurses
suggested that better introduction to the hospital’s
spiritual care department and its roles would help
new graduates, who often have limited exposure to
spiritual care when starting their career. With guided,
repeated exposure to patients in crisis, nursing stu-
dents can recognize their nursing presence at work.13
In addition to periodic, scheduled, case-based
rounds after a death,33 nurses valued informal,
immediate debriefing with chaplains after chal-
lenging clinical situations; this finding aligned
with those of other reports.34
Strengths of this study include the descriptive
summary of the findings developed by a multidisci-
plinary team, with minimal theoretical interpreta-
tion. The interviews provided nurses an opportunity
to talk about and reflect on spirituality and their
practice. Results were presented in the words of
the research partici-
pants,21 and member
checking affirmed that
the findings resonated
with nurses. Limita-
tions of this study
include the single-
center design and the
focus on dying patients.
The generalizability of these findings should take
the setting into account: This study was conducted
in a faith-based hospital with a designated ICU
chaplain, 24-hour on-call chaplain coverage, a
chaplain to bed ratio of 0.70 to 21, periodic visiting
community clergy, and where a collaborative end-of-
life program was in place.35
Chaplains synergistically add a key dimension
to the care of the patient that no other member of
the health care team can provide,8 because spiritual
care is what chaplains do, rather than being a part
of what they do.11,36 The role of chaplains is crucial;
however, clearly they are not the only ones who pro-
vide spiritual care in the hospital.8,11,16 Ultimately,
nursing care focuses on wholeness, including spiri-
tuality,37 and meeting a patient’s spiritual needs is

218 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
not only consistent with best practice but may posi-
tively affect nurses themselves. Chaplains have the
skills and knowledge to help nurses identify when
they are engaging in spiritual care. Nurses in our study
recognized, with relative ease, acts of compassion
in their practice, manifested not just in words but in
actions. However, some nurses were unaware of
when, and how often, they provided spiritual care.38
In summary, we found that ICU nurses consid-
ered spiritual care to be an essential aspect of car-
ing holistically for critically ill patients. Nurses we
interviewed value the support chaplains provide to
patients, families, and clinicians, particularly, but
not only, when patients are dying. Nurses found
making referrals to the chaplains to be a positive
experience, contributing importantly to patient-
and family-centered care at the end of life in today’s
spiritually diverse society.
ACKNOWLEDGMENTSWe thank the nurses of the ICU at St Joseph’s Health-care Hamilton who participated in the SPIRIT Study. We appreciate the assistance of Diana Clancy with the tran-scription and of Nicole Zytaruk with the SPIRIT logo. We thank Gary Payne, manager of the Spiritual Care Depart-ment, for his encouragement with this project and for establishing a fellowship in spiritual care with a research component. We thank Lily Waugh, ICU manager, for her support of this study. We are grateful for Tammy French, RN, who helped to develop the project and provided clin-ical coverage for participants when they were being interviewed. This work was inspired by the work of the Sisters of St Joseph in Hamilton.
FINANCIAL DISCLOSURESThis study was supported by the St Joseph’s Healthcare Hamilton Spiritual Care Department and Academic Critical Care Office, and by peer-review funds from the St Joseph’s Healthcare Hamilton Professional Advisory Committee Research Award Program, the Canadian Foundation for Spiritual Care, and a grant from the Canadian Institutes of Health Research.
SEE ALSO For more about family support, visit the Critical Care Nurse website, www.ccnonline.org, and read the arti-cle by Mureau-Haines et al, “Family Support During Resuscitation: A Quality Improvement Initiative” (Decem-ber 2017).
REFERENCES
1. Canfield C, Taylor D, Nagy K, et al. Critical care nurses’ per-ceived need for guidance in addressing spirituality in criti-cally ill patients. Am J Crit Care. 2016;25(3);206-211.
2. Culliford L. Spirituality and clinical care: spiritual values and skills are increasingly recognized as necessary aspects of clinical care. BMJ. 2002;25(3):1434-1435.
3. Dickinson C. The search for spiritual meaning. Am J Nurs. 1975;75(10):1789-1794.
4. Hewa S, Hetherington RW. Specialists without spirit: crisis in the nursing profession. J Med Ethics. 1990;16(4):179-184.
5. Koenig HD. Spirituality in Patient Care: Why, How, When, and What? 2nd ed. West Conshohocken, PA: Templeton Press; 2007.
6. Davidhizar R, Bechtel GA, Cosey EJ. The spiritual needs of hospitalized patients. Am J Nurs. 2000;100(7):24C-24D.
7. Dickinson C. Reviewed Works: Spiritual Care; The Nurse’s Role by Sharon Fish, Judith Allen Shelly; Spiritual Care Workbook by Judith Allen Shelly. Am J Nurs. 1978;78(12): 2149.
8. Dimeo E. Nursing: significance for spiritual care. J Relig Health. 1980;19(3):240-245.
9. Murray CK. Addressing your patient’s spiritual needs. Am J Nurs. 1995;95(11);16N-16P.
10. Taylor EJ, Marnier I, Ricci-Allegra P, Foith J. Self-reported frequency of nurse-provided spiritual care. Appl Nurs Res. 2017;35:30-35.
11. Mohrmann ME. Ethical grounding for a profession of hospital chaplaincy. Hastings Cent Rep. 2008;38(6):18-23.
12. Grant D, O’Neil K, Stephens L. Spirituality in the workplace: new empirical directions in the study of the sacred. Sociol Relig. 2004;65(3):265-283.
13. Rankin, EA, Delashmutt MB. Finding spirituality and nursing presence the student’s challenge. J Holist Nurs. 2006; 24(4): 282-288.
14. Ho JQ, Nguyen CD, Lopes R, Ezeji-Okoye SC, Kuschner WG. Spiritual care in the intensive care unit: a narrative review [published online January 1, 2017]. J Intensive Care Med. doi:10.1177/0885066617712677.
15. Puchalski C, Ferrell B, Virani R, et al. Improving the quality of spiritual care as a dimension of palliative care: the report of the Consensus Conference. J Palliat Med. 2009; 12(10): 885-904.
16. Landry VL. Pastoral care in a trauma center. J Relig Health. 1996;35(3):211-214.
17. Sumner CH. CE credit: recognizing and responding to spiritual distress. Am J Nurs. 1998;98(1):26-31.
18. Hughes BP, DeGregory C, Elk R, Graham D, Hall EJ, Ressallat J. Spiritual Care and Nursing: A Nurse’s Contribution and Prac-tice. New York, NY: HealthCare Chaplaincy Network; 2017.
19. Pembroke NF, Pembroke JJ. The spirituality of presence in midwifery care. Midwifery. 2006:24(3);321-327.
20. Pesut B, Reimer-Kirkham S, Sawatzky R, Woodland G, Pever-all P. Hospitable hospitals in a diverse society: from chap-lains to spiritual care providers. J Relig Health. 2012; 51(3): 825–836.
21. Swinton J. What is missing from our practice? Spirituality as presence and absence. J Study Spiritual. 2011;1(1):13-16.
22. Sandelowski M. Whatever happened to qualitative descrip-tion? Res Nurs Health. 2000;23(1):334-340.
23. Hsieh HF, Shannon SE. Three approaches to qualitative con-tent analysis. Qual Health Res. 2005;15(9):1277-1288.
24. Rodgers BL, Cowles KV. The qualitative research audit trail: a complex collection of documentation. Res Nurs Health. 1993;16(3):219-226.
25. Burckhardt M., Nagai-Jacobson M. Spirituality: Living Our Connectedness. Albany, NY: Delmar; 2002.
26. Chase SK. Response to “The concept of nursing presence: state of the science.” Sch Inq Nurs Pract. 2001;15(4):323-327.
27. Doona ME, Chase SK, Haggerty LA. Nursing presence: as real as the Milky Way Bar. J Holist Nurs. 1999;17(1):54-70.
28. Duis-Nittsche ER. A Study of Nursing Presence [disserta-tion]. Galveston, TX: University of Texas at Galveston, 2002. Dissertation Abstracts International, 62, 10B.
29. Smith TD. The concept of nursing presence: state of the sci-ence. Sch Inq Nurs Pract. 2001;15(4):299-323.
30. Nolan S. Spiritual Care at the End of Life: The Chaplain as a “Hopeful Presence.” London, UK: Jessica Kingsley Pub-lishers; 2012.
31. DeLashmutt M. Spiritual Needs of Mothers Raising Children While Homeless [dissertation]. Fairfax, VA: George Mason University; 2000. Dissertation Abstracts International, 61, 03B.
32. Godkin J. Healing presence. J Holist Nurs. 2001;19(1): 5-21.33. Hough CL, Hudson LD, Salud A, et al. Death rounds: end-of-
life discussions among medical residents in the intensive care unit. J Crit Care. 2005;20(1):20-25.
34. Canadian Association for Spiritual Care. Scope of practice. http://www.spiritualcare.ca/profession/scope-of-practice/. Accessed January 25, 2018.
35. Cook D, Swinton M, Toledo F, et al. Personalizing death in the intensive care unit: the 3 Wishes Project: a mixed-methods study. Ann Intern Med. 2015;163(4):271-279.
36. Choi PJ, Curlin FA, Cox CE. “The patient is dying, please call the chaplain”: the activities of chaplains in one medical center’s intensive care units. J Pain Symptom Manage. 2015;50(4):501-506.
37. Canadian Nurses Association. Framework for the Practice of Registered Nurses in Canada. 2nd ed. Ottawa, Ontario,

Canada: Canadian Nurses Association; 2015. https://cna-aiic .ca/~/media/cna/page-content/pdf-en/framework-for-the-pracice-of-registered-nurses-in-canada.pdf?la=en. Accessed January 25, 2018.
38. Goldberg B. Connection: an exploration of spirituality in nursing care. J Adv Nurs. 1998;27:836-842.
1.0 Hour Category BC E Notice to CE enrollees:
This article has been designated for CE contact hour(s). The evaluation demonstrates your knowledge of the
following objectives:
1. Identify the value of having chaplains present in the intensive care unit for patients and family members as
well as the interprofessional team.
2. Describe the relationship between nurses and chaplains within the context of critical care.
3. Analyze the provision of spiritual care by critical care nurses and identify reasons they may be unaware of
providing it.
To complete the evaluation for CE contact hour(s) for this article #A1827032, visit www.ajcconline.org and
click the “CE Articles” button. No CE evaluation fee for AACN members. This expires on May 1, 2021.
The American Association of Critical-Care Nurses is an accredited provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. AACN has been approved as a provider of continuing education in nursing by the State Boards of Registered Nursing of California (#01036) and Louisiana (#LSBN12).
To purchase electronic or print reprints, contact American Association of Critical-Care Nurses, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; email, [email protected].

Pulmonary Critical CarePulmonary Critical Care
©2018 American Association of Critical-Care Nursesdoi:https://doi.org/10.4037/ajcc2018515
Background Case series have reported favorable out-comes with extracorporeal membrane oxygenation (ECMO) in patients with severe acute respiratory distress syndrome. However, those patients were generally young, with few comorbid conditions.Objective To characterize the clinical features and sur-vival rates of patients with severe acute respiratory distress syndrome who met criteria for ECMO but were managed without it.Methods Patients who met the study criteria were iden-tified prospectively. Inclusion criteria for ECMO included severe hypoxemia, uncompensated hypercapnia, or elevated end-inspiratory plateau pressures despite low tidal volume ventilation. Predicted survival rates with ECMO were calculated using the Respiratory ECMO Survival Prediction score.Results Of the 46 patients who met the criteria for severe acute respiratory distress syndrome and ECMO consid-eration, 5 received ECMO and 16 patients had at least 1 contraindication to it. The remaining 25 patients met ECMO criteria but did not receive the treatment. The patients’ mean age was 53.5 (SD, 14.3) years; 84% had at least 1 major comorbid condition. The median pre-dicted survival rate with ECMO was 57%. The actual hospi-tal discharge survival rate without ECMO was 56%.Conclusions The general medical intensive care patient population with severe acute respiratory distress syn-drome is older and sicker than patients reported in prior case series in which patients were treated with ECMO. In this study, the survival rate without ECMO was similar to predicted survival rates with ECMO. (American Journal of Critical Care. 2018; 27:220-227)
SURVIVAL OF PATIENTS WITH
SEVERE ACUTE RESPIRATORY
DISTRESS SYNDROME TREATED
WITHOUT EXTRACORPOREAL MEMBRANE OXYGENATIONBy Sarina K. Sahetya, MD, Roy G. Brower, MD, and R. Scott Stephens, MD
220 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org

Most patients with acute respiratory distress syndrome (ARDS) require mechani-cal ventilation to facilitate gas exchange while allowing time for supportive care and healing to occur. However, in some patients, mechanical ventilation cannot maintain gas exchange goals and may cause ventilator-induced lung injury, exacerbating the underlying inciting injury. In recent years, extracorpo-
real membrane oxygenation (ECMO) has been used increasingly for the treatment of patients with severe ARDS. This support can allow mechanical ventilation to be modified or removed, lowering the risks of ventilator-induced lung injury and oxygen toxicity. Yet, ECMO itself con-fers risks, including bleeding, vascular access complications, thrombosis, and infection.1-3
Despite its increasing use, the benefits of
ECMO for the treatment of ARDS have not been
clearly established. Early randomized controlled
trials in 1979 and 1994 did not show benefit with
ECMO in ARDS.4,5 However, ECMO technology
has advanced significantly with improved pumps,
oxygenators, and biocompatible circuits since that
time.6 In a recent controlled clinical trial, patients
with ARDS were randomly assigned to either usual
care at their local hospitals or transfer to a single,
ECMO-capable, high-volume tertiary hospital. Clini-
cal outcomes were better in the patients transferred
to the ECMO-capable hospital than in patients who
remained at their local hospitals. However, only
75% of the intervention group actually received
ECMO at the tertiary hospital.7 Moreover, medical
care in the control group was not standardized, and
fewer patients in the control group received lung-
protective ventilation. As a result, it is unclear if ECMO
or better care at a high-volume tertiary center was
the variable most responsible for the reduction in
mortality between the 2 groups.6,8
Adoption of ECMO increased further after
researchers reported findings of several uncon-
trolled case series indicating low mortality rates in
patients with ARDS associated with H1N1 influ-
enza who received ECMO.9-12 However, a significant
limitation of these encouraging case series is that the
patients who received ECMO were young (median
age, 36 years) and had mostly single-organ disease
(median Sequential Organ Failure Assessment score,
9),13 in contrast to the typical ARDS population, which
is substantially older and has more comorbid condi-
tions.14,15 Moreover, in case series of comparably ill
patients with H1N1 influenza who were treated
without ECMO, similar low mortality rates were
reported.16,17 Because these were uncontrolled case
series, and owing to the young age of patients reported
therein, it is not clear whether ECMO actually provided
a survival advantage in the setting of severe ARDS.
Because of the lack of strong evidence support-
ing the use of ECMO in severe ARDS, most patients
with severe ARDS at our institution, a high-volume
tertiary center, are treated without ECMO. In this
prospective cohort study, we report the demographic
and clinical features and clinical outcomes of patients
with severe ARDS who were treated without ECMO
despite meeting previously published criteria for
receiving it.6
Methods This prospective, observational study was con-
ducted at a single tertiary academic center. This study
was approved by the institutional review board at
Johns Hopkins University. We screened for eligible
patients each day by reviewing electronic medical
records of patients admitted to
the medical intensive care unit
from February 2014 to June 2015.
Patients were identified on the
basis of the Berlin definition of
severe ARDS.18 Patients with severe
ARDS were included in our cohort
if they met 1 of the following crite-
ria for ECMO consideration, which
were modified from Brodie and
Bacchetta6: (1) ratio of PaO2 to fraction of inspired
oxygen (FIO2) was less than 100 mm Hg despite
levels of positive end-expiratory pressure of at least
10 cm H2O for at least 6 hours; (2) uncompensated
About the AuthorsSarina K. Sahetya, Roy G. Brower, and R. Scott Stephens are physicians, Division of Pulmonary and Critical Care Medicine, Johns Hopkins University School of Medicine, Baltimore, Maryland.
Corresponding author: R. Scott Stephens, MD, Division of Pulmonary and Critical Care Medicine, Johns Hopkins University School of Medicine, 1830 Building, 5th Floor–Pulmonary, Baltimore, MD 21287 (e-mail: rsteph13 @jhmi.edu).
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 221
Despite its increasing use, the benefits of ECMO in ARDS have not been clearly established.

222 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
hypercapnia with acidemia (PCO2 > 50 mm Hg with
arterial pH < 7.15 or venous pH < 7.12); or (3) end-
inspiratory plateau pressure greater than 35 cm H2O
with either tidal volume no greater than 6 mL/kg
predicted body weight or with arterial pH less than
7.15.6,18 Eligibility criteria were confirmed by 2 of
the physician investigators. Time of enrollment
was defined as the time and date when criteria for
severe ARDS and ECMO eligibility first were met.
We additionally noted whether a contraindication to
ECMO was present, such as inability to receive anti-
coagulation (eg, because of intracranial hemorrhage,
major internal or gastrointestinal bleeding requiring
red blood cell transfusion within 7 days); high pres-
sure ventilation (plateau pressure > 30 cm H2O) for
longer than 7 days; high FIO2 (ie, FIO
2 > 0.80)
requirements for longer than 7 days; or any condi-
tion that would limit the likelihood of overall bene-
fit from ECMO (eg, severe neurologic dysfunction,
diffuse anoxic brain injury, end-stage lung disease
and not a transplant candidate, untreatable meta-
static cancer).6
For patients who met the study’s inclusion
criteria, we recorded the following data from
inclusion until time of discharge: ventilator set-
tings, laboratory results, length of stay, vital status
at hospital discharge, and use of adjunct therapies
such as prone positioning and neuromuscular
blockade. Comorbid conditions were defined as
the presence of 1 or more of the following chronic
medical conditions in the past year:
• Chronic lung disease (eg, use of home oxygen,
chronic hypercapnia [PaCO2 ≥ 50 mm Hg] severe pul-
monary hypertension [mean positive airway pres-
sure ≥ 40 mm Hg or New York Heart Association
class IV symptoms], chronic ventilator dependence);
• Chronic liver disease (ie, biopsy-proven cirrho-
sis, portal hypertension, hepatic failure based on
Child-Pugh score ≥ 10);
• Chronic renal disease requiring dialysis;
• Vasculitis;
• Sickle cell disease;
• malignant neoplasia (eg, leukemia, lym-
phoma, known metastatic cancer, or currently
receiving cancer treatment);
• AIDS;
• Receiving immunosuppressive therapy (eg,
treatment in the past year with agents such as aza-
thioprine, mycophenolate, tacrolimus, sirolimus,
cyclophosphamide, or corticosteroids [≥ 15 mg of
prednisone daily or equivalent for ≥ 20 days]); or
• Other conditions, such as Parkinson disease.
Severity of illness was assessed by using Acute Physi-
ology and Chronic Health Evaluation (APACHE) II
and Sequential Organ Failure Assessment scores.
We calculated the Respiratory ECMO Survival
Prediction (RESP) score19 for each patient to esti-
mate the probability of survival while receiving
ECMO had ECMO been used. The RESP score is a
validated model for predicting hospital survival for
respiratory failure based on patient and treatment
variables before ECMO is initiated.19
Descriptive statistics are reported as frequency
(percentage) for categorical variables and mean (stan-
dard deviation) or median (interquartile range [IQR])
for continuous variables. Statistical analyses were
conducted by using Stata, version 14 (StataCorp).
Results At the end of the 16-month screening period, 46
patients met criteria for severe ARDS and ECMO con-
sideration. Of these 46 patients, 5 (11%) actually
received rescue ECMO. These patients were younger,
more hypoxemic, and had fewer comorbid conditions
than the remaining 41 patients who did not receive
Table 1Demographics, clinical features, and outcomes of the 5 patients receiving ECMO
Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; ECMO, extracorporeal membrane oxygenation; FIO2, fraction of inspired oxygen; ICU, intensive care unit; IQR, interquartile range; PEEP, positive end-expiratory pressure; Pplat, plateau pressure; PBW, predicted body weight; RESP, Respiratory Extracor-poreal Membrane Oxygenation Survival Prediction; SOFA, Sequential Organ Fail-ure Assessment.
Characteristic
Age, mean (SD), y
APACHE II score, mean (SD)
SOFA score, mean (SD)
RESP score, median (IQR)
Pneumonia, No. (%) of patients
Lowest PaO2/FIO2, median (IQR)
Highest FIO2, mean (SD)
Highest PEEP, median (IQR), cm H2O
Highest Pplat, median (IQR), cm H2O
Highest PCO2, mean (SD), mm Hg
Lowest pH, mean (SD)
Lowest tidal volume, mL/kg PBW
Mechanical ventilation before ECMO, mean (SD), d
Adjunct therapies, No. (%) of patients Neuromuscular blockade Prone positioning
ICU length of stay, median (IQR), d
Hospital length of stay, median (IQR), d
Mortality, No. (%) of patients
29 (7)
21.6 (2.3)
12.6 (3.2)
0 (-1 to 1)
4 (80)
49 (41-50)
100 (0)
18 (16-20)
44 (41-46)
102.2 (29.3)
7.15 (0.10)
3.76 (0.70)
6.4 (2.9)
5 (100)4 (80)3 (60)
8 (5-10)
30 (16-33)
4 (80)
Patients receiving ECMO

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 223
ECMO (Table 1). The hospital discharge survival rate
of these 5 patients who received ECMO was 20%.
Of the 41 patients treated without ECMO, the
mean age was 52.6 (SD, 16.0) years, 19 patients
(46%) were female, and 37 patients (90%) had at
least 1 comorbidity. At day 1 of admission to the
intensive care unit, the mean APACHE II score was
28.3 (SD, 7.5), and the mean Sequential Organ Fail-
ure Assessment score was 12.6 (SD, 4.0) (Table 2).
Of the 41 patients, 16 patients had at least 1 contra-
indication to ECMO, which included an inability to
receive anticoagulation (7 patients) or a nonrecover-
able comorbidity (9 patients: 3 had anoxic brain
injury, 2 had metastatic cancer, and 4 had end-stage
lung disease and were not transplant candidates).
No patient had a contraindication due to receiving
ventilatory support for longer than 7 days. Of this
group with contraindications to ECMO, the survival
rate at time of hospital discharge was 25%.
The remaining 25 patients met criteria for ECMO
but did not receive it (see Figure). The mean age of
these 25 patients was 53.5 (SD, 14.3) years, 56%
were female, and 84% had at least 1 major comor-
bidity. The most common comorbidities were chronic
liver disease and chronic lung disease (Table 3). In
most of these patients, ARDS developed in associa-
tion with pneumonia (64%). The mean APACHE II
score was 28.9 (SD, 7.4) and the mean Sequential
Organ Failure Assessment score was 13.2 (SD, 3.6)
on the first day of admission to the intensive care
unit. The median lowest PaO2/FIO
2 ratio for this group
was 66 (IQR, 58-93) mm Hg, with a concomitant
median FIO2 of 0.90 (IQR, 70%-100%) and positive
end-expiratory pressure of 14 (IQR, 12-18) cm H2O.
Most patients (64%) met criteria for ECMO consid-
eration because of isolated severe hypoxemia rather
than uncompensated hypercapnia (16%) or exces-
sive inspiratory pressures (0%). Five patients (20%)
met more than 1 criterion, having severe hypoxemia
combined with either hypercapnia or excessive
Characteristic
Table 2Demographics and clinical features of patients in the intensive care unit who met the criteria for severe ARDS and ECMO consideration
Age, mean (SD), y
Female sex, No. (%) of patients
APACHE II score, mean (SD)
SOFA score, mean (SD)
RESP score, median (IQR)
Pneumonia, No. (%) of patients
Lowest Pao2/Fio2, median (IQR)
Highest Fio2, mean (SD)
Highest PEEP, median (IQR), cm H2O
Highest Pplat, median (IQR), cm H2O
Highest Pco2, mean (SD), mm Hg
Lowest pH, mean (SD)
Lowest tidal volume, mL/kg PBW
51.2 (18.9)
5 (31.2)
27.4 (7.3)
11.6 (46)
-1 (-4 to 2)
8 (50)
67.5 (49.5-75)
95 (70-100)
12 (10.5-16)
34.5 (30.5-36.5)
70.5 (24.5)
7.16 (0.10)
5.56 (0.62)
53.5 (14.3)
14 (56)
28.9 (7.4)
13.2 (3.6)
1 (-2 to 2)
16 (64)
66 (58-93)
90 (70-100)
14 (12-18)
32 (30-36)
61 (20)
7.16 (0.12)
5.32 (0.77)
52.6 (16.0)
19 (46)
28.3 (7.5)
12.6 (4.0)
0 (-2 to 2)
24 (59)
61 (51-91)
90 (70-100)
14 (11-16)
33 (30-36)
67.5 (22.5)
7.16 (0.11)
5.41 (0.72)
Contraindication to ECMO (n = 16)
Eligible for ECMO(n = 25)
All patientsa
(n = 41)
Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; ARDS, acute respiratory distress syndrome; ECMO, extracorporeal membrane oxygen-ation; FIO2, fraction of inspired oxygen; ICU, intensive care unit; IQR, interquartile range; PEEP, positive end-expiratory pressure; Pplat, plateau pressure; PBW, predicted body weight; RESP, Respiratory Extracorporeal Membrane Oxygenation Survival Prediction; SOFA, Sequential Organ Failure Assessment.a Includes all patients meeting criteria for severe ARDS and at least 1 criterion for ECMO consideration, subdivided into patients with a contraindication to
ECMO and patients who were eligible for ECMO but did not receive it. Specific demographics of the 5 patients who received ECMO are reported in Table 1.
Figure Flowchart of patients who met criteria for severe acute respiratory distress syndrome (ARDS) and extracorporeal mem-brane oxygenation (ECMO).
5 Patients received ECMO
46 Patients with severe ARDS met the ECMO criteria
25 Patients with no contraindication but did not receive ECMO
16 Patients with contraindication to ECMO

224 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
The predicted sur-vival rate with ECMO was 57%; the actual survival rate without
ECMO was 56%.
pressures. Most received lung protective ventilation
with a mean lowest tidal volume per kilogram of
predicted body weight of 5.3 (SD, 0.8). Two patients
who received tidal volumes greater than 6 mL/kg of
predicted body weight had isolated uncompensated
hypercapnia rather than severe
hypoxemia. Approximately one-
half of patients (48%) received
neuromuscular blockade, and 3
(12%) were placed in the prone
position. The median length of
stay in the intensive care unit was
13 (IQR, 9.5-26) days, and
median hospital stay was 21 (IQR,
13-35) days (Table 4). On the day
that the patient met the criteria for severe ARDS and at
least 1 criterion for ECMO, the median RESP score was
1 (IQR, -2 to 2), which corresponds to a predicted
survival rate while receiving ECMO of 57%.19 Our
group of 25 patients who met ECMO eligibility cri-
teria but did not receive ECMO had an actual sur-
vival rate of 56% at the time of hospital discharge.
Discussion Many institutions have developed ECMO pro-
grams for use in the treatment of severe ARDS
despite the lack of high-level evidence supporting
the assumption that the benefits of ECMO outweigh
the risks. With this prospective observational cohort
study, we sought to characterize the features and
outcomes of patients with severe ARDS who might
have received ECMO at other institutions but did not
receive ECMO at our hospital. To our knowledge, no
other prospective studies have been done to assess
the outcomes of patients with ARDS who met crite-
ria to receive ECMO but did not receive it.
Our data support several key conclusions. First,
the unselected population arriving in our tertiary
medical intensive care unit with severe ARDS is older
and has more comorbidities and higher illness sever-
ity scores than did the patients reported in prior case
series describing low mortality rates with the use of
ECMO for H1N1 influenza–related severe ARDS.9-12
Patients in these case series were relatively young,
lacked substantial comorbid conditions, and
potentially would have survived without ECMO.
In other case series evaluating outcomes in criti-
cally ill patients with H1N1 influenza, researchers
reported comparably low mortality rates when ECMO
was not used.16,17 In contrast, very few of our patients
with severe ARDS were young and had isolated
respiratory failure. A strength of our study is that
all critically ill patients with ARDS severe enough
to meet the criteria for ECMO consideration were
Characteristic
Table 3Comorbid conditions of patients in the intensive care unit meeting the criteria for severe acute respiratory distress syndrome (ARDS) and consideration for extracorporeal membrane oxygenation (ECMO)
None
Chronic liver diseaseb
Chronic lung diseasec
Chronic dialysis
Malignant neoplasiad
AIDS
Immunosuppressione
Sickle cell disease
Vasculitis
Otherf
0 (0)
5 (31)
6 (38)
1 (6)
2 (12)
0 (0)
1 (6)
1 (6)
0 (0)
1 (6)
4 (16)
12 (48)
6 (24)
2 (8)
1 (4)
4 (16)
4 (16)
1 (4)
1 (4)
0 (0)
4 (10)
17 (41)
12 (29)
3 (7)
3 (7)
4 (10)
5 (12)
2 (5)
1 (2)
1 (2)
Contraindication to ECMO (n = 16)
Eligible for ECMO(n = 25)
No. (%) of patients
All patientsa
(n = 41)
a Includes all patients meeting criteria for severe ARDS and at least 1 criterion for ECMO consideration, subdivided into patients with a contraindication to ECMO and patients who were eligible for ECMO but did not receive it. Specific demographics of the 5 patients who received ECMO are reported in Table 1.
b Biopsy-proven cirrhosis, portal hypertension, hepatic failure based on Child-Pugh score 10.c Use of home oxygen, chronic hypercapnia PaCO2 50 mm Hg, severe pulmonary hypertension (mean pulmonary artery pressure 40 mm Hg or New York Heart
Association class IV symptoms), chronic ventilator dependence.d Leukemia, lymphoma, solid tumor currently receiving cancer treatment, or known metastatic cancer.e Treatment in the past year with immunosuppressive agents such as azathioprine, mycophenolate, tacrolimus, sirolimus, cyclophosphamide, or corticosteroids
( 15 mg of prednisone daily or equivalent for at least 20 days).f Parkinson disease.

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 225
included prospectively. As a result, our cohort was
substantially older, with more organ failures, and
was most likely more representative of a general
population with severe ARDS (Table 5).
Second, although the overall survival rate in the
cohort without ECMO in our study was 44%, which
compares unfavorably with published series of ECMO
in severe ARDS, more than one-third of our patients
with severe ARDS would have been considered ineli-
gible for ECMO owing to a contraindication such as
an inability to receive anticoagulation or a condition
that severely limited the likelihood of benefit from
ECMO (eg, metastatic cancer, anoxic brain injury).
This is a key finding, suggesting that many patients
with severe ARDS may not even be eligible for ECMO
support. Notably, these possibly ineligible patients
had a hospital survival rate of only 25%, which was
substantially lower than the survival rate of patients
without contraindications to ECMO. This low sur-
vival rate is not surprising, because the conditions
that make patients ineligible for ECMO, such as
cerebral hemorrhage, life-threatening bleeding, and
end-stage lung disease, frequently portend poor
prognoses regardless of the treatment strategy. Indeed,
in a recent retrospective analysis of patients with
interstitial lung disease treated with ECMO for acute
respiratory failure, authors reported a 7% survival rate
in those who did not qualify for lung transplant.20
Finally, among the patients who would have been
eligible but did not receive ECMO, we report a survival
Characteristic
Table 4Clinical course and survival rates at time of hospital discharge of patients in the intensive care unit meeting criteria for severe ARDS and ECMO consideration
Adjunct therapies, No. (%) of patients Neuromuscular blockade Prone positioning
ICU length of stay, median (IQR), d
Hospital length of stay, median (IQR), d
Survival, No. (%) of patients
5 (31) 5 (31)1 (6)
20 (6-33)
22 (14.5-43)
4 (25)
12 (48)12 (48) 3 (12)
13 (9.5-26)
21 (13-35)
14 (56)
17 (41)17 (41) 4 (10)
17.5 (7.5-27)
21 (13-35)
18 (44)
Contraindication to ECMO (n = 16)
Eligible for ECMO(n = 25)
All patientsa
(n = 41)
Abbreviations: ARDS, acute respiratory distress syndrome; ECMO, extracorporeal membrane oxygenation; IQR, interquartile range.a Includes all patients meeting criteria for severe ARDS and at least 1 criterion for ECMO consideration, subdivided into patients with a contraindication to
ECMO and patients who were eligible for ECMO but did not receive it. Specific demographics of the 5 patients who received ECMO are reported in Table 1.
Reference
Table 5Comparison of demographics and mortality from severe ARDS in previously published case series
Davies et al9: Australia, New Zealand
Patroniti et al10: Italy
Noah et al11: United Kingdom
Pham et al12: France
Kumar et al17: Canada
Miller et al16: Utah
Peek et al7: CESAR intervention group
Peek et al7: CESAR, control group
Schmidt et al19: ELSO database
Johns Hopkinsa
23
29
28
36
17.3
27
37
45
43
44
56
63
55
59
147
61
75.9
75
NR
66
NR
NR
NR
NR
19.7
25
19.7
19.9
NR
28.9
NR
7
9
9.5
6.8
7
NR
NR
NR
13.2
36
39
34
42
32
34
39.9
40.4
41
53.5
Yes
Yes
Yes
Yes
Yes
Yes
No
No
No
No
100
100
86.3
100
4.2
0
75
0
100
0
68
49
80
123
168
47
90
90
2355
25
Mortality, %PaO2/FIO2
APACHE II score
SOFA score
Age, mean, y
H1N1 influenzaN
ECMO received, %
Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; ARDS, acute respiratory distress syndrome; CESAR, conventional ventilatory support vs extracorporeal membrane oxygenation for severe adult respiratory failure; ELSO, Extracorporeal Life Support Organization; ECMO, extracorporeal membrane oxygenation; FIO2, fraction of inspired oxygen; NR, not reported; SOFA, Sequential Organ Failure Assessment.a Data reported here include the 25 patients who were eligible for ECMO but did not receive it, that is, patients with severe ARDS who met at least 1 ECMO
criterion and did not have a contraindication to ECMO.

226 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
Actual survival rates without ECMO
were similar to pre-dicted survival
rates with ECMO.
rate of 56%. This study was not a randomized trial;
therefore, we cannot directly compare this survival
rate with the survival rate obtained in patients receiv-
ing ECMO. However, to compensate for this limita-
tion, we calculated the RESP score for each patient
at the time they met the criteria for ECMO consider-
ation to estimate the predicted survival for our
patients had they received ECMO. Based on the
RESP score, predicted survival for our cohort receiv-
ing ECMO was 57%, indicat-
ing that the outcomes without
ECMO are similar to the out-
comes predicted for patients
who received ECMO. Moreover,
the survival rate of 56% deter-
mined in this study is similar
to the survival rate reported in
multiple clinical studies and
the Extracorporeal Life Support
Organization database (Table 5). Although caution
should be applied to any conclusions drawn from
this observational series, we suggest, on the basis
of the data, that the survival rate of patients with
severe ARDS treated without ECMO may be similar
to the survival rate of patients with severe ARDS who
receive ECMO.
Our institution is a high-volume center for treat-
ment of ARDS and use of ECMO. In the calendar
year 2016, more than 60 patients were treated with
ECMO. However, we use ECMO primarily for patients
after cardiotomy or who are experiencing cardiogenic
shock. In our medical intensive care unit, patients with
severe ARDS are typically treated with lung protective
ventilation, antibiotics for infections, conservative
fluid management, adjuncts such as neuromuscular
blockade and prone positioning, and supportive
care strategies. Fewer than half of the patients with
severe ARDS in the present study were treated with
neuromuscular blockade, and less than 10% were
treated with prone positioning, perhaps because
the implementation of these interventions took
time after their use was supported by findings in
landmark publications.21,22 Our implementation
rates of these adjunct therapies are similar to imple-
mentation rates across the world in 2016, as identi-
fied in the Large Observational Study to Understand
the Global Impact of Severe Acute Respiratory Fail-
ure (LUNG-SAFE) study.15 Furthermore, had these
proven therapies been used more widely, it is possi-
ble that our outcomes without ECMO would have
been even better.
This study has several limitations. Although data
were collected prospectively to capture all patients
who met the criteria for ECMO consideration, this is
an observational study of only 46 patients. As such,
no attempt was made to randomly assign patients
to receive ECMO or usual care. Most other ECMO
case series and case-control series are from the H1N1
influenza population; thus, it is difficult to draw
comparisons to our study. In addition, the RESP
score was developed on the basis of patients who
received ECMO, even though only pre-ECMO vari-
ables were included in the model. This score has
not been validated for patients who did not receive
ECMO, although it does appear to be a relevant
instrument for predicting survival in patients receiv-
ing ECMO for severe acute respiratory failure.
Finally, 5 patients in our sample did receive
ECMO. These patients were substantially younger,
but they had more severely impaired gas exchange
(mean PaO2/FIO
2 ratio, 52.6 mm Hg; PCO
2, 102.2
mm Hg), worse respiratory mechanics (median pla-
teau pressure, 44 [IQR, 41-46] cm H2O; mean tidal
volume, 3.76 [SD, 0.70] mL/kg predicted body
weight), and adjunctive therapies. The mortality rate
for the patients receiving ECMO was 80%, which is
higher than mortality rates reported for prior ECMO
series (see Table 5). In all 5 patients, ECMO was
offered as a late salvage therapy by the clinical team
caring for them. Three of the patients who received
ECMO had received mechanical ventilatory support
for at least 7 days, which could have been considered
a contraindication to ECMO.6 The high mortality rate
of these patients further emphasizes the need to iden-
tify the appropriate patient population for ECMO.
Conclusions The general patient population with severe ARDS
in this study was older and had more comorbid con-
ditions than the patient populations in many of the
case reports of favorable outcomes of severe ARDS
treated with ECMO. The reports of low mortality
rates in those case series could be attributable to the
patients’ young age and lack of comorbid conditions
rather than to the use of ECMO. Almost all of our
institution’s patients with severe ARDS were treated
medically, even if they were eligible for ECMO. Their
actual survival rate without ECMO was similar to their
predicted survival rates with ECMO. A new random-
ized controlled trial evaluating ECMO versus con-
ventional management for severe ARDS is currently
enrolling patients (ClinicalTrials.gov identifier:
NCT01470703). However, until reduced mortality
with ECMO is demonstrated in patients with acute
respiratory failure in future randomized controlled
trials, we suggest, on the basis of our results, that it

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 227
is reasonable to treat patients with severe ARDS with
usual best-care clinical practices without ECMO.
ACKNOWLEDGMENTSWe thank Bernice Frimpong and Karen Oakjones- Burgess for invaluable assistance with screening and data management.
FINANCIAL DISCLOSURESThis research was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health (Award T32HL007534).
SEE ALSO For more about ECMO, visit the Critical Care Nurse web-site, www.ccnonline.org, and read the Cochrane Review Summary by Sandoval, “Extracorporeal Membrane Oxygenation for Critically Ill Adults” (December 2016).
REFERENCES 1. Ventetuolo CE, Muratore CS. Extracorporeal life support in
critically ill adults. Am J Respir Crit Care Med. 2014; 190(5): 497-508.
2. Combes A, Leprince P, Luyt C-E, et al. Outcomes and long-term quality-of-life of patients supported by extracorporeal membrane oxygenation for refractory cardiogenic shock. Crit Care Med. 2008;36(5):1404-1411.
3. Brogan TV, Thiagarajan RR, Rycus PT, Bartlett RH, Bratton SL. Extracorporeal membrane oxygenation in adults with severe respiratory failure: a multi-center database. Inten-sive Care Med. 2009;35(12):2105-2114.
4. Zapol WM, Snider MT, Hill J, et al. Extracorporeal membrane oxygenation in severe acute respiratory failure: a random-ized prospective study. JAMA. 1979;242(20):2193-2196.
5. Morris AH, Wallace CJ, Menlove RL, et al. Randomized clini-cal trial of pressure-controlled inverse ratio ventilation and extracorporeal CO2 removal for adult respiratory distress syndrome. Am J Respir Crit Care Med. 1994;149(2):295-305.
6. Brodie D, Bacchetta M. Extracorporeal membrane oxygenation for ARDS in adults. N Engl J Med. 2011;365(20):1905-1914.
7. Peek GJ, Mugford M, Tiruvoipati R, et al. Efficacy and eco-nomic assessment of conventional ventilatory support ver-sus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised con-trolled trial. Lancet. 2009;374(9698):1351-1363.
8. Kahn JM, Goss CH, Heagerty PJ, Kramer AA, O’Brien CR, Rubenfeld GD. Hospital volume and the outcomes of mechanical ventilation. N Engl J Med. 2006;355(1):41-50.
9. Davies A, Jones D, Bailey M, et al. Extracorporeal mem-brane oxygenation for 2009 influenza A(H1N1) acute respi-ratory distress syndrome. JAMA. 2009;302(17):1888-1895.
10. Patroniti N, Zangrillo A, Pappalardo F, et al. The Italian ECMO network experience during the 2009 influenza A(H1N1) pan-demic: preparation for severe respiratory emergency out-breaks. Intensive Care Med. 2011;37(9):1447-1457.
11. Noah MA, Peek GJ, Finney SJ, et al. Referral to an extracor-poreal membrane oxygenation center and mortality among patients with severe 2009 influenza A(H1N1). JAMA. 2011; 306(15): 1659-1668.
12. Pham T, Combes A, Rozé H, et al. Extracorporeal membrane oxygenation for pandemic influenza A(H1N1)–induced acute respiratory distress syndrome. Am J Respir Crit Care Med. 2013;187(3):276-285.
13. Zangrillo A, Biondi-Zoccai G, Landoni G, et al. Extracorporeal membrane oxygenation (ECMO) in patients with H1N1 influenza infection: a systematic review and meta-analysis including 8 studies and 266 patients receiving ECMO. Crit Care. 2013;17(1):R30.
14. Rubenfeld GD, Caldwell E, Peabody E, et al. Incidence and outcomes of acute lung injury. N Engl J Med. 2005; 353(16): 1685-1693.
15. Bellani G, Laffey JG, Pham T, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315(8):788-800.
16. Miller RR III, Markewitz BA, Rolfs RT, et al. Clinical findings and demographic factors associated with ICU admission in utah due to novel 2009 influenza A(H1N1) infection. Chest. 2010;137(4):752-758.
17. Kumar A, Zarychanski R, Pinto R, et al. Critically ill patients with 2009 influenza A(H1N1) infection in Canada. JAMA. 2009; 302(17):1872-1879.
18. Force ADT, Ranieri VM, Rubenfeld GD, et al. Acute respira-tory distress syndrome: the Berlin definition. JAMA. 2012; 307(23):2526-2533.
19. Schmidt M, Bailey M, Sheldrake J, et al. Predicting survival after extracorporeal membrane oxygenation for severe acute respiratory failure. The Respiratory Extracorporeal Membrane Oxygenation Survival Prediction (RESP) score. Am J Respir Crit Care Med. 2014;189(11):1374-1382.
20. Trudzinski FC, Kaestner F, Schäfers H-J, et al. Outcome of patients with interstitial lung disease treated with extracor-poreal membrane oxygenation for acute respiratory failure. Am J Respir Crit Care Med. 2015;193(5):527-533.
21. Guerin C, Reignier J, Richard JC, et al. Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368(23):2159-2168.
22. Papazian L, Forel JM, Gacouin A, et al. Neuromuscular block-ers in early acute respiratory distress syndrome. N Engl J Med. 2010;363(12):1107-1116.
To purchase electronic or print reprints, contact American Association of Critical-Care Nurses, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; email, [email protected].

Cardiovascular Critical Care
©2018 American Association of Critical-Care Nursesdoi:https://doi.org/10.4037/ajcc2018867
Background Intravenous fluid boluses are administered to patients in shock to improve tissue hypoperfusion. However, fluid boluses result in clinically significant stroke volume increases in only about 50% of patients. Hemodynamic responses to passive leg raising mea-sured with invasive and minimally invasive methods are accurate predictors of fluid responsiveness. However, few studies have used noninvasive blood pressure mea-surement to evaluate responses to passive leg raising.Objective To determine if passive leg raising–induced increases in pulse pressure or systolic blood pressure can be used to predict clinically significant increases in stroke volume index in healthy volunteers. Methods In a repeated-measures study, hemodynamic measurements were obtained in 30 healthy volunteers before, during, and after passive leg raising. Each partici-pant underwent the procedure twice.Results In the first test, 20 participants (69%) were respon-ders (stroke volume index increased by ≥ 15%); 9 (31%) were nonresponders. In the second test, 15 participants (50%) were responders and 15 (50%) were nonresponders. A passive leg raising–induced increase in pulse pressure of 9% or more predicted a 15% increase in stroke volume index (sensitivity, 50%; specificity, 44%). There was no association between passive leg raising–induced changes in systolic blood pressure and fluid responsiveness.Conclusion A passive leg raising–induced change in stroke volume index measured by bioreactance differenti-ated fluid responders and nonresponders. Pulse pressure and systolic blood pressure measured by oscillometric noninvasive blood pressure monitoring were not sensi-tive or specific predictors of fluid responsiveness in healthy volunteers. (American Journal of Critical Care. 2018; 27:228-237)
NONINVASIVE BLOOD PRESSURE MONITORING
AND PREDICTION OF FLUID
RESPONSIVENESS TO
PASSIVE LEG RAISINGBy Joya D. Pickett, RN, PhD, ARNP-CNS, CCNS, ACNS-BC, CCRN, Elizabeth Bridges, RN,
PhD, CCNS, Patricia A. Kritek, MD, EdM, and JoAnne D. Whitney, RN, PhD, CWCN
228 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 229
Static parameters such as central venous pressure are not predictive of fluid responsiveness.
Administration of intravenous fluid boluses is often one of the first interventions considered for patients in shock with signs of hypoperfusion.1-4 However, only about 50% of patients respond to fluid administration with a clinically significant (10%-15%) increase in stroke volume (SV) or stroke volume index (SVI).5-12 Administration of fluids to patients whose SV does not improve may exacerbate
pulmonary edema, precipitate respiratory failure, and prolong mechanical ventilation.12-15 Alternatively, undertreated hypovolemia may lead to inappropriate use of vasopressors and exacerbate organ hypoperfusion and ischemia.12 To avoid the deleterious effects associated with fluid overload and undertreated hypovolemia, it is important to predict which patients’ SV will increase in response to fluid administration.3,12
Traditionally, static parameters such as central
venous pressure have been used to guide fluid admin-
istration, but these parameters do not predict fluid
responsiveness.3,12,16,17 Dynamic parameters, such as
pulse pressure (PP) variation measured from an
arterial catheter, are highly predictive of response
to a fluid bolus.12,18,19 However, these indices can
be used only in patients who are fully supported
with mechanical ventilation and receiving ade-
quate tidal volumes (8 mL/kg) or patients without
cardiac arrhythmias.18
Passive leg raising (PLR) is a reliable alternative
method to predict fluid responsiveness in patients
who are spontaneously breathing, are receiving
mechanical ventilation, or have cardiac arrhyth-
mias.20 Semirecumbent PLR is performed by lifting
the legs to a 45° angle while lowering the head and
upper trunk from a 45° semirecumbent position to
the supine (flat) position.21 PLR causes a transient,
reversible autotransfusion, temporarily increasing
preload and thus mimicking a fluid bolus.13,22-24 The
PLR-induced increase in preload will induce a
clinically significant increase in SV if both the right
and left ventricles are functioning on the ascending
portion of the Frank-Starling curve.12 If a patient
responds to PLR with an increase in SV or its surro-
gates, the patient would most likely respond to a
fluid bolus.
Rapid fluid administration is recommended
during the first few hours after onset of symptoms in
patients with sepsis and septic shock.1,2,4 PLR-induced
changes in SV, PP, and systolic blood pressure (SBP)
measured with direct arterial monitoring are accurate
indicators of fluid responsiveness.6,8,20,23,25 However,
these parameters require invasive
monitoring. Oscillometric nonin-
vasive blood pressure (NIBP)
monitoring is readily available at
the bedside and is often the initial
method used to measure the
response to fluid administration.
In only 1 previous study have
PLR-induced changes in PP and
SBP as determined by NIBP moni-
toring been evaluated.9 However, the study included
central intravenous catheter placement, which may
delay initial treatment. The purpose of our study was
to determine if PLR-induced changes in PP and SBP
measured by oscillometric NIBP monitoring are sen-
sitive and specific indicators of a clinically significant
increase in SVI in healthy volunteers.
Methods Design
The study was a single-group repeated-measures
design. We measured the following parameters
noninvasively before, during, and after PLR: SBP,
diastolic blood pressure (DBP), mean arterial pres-
sure (MAP), heart rate, SVI, and cardiac index. We
repeated PLR with the same participants after a
5-minute washout period.
SampleWe enrolled a convenience sample of 30 vol-
unteers who reported no major health problems
About the AuthorsJoya D. Pickett is a critical care clinical nurse specialist at Swedish Medical Center, Seattle, Washington. Elizabeth Bridges is a professor at University of Washington School of Nursing and a clinical nurse researcher at University of Washington Medical Center, University of Washington Medicine, Seattle, Washington. Patricia A. Kritek is medi-cal director of critical care and an associate professor in the Division of Pulmonary and Critical Care Medicine at University of Washington Medical Center. JoAnne D. Whitney is a professor at the University of Washington School of Nursing and endowed professor in critical care nursing at Harborview Medical Center, University of Washington Medicine.
Corresponding author: Joya D. Pickett, Swedish Medical Center, 747 Broadway, Seattle, WA 98122 (email: [email protected]).

230 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
SVI was measured by using a noninva-
sive continuous car-diac monitoring
system that uses bio-reactance technology.
(Figure 1). We included or excluded candidates on
the basis of their responses to a health history ques-
tionnaire. Candidates included were aged 18 years
or older and had a regular pulse rhythm, pulse rate
of 60/min to 120/min, and SBP of 90 to 160 mm
Hg. Exclusion criteria were self-reported history of
pulmonary edema, mitral or
aortic stenosis, cardiac dysrhyth-
mias, peripheral vascular disease,
musculoskeletal deformities (eg,
limb amputations), implanted
devices (eg, pacemakers), preg-
nancy, and inability to lie fl at
with the legs elevated.
For the power analysis, we
used the results of a meta-
analysis of PLR-induced changes
in radial artery PP to predict
fl uid responsiveness.20 With an level of .05 and
level of .80, a sample size of 30 participants would
provide ± 15% precision in measurement of the
response to PLR.
Variables and Measurement InstrumentsBlood Pressure Measurements. We measured SBP,
DBP, MAP, and heart rate from the brachial artery
by using oscillometric NIBP monitoring (Critikon
Dinamap, GE Healthcare). Oscillometric NIBP
monitoring is accurate in a wide variety of clinical
situations.26 We used appropriately sized adult (arm
circumference 27-34 cm) and extra large (arm circum-
ference > 45 cm) blood pressure (BP) cuffs.
Stroke Volume Index. We measured SVI with a
noninvasive continuous cardiac output monitoring
system that uses bioreactance technology (NICOM,
Cheetah Medical).5 This system involves 4 electrodes
placed on the thorax. An alternating electric current
is passed between the outer pair of electrodes, and
the resulting voltage signal is sensed by the inner pair
of electrodes. Comparison of phase shifts between
the current and the voltage signal provides an instan-
taneous recording that is proportional to aortic blood
fl ow. The frequency shift is used to determine the SVI.
The signal is averaged every 10 seconds and recorded
as a digital display.5
The accuracy of this monitoring system has been
demonstrated in various patient populations. Accord-
ing to Critchley and Critchley,27 acceptance of a new
technique should require a limit of agreement of up
to 30% between 2 devices. A study of cardiac output
monitoring in 110 critically ill patients revealed an
error rate of 9% to 20% (depending on whether
cardiac output was stable or increasing) between
continuous measurement with the noninvasive
bioreactance device and measurement with ther-
modilution via a pulmonary artery catheter.28
Procedure We obtained approval from our institution’s
Human Subjects Division. Participants gave consent,
and we conducted the study in accordance with the
ethical standards of the Declaration of Helsinki.
Before each test, the noninvasive cardiac output
monitoring system underwent internal calibration.
We prepared the skin on each participant’s anterior
chest and abdomen according to the monitoring
system manufacturer’s instructions. We placed elec-
trodes on the thorax (2 on the shoulders, 2 on the
abdomen). We obtained NIBP measurements in
each arm and used the reading from the arm with
the highest SBP.29 We positioned the arm at the
level of the phlebostatic axis.30
The procedure began after the participant had
undergone a 10-minute stabilization period in the
baseline position (supine with the backrest elevated
45° by a wedge pillow and legs horizontal on the
bed). We then moved the participant into the PLR
position by removing the wedge pillow from the
upper torso and lowering the head and torso to hori-
zontal while simultaneously elevating the legs to a
45° angle with the support of the wedge pillow. We
Figure 1 CONSORT diagram representing the study enrollment and description of participants.
Assessed for study eligibility
N = 31
Total participants N = 30
Test A: n = 29(1 participant’s sensor
detached)
Responders n = 20
Nonresponders n = 9
Excluded n = 1
Test B: n = 30 (All participants repeated
and completed test)
Responders n = 15
Nonrespondersn = 15

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 231
Figure 2 Diagram of procedure for passive leg raising.
Abbreviations: HOB, head of bed; PLR, passive leg raise.
3 min 3 min 3 min 5-min washout
Baseline During PLR After PLR
HOB45°
Legs45°
HOB45°
Characteristic
Table 1Characteristics of study participants
40 (14)35 (13)
12 (63) 7 (37)
3 (27) 8 (73)
67 (4)69 (3)
178 (51)184 (42)
1.90 (0.24)1.98 (0.22)
38 (14)38 (15)
11 (61) 7 (39)
9 (82) 2 (18)
68 (3)68 (4)
185 (42)163 (45)
1.96 (0.19)1.86 (0.29)
Age, mean (SD), y Responder Nonresponder
Sex, No. (%) Female, 19 (63) Responder Nonresponder Male, 11 (37) Responder Nonresponder
Height, mean (SD), in Responder Nonresponder
Weight, mean (SD), lb Responder Nonresponder
Body surface area, mean (SD), m2
Responder Nonresponder
Test B (n = 30) Test A (n = 29)
SI conversion factors: To convert height to centimeters, multiply by 2.54; to convert weight to kilograms, multiply by 0.45.
activated the NIBP readings immediately after plac-
ing the participant in this position. After the
3-minute PLR procedure was complete, we returned
the participant to the baseline position. The partici-
pant walked in place for a washout period of 5 min-
utes. We then repeated the procedure, designating the
first procedure as test A and the second as test B (Fig-
ure 2). Hemodynamic measurements were obtained
at baseline, immediately after the participant was
placed in the PLR position, and after the PLR proce-
dure. During each phase we took 3 measurements
at approximately 1 minute, 1 minute 40 seconds,
and 2 minutes 20 seconds.
Statistical Analysis We used descriptive statistics to summarize
the sample demographics. Continuous data were
expressed as means (SD). On the basis of a litera-
ture review, we classified each participant a priori
as a fluid responder if the SVI increased by 15% or
more in response to PLR.3,20,22 If the PLR-induced
change in SVI was less than 15%, we classified the
participant as a fluid nonresponder. We calculated
the PLR-induced increase in SVI according to the
proprietary protocol of the noninvasive continuous
cardiac output monitoring device.
We used the mean and standard deviation of
3 repeated measurements to calculate the variables
(eg, PP, SBP, heart rate). The PP was calculated by
subtracting DBP from SBP. We used paired t tests to
compare hemodynamic measurements before and
after the PLR procedure. We used the independent
t test to compare the measurements of responders
and nonresponders. We used the 2 statistic to com-
pare responders and nonresponders according to
SVI, PP, and SBP.
We analyzed the sensitivity and specificity of
PLR-induced changes by using cutoff values based
on a priori studies of fluid responsiveness: PP change
of 9% or greater20 and SBP change of 9% or greater.9
We also evaluated post hoc cutoff values by using
the Youden index, a statistic used to weigh the pro-
portion of false-positive and false-negative results
to identify the optimum cutoff point.31 We analyzed
the data with statistics software (SPSS version 19,
IBM). All tests of significance were 2-tailed, and we
set the level of significance at .05.
Results Sample
We enrolled 30 healthy volunteers who met the
inclusion criteria. All participants completed the study
without complication. We excluded 1 potential
participant from the study because of an implanted
device. In test A, 1 participant’s noninvasive cardiac
output monitoring sensor detached and the response
to PLR could not be measured. The baseline charac-
teristics of responders and nonresponders were not
significantly different (Table 1).
PLR-Induced Changes in SVI Of 29 participants in test A, 20 (69%) were
responders and 9 (31%) were nonresponders. Of 30
participants in test B, 15 (50%) were responders and
15 (50%) were nonresponders. In test A, the mean
(SD) PLR-induced change in SVI was 26% (10%) in
responders and 7% (6%) in nonresponders (P < .001).
The results of test B were similar. Tables 2 and 3 show
the hemodynamic variables of responders and non-
responders in tests A and B.

232 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
Prediction of Fluid Responsiveness: PP In test A, the PLR-induced change in PP was not
significantly different between responders and non-
responders (mean [SD]: responders, 9% [11%]; non-
responders, 8% [11%]; P = .90). However, in responders
the PLR-induced absolute increase in PP was signifi-
cantly higher than the baseline PP (mean [SD]: base-
line, 47 [11] mm Hg; during PLR, 51 [13] mm Hg;
P < .001). SVI increased in all but 1 participant. How-
ever, the association between the change in PP and
change in SVI was not significant (r = 0.03, P = .88).
Using the a priori threshold of a 9% or greater
change in PP, we calculated that the sensitivity of
the PLR-induced increase in PP in test A was 50%
(95% CI, 27%-73%) and specificity was 44% (95%
CI, 14%-79%). The area under the curve was 0.49
(95% CI, 0.25-0.74; P = .96), indicating that the
PLR-induced change in PP did not differentiate
between responders and nonresponders. Analysis
using the Youden index cutoff of 6% yielded a
sensitivity of 70% and a specificity of 44%. We
found similar results in test B (Table 4). Analysis
using the a priori threshold of a 9% or greater
increase in PP yielded a sensitivity of 47% and a
specificity of 67%. Using the Youden index cutoff of
2% revealed a sensitivity of 60% and a specificity of
46%. The PLR-induced changes in SVI and PP were
not associated (r = 0.10, P = .61).
Prediction of Fluid Responsiveness: SBP In both tests, SBP decreased from baseline
values in both responders and nonresponders. The
PLR-induced changes in SBP were similar in test A
(mean [SD]: responders, −4% [4%]; nonrespond-
ers, −4% [6%]; P = .99) and test B (mean [SD]:
responders, −4% [4%]; nonresponders, −6 %
[4%]; P = .12). The PLR-induced increase in SVI
and the change in SBP were not associated in test
A (r = 0.12, P = .53) or in test B (r = 0.23, P = .17).
Figure 3 depicts test A results.
Variable
Table 2Hemodynamic variables of participants classified as responders (n = 20) and nonresponders (n = 9) in test Aa
Heart rate, beats per minute Responder Nonresponder
Systolic blood pressure, mm Hg Responder Nonresponder
Diastolic blood pressure, mm Hg Responder Nonresponder
Mean arterial pressure, mm Hg Responder Nonresponder
Pulse pressure, mm Hg Responder Nonresponder
Cardiac indexe
Responder Nonresponder
Stroke volume indexh
Responder Nonresponder
69 (9)64 (11)
114 (16)115 (16)
68 (8)71 (9)
84 (10)87 (10)
47 (11)44 (12)
3.4 (0.60)3.6 (0.38)
53 (8) 57 (11)
-1 (7)-1 (7)
-4 (4)-4 (6)
-12 (6)-13 (6)
-12 (6)-11 (6)
9 (11)8 (11)
26 (12)g
7 (6)
26 (10)g
7 (6)
69 (10)64 (11)
113 (18)111 (15)
66 (7)69 (8)c
84 (10)84 (12)d
47 (13)43 (11)
3.8 (0.64)f
5.0 (4.0)
55 (9) 59 (12)
68 (10)63 (12)
109 (17)b
109 (15)
58 (6)b
62 (11)b
74 (10)b
77 (13)b
51 (13)b
47 (11)
4.3 (0.64)b
3.9 (0.47)
63 (10)i 62 (14)
Baseline During PLR After PLR % Change in response
to PLR
Abbreviation: PLR, passive leg raising. a Data are expressed as mean (SD).b During PLR versus baseline: P = .001. c After PLR versus baseline: P = .04.d After PLR versus baseline: P = .05.e Calculated as cardiac output in liters per minute divided by body surface area in square meters.f After PLR versus baseline: P = .003.g Responder versus nonresponder: P < .001.h Calculated as stroke volume in milliliters per beat divided by body surface area in square meters.i During PLR versus baseline: P = .002.

www.ajcconline.org
Table 4Accuracy of pulse pressure for evaluating noninvasive blood pressure measurements of the response to passive leg raising
Statistic
0.61
9
47
67
1.40
0.80
58
56
0.49
9
50
44
0.90
1.12
67
29
Area under curve
Cutoff, %
Sensitivity, %
Specificity, %
Positive likelihood ratio
Negative likelihood ratio
Positive predictive value, %
Negative predictive value, %
Test B Test A
% Change in pulse pressure
Using the a priori threshold of a 9% or greater
PLR-induced increase in SBP, we calculated that the
change in SBP was not predictive of fluid responsive-
ness (area under the curve, 0.42; 95% CI, 0.18-0.66;
P = .48). Test B yielded similar results.
PLR-Induced Changes in Other Hemodynamic Variables
The responses of other hemodynamic variables
are summarized in Tables 2 and 3. The only signifi-
cant change was in the cardiac index. In both test A
and test B, the PLR-induced increase in cardiac index
in responders was significantly higher than in non-
responders (P < .001).
Variable
Table 3Hemodynamic variables of participants classified as responders (n = 15) and nonresponders (n = 15) in test Ba
Heart rate, beats per minute Responder Nonresponder
Systolic blood pressure, mm Hg Responder Nonresponder
Diastolic blood pressure, mm Hg Responder Nonresponder
Mean arterial pressure, mm Hg Responder Nonresponder
Pulse pressure, mm Hg Responder Nonresponder
Cardiac indexi
Responder Nonresponder
Stroke volume indexm
Responder Nonresponder
69 (13) 64 (9)
109 (12)c
122 (17)
65 (7) 69 (7)
81 (8)f
88 (10)
44 (10)g
53 (13)
3.3 (0.80)3.9 (0.46)
47 (9)n
59 (11)
71 (13)66 (10)b
109 (12)f
121 (17)
65 (6)70 (8)
81 (9)88 (11)
44 (10)52 (14)
3.6 (0.81)k
3.8 (0.47)
52 (11)o 58 (11)
68 (11)64 (9)
105 (12)d
114 (15)e
58 (5)d
60 (9)d
73 (6)d
78 (11)d
47 (10)h 53 (11)
4.1 (0.82)j
4.0 (0.43)
61 (12)d
63 (11)
Baseline During PLR After PLR % Change in response
to PLR
Abbreviation: PLR, passive leg raising.a Data are expressed as mean (SD). b After PLR versus baseline: P = .045.c Responder versus nonresponder: P = .03. d During PLR versus baseline: P = .001. e During PLR versus baseline: P < .001.f Responder versus nonresponder: P = .04. g Responder versus nonresponder: P = .05. h During PLR versus baseline: P = .04.i Calculated as cardiac output in liters per minute divided by body surface area in square meters.j During PLR versus baseline: P = .05.k After PLR versus baseline: P = .001.l Responder versus nonresponder: P < .001. m Calculated as stroke volume in milliliters per beat divided by body surface area in square meters.n Responder versus nonresponder: P = .004. o After PLR versus baseline: P < .001.
-0.59 (6) -0.15 (4)
-4 (4) -6 (4)
-11 (6) -13 (9)
-10 (6) -11 (7)
7 (10) 3 (9)
25 (12)l
3 (7)
31 (12)l 5 (6)

234 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
Oscillometric NIBP monitoring has an
inherent time lag . . . thus missing the
peak effect of the PLR maneuver.
Discussion The main fi nding of our study is that PP measured
by NIBP monitoring is not a sensitive or specifi c pre-
dictor of fl uid responsiveness in
healthy volunteers. Approxi-
mately 50% of the participants
in our study had a 15% or
greater PLR-induced increase in
SVI, consistent with the result
of a previous study of healthy
volunteers.32 Participants’ SBP
decreased in response to PLR in
both of our tests and could not
be used to detect fl uid respon-
siveness. The general decrease in
SBP from baseline to maneuver is contrary to the
expected response to PLR.
The PLR-induced decreases in SBP, DBP, and MAP
in our study are congruent with the results of other
studies in healthy volunteers.32-36 In a study of the
effects of PLR on central hemodynamics in 50 healthy
volunteers, central aortic pressures (measured with
radial artery applanation tonometry) and brachial
artery SBP, DBP, MAP, and PP (all measured with
NIBP monitoring) decreased 1 minute after PLR
performed with 60° leg and head elevations.33 These
fi ndings suggest brachial artery dilation. Researchers
in several other studies have noted brachial artery
dilation in healthy volunteers in response to PLR.37-40
Various researchers have concluded that the decrease
in BP is most likely due to activation of low-pressure
baroreceptors as a result of intrathoracic blood
pooling,37,38,41 which inhibits sympathetic vasomo-
tor discharge (causing a decrease in vascular tone),
or activation of arterial baroreceptors in addition to
low-pressure baroreceptors.42,43 Moreover, changes
in arterial tone maintain a constant MAP despite vari-
ation in cardiac output.42,44 Therefore, PLR may cause
simultaneous but opposing refl exive responses result-
ing in an increase in cardiac output and simultaneous
dilation of peripheral arteries, which combined may
contribute to the BP response.41
Responses to PLR may differ in critically ill
patients receiving mechanical ventilation and in
healthy volunteers. The results of our study con-
trast with those of a meta-analysis of PLR that
included direct arterial BP measurements in criti-
cally ill patients receiving vasopressors.20 In the
meta-analysis, pooled data from 4 studies showed
that a PLR-induced increase in direct radial artery
PP (threshold, 9%-12%) was predictive of a response
to a fl uid bolus with a sensitivity of 60% (95% CI,
47%-71%) and a specifi city of 86% (95% CI, 75%-
94%). In a study of 39 critically ill patients, Boulain
et al23 concluded that the arteries of the upper
limbs dilate in response to PLR. However, because
of increases in positive intrathoracic pressure, mechan-
ical ventilation reduces the stretch of the baroreceptors
in the pulmonary vessels, thus attenuating barorecep-
tor stimulation and the subsequent arterial dilation.
Similarly, Delerme et al36 and Geerts et al45 suggested
that a supine PLR technique (lifting the legs pas-
sively from horizontal to a 30° to 45° elevation
while the head and upper torso remain fl at) main-
tains the level of the heart and baroreceptors and
thus may limit baroreceptor activation. Because the
participants in our study were spontaneously breath-
ing and not receiving mechanical ventilation, the
increase in vasodilation may have been relatively
greater, resulting in a decrease in BP in comparison
with patients receiving mechanical ventilation. Bou-
lain et al23 also suggested that in patients in shock,
administration of -adrenergic catecholamines, which
Figure 3 Relationship between percentage changes in stroke volume index (SVI) and systolic blood pressure induced by passive leg raising (PLR) in test A. The horizontal line rep-resents the a priori threshold of a 15% increase in SVI. Partici-pants with PLR-induced increases in SVI over this threshold were classifi ed as responders (triangles). Participants with PLR-induced increases in SVI below this threshold were classi-fi ed as nonresponders (asterisks). The vertical line represents the a priori threshold of a 9% change in SBP induced by PLR.
-20 -10
-10
0
10
20
30
40
50
0 10 20
Test A, % change in SBP
Test
A, %
ch
ang
e in
SV
I

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 235
PLR-induced changes in oscillometric NIBP measurements of PP and SBP are not recom-mended for predicting fluid responsiveness in healthy volunteers.
result in venous vasoconstriction, may shift venous
blood from an unstressed to a stressed volume and
thus amplify the preload augmentation of the PLR
response.
Another explanation for the differences in results
may be the limitations of NIBP monitoring. NIBP
measurements can be obtained only after the BP cuff
is inflated to approximately 160 to 200 mm Hg, with
variable peak inflation pressure depending on the
participant’s initial SBP reading. This constraint may
create a lag time and variability between the peak
effect of the PLR maneuver and the time of mea-
surement. If this occurs, the PLR peak effect may be
missed, potentially causing a false-negative response.
Additionally, oscillometric NIBP monitoring devices
directly measure the MAP and extrapolate the SBP
and DBP. PP is determined by both SBP and DBP,
both of which are extrapolated measurements, poten-
tially increasing measurement error in PP.
The noninvasive cardiac output monitoring
device that we employed uses bioreactance to
measure responses to PLR. Validation studies have
found the device to be accurate and reliable,28,46
and another study validated the device’s ability to
measure the response to PLR.47 Researchers in 1
study concluded that bioreactance was not reliable
for estimating cardiac output in response to PLR in
critically ill patients.48 In that study, investigators
averaged 3 thermodilution boluses from the ref-
erence method and compared the result with 1
instantaneous bioreactance value. In other stud-
ies, satisfactory concordance was observed when
10 minutes’ worth of bioreactance values were com-
pared with the results of thermodilution boluses.28,46,47
Averaging cardiac output data over 10 minutes adjusts
for the differences in time responses between devices
and most likely explains much of the difference
in the study findings.49
Nursing ImplicationsFluid responsiveness alone is not an indication
to administer fluid boluses.50 Fluid resuscitation is
indicated in patients with evidence of inadequate
tissue perfusion (eg, MAP ≤ 65 mm Hg, increased
serum lactate level1,50,51). Nurses must identify the
need for fluid resuscitation as well as a patient’s
likelihood of increasing SV in response to fluid
administration (fluid responsiveness).
The results of 2 systematic reviews and meta-
analyses suggested that PLR-induced changes in SV
and its surrogates are reliable predictors of fluid
responsiveness.20,25 The PLR-induced change in the
invasive radial artery PP is a weaker, but also signifi-
cant, predictor of fluid responsiveness. These
results were independent of the type of measure-
ment device used (eg, esophageal Doppler imag-
ing, echocardiography, bioreactance) to measure
the PLR-induced change. However, the results of
our study in healthy volunteers do not support the
use of PLR-induced changes in NIBP measure-
ments. Thus, the use of NIBP monitoring as a part
of PLR is not recommended.
Study Limitations and Future Research A limitation of this study is that it was not per-
formed in critically ill patients and therefore conclu-
sions cannot be generalized to the critically ill. We
did not measure other stressors, such as pain, that
may change the cardiopulmonary response to PLR.
Measuring these variables
may have helped to distin-
guish causes of the change
in hemodynamic variables
in contrast to the PLR-
induced changes.
Future studies need to
focus on the population of
critically ill patients. Other
considerations for future
research include compari-
son studies of participants
with different types of
shock (eg, septic vs hemor-
rhagic shock). Few studies in critically ill patients
have used a 60° leg elevation, which may increase
diagnostic accuracy in patients with certain conditions
(eg, hypovolemia). Whether the volume status of a
patient changes the volume of autotransfusion by
PLR is unknown.45 Studies comparing normovolemic
with hypovolemic patients may increase the under-
standing of differences between conditions.
Conclusion PLR-induced changes in oscillometric NIBP mea-
surements of PP and SBP were not sensitive or specific
predictors of fluid responsiveness in healthy volun-
teers and are not recommended.
FINANCIAL DISCLOSUREThis study received partial support from the University of Washington School of Nursing Hester McLaws Nursing Scholarship Award.
SEE ALSO For more about passive leg raising, visit the Critical Care Nurse website, www.ccnonline.org, and read the article by Pickett et al, “Passive Leg-Raising and Predic-tion of Fluid Responsiveness: Systematic Review” (April 2017).

236 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
REFERENCES1. Dellinger RP, Levy MM, Rhodes A, et al; Surviving Sepsis
Campaign Guidelines Committee Including the Pediatric Subgroup. Surviving Sepsis Campaign: international guide-lines for managment of severe sepsis and septic shock, 2012. Intensive Care Med. 2013;39(2):165-228.
2. Marik PE. Early management of severe sepsis. Chest. 2014; 145(6):1407-1418.
3. Marik PE. Techniques for assessment of intravascular vol-ume in critically ill patients. J Intensive Care Med. 2009; 24(5): 329-337.
4. Surviving Sepsis Campaign. Updated bundles in response to new evidence. http://www.survivingsepsis.org/SiteCol-lectionDocuments/SSC_Bundle.pdf. Updated April 2015. Accessed February 3, 2018.
5. Marik PE, Levitov A, Young A, Andrews L. The use of biore-actance and carotid Doppler to determine volume respon-siveness and blood flow redistribution following passive leg raising in hemodynamically unstable patients. Chest. 2013;143(2):364-370.
6. Préau S, Saulnier F, Dewavrin F, Durocher A, Chagnon JL. Passive leg raising is predictive of fluid responsiveness in spontaneously breathing patients with severe sepsis or acute pancreatitis. Crit Care Med. 2010;38(3):819-825.
7. Biais M, Vidil L, Sarrabay P, Cottenceau V, Revel P, Sztark F. Changes in stroke volume induced by passive leg raising in spontaneous breathing patients: comparison between echocardiography and Vigileo/FloTrac device. Crit Care. 2009; 13(6):R195.
8. Lakhal K, Ehrmann S, Runge I, et al. Central venous pressure measurements improve the accuracy of leg raising-induced change in pulse pressure to predict fluid responsiveness. Intensive Care Med. 2010;36(6):940-948.
9. Lakhal K, Ehrmann S, Benzekri-Lefèvre D, et al. Brachial cuff measurements of blood pressure during passive leg raising for fluid responsiveness prediction. Ann Fr Anesth Reanim. 2012;31(5):e67-72.
10. Monnet X, Bleibtreu A, Ferré A, et al. Passive leg-raising and end-expiratory occlusion tests perform better than pulse pressure variation in patients with low respiratory system compliance. Crit Care Med. 2012;40(1):152-157.
11. Maizel J, Airapetian N, Lorne E, Tribouilloy C, Massy Z, Slama M. Diagnosis of central hypovolemia by using pas-sive leg raising. Intensive Care Med. 2007;33(7):1133-1138.
12. Marik PE, Monnet X, Teboul JL. Hemodynamic parameters to guide fluid therapy. Ann Intensive Care. 2011;1(1):1.
13. Thiel SW, Kollef MH, Isakow W. Non-invasive stroke vol-ume measurement and passive leg raising predict volume responsiveness in medical ICU patients: an observational cohort study. Crit Care. 2009;13(4):R111.
14. Upadya A, Tilluckdharry L, Muralidharan V, Amoateng-Adjepong Y, Manthous CA. Fluid balance and weaning outcomes. Intensive Care Med. 2005;31(12):1643-1647.
15. Rosenberg AL, Dechert RE, Park PK, Bartlett RH; NIH NHLBI ARDS Network. Review of a large clinical series: association of cumulative fluid balance on outcome in acute lung injury: a retrospective review of the ARDSnet trial volume study cohort. J Intensive Care Med. 2009;24(1):35-46.
16. Bridges EJ. Arterial pressure-based stroke volume and func-tional hemodynamic monitoring. J Cardiovasc Nurs. 2008;23(2):105-112.
17. Marik PE, Cavallazzi R. Does the central venous pressure predict fluid responsiveness? An updated meta-analysis and a plea for some common sense. Crit Care Med. 2013; 41(7): 1774-1781.
18. Marik PE, Cavallazzi R, Vasu T, Hirani A. Dynamic changes in arterial waveform derived variables and fluid responsiveness in mechanically ventilated patients: a systematic review of the literature. Crit Care Med. 2009;37(9):2642-2647.
19. DeBacker D, Heenen S, Piagnerelli M, Koch M, Vincent JL. Pulse pressure variations to predict fluid responsiveness: influence of tidal volume. Intensive Care Med. 2005;31(4): 517-523.
20. Cavallaro F, Sandroni C, Marano C, et al. Diagnostic accuracy of passive leg raising for prediction of fluid responsiveness in adults: systematic review and meta-analysis of clinical studies. Intensive Care Med. 2010;36(9):1475-1483.
21. Jabot J, Teboul JL, Richard C, Monnet X. Passive leg raising for predicting fluid responsiveness: importance of the pos-tural change. Intensive Care Med. 2009;35(1):85-90.
22. Monnet X, Rienzo M, Osman D, et al. Passive leg raising predicts fluid responsiveness in the critically ill. Crit Care Med. 2006;34(5):1402-1407.
23. Boulain T, Achard JM, Teboul JL, Richard C, Perrotin D, Ginies G. Changes in BP induced by passive leg raising predict response to fluid loading in critically ill patients. Chest. 2002;121(4):1245-1252.
24. Teboul JL, Monnet X. Prediction of volume responsiveness in critically ill patients with spontaneous breathing activity. Curr Opin Crit Care. 2008;14(3):334-339.
25. Cherpanath TG, Hirsch A, Geerts BF, et al. Predicting fluid respon-siveness by passive leg raising: a systematic review and meta-analysis of 23 clinical trials. Crit Care Med. 2016; 44(5): 981-991.
26. Lakhal K, Ehrmann S, Runge I, et al. Tracking hypotecxnsion and dynamic changes in arterial blood pressure with bra-chial cuff measurements. Anesth Analg. 2009;109(2):494-501.
27. Critchley LA, Critchley JA. A meta-analysis of studies using bias and precision statistics to compare cardiac output mea-surement techniques. J Clin Monit Comput. 1999; 15(2): 85-91.
28. Squara P, Denjean D, Estagnasie P, Brusset A, Dib JC, Dubois C. Noninvasive cardiac output monitoring (NICOM): a clinical validation. Intensive Care Med. 2007;33(7):1191-1194.
29. Pickering TG, Hall JE, Appel LJ, et al. Recommendations for blood pressure measurement in humans and experimental animals: part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Pro-fessional and Public Education of the American Heart Asso-ciation Council on High Blood Pressure Research. Circulation. 2005;111(5):697-716.
30. Obtaining accurate noninvasive blood pressure measure-ments in adults. Crit Care Nurse. 2016;36(3):e12-16.
31. Fluss R, Faraggi D, Reiser B. Estimation of the Youden index and its associated cutoff point. Biom J. 2005;47(4):458-472.
32. Keller G, Cassar E, Desebbe O, Lehot JJ, Cannesson M. Ability of pleth variability index to detect hemodynamic changes induced by passive leg raising in spontaneously breathing volunteers. Crit Care. 2008;12(2):R37.
33. Kamran H, Salciccioli L, Gusenburg J, et al. The effects of passive leg raising on arterial wave reflection in healthy adults. Blood Press Monit. 2009;14(5):202-207.
34. Kamran H, Salciccioli L, Kumar P, et al. The relation between blood pressure changes induced by passive leg raising and arterial stiffness. J Am Soc Hypertens. 2010;4(6):284-289.
35. Delerme S, Renault R, Le Manach Y, et al. Variations in pulse oximetry plethysmographic waveform amplitude induced by passive leg raising in spontaneously breathing volunteers. Am J Emerg Med. 2007;25(6):637-642.
36. Delerme S, Castro S, Freund Y, et al. Relation between pulse oximetry plethysmographic waveform amplitude induced by passive leg raising and cardiac index in spon-taneously breathing subjects. Am J Emerg Med. 2010; 28(4):505-510.
37. London GM, Pannier BM, Laurent S, Lacolley P, Safar ME. Brachial artery diameter changes associated with cardio-pulmonary baroreflex activation in humans. Am J Physiol. 1990; 258(3 Pt 2):H773-777.
38. Roddie IC, Shepherd JT, Whelan RF. Reflex changes in vaso-constrictor tone in human skeletal muscle in response to stimulation of receptors in a low-pressure area of the intra-thoracic vascular bed. J Physiol. 1957;139(3):369-376.
39. Kamran H, Salciccioli L, Namana V, et al. Passive leg raising induced brachial artery dilation: is an old technique a simpler method to measure endothelial function? Atherosclerosis. 2010;212(1):188-192.
40. Bapat M, Musikantow D, Khmara K, et al. Comparison of passive leg raising and hyperemia on macrovascular and microvascular responses. Microvasc Res. 2013;86:30-33.
41. Cherpanath TG, Aarts LP, Groeneveld JA, Geerts BF. Defin-ing fluid responsiveness: a guide to patient-tailored volume titration. J Cardiothorac Vasc Anesth. 2014;28(3):745-754.
42. Mamontov OV, Kalinichenko AN, Conrady AO, Shlyakhto EV. Cardiopulmonary reflex influence on the system hemody-namic rapid regulation mechanisms. Comput Cardiol. 2008; 35:801-804.
43. Mark AL, Abboud FM, Fitz AE. Influence of low- and high-pressure baroreceptors on plasma renin activity in humans. Am J Physiol. 1978;235(1):H29-33.
44. Monnet X, Teboul J. Assessment of volume responsiveness during mechanical ventilation: recent advances. Crit Care. 2013;17(2):217.

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 237
45. Geerts B, de Wilde R, Aarts L, Jansen J. Pulse contour analy-sis to assess hemodynamic response to passive leg raising. J Cardiothorac Vasc Anesth. 2011;25(1):48-52.
46. Raval NY, Squara P, Cleman M, Yalamanchili K, Winklmaier M, Burkhoff D. Multicenter evaluation of noninvasive car-diac output measurement by bioreactance technique. J Clin Monit Comput. 2008;22(2):113-119.
47. Benomar B, Ouattara A, Estagnasie P, Brusset A, Squara P. Fluid responsiveness predicted by noninvasive bioreactance-based passive leg raise test. Intensive Care Med. 2010;36(11):1875-1881.
48. Kupersztych-Hagege E, Teboul JL, Artigas A, et al. Bioreac-tance is not reliable for estimating cardiac output and the effects of passive leg raising in critically ill patients. Br J Anaesth. 2013;111(6):961-966.
49. Squara P. Bioreactance for estimating cardiac output and the effects of passive leg raising in critically ill patients. Br J Anaesth. 2014;112(5):942.
50. Marik PE. Fluid responsiveness and the six guiding principles of fl uid resuscitation. Crit Care Med. 2016;44(10):1920-1922.
51. Garcia X, Pinsky MR. Clinical applicability of functional hemodynamic monitoring. Ann Intensive Care. 2011;1:35.
To purchase electronic or print reprints, contact American Association of Critical-Care Nurses, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; email, [email protected].
Your ticket to a great job offer.
15-0876
Search daily job postings
on the homepage.
You’re admitted to AACN’s Official Career Center.
Designed as a comprehensive career resource for nurses of all levels, the Career Center enables you to explore job postings by specialty area, location, and hospital/facility.
AACNCareerCenter.org
Post your CV or résumé today.
Choose from the best career
opportunities in nursing.
Start now. The perfect job
may be waiting for you.

Brief Report
©2018 American Association of Critical-Care Nursesdoi:https://doi.org/10.4037/ajcc2018513
Background Unplanned admissions of patients to inten-sive care units from medical-surgical units often result from failure to recognize clinical deterioration. The early warning score is a clinical decision support tool for nurse surveillance but must be communicated to nurses and implemented appropriately. A communication process including collaboration with experienced intensive care unit nurses may reduce unplanned transfers.Objective To determine the impact of an early warning score communication bundle on medical-surgical trans-fers to the intensive care unit, rapid response team calls, and morbidity of patients upon intensive care unit transfer.Methods After an early warning score was electronically embedded into medical records, a communication bun-dle including notification of and telephone collaboration between medical-surgical and intensive care unit nurses was implemented. Data were collected 3 months before and 21 months after implementation.Results Rapid response team calls increased nonsignifi-cantly during the study period (from 6.47 to 8.29 per 1000 patient-days). Rapid response team calls for patients with early warning scores greater than 4 declined (from 2.04 to 1.77 per 1000 patient-days). Intensive care unit admissions of patients after rapid response team calls significantly declined (P = .03), as did admissions of patients with early warning scores greater than 4 (P = .01), suggesting that earlier intervention for patient deterio-ration occurred. Documented reassessment response time declined significantly to 28 minutes (P = .002). Conclusion Electronic surveillance and collaboration with experienced intensive care unit nurses may improve care, control costs, and save lives. Critical care nurses have a role in coaching and guiding less experienced nurses. (American Journal of Critical Care. 2018; 27:238-242)
EARLY WARNING SCORE COMMUNICATION BUNDLE:A PILOT STUDYBy Cheryl Gagne, RN, DNP, CNEA, and Susan Fetzer, RN, PhD
E RBEvidence-Based Review on pp 243-244
238 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 239
Collaborative support from seasoned colleagues improves outcomes.
Up to 40% of intensive care unit (ICU) admissions may be avoidable,1 with nearly half of the admissions from medical-surgical units related to deterioration in the patient’s condition since the admitting diagnosis.2 Although patients exhibit clinical signs of deterioration up to 8 hours before a cardiac arrest,3 unplanned transfers to the ICU often result from failure to recognize clinical deterioration.4
Failure to rescue, described by Silber and colleagues5 in 1992, has been attributed to an inability to recognize early signs of deterioration.
The Institute for Healthcare Improvement
describes a “bundle of care” as 3 to 5 evidence-based
interventions uniformly applied together to improve
patient outcomes.6 To improve timely assessment of
and interventions for medical-surgical patients whose
condition was deteriorating, we created a communi-
cation bundle consistent with the Institute for Health-
care Improvement’s guidelines. The communication
bundle includes an electronically embedded early
warning score (EWS), an electronic medical record
(EMR) nurse alert, a pager alert to an experienced
ICU nurse, and a telephone consultation between a
medical-surgical nurse and an ICU nurse. We con-
ducted a pilot study to determine the effectiveness of
the communication bundle on ICU patient admis-
sions, patient morbidity, and rapid response team
(RRT) calls from medical-surgical units.
BackgroundIn the late 1990s, scoring systems arose as a
way to quickly warn of deterioration. Patient EWSs
are derived from physiological parameters, such as
blood pressure, heart rate, and temperature, gleaned
from nursing assessments. A predetermined score
prompts specific nursing action, such as as-needed
respiratory treatment, to ameliorate further deterio-
ration. Smith and others7 conducted a systematic
review of EWS outcomes of adult medical-surgical
patients. In 4 studies, at least a 50% increase in RRT
calls following EWS implementation was reported.
In 5 studies, the impact of EWS systems on ICU use
was measured; a significant increase in ICU admis-
sions was reported in 3 studies, and no difference
was found in 2 studies.
An EWS embedded in the EMR allows tracking,
trending, and automatic triggering by patient status.
Although the EWS provides timely recognition of
deterioration, information must be communicated
to a nurse with an appreciation for the urgency of
the situation and the knowledge to take action. The
lack of communication and action may explain the
conflicting findings reported by Smith and others.7
To improve communication, Bailey and colleagues8
added an EWS alert to the medical-surgical charge
nurse’s pager but could not explain a lack of improve-
ment in patients’ out-
comes, suggesting that
a more integrated
approach to identify
interventions is needed.
Jackson and others9
reported a strong nega-
tive correlation between medical-surgical nurses’
years of experience and reluctance to activate an RRT
call. They concluded that “collaborative support
from seasoned colleagues” targeting inexperienced
medical-surgical nurses could improve outcomes
of patients whose condition is deteriorating.9
Experienced ICU nurses serving on RRTs are
trained to recognize and intervene in situations of
clinical deterioration. We hypothesized that an EWS
communication bundle including an experienced ICU
nurse would decrease transfers, RRT calls, and morbid-
ity of medical-surgical patients transferred to the ICU.
Methods In this interrupted time-series study, measure-
ments recorded before and after intervention provided
EWS, RRT, and admission data on medical-surgical
patients transferred to the ICU.
Setting and SampleA 189-bed, Magnet-designated community hos-
pital in the Northeast with 97 medical-surgical beds
and 11 ICU beds was the setting for the study. We
studied inpatient medical-surgical patients with an
EWS greater than 4, indicating clinical deterioration.
InterventionWe embedded a 7-item modified EWS system10
with possible scores ranging from 0 to 21 into the
About the AuthorsCheryl Gagne is vice president and Susan Fetzer is a nurse researcher in patient care services at Southern New Hamp-shire Medical Center, Nashua, New Hampshire.
Corresponding author: Susan Fetzer, RN, PhD, Southern New Hampshire Medical Center, 8 Prospect Street, Nashua, New Hampshire, 03061 (email: [email protected]).

240 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
Both transfer of medical-surgical
patients to the ICU and ICU admis-
sions of RRT patients declined.
EMR (Table 1). In this system, EWS parameters are
manually entered into the EMR, and scores are auto-
matically generated. A score greater than 4 activates
a red exclamation point next to the patient’s name on
the EMR, visible to the nurse and
unit secretary. An electronic page
including room, medical record
number, and EWS score simulta-
neously notifies an experienced
ICU nurse preassigned to respond
to RRT calls. The ICU nurse
reviews the EMR and contacts the
patient’s nurse by telephone. The
nurses discuss the EWS alert and
develop a plan. The collaboration
results in reassessment of at least 1
EWS parameter and may include notifying a pro-
vider, administering as-needed medications, or fol-
lowing established protocols for interventions.
MeasuresOutcome measures included the number of
patients transferred to the ICU from the medical-
surgical units, the number of RRT calls per 1000
patient-days, ICU admissions, and RRT calls to
patients with an EWS greater than 4. Communica-
tion bundle response time was defined as the differ-
ence between EWS alert and EMR documentation
of the patient’s reassessment.
ProcedureThe institutional review board granted approval,
and the information technology department provided
quarterly outcome data. We obtained preimplemen-
tation data before embedding the EWS into the EMR.
The communication bundle was hardwired into 4
medical-surgical units and the ICU from January
through December 2015, with postimplementation
data collected from January through June 2016. We
used statistics software (SPSS v24, IBM) to generate
descriptive statistics and conduct analyses of variance.
Results The number of RRT calls before implementation
was 6.47 per 1000 patient-days. Among patients with
an EWS greater than 4, RRT calls numbered 2.04 per
1000 patient-days (Table 2). Medical-surgical trans-
fers accounted for 21.3% of ICU admissions, with
nearly half (18 of 41, or 44%) of medical-surgical
patients who had received an RRT call transferred
to the ICU.
We analyzed 6 quarters of postimplementation
data. After implementation, RRT calls increased
from 6.47 to 8.29 per 1000 patient-days, although
this finding was not significant. However, calls for
patients with an EWS greater than 4 declined. With
the exception of quarter 6, medical-surgical trans-
fers to ICU declined. ICU admissions of patients
who had received an RRT call declined significantly
(P = .03), as did ICU admissions of patients with an
EWS greater than 4 (P = .01). EWS response time
decreased significantly (P = .002), indicating a success-
ful implementation of the communication bundle.
Discussion After implementation, RRT calls increased, a
finding similar to that of Kollef et al,2 who also
found an increase in the number of RRT calls with
EWS alerts. However, in our study, the increase in
RRT calls occurred in patients with lower EWS
scores. Fewer patients who received an RRT call
exhibited EWS scores greater than 4. These findings
suggest that deterioration was identified sooner,
prompting earlier intervention. As a result, the
Item
Table 1Early warning scoring systema
Central nervous system
Respiratory rate, breaths per minute
Heart rate, beats per minute
Systolic blood pressure, mm Hg
Body temperature, ºC
Oxygen saturation with therapy, %
Urine output in 2 h, mL/h
a The composite score for all 7 items ranges from 0 to 21. The higher the score, the greater the physiological deterioration, with a composite score greater than 4 generating a communication alert.
No response
>30
>190
>220
>40
Respond to pain
111-190
201-220
38.6-40.0
Respond to voice
21-30
101-110
181-200
37.6-38.5
Alert
8-20
91-100
101-180
35.1-37.5
>94
40-90
81-100
Confused, agitated
71-80
34-35
91-93
<8
<40
<70
<34
<90
<30
3210123
Early warning score

www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 241
number of ICU admissions declined, although the
unexplained increase during quarter 6 contributed
to the nonsignificance of this outcome measure. The
decline in ICU patients with EWS scores greater than
4 admitted to the ICU reflects a decrease in transfer
morbidity. The communication bundle may have
resulted in more effective interventions by medical-
surgical nurses. The addition of ICU nurse collabo-
ration may be a facilitator.
Dummett and others11 described the EWS as
enhancing situational awareness, a first step in pro-
ducing cognitive change. The decreased EWS response
time may reflect this type of cognitive change.
LimitationsThe fact that we used only 1 quarter of preim-
plementation data for comparison may be a limita-
tion because patients’ acuity can be influenced by
seasonal changes. Although the communication
bundle resulted in earlier interventions, the effect
on patients’ survival is not known.
Conclusion The EWS is a clinical measurement tool that
complements nursing judgment. Electronic surveil-
lance together with experienced ICU nurse collabora-
tion has the potential to improve care, preserve
health care dollars, and save lives. An electronically
embedded EWS together with a communication
bundle reduced ICU admissions from
medical-surgical units and decreased patient mor-
bidity. Obtaining the perspective of nurses imple-
menting the EWS communication bundle is
warranted.
ACKNOWLEDGMENTThe authors appreciate the support of Andrew Watt, MD.
FINANCIAL DISCLOSURESNone reported.
REFERENCES1. Robertson LC, Al-Haddad M. Recognizing the critically ill
patient. Anaesth Intensive Care Med. 2013;14(1):11-14. 2. Kollef MH, Chen Y, Heard K, et al. A randomized trial of
real-time automated clinical deterioration alerts sent to a rapid response team. J Hosp Med. 2014; 9(7):424-429.
3. Mapp ID, Davis LL, Krowchuk H. Prevention of unplanned intensive care unit admissions and hospital mortality by early warning systems. Dimens Crit Care Nurs. 2013; 32(6): 300-309.
4. Alam N, Hobbelink EL, Tienhoven AJ, van de Ven PM, Jansma EP, Nanayakkara PW. The impact of the use of the Early Warning Score (EWS) on patient outcomes: a systematic review. Resuscitation. 2014;85(5):587-594.
5. Silber JH, Williams SV, Krakauer H, Schwartz JS. Hospital and patient characteristics associated with death after surgery: a study of adverse occurrence and failure to rescue. Med Care. 1992;30(7):615-629.
6. Resar R, Griffin FA, Haraden C, Nolan TW; Institute for Healthcare Improvement. Using care bundles to improve health care quality. IHI Innovation Series. http://www.ihi .org/resources /Pages/IHIWhitePapers/UsingCareBundles .aspx. Published 2012. Accessed January 29, 2018.
7. Smith ME, Chiovaro JC, O’Neil M, et al. Early warning system scores for clinical deterioration in hospitalized patients: a systematic review. Ann Am Thorac Soc. 2014; 11(9):1454-1465.
8. Bailey TC, Chen Y, Mao Y, et al. A trial of a real-time alert for clinical deterioration in patients hospitalized on general medical wards. J Hosp Med. 2013;8(5):236-242.
Outcome measure
Table 2Outcomes before and after implementation of an early warning score communication bundle
Rapid response calls Total number Number per 1000 patient-days
Rapid response calls with EWS >4 per 1000 patient-days
ICU admissions from medical- surgical units, No. (%)
ICU admissions from medical- surgical units after RRT,a No. (%)
ICU admissions from medical- surgical units with EWS >4 per
1000 patient-daysb
EWS communication response time,c minutes
Abbreviations: EWS, early warning score; ICU, intensive care unit; NA, not applicable; Q, quarter; RRT, rapid response team.a df = 6, F = 8.794, P = .03.b df = 6, F = 15.653, P = .01.c df = 5, F = 34.714, P = .002.
568.29
1.77
46 (17.8)
11 (20)
0.75
28
79 11.78
2.09
82 (31.4)
15 (19)
0.44
29
54 8.71
2.08
54 (20.3)
14 (26)
0.62
33
619.02
1.77
59 (21.5)
16 (26)
0.74
27
619.04
2.57
55 (20.5)
19 (31)
0.86
39
527.40
3.70
64 (24.6)
17 (33)
1.00
85
416.47
2.04
57 (21.3)
18 (44)
1.56
NA
Q7Q6Q5Q4Q3Q2Q1
After implementation, by quarterBefore
implementation

242 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
9. Jackson S, Penprase B, Grobbel C. Factors influencing reg-istered nurses’ decision to activate an adult rapid response team in a community hospital. Dimens Crit Care Nurs. 2016; 35(2):99-107.
10. Moon A, Cosgrove JF, Lea D, Fairs A, Cressey DM. An eight year audit before and after the introduction of modified early warning score (MEWS) charts, of patients admitted to a tertiary referral intensive care unit after CPR. Resuscitation. 2011;82(2):150-154.
11. Dummett BA, Adams C, Scruth E, Liu V, Guo M, Escobar GJ. Incorporating an early detection system into routine clinical
practice in two community hospitals. J Hosp Med. 2016;11 (Suppl 1):S25-S31.
To purchase electronic or print reprints, contact American Association of Critical-Care Nurses, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; email, [email protected].
THE DEFINITIVE RESOURCEfor critical care nursing
and practice
• NEW! corresponds to the most recent CCRN®
current literature, national and international guidelines, clinical studies, AACN/ANA scope of practice, and ECCO 3.0.
• NEW! addresses the healthcare needs of today’s patients, including pain management, palliative care, and end-of-life care; nutritional support; transplantation; and key AACN initiatives.
• NEW! Clinical Pearls Key Concepts highlight important content and serve as a convenient quick reference.
• NEW!• with an emphasis on clinical nursing practice, prepare you for the full range of knowledge you will encounter on the CCRN exam and in practice.
American Association of Critical-Care Nurses; and Tonja M. Hartjes, DNP, ACNP-BC, FNP-BC, CCRN-CSC, FAANP
October 2017 ISBN: 978-1-4557-1065-2
NEW EDITION!

Evidence-Based Review and Discussion PointsBy Ronald L. Hickman, RN, PhD, ACNP-BC
Evidence-Based Review (EBR) is the journal club feature in the American Journal of Critical Care. In a journal club, attend ees review and critique published research articles: an important first step toward integrating evidence-based practice into patient care. General and specific questions such as those outlined in the “Discussion Points” box aid journal club participants in probing the quality of the research study, the appropriateness of the study design and methods, the validity of the conclusions, and the implications of the article for clinical practice. When critically appraising this issue’s EBR article, “Early Warning Score Communication Bundle: A Pilot Study” (pp 238-242), consider the questions and discussion points outlined in the “Discussion Points” box.
F ailure to recognize early signs of deteriora-
tion can result in unplanned and unneces-
sary admissions to an intensive care unit
(ICU) for acutely ill patients convalescing in the
hospital. Clinical deterioration is likely to occur up
to 8 hours before decisions to initiate a transfer
to an ICU. However, failure to recognize a patient’s
clinical deterioration accounts for 40% of the
unplanned and avoidable transfers to an ICU.
Early warning scores (EWSs), systematic
methods for early detection of a patient’s risk
for clinical deterioration, are often derived from
physiological parameters and nursing assessments
to prompt nursing action. The adoption of elec-
tronic medical records by health care systems has
provided an opportunity for the integration of
EWSs as a clinical decision support tool to mini-
mize unplanned transfers and avoid ICU trans-
fers. However, one of the significant
limitations of EWSs integrated into
electronic medical records has been the
inability to alert nurses of the urgency
of the situation and facilitate commu-
nication to a rapid response team.
To address the current limitations
of EWSs integrated into electronic medi-
cal records, the authors have developed
an EWS communication bundle, which
they hypothesized would decrease trans-
fers to an ICU, rapid response team calls,
and morbidity of medical-surgical patients.
This study had an interrupted time-series
design with pretest and posttest measure-
ments and was conducted in a 189-bed
community hospital. A 7-item modified
EWS system was embedded into the elec-
tronic medical record, and scores greater
than 4 indicated evidence of a patient’s
clinical deterioration. For patients with
EWSs greater than 4, the communication
bundle was activated and included 2
alerts: (1) a red exclamation mark next
to the patient’s name in the electronic
medical record and (2) a simultaneous
page sent to the rapid response team’s
nurse. The activation of the communica-
tion bundle was designed to facilitate the
reassessment of the patient, notifying a
provider, and prompt the administration
of medications or initiation of protoco-
lized interventions.
Investigator Spotlight
This feature briefly describes the personal journey and background story of the EBR article’s investigators, discussing the circumstances that led them to undertake the line of inquiry represented in the research article featured in this issue.
Cheryl Gagne, RN, DNP, CNEA, is the vice president for patient
care services at Southern New Hampshire Medical Cen-
ter in Nashua, New Hampshire. She has been a registered
nurse for more than 35 years and practiced for more than
20 years as a critical care nurse.
Gagne says that she has been motivated to influence
the care of the critically ill through personal and profes-
sional experiences. “From my first assignment as a nurse
through today, I relentlessly pursue solu-
tions to challenges patients, and their
nurses, face on a daily basis,” she shares.
She adds that her interest in early warn-
ing scores was influenced by an endur-
ing childhood experience where her
brother acquired an acute but devastat-
ing illness, since which she has been
compelled to find a solution to help
patients like her brother.
According to Dr Gagne, clinical decision support is a
promising method that will affect the delivery and quality
of health care. Clinical decision support will become the
norm in electronic medical records and, as algorithms
become more sophisticated, we will be able to examine
everything from nursing care intensity to early detection
of infection, predicts Gagne. “I look forward to seeing how
early warning scores and similar tools will evolve and impact
the future of health care,” she adds.
©2018 American Association of Critical-Care Nurses, doi:https://doi.org/10.4037/ajcc2018196
Cheryl Gagne
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 243

About the AuthorRonald L. Hickman is an associate professor and assistant dean for nursing research, Case Western Reserve University, Cleveland, Ohio.
Discussion Points
A. Description of the Study
What is the significance of the problem
posed by the authors?
What is the purpose of the study?
B. Literature Evaluation
What evidence is provided in support of early
warning scores in hospitalized adults?
What was identified as a major barrier
related to the implementation of early warning
scores?
C. Methods and Design
Describe how the authors conceived the
early warning score with a communication
bundle.
Describe what data were collected for this
publication.
D. Results
What were the major findings of this study?
What was one of the limitations of the study
cited by the authors?
How can you use the findings of this study to
improve the quality of nursing care at your
facility?
The authors report that electronic surveillance
of a patient’s clinical deterioration can be feasibly
integrated into an electronic medical record and
minimize unplanned and avoidable ICU transfers.
Based on the results of their study, the authors were
able to demonstrate that the use of an EWS commu-
nication bundle significantly reduced ICU transfers
for patients who met the alert criterion. They also
noted a slight increase in the number of rapid response
team calls, which was not statistically significant.
The authors conclude that an EWS communication
bundle is an effective strategy for surveillance and
promotes collaboration among health care providers
to optimize the quality of patient care.
Information From the AuthorsCheryl Gagne, RN, DNP, CNEA, lead author on this
EBR article, provides personal and professional per-
spectives that influenced the implementation of the
EWS communication bundle. Dr Gagne comments
that she had a longstanding desire to identify innova-
tive solutions to improve patient care, which motivated
her to investigate the effects of an EWS communica-
tion bundle.
Every day, nurses are assessing patients while bal-
ancing the competing demands of delivering high-qual-
ity nursing care. “Of the hundreds of clinical decisions
nurses make every shift, the decision that results in
earlier rather than later recognition of deterioration
is perhaps one of the most important,” comments
Dr Gagne. “As nurses, we intervene on behalf of our
patients throughout the day, and an EWS can be a
seamless, electronically driven strategy to identify
and respond to subtle and progressive changes in a
patient’s condition,” she says.
From Dr Gagne’s perspective, the EWS communica-
tion bundle is a solution that enhances nurse-to-nurse
collaboration. She remarks that “through the interac-
tions between the bedside nurse and [the] critical care
nurse on the response rapid response team prompted
by the EWS alert, our patients are received effective care
earlier and [are] being transferred less to the ICU.”
An unintended consequence of the EWS commu-
nication bundle is the increased confidence of the
nurses in recognizing and initiating appropriate nurs-
ing care for patients with declining health. “Our
bedside nurses are experiencing more confidence
because of their ability to more quickly respond to
and even reverse signs of impending deterioration of
their patients’ condition,” she mentions.
Implications for PracticeGagne encourages readers of the American Journal
of Critical Care to consider implementing the use of
EWS with a communication bundle to potentially
improve care. Dr Gagne and her coauthor comment
that the EWS is a clinical measurement that comple-
ments nursing judgment; however, they recognize the
limitations of the current state of the science regarding
early warning assessment tools. Gagne comments that
“the most obvious unresolved early warning score issue
is the lack of reliability and validity of available tools.”
Despite the lack of evidence of the reliability and valid-
ity of early warning scores across clinical populations,
Dr Gagne envisions that such early warning scores
will be routinely embedded in electronic medical
records and provide health care providers with robust
clinical decision support to detect and minimize a
patient’s clinical deterioration.
244 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org

Brief Report
©2018 American Association of Critical-Care Nursesdoi:https://doi.org/10.4037/ajcc2018908
Background Exposure to bright light has alerting effects. In nurses, alertness may be decreased because of shift work and high work pressure, potentially reducing work performance and increasing the risk for medical errors. Objectives To determine whether high-intensity dynamic light improves cognitive performance, self-reported depressive signs and symptoms, fatigue, alertness, and well-being in intensive care unit nurses.Methods In a single-center crossover study in an inten-sive care unit of a teaching hospital in the Netherlands, 10 registered nurses were randomly divided into 2 groups. Each group worked alternately for 3 to 4 days in patients’ rooms with dynamic light and 3 to 4 days in control lighting settings. High-intensity dynamic light was administered through ceiling-mounted fluorescent tubes that delivered bluish white light up to 1700 lux during the daytime, versus 300 lux in control settings. Cognitive performance, self-reported depressive signs and symptoms, fatigue, and well-being before and after each period were assessed by using validated cognitive tests and questionnaires. Results Cognitive performance, self-reported depressive signs and symptoms, and fatigue did not differ signifi-cantly between the 2 light settings. Scores of subjective well-being were significantly lower after a period of working in dynamic light.Conclusions Daytime lighting conditions did not affect intensive care unit nurses’ cognitive performance, per-ceived depressive signs and symptoms, or fatigue. Per-ceived quality of life, predominantly in the psychological and environmental domains, was lower for nurses working in dynamic light. (American Journal of Critical Care. 2018; 27:245-248)
EFFECT OF DYNAMIC LIGHT APPLICATION ON COGNITIVE PERFORMANCE AND WELL-BEING OF INTENSIVE CARE NURSESBy Koen S. Simons, MD, Enzio R. K. Boeijen, RN, BSc, Marlies C. Mertens, PhD, Paul Rood, RN, MSc, Cornelis P.C. de Jager, MD, PhD, and Mark van den Boogaard, RN, PhD
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 245

Exposure to environmental light has profound effects on humans in health and dis-ease.1 Apart from entraining the biological clock, light exposure also influences cog-nitive performance and alertness.2 Alertness may be decreased in nursing care because of variable shifts and high work pressure.3 Stimulating alertness by means of bright light therapy can improve performance4,5 and in health care settings may lead to
better patient care, possibly by reducing the number of errors. Studies on the alerting effect of lighting therapy on the performance of nurses are scarce. Some results suggest a beneficial effect of a brief exposure to bright light6 or improved alertness in nurses exposed to bright light, compared with dim light conditions, during the night shift.7
Bright light may improve alert-
ness and reduce medical errors.
246 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
Methods The intensive care unit (ICU) of the Jeroen Bosch
Hospital, ‘s-Hertogenbosch, the Netherlands, a teach-
ing hospital with a 16-bed mixed medical-surgical
ICU, has a dynamic lighting system. This system,
the dynamic lighting application (DLA), offers bright
light intensities (up to 1700 lux, compared with 300
lux in standard settings) and colors according to a
fixed rhythm via conventional, ceiling-mounted flu-
orescent tubes inside patients’ rooms.
Details of a DLA study with ICU patients
have been published.8
We performed a crossover study
to determine the effect of daytime
DLA on cognitive function and self-
reported measures of well-being in 10
ICU nurses. Participants were divided
into 2 groups. In the first group, participants were
scheduled to work at least 3 to a maximum of 4
consecutive daytime shifts in patients’ rooms where
the light was set to DLA. After a washout period,
the participants were subsequently scheduled to 3
to 4 daytime shifts in patients’ rooms with standard
lighting settings. In the second group, the partici-
pants followed the same schedule, starting with
standard lighting settings and ending with DLA.
Before and directly after each test period, partic-
ipants were asked to undergo cognitive performance
tasks by using 2 validated computer-based tests, the
Test of Divided Attention (TODA)9 and the Test of
Selective Sustained Attention (TOSSA).10 In the TODA,
participants listen to groups of beeps and are requested
to distinguish the groups of 3 beeps while simultane-
ously determining the correctness of a sum. TODA
scores range from 0% to 100% and are a measure of
the functioning of divided attention. In the TOSSA,
participants listen to groups of beeps and are asked
to distinguish the groups of 3 beeps by pushing the
space bar on the computer keyboard as quickly as
possible. TOSSA produces 3 scores: concentration
strength, detection strength, and response inhibition
strength.10 Scores for each of the 3 range from 0% to
100%. To minimize the influence of a learning effect
on the performance on these tests, participants com-
pleted a practice session of both tests 1 time before
the actual study started.
Information on subjective well-being, mental
health, and sleep quality of the participants was
assessed by using validated questionnaires11-15: the
Center for Epidemiologic Studies Depression scale
(CES-D), the Fatigue Assessment Scale (FAS), and
the World Health Organization Quality of Life abbre-
viated version (WHOQOL-BREF). An additional ques-
tionnaire (a diary) was developed to obtain baseline
characteristics and subjective measures of alertness
and fatigue (Table 1); the diary was filled in daily by
using a numeric rating scale. Syntax formats were
used to analyze the outcomes of the CES-D, the FAS,
and the WHOQOL-BREF. The first and last measure-
ments during the working period were used to com-
pute difference scores. The delta (di) of these scores
was used for comparisons between DLA and the
control period.
About the AuthorsKoen S. Simons is an intensivist, Department of Intensive Care Medicine, Jeroen Bosch Hospital, ‘s-Hertogenbosch, the Netherlands, and Department of Intensive Care, Rad-boud University Medical Center, Nijmegen, the Nether-lands. Enzio R. K. Boeijen is a student in nursing sciences, Paul Rood is a PhD student, and Mark van den Boogaard is an assistant professor, Department of Inten-sive Care, Radboud University Medical Center. Cornelis P. C. de Jager is an intensivist, Department of Intensive Care Medicine, Jeroen Bosch Hospital. Marlies C. Mertens is a psychologist, Department of Medical Psychology, Jeroen Bosch Hospital and at Eindhoven Corporation of Primary Health Care Centers (SGE), Eindhoven, the Netherlands.
Corresponding author: Koen S. Simons, MD, Department of Intensive Care Medicine, Jeroen Bosch Ziekenhuis, Henri Dunantstraat 1, 5223 GZ ’s-Hertogenbosch, the Netherlands (email: [email protected]).

Results The mean age of participants was 34 years, and
70% were female. Participants worked a similar num-
ber of hours in the DLA period and the control period.
Scores on the TODA and all outcome measures of
the TOSSA did not change significantly in both peri-
ods after each testing period (Table 2). Mean CES-D
and FAS scores did not change significantly during
either the DLA period or the control period. Total
scores of the WHOQOL-BREF decreased from 109.7
to 108.0 during the testing period in the DLA period
and improved from 103.9 to 112.5 in the control
period; the difference score during the testing period
was -1.7 in the DLA period and +8.6 in the control
period (P = .01). Significant changes occurred in the
domain of psychological health and environment
(Table 2).
DLA was generally well tolerated by nurses. Two
participants reported headaches due to constantly
squinting their eyes because of the DLA brightness.
Discussion In this crossover study, we found no differences
in cognitive performance, fatigue, or depressive
feelings of ICU nurses when they worked in an envi-
ronment of enhanced light levels compared with
when they worked in an environment with normal
Type of question
Table 1“Diary” questionnaire consisting of baseline characteristics and subjective questions about well-being
General
Specific
Dailya
AgeSexMarital statusWorking hours during research period
Physical health problemsPsychiatric health problemsUse of (psychotropic) medicationSleep experienceExperience working in lighting and type of lighting
Topic Numeric Rating Scale, 0-10Sleeping quality Bad - good Feeling dull Not dull - very dull Feeling good Bad - goodSubjective sleep Minimum hours slept - duration maximum hours sleptActivity Not active - very activePositive thoughts Negative thoughts - positive thoughtsPositive events Negative events - positive events
Topic
a Daily scores were filled in using a numeric rating scale from 0 to 10.
Variable
Table 2Clinical outcomes of dynamic light application (DLA)a
Cognitive performance TODA, mean (SD) TOSSA, mean (SD) Concentration strength Detection strength Response inhibition strength
Mental health CES-D, mean (SD) FAS, mean (SD) WHOQOL-BREF, mean (SD) Overall QOL and health Domain 1: Physical health Domain 2: Psychological health Domain 3: Social relationships Domain 4: Environment Diary, median (IQR) Sleep quality Feeling dull Feeling good Subjective sleep duration Activity Positive thoughts Positive events
Abbreviations: CES-D, Center for Epidemiologic Studies Depression scale; FAS, Fatigue Assessment Scale; IQR, interquartile range; TODA, Test of Divided Attention; TOSSA, Test of Selective Sustained Attention; WHOQOL-BREF, World Health Organization Quality of Life abbreviated version.
a Data were collected directly before and after the specified testing period. b Difference between the scores.c P = .008 for difference between DLA before and Control before.d P = .006 for difference between DLA after and Control after.
.06
.92
.89
.87
.61 .40< .01 .10 .31 .05 .08 .01
.78
.15
.61
.95
.40
.34
.86
3.3
3.83.57.3
0.0-0.48.60.20.50.60.50.9
-0.30.6-0.4-1.00.40.00.2
94.5 (8.1)
95.4 (7.3)96.5 (5.7)98.8 (2.1)
2.4 (2.5) 17.4 (3.5)112.5 (6.0) 9.0 (0.9) 16.8 (1.0) 16.8 (1.0) 18.0 (1.6) 17.7 (1.2)
8.0 (6.5-8.0)8.0 (6.0-8.0)8.0 (7.0-9.0)6.0 (5.0-7.0)7.0 (7.0-8.5)8.0 (7.0-9.0)9.0 (7.0-9.0)
91.3 (10.9)
91.6 (19.1)92.9 (17.6)98.5 (3.5)
2.4 (2.8) 17.8 (3.3)103.9 (7.4) 8.8 (1.1) 16.3 (1.3) 16.2 (1.4) 17.5 (1.6) 16.8 (1.1)
8.5 (5.8-10.0)7.5 (5.8-8.3)8.5 (7.0-9.0)7.0 (6.0-8.3)8.0 (7.0-8.0)9.0 (7.8-10.0)8.0 (7.0-10.0)
-0.7
0.80.65.0
0.4 0.2-1.7-0.6 0.2-0.3-0.3-0.2
-0.2-1.9-0.8-1.2-0.4 0.8 0.3
93.1 (11.0)
95.0 (9.0)95.8 (8.3)99.2 (1.1)
2.3 (2.3)17.1 (2.9)
108.0 (4.9)d
8.6 (0.8)16.9 (0.8)15.9 (0.8)16.9 (0.9)16.8 (1.2)
7.0 (7.0-8.3)6.0 (2.8-9.0)8.0 (7.3-9.0)5.5 (5.0-7.0)7.5 (6.8-8.0)8.0 (7.8-8.5)8.0 (6.3-8.3)
93.9 (9.7)
94.2 (9.2)95.2 (8.3)99.0 (1.3)
1.9 (2.4) 16.9 (2.5)
109.7 (4.9)c
9.2 (0.8)16.7 (0.8)16.2 (0.8)17.2 (1.3)17.1 (1.4)
8.0 (7.0-9.0)8.0 (6.8-8.3)9.0 (8.0-9.0)8.0 (6.8-8.3)8.0 (6.8-9.0)8.0 (7.3-9.3)8.0 (6.5-9.0)
Pdibdi
b AfterAfter BeforeBefore
Scores in control groupScores in DLA group

248 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
light levels. Interestingly, we found a significant
increase in subjective well-being, specifically in the
psychological and environmental domains of the
WHOQOL-BREF, in participants working in control
lighting settings compared with participants work-
ing in rooms with DLA.
Several reasons may explain our findings. First,
although exposure to bright light has beneficial effects
in specific conditions, it is only one of many factors
that influence cognitive performance and well-being.
Shift work, personal stress, physical complaints, and
sleep quality are all major contributors to subjective
well-being and occur frequently among nurses.3
These contributors may play such a large role that
the light therapy itself cannot alter feelings of cogni-
tive performance, well-being, depression, or fatigue.
Second, the difference in light exposure between the
DLA and the control periods may be too small for
an additional alerting effect of DLA to be detected,
because of a sufficient magnitude of lighting inten-
sity in the control group and because nursing care
also involves activity outside the brightly lit patients’
rooms, thereby diluting the total light exposure in
the DLA group. Third, differences in perceived well-
being at baseline between the 2 groups, as indicated
by the WHOQOL-BREF domain scores, might be
related to expected benefits of working in a DLA
environment or might just be serendipitous find-
ings. An adverse effect of DLA, thereby preventing
an improvement in quality of life, as found in the
control period, appears to be unlikely, yet cannot
be entirely excluded. Finally, we did not measure
the number of errors. Although we did not find ben-
eficial effects of exposure to bright light on alertness
or well-being, beneficial effects on reduction in the
number of errors still may be possible; however,
such effects seem unlikely.
Our study had several limitations. For practical
reasons, we were unable to increase the duration of
the daytime shifts for longer than 4 consecutive days.
Shift work is associated with disruption of circadian
rhythm, and realignment of circadian rhythmicity
may require up to 1 month.16 Second, we did not take
into account the type of patient and the workload of
the participants, variables that may have influenced
subjective well-being and cognitive performance.
Up to now, most research on effects of environ-
mental light has been performed in experimental
settings. In our study, we found no improvement in
cognitive performance or psychological function-
ing in a real working environment. Future research
should focus on longer duration of light exposure
and possibly higher light intensities in the whole
work area, especially during conditions of dim light,
and on effects of light therapy on the number of
errors in daily ICU nursing.
ACKNOWLEDGMENTThis study was performed at Jeroen Bosch Ziekenhuis, ’s-Hertogenbosch, the Netherlands.
FINANCIAL DISCLOSURESNone reported.
REFERENCES1. Münch M, Bromundt V. Light and chronobiology: implica-
tions for health and disease. Dialogues Clin Neurosci. 2012; 14(4):448-453.
2. Chellappa SL, Steiner R, Blattner P, Oelhafen P, Götz T, Cajo-chen C. Non-visual effects of light on melatonin, alertness and cognitive performance: can blue-enriched light keep us alert? PLoS One. 2011;6(1):e16429.
3. Dall’Ora C, Ball J, Recio-Saucedo A, Griffiths P. Characteristics of shift work and their impact on employee performance and wellbeing: a literature review. Int J Nurs Stud. 2016; 57:12-27.
4. Viola AU, James LM, Schlangen LJ, Dijk DJ. Blue-enriched white light in the workplace improves self-reported alertness, performance and sleep quality. Scand J Work Environ Health. 2008;34(4):297-306.
5. Daurat A, Aguirre A, Foret J, Gonnet P, Keromes A, Benoit O. Bright light affects alertness and performance rhythms during a 24-h constant routine. Physiol Behav. 1993; 53(5): 929-936.
6. Tanaka K, Takahashi M, Tanaka M, et al. Brief morning expo-sure to bright light improves subjective symptoms and perfor-mance in nurses with rapidly rotating shifts. J Occup Health. 2011;53(4):258-266.
7. Yoon IY, Jeong DU, Kwon KB, Kang SB, Song BG. Bright light exposure at night and light attenuation in the morning improve adaptation of night shift workers. Sleep. 2002; 25(3):351-356.
8. Simons KS, Laheij RJ, van den Boogaard M, et al. Dynamic light application therapy to reduce the incidence and duration of delirium in intensive-care patients: a randomised controlled trial. Lancet Respir Med. 2016;4(3):194-202.
9. Kovács F. TODA Test of Divided Attention: Manual [in Dutch]. Voorhout, the Netherlands: Pyramid Productions; 2009:1-23. http://www.how-psychology-tests-brain-injury.com/support-files/toda_handleiding.pdf. Accessed February 28, 2018.
10. Kovács F. TOSSA Test of Sustained Selective Attention: Man-ual. Version 4. Voorhout, the Netherlands: Pyramid Productions; 2016:1-59. http://pyramidproductions.nl.server41.firstfind.nl/Bijlage/TOSSA_manual.pdf. Accessed February 28, 2018.
11. Bouma JR, Ranchor AV, Sanderman R, van Sonderen E. Het meten van symptomen van depressie met de CES-D: een han-dleiding [in Dutch]. 2nd ed. Groningen, the Netherlands: Research Institute SHARE, University of Groningen; 2012.
12. Schroevers MJ, Sanderman R, van Sonderen E, Ranchor AV. The evaluation of the Center for Epidemiologic Studies Depression (CES-D) scale: depressed and positive affect in cancer patients and healthy reference subjects. Qual Life Res. 2000;9(9):1015-1029.
13. De Vries J, Michielsen H, Van Heck GL, Drent M. Measuring fatigue in sarcoidosis: the Fatigue Assessment Scale (FAS). Br J Health Psychol. 2004;9(pt 3):279-291.
14. Michielsen HJ, De Vries J, Van Heck GL. Psychometric qualities of a brief self-rated fatigue measure: the Fatigue Assessment Scale. J Psychosom Res. 2003;54(4):345-352.
15. The WHOQOL Group. Development of the World Health Orga-nization WHOQOL-BREF quality of life assessment. Psychol Med. 1998;3:551-558.
16. Arendt J. Shift work: coping with the biological clock. Occup Med (Lond). 2010;60(1):10-20.
To purchase electronic or print reprints, contact American Association of Critical-Care Nurses, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; email, [email protected].

THE VALUE OF LEAD aVR: A FREQUENTLY NEGLECTED LEADBy Salah S. Al-Zaiti, RN, PhD, CRNP, Teri M. Kozik, RN, PhD, CNS, CCRN, Michele M. Pelter, RN, PhD, and Mary G. Carey, RN, PhD, CNS
©2018 American Association of Critical-Care Nurses doi:https://doi.org/10.4037/ajcc2018523
Salah S. Al-Zaiti is an assistant professor at the Department of Acute and Tertiary Care Nursing, University of Pittsburgh, Pennsylva-nia. Teri M. Kozik is a nurse researcher at St Joseph’s Medical Center, Stockton, California. Michele M. Pelter is an assistant profes-sor at the Department of Physiological Nursing, University of California, San Francisco, California. Mary G. Carey is associate director for clinical nursing research, Strong Memorial Hospital, Rochester, New York.
ECG Puzzler A regular feature of the American Journal of Critical Care, the ECG Puzzler addresses electrocardiogram (ECG) interpretation for clinical practice. We welcome letters regarding this feature.
Yes No NA
Yes No NA
Yes No NA
Yes No NA
Yes No NA
Yes No NA
Yes No NA
Yes No NA
Scenario: The following 12-lead electrocardiogram
(ECG) was obtained from a 71-year-old woman who
called 9-1-1 for new onset acute chest pain associated
with dyspnea. She had no significant cardiac history.
The paramedics transmitted this prehospital
ECG to a medical command physician, request-
ing specific medical directions. What is your
assessment of this ECG?
www.ajcconline.org AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 249
Interpretation Questions:
1. Is the ECG properly calibrated (10 mm) and are leads properly placed?
If no, interpret cautiously.
2. Is this a sinus rhythm (one P wave preceding every QRS complex)?
If no, check for number of P waves in relation to QRS complexes.
3. Is the heart rate (R-R interval) normal (60-100/min)?
If no, check for supraventricular or ventricular arrhythmias.
4. Is the QRS complex narrow (duration ≤ 110 milliseconds [ms] in V1)?
If no, check for bundle branch blocks (BBBs), pacing, or ventricular arrhythmia.
5. Is the ST segment deviated (≥ 2 mm in V2-V
3, or ≥ 1 mm in other leads)?
If yes, check for similar deviations in contiguous cardiac territories.
6. Is the T wave inverted in relation to the QRS (> 5 mm)?
If yes, check for ST deviation or conduction abnormalities.
7. Is the QT interval lengthened (> 450 ms [men] or > 470 ms [women])?
If yes, check for ventricular arrhythmias or left ventricular hypertrophy.
8. Is R- or S-wave amplitude enlarged (S wave V1 + R wave V
5 > 35 mm)?
If yes, check for axis deviation or other chamber hypertrophy criteria.
II
III aVF
aVL
aVR V1
V4
V2
V5
V3
V6
I

Interpretation Sinus tachycardia with ST-segment elevation in lead
aVR and profound ST-segment depression in multiple leads,
consistent with severe left main coronary artery disease and/or
possibly occlusion of the left anterior descending coronary
artery (LAD). These findings are consistent with high-risk
acute coronary syndrome (ACS), and the patient should be
transported emergently to a tertiary care hospital that can
provide primary percutaneous coronary intervention.
Rationale Lead aVR is the augmented unipolar right arm lead,
which is the only lead that opposes the direction of the
main cardiac vector. This “view” makes lead aVR a valuable
lead for diagnosing not only ACS, but cardiac arrhythmias
with retrograde conduction (eg, junctional rhythm, ven-
tricular tachycardia), yet this lead has historically received
the least attention during ECG evaluation. Some ECG
experts ironically call the standard ECG the “11-lead
ECG” to prompt clinicians to consider examining lead
aVR in their evaluation. Within the context of ACS,
ST-segment elevation in lead aVR is frequently associated
with LAD occlusion proximal to the first septal perforator
(sensitivity and specificity >80%), with high probability of
multivessel disease. Importantly, this ST-segment pattern
is a strong predictor of hospital death, recurrent ischemia,
and heart failure, suggesting that early angiography, with
intervention if indicated, may improve clinical outcomes.
Management In this case study, the patient was sent to the catheter-
ization laboratory, which revealed a 90% occlusion of the
LAD and 70% occlusion of the left circumflex coronary artery,
which is consistent with the ST-segment pattern seen on
this ECG. Both vessels were successfully stented. The patient
was discharged home a few days after the procedure, and
no adverse events were reported within 30 days of the initial
presentation. Clinical training curriculums should empha-
size the value of examining all 12 leads of the standard ECG,
including lead aVR, which is often forgotten.
250 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
Answers:1. The calibration marks indicate proper gain (10 mm/mV).
2. Yes, there is 1 P wave per QRS complex.
3. No, the heart rate is tachycardiac at 103/min.
4. Yes, the QRS duration is normal.
5. Yes, the ST segment is elevated in lead aVR, and depressed in leads I, II, aVF, aVL, and V2 throughV
6.
6. Yes, the T wave is inverted in lead aVL.
7. No, the QT interval is not lengthened.
8. No, no signs of chamber hypertrophy are apparent.
II
III aVF
aVL
aVR V1
V4
V2
V5
V3
V6
I


The American Journal of Critical Care offers an exclusively online publication process that disseminates cutting-edge research on high acuity and critical care in the most timely and efficient manner possible. The abstracts below represent full-text articles available exclusively on the American Journal of Critical Care Web site, www.ajcconline.org. These OnlineNOW articles are fully peer reviewed, edited, formatted, and citable. Reprints of the full-text articles are available by calling (800) 899-1712 or (949) 362-2050 (ext 532) or by e-mailing [email protected].
OnlineNOW
2018 NATIONAL TEACHING INSTITUTE RESEARCH ABSTRACTS The 2018 National Teaching Institute (NTI) Research Abstracts are now available online. You can search, download, and print the 2018 NTI Research Abstracts at your convenience. Go to the AJCC website at www.ajcconline.org and click on the May issue. The 2018 research abstracts are listed in the OnlineNOW offerings. Abstracts can be searched using keywords or author names. (American Journal of Critical Care. 2018;27:e1-e17)
©2018 American Association of Critical-Care Nurses doi:https://doi.org/10.4037/ajcc2018805
Do you have a QR scanner app on your iPhone or Android? Scan this QR code with your phone to access this article instantly.
252 AJCC AMERICAN JOURNAL OF CRITICAL CARE, May 2018, Volume 27, No. 3 www.ajcconline.org
NEW HAMPSHIREManchesterHorizons 2018 - Call for Poster AbstractsDate: October 9-11, 2018. Place: Manchester, NH. Sponsor: Horizon Chapter of AACN. Contact: Pat Rosier. E-mail: [email protected]. Deadline for abstracts: May 1, 2018.
For AJCC Education Directory submission information, phone (800) 809-2273, ext 532, or e-mail [email protected].
Education DirectorySave Time. Learn More.We know you’re busy — busy at work, busy at home, busy all around.
most important articles in each issue of the American Journal of Critical Care.
Now you can get an early look at what’s coming in each issue of the American Journal of Critical Care — before the journal arrives in your mailbox — with eTOCs (electronic tables of contents).
Go toajcc.aacnjournals.org/cgi/alerts and sign up today

Watch Jillian’s story at
renalacute.com/stories
CRRTBUILT FOR my ICU.
When Jillian Kouns decided to make a career change
and become an ICU nurse 6 years ago, she was
amazed to see the difference that CRRT with the
PRISMAFLEX System could make for her patients,
but she really wanted to know more about the
therapy. Working closely with her Baxter rep, Amy,
she realizes she always has someone to count on,
whether that’s help with troubleshooting, getting the
latest updates on the therapy, or just showing her
new best practices. Because at Baxter, supporting
RNs like Jillian to deliver the best CRRT program
possible is our priority.
COMPLETE SUPPORT | PATIENT SAFETY | FLEXIBILITY
Baxter and Prismaflex are registered trademarks of Baxter International Inc. or its subsidiaries.USMP/MG120/18-0006a 02/18
The PRISMAFLEX Control Unit is intended for:
Continuous Renal Replacement Therapy (CRRT) for patients weighing 20 kilograms or more with acute renal failure and/or fluid overload.
Therapeutic Plasma Exchange (TPE) therapy for patients weighing 20 kilograms or more with diseases where fluid removal of plasma components is indicated.
Rx Only. For safe and proper use of this device, refer to the Operator’s Manual.
Baxter’s support has been such a service for our staff. They have provided amazing education and helped our leadership to continueto carry that on.”
Jillian, RN