Embed Size (px)
Citation preview

ARTICLE IN PRESS+ModelALLER-588; No. of Pages 3
Allergol Immunopathol (Madr). 2014;xxx(xx):xxx---xxx
Allergologia etimmunopathologia
Sociedad Espa nola de Inmunologıa Clınica,Alergologıa y Asma Pedi atrica
www.elsevier.es/ai
RESEARCH LETTER
Adolescent form of sporadiclymphangioleiomyomatosis
Fta
i4Lronbwatc
(S-LAM)
To the Editor,
Lymphangioleiomyomatosis (LAM) is a rare progressive dis-ease that has gone largely unrecognised by paediatricians,even by paediatric pulmonologists. We report a paediatriccase of sporadic LAM (S-LAM) that first manifested as recur-rent spontaneous pneumothorax.
We report the case of a 17-year-old girl who was broughtto the emergency department because of a 12-h history ofacute onset of chest pain on the left side and shortness ofbreath of sudden onset, with a two-hour history of transientepisodes of loss of consciousness, squinting of the eyes, andstiffening of the hands for two minutes, followed by a 10-min period of postictal state. She had no history of trauma,fever or previous respiratory symptoms. She had started herlatest menstrual period two days before. There was no fam-ily history of any respiratory disease, neurologic or othermedical conditions. Her past medical history, including anyintellectual disability, was negative, except for a previousepisode of spontaneous pneumothorax one year previouslythat had not been studied after treatment with chest tubethoracostomy.
On physical examination, pulse rate was 104 beats perminute, respiratory rate was 24 breaths per minute, andpulse oximetry measurement was 94% O2 saturation in ambi-ent air at rest, and she had decreased breath sounds onthe left hemithorax. The remainder of her examination,including a thorough neurological exam, was unremark-able. Echocardiogram, ophthalmologic examination, andskin examination under ultraviolet light did not show abnor-malities. A chest radiograph revealed right upper lobe cysticparenchymal lesions and a pneumothorax greater than 50%on the left side, requiring thoracostomy tube placement(Fig. 1). High-resolution computed tomography of the chestrevealed multiple, well-circumscribed, round, and thin-walled cysts that were scattered in a bilateral, roughlysymmetric pattern (Fig. 2). Open lung biopsy showed multi-ple cysts that distorted the lung parenchyma and contained
Please cite this article in press as: Restrepo-Gualteros SM, et a(S-LAM). Allergol Immunopathol (Madr). 2014. http://dx.doi.or
proliferating bundles of ‘‘modified’’ smooth muscle cellsin their walls, involving alveolar septa, airways, lymphat-ics, and blood vessels. The smooth muscle component waspositive for antibodies to vimentin, actin and desmin, but
aowt
0301-0546/$ – see front matter © 2013 SEICAP. Published by Elsevier Esphttp://dx.doi.org/10.1016/j.aller.2013.10.004
igure 1 Chest radiograph showing right upper lobe cys-ic parenchymal lesions, pneumothorax with left lung passivetelectasis, with normal cardiovascular silhouette.
t also reacted with antibodies to human melanin black5 (HMB 45) (Fig. 3). Having established a diagnosis ofAM, the patient underwent abdominal computed tomog-aphy, which showed a rounded lesion in the upper polef the right kidney. Three months later, she underwentephrectomy. The piece weighed 207 grams and had a rub-ery, oval mass that measured 7.5 cm × 6.2 cm × 4.5 cm,ell defined but unencapsulated, with yellow, ochre,nd brown colours. Microscopic study showed a tripar-ite composition of fat, blood vessels, and smooth muscleells in variable proportions, which reacted to the same
l. Adolescent form of sporadic lymphangioleiomyomatosisg/10.1016/j.aller.2013.10.004
ntibodies as did the lung cysts. A diagnosis of angiomy-lipoma was made. Cerebral magnetic resonance imagingith a gadolinium contrast agent revealed no abnormali-
ies.
aña, S.L. All rights reserved.

ARTICLE IN+ModelALLER-588; No. of Pages 3
2
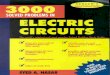
Figure 2 High-resolution computed tomography scan ofthe chest showing multiple well-defined, thin-walled cysticparenchymal lesions distributed diffusely throughout the lungs,and closed left thoracostomy tube with a small residual leftpneumothorax, with normal cardiovascular structures.
Fo
fi
paoacpsa(((pmmoeao
hcTdw(sS
atrbrmoptgfbem
ctopOhoamsfiiepcoest
ptdscw3nfihtp
igure 3 Surgical lung biopsy showing spindle cells in the wallf a cystic space stain for HMB-45; 400×.
At the present time, the patient is scheduled for the per-ormance of a surgical pleurodesis and for administration ofnhibitors of mTOR (Sirolimus).
Lymphangioleiomyomatosis (LAM) is a rare and slowlyrogressive multi-system disease which predominantlyffects young women of childbearing age, and also occursccasionally in males and children.1 It is characterised byn abnormal proliferation of smooth muscle-like cells (LAMells) leading to progressive cystic destruction of the lungarenchyma, development of fluid-filled lymphatic cystictructures (lymphangioleiomyomas) in the axial lymphatics,nd benign tumours, which primarily involve the kidneysangiomyolipomas). LAM can occur in a sporadic formS-LAM) or in association with the genetic disease TSCTSC-LAM), an autosomal dominant syndrome of variableenetrance characterised by hamartoma formation inultiple organ systems, cerebral calcifications, seizures,ental retardation, cognitive defects, autism, and tumours
Please cite this article in press as: Restrepo-Gualteros SM, et a(S-LAM). Allergol Immunopathol (Madr). 2014. http://dx.doi.or
f the brain, kidney, heart, retina and skin. S-LAM has anstimated prevalence of 1 in 400,000 adult females andbout 34% of patients with TSC (TSC itself has a prevalencef 1 in 5800 live births).
crcd
PRESSRESEARCH LETTER
Since the first reports of LAM in 1937, significant progressas been made in understanding the disease through the dis-overy of mutations in the tuberous sclerosis genes TSC1 andSC2 as underlying causes for S-LAM and TSC-LAM. S-LAMevelops due to two acquired mutations (usually in TSC2),hile patients with TSC-LAM have one germline mutation
usually in TSC2) and one acquired mutation.2 For these rea-ons, LAM occurs frequently in association with TSC, and-LAM is a relatively infrequent disease.
The protein products of TSC1 and TSC2 are hamartinnd tuberin, respectively,3 which have an important role inhe transduction of signals from cell membrane-associatedeceptors. Mutations in both hamartin and tuberin haveeen shown to inactivate the tuberin---hamartin complex,esulting in increased activity of a kinase known as theammalian target of rapamycin (mTOR) (a central regulator
f cell growth), leading to proliferation of LAM cells. Theathogenesis of LAM also comprises LAM-cell propagationhrough lymphatic channels, secretion of two lymphangio-enic growth factors: VEGF-D (vascular endothelial growthactor D) and VEGF-C (vascular endothelial growth factor C)y LAM cells,4 oestrogen (through interaction with signallingvents in LAM cells), and altered metabolism of extracellularatrix.5,6
Clinical manifestations of LAM are pneumothorax fromyst rupture (which is often the first manifestation and tendso be recurrent), progressive dyspnoea (which is the resultf airflow obstruction and cystic destruction of the lungarenchyma), and less commonly chylous pleural effusions.ther respiratory manifestations are cough, chyloptysis, andaemoptysis. Extrapulmonary manifestations are angiomy-lipomas, which occur mostly in the kidneys, chylous ascites,bdominal lymphadenopathy, and large cystic lymphaticasses termed lymphangioleiomyomas. Finally, signs con-
istent with TSC, such as facial angiofibromas, periungualbromas, nail ridging and the shagreen patch, can be seen
n patients with TSC-LAM. S-LAM and TSC-LAM have differ-ntial characteristics. Compared to patients with TSC-LAM,atients with S-LAM have a higher frequency of lung cysts,hylous plural effusion, and abdominal lymphangioleiomy-mas. Patients with TSC-LAM have a higher frequency oflevated serum levels of VEGF-D, pneumocyte hyperpla-ia, renal angiomyolipomas, and perivascular epithelioid cellumour (‘PEComa’) of the uterus.
Based on pathological and clinical findings, extra-ulmonary manifestations, and high-resolution computedomography (HRCT) scans, the diagnosis of LAM can beefined as definite, probable, or possible. The diagno-is of LAM is considered definite in the presence of: (1)haracteristic HRCT lung changes (>10 thin-walled, round,ell-defined, air-filled cysts, 2---5 mm in diameter and up to0 mm in size, distributed evenly throughout the lungs withormal lung pulmonary parenchyma), and (2) lung biopsytting the pathological criteria for LAM (including immuno-istochemical reactivity with HMB-45), angiomyolipoma ofhe kidney, thoracic or abdominal chylous effusion, lym-hangioleiomyoma, or lymph-node involved by LAM.7,8
Treatment is mainly supportive and includes bron-
l. Adolescent form of sporadic lymphangioleiomyomatosisg/10.1016/j.aller.2013.10.004
hodilators, supplemental oxygen if necessary, pulmonaryehabilitation, prophylactic vaccinations, and treatment ofomplications (surgical or chemical pleurodesis, low-fatiet, therapeutic thoracentesis, thoracic duct ligation, and

IN+Model
1
SL
a
Lb
SCc
Ud
CBe
Cf
Ug
Mh
Ui
Mj
GHfU
ARTICLEALLER-588; No. of Pages 3
RESEARCH LETTER
lung transplantation if appropriate). Current managementoptions for renal angiomyolipomas include embolisation,and partial or total nephrectomy, with the former beingpreferred to the later. Yearly follow-ups should also beconsidered for these renal tumours. Hormonal therapy(mostly using progesterone) should only be used in individ-ual cases with rapid progression of the disease. Inhibitorsof mTOR (Sirolimus) and inhibitors of matrix metallopro-teinase (MMPs) and angiogenesis (Doxycyline) are promisingnew therapeutic strategies. Given that early therapy withSirolimus can stabilise lung function,9 and sometimes resolvepulmonary disease in LAM,10 the prompt identification ofatypical early forms of LAM in young female adolescents,in cases such as our patient, can significantly impact theclinical outcome of paediatric patients with this condition.
Conclusions
Lymphangioleiomyomatosis is a rare disease that only occa-sionally affects children. The disease should always beconsidered in the presence of spontaneous pneumothoraxalong with multiple thin-walled cystic parenchymal lesions.One should also look for characteristic features of tuber-ous sclerosis complex. Accurate and early diagnosis, coupledwith appropriate treatment, is essential in order to minimisesecondary progressive impairment of pulmonary function.
Conflict of interest
The authors have no conflict of interests to declare.
Funding source
This work was supported in part by the NationalInstitute of Health (NIH) Career Development Award1K12HL090020/NHLBI, Bethesda, Maryland, U.S.A. (GN).
Ethical disclosures
Patients’ data protection. Confidentiality of Data. Theauthors declare that they have followed the protocols oftheir work centre on the publication of patient data andthat all the patients included in the study have received suf-ficient information and have given their informed consent inwriting to participate in that study.
Right to privacy and informed consent. Right to privacyand informed consent. The authors have obtained theinformed consent of the patients and/or subjects mentionedin the article. The author for correspondence is in possessionof this document.
Protection of human subjects and animals in research.The authors declare that no experiments were performedon humans or animals for this investigation.
Acknowledgment
We thank Mr. Charlie Barret for his editorial assistance.
Please cite this article in press as: Restrepo-Gualteros SM, et a(S-LAM). Allergol Immunopathol (Madr). 2014. http://dx.doi.or
References
1. Taille C, Borie R, Crestani B. Current management of lymphan-gioleiomyomatosis. Curr Opin Pulm Med. 2011;17:374---8.
∗
Ec
PRESS3
2. Juvet SC, McCormack FX, Kwiatkowski DJ, Downey GP.Molecular pathogenesis of lymphangioleiomyomatosis: lessonslearned from orphans. Am J Respir Cell Mol Biol. 2007;36:398---408.
3. van Slegtenhorst M, Nellist M, Nagelkerken B, Cheadle J, Snell R,van den Ouweland A, et al. Interaction between hamartin andtuberin, the TSC1 and TSC2 gene products. Hum Mol Genet.1998;7:1053---7.
4. Cottin V, Archer F, Leroux C, Mornex JF, Cordier JF.Milestones in lymphangioleiomyomatosis research. Eur RespirRev. 2011;20:3---6.
5. Harari S, Torre O, Moss J. Lymphangioleiomyomatosis: whatdo we know and what are we looking for? Eur Respir Rev.2011;20:34---44.
6. Dilling DF, Gilbert ER, Picken MM, Eby JM, Love RB, Le Poole IC.A current viewpoint of lymphangioleiomyomatosis supportingimmunotherapeutic treatment options. Am J Respir Cell MolBiol. 2012;46:1---5.
7. Johnson SR, Cordier JF, Lazor R, Cottin V, Costabel U, Harari S,et al. European Respiratory Society guidelines for the diagnosisand management of lymphangioleiomyomatosis. Eur Respir J.2014;35:14---26.
8. Glasgow CG, El-Chemaly S, Moss J. Lymphatics in lymphangi-oleiomyomatosis and idiopathic pulmonary fibrosis. Eur RespirRev. 2012;21:196---206.
9. McCormack FX, Inoue Y, Moss J, Singer LG, Strange C, Nakata K,et al. Efficacy and safety of Sirolimus in lymphangioleiomy-omatosis. N Engl J Med. 2011;364:1595---606.
0. Moua T, Olson EJ, St Jean HC, Ryu JH. Resolution of chylous pul-monary congestion and respiratory failure in LAM with Sirolimustherapy. Am J Respir Crit Care Med. 2012 [Epub ahead ofprint].
.M. Restrepo-Gualterosa,b, C.E. Rodriguez-Martinezc,d,e,∗,
.E. Jaramillo-Barberi f,g, A.F. Lopez-Cadenah,i, G. Ninoj
Department of Pediatric Pulmonology, Fundacion Hospitala Misericordia, Bogota, ColombiaDepartment of Pediatrics, School of Medicine. FundacionantaFe de Bogota, Universidad de los Andes, Bogota,olombiaDepartment of Pediatrics, School of Medicine,niversidad Nacional de Colombia, Bogota, ColombiaDepartment of Pediatric Pulmonology and Pediatricritical Care Medicine, School of Medicine, Universidad Elosque, Bogota, ColombiaResearch Unit, Military Hospital of Colombia, Bogota,olombiaDepartment of Pathology, School of Medicine,niversidad Nacional de Colombia, Bogota, ColombiaDepartment of Pathology, Fundación Hospital Laisericordia, Bogota, ColombiaDepartment of Radiology, School of Medicine,niversidad El Bosque, Bogota, ColombiaDepartment of Radiology, Fundación Hospital Laisericordia, Bogota, Colombia
Sleep Medicine and Integrative Systems Biology, Theeorge Washington University School of Medicine andealth Sciences, Children’ National Medical Center, Centeror Genetic Medicine Research (CGMR), Washington, DC,SA
l. Adolescent form of sporadic lymphangioleiomyomatosisg/10.1016/j.aller.2013.10.004
Corresponding author.-mail addresses: [email protected],[email protected] (C.E. Rodriguez-Martinez).