Embed Size (px)
Citation preview

GastrointestinalManifestations ofFood Allergies
Jaime Liou Wolfe, MDa, Seema S. Aceves, MD, PhDb,*
KEYWORDS
� Eosinophilic esophagitis � Eosinophilic gastroenteritis� Food allergy � Allergy testing
INTRODUCTION
IgE-mediated food hypersensitivity affects 4% of children in the United States, withincreasing incidence rates over the last 10 years. In addition, an increasing numberof children with food allergy are reporting other concurrent allergic diatheses suchas asthma, eczema, and allergic rhinitis. The eosinophilic gastrointestinal disorders(EGIDs), often a manifestation of food allergy, have become increasingly prevalentover the past 20 years, with eosinophilic esophagitis affecting at least 4/10,000 USchildren, with case reports on all continents except Africa.1,2
Manifestations of food allergy range from clinical anaphylaxis, mediated primarily byspecific IgE and immediate hypersensitivity, to EGIDs, which are mediated throughcombined IgE hypersensitivity and delayed-type hypersensitivity. Subsets of EGIDssuch as eosinophilic colitis seem to be largely IgE independent. Additional diseasesthat involve food intolerance include autoimmune processes, such as in celiacdisease. Understanding the multiple mechanisms and manifestations of food allergyis of paramount importance when choosing the appropriate diagnostic modality andinterpreting the test results. Immediate hypersensitivity reactions to foods areassessed by testing that evaluates the presence and/or levels of food-specific IgE.This can be achieved using skin prick testing (SPT) or serum specific IgE levels. Serumfood-specific IgE levels can have prognostic usefulness in children with a history ofurticaria, respiratory distress, hypotension, and other clinical symptoms of anaphy-laxis. In contrast, autoantibody testing for tissue transglutaminase and endomysialIgA are used in the diagnosis of celiac disease. Food atopy patch testing is intendedto evaluate a delayed hypersensitivity to foods but remains a research tool.
a Division of Gastroenterology, Department of Surgery, Children’s National Medical Center,Washington, DC, USAb Division of Allergy, Immunology, Departments of Pediatrics and Medicine, University ofCalifornia, San Diego, Rady Children’s Hospital, San Diego, CA, USA* Corresponding author. Division of Allergy and Immunology, 3020 Children’s Way, MC-5114,San Diego, CA 92123.E-mail address: [email protected]
Pediatr Clin N Am 58 (2011) 389–405doi:10.1016/j.pcl.2011.02.001 pediatric.theclinics.com0031-3955/11/$ – see front matter � 2011 Elsevier Inc. All rights reserved.

Wolfe & Aceves390
This article reviews the clinical manifestations, pathogenesis, testing modalities,and treatments of food allergies that involve the gastrointestinal (GI) tract.
EOSINOPHILIC ESOPHAGITISClinical Features
Eosinophilic esophagitis (EoE) is a clinicopathologic condition defined by diffuseeosinophilic infiltration of the esophagus. It is becoming increasingly recognized inadults and children, and the first consensus guidelines for its diagnosis and manage-ment were published in 2007.2 The recommended guideline diagnostic criteria werebased on published literature and expert opinion, and were defined as: (1) character-istic symptoms, (2) 15 eosinophils/high power field (HPF) or greater, and (3) exclusionof other disorders, including failure of response with high-dose proton pump inhibitors(PPI) therapy, or normal pH monitoring.2
EoE was first described in the mid-1970s by Dobbins and colleagues3 and Landresand colleagues,4 who reported 2 adult men with symptoms of dysphagia, epigastricpain, esophageal spasms, and eosinophilia of the esophagus with negative pHprobes. In 1993, Atwood and colleagues5 published a retrospective review of12 patients with increased esophageal eosinophils. In this study, 11 of 12 patientshad normal pH monitoring and 7 of 12 were atopic. Most patients had dysphagiaand frequent food impaction, and a mean of 56 eosinophils/HPF compared with90 patients with pH-probe–proven gastroesophageal reflux (GER) who had meaneosinophils of 3.3 eosinophils/HPF.Since its first description, the reports of EoE have steadily increased, with currently
reported incidence rates of 1.25/10,000 and prevalence of 4.3/10,000 in children lessthan 19 years of age.1 It is more common in young White males, and affected patientshave high rates of concurrent atopy.6 Greater than 70% of patients have a history ofasthma, eczema, food allergies or food sensitization, environmental allergy, or chronicrhinitis, and up to 75% have a personal or family history.2 Current reports show thata subset of patients have a genetic variant of EoE and reported disease risk genesfor EoE include eotaxin-3 and thymic stromal lymphopoeitin and a single nucleotidepolymorphisms at the transforming growth factor b1 (TGFb1) promoter may havedisease-modifying effects on therapeutic response. Eotaxin-3 genotype GG wasstatistically significant in patients with EoE versus controls and comprised 14% ofthe patients with EoE.7–9
Classic EoE symptoms include abdominal pain, vomiting, and dysphagia, althoughsymptoms vary by age.2 Infants and toddlers present with gagging, choking, feedingrefusal, or poor growth. Whereas GER symptoms tend to improve in the second half ofthe first year, symptoms from EoE may not. Feeding difficulties likely arise fromnausea, dysphagia, or the attempt to avoid pain with eating, which are perpetuatedby continual negative reinforcement. When evaluating these children, primaryswallowing dysfunction, cardiac or respiratory disease, and underlying anatomicabnormalities must also be considered and evaluated.School-aged children tend to present with pain or vomiting. Pain can vary in loca-
tion, frequency, and severity, with complaints of chest, epigastric, or periumbilicalpain being most common.2 Symptoms rarely occur in association with a particularfood trigger, tend to be intermittent, and tend not to predict the severity ofinflammation.10 In some instances, parents may recall an infant in whom reflux symp-toms began early in life, were associated with eczema, and worsened with the intro-duction of solid foods.11
Dysphagia and food impaction are more common in adolescents and adults. Theassociation of dysphagia with EoE has been reported as high as 80% and is the

Gastrointestinal Manifestations of Food Allergies 391
most frequent indication for endoscopic evaluation in adults.12–14 Endoscopic ultra-sound has shown the thickening of the entire mucosa and muscular layers of theesophagus, which may affect esophageal motility.15 Dysphagia has not been directlyrelated to the duration of inflammation or degree of eosinophilic infiltration, but chronicinflammation with subsequent tissue remodeling has been postulated, and dysphagiacomplaints correlate directly with episodes of dysmotility in pediatric patients.16 Adultpatients with EoE have chronic complaints of dysphagia when treated with intermittentdilation only.17
Histologic Features
The esophagus, unlike other areas of the GI tract, is normally devoid of eosinophils.However, esophageal eosinophilia can occur with other diseases including GERdisease, connective tissue disorders, parasitic infections, inflammatory boweldisease, and as a drug reaction. In addition, adults with allergic rhinitis can haveesophageal eosinophilia during the pollen season independently of an EoEdiagnosis.18 Other causes of esophageal eosinophilia must be investigated beforediagnosing primary EoE.Histologically, EoE esophageal biopsies have several characteristic features,
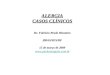
including eosinophil microabscesses, degranulation, and superficial layering as wellas basal zone hyperplasia and vascular papillary elongation.2 EoE is diagnosedwhen there are at least 15 eosinophils or more per HPF on 400� light microscopy usinga hematoxylin and eosin stain (Fig. 1).2 The eosinophil count of the highest density seen(peak eosinophils) is currently used in diagnosis. Unlike acid-induced esophagealeosinophilia, EoE is a patchy, diffuse disease. Procuring 5 biopsies increases the
Fig. 1. Eosinophilic esophagitis. Eosinophilic abscesses and numerous eosinophils.

Wolfe & Aceves392
diagnostic yield to more than 90%. In addition, obtaining biopsies from at least 2 levelsof the esophagus is recommended.19
Endoscopic Features
Endoscopic findings can be obvious or subtle. Up to 30% of patients with histologicEoE have an endoscopically normal mucosa.2 However, classic EoE findings includelinear furrowing, concentric rings (or felinization/trachealization), white exudates thatmimic Candida, friability, or an attenuated subepithelial vascular pattern (Fig. 2).2
Small-caliber esophagus, characterized by a uniformly narrowed esophagus, alsohas been described in patients with EoE with dysphagia.20 Ongoing inflammationmay lead to esophageal strictures, the most severe EoE complication reported todate.
Distinction of EoE from GER
Almost 2 decades ago, Winter and colleagues21 reported distal and proximal esoph-ageal eosinophilia in patients with GER. Whereas GER biopsies tend to have fewerthan 7 eosinophils in the distal esophagus, EoE biopsies show significantly moresevere eosinophilia.22,23 Liacouras and colleagues24 showed an average of 34.2 �9.6 eosinophils/HPF in patients with EoE compared with children with esophagitiswho responded to PPI therapy (2.26 � 1.16 eosinophils/HPF, P<.001). Case-controlstudies of patients with EoE versus GER show that EoE is more often associatedwith younger age, dysphagia, endoscopic findings such as rings and furrows, andeosinophil degranulation, severe basal zone hyperplasia, and lamina propriafibrosis.25–27
Because of the similarities in symptom complex, the clinical distinction betweenGER and EoE is particularly challenging. However, dysphagia and anorexia/earlysatiety have been reported to both correlate with inflammation, remodeling, and todistinguish GER from EoE in children.28 Symptomatically, children with GER tend toimprove with acid suppression therapy, whereas patients with EoE remain partiallyor completely symptomatic despite acid blockade.2 Adult studies have shown thatinfusion of acid into the esophagus of patients with EoE causes significant pain.29
However, the interplay between EoE and acid may be complex, involving an unclearrelationship between eosinophilic secretory factors as well as epithelial changes
Fig. 2. Esophageal exudates in EoE (A). Linear furrowing and concentric rings (felinization/trachealization) in the esophagus (B).

Gastrointestinal Manifestations of Food Allergies 393
secondary to acid damage.30 Consistent with this hypothesis, Ngo and colleagues31
described 3 patients with mean esophageal eosinophil counts of 36 (range 21–52)who responded both clinically and histologically to isolated acid suppression. Forthis reason, a trial of acid suppression before establishing the diagnosis of EoE isrecommended.32 In addition, this complexity underscores the importance of repeatendoscopic and biopsy evaluation after each therapeutic intervention in patientswith EoE.
Disease Mechanisms
EoE combines immediate and delayed-type hypersensitive reactions to inhaled andingested antigens. Murine EoE models have been instructive in dissecting the mech-anistic pathways of esophageal inflammation. Experimental EoE is instigated by intra-nasal aeroallergens (Aspergillus, Dermatophagoides) and gavaged food allergens(ovalbumin).33–35 Disease initiation depends on the presence of T cells but is indepen-dent of IgE.36 Animals deficient in CD41 T cells, eotaxin receptor CCR3, interleukin15 (IL-15) receptor a, IL-13 receptor a, or IL-5 are all relatively to completely protectedfrom experimental EoE, showing the importance of these pathways in EoE.7,37,38
Gene microarray studies have significantly contributed to our understanding ofhuman EoE pathogenesis.7 Compared with normal children or patients with GER,children with EoE have a 53-fold increase in the expression of eotaxin-3, a chemokinethat functions as an eosinophil chemoattractant. Both IL-5 and IL-13 are increasedand seem to function upstream of eotaxin-3. Treatment of cultured human esophagealepithelial cells from patients with EoE with IL-13 causes increased eotaxin-3 geneexpression.39 More recently, IL-15, which can function in a similar manner to IL-2,has been shown to be increased in pediatric patients with EoE, is expressed indendritic cells in EoE, increases IL-5 and IL-13 production from T cells as well aseotaxin-3 production from epithelial cells, and is detectable in the serum of patientswith EoE.37 CD81 cells are increased in biopsies of patients with EoE, and it ispossible that IL-15 is important in their genesis and maintenance.40,41
IL-5 is important for both eosinophilopoesis and eosinophil trafficking into theesophagus. In addition, IL-5 in combination with eotaxins activates eosinophils.Patients with EoE show increased deposition of eosinophil granule products, includingmajor basic protein, eosinophil derived neurotoxin, and eosinophil peroxidase.42–44
These products can potentially affect esophageal function by increasing tissuedamage and epithelial proliferation.45
In IgE-mediated hypersensitivity, mast cells classically mediate the downstreameffects of specific IgE. EoE biopsies have shown increased numbers of mast cellsas well as increased mast cell degranulation compared with non-EoE biopsies, sug-gesting mast cell activation.46 In addition, there are increased numbers of tryptase-positive mast cells and IgE-positive cells as well as increased numbers of cells bearingthe high-affinity IgE receptor, FceRI, in the esophagus of patients with EoE.47,48
Whereas tryptase-positive mucosal mast cells are decreased after topical corticoste-roid treatment,49 the submucosal mast cell pool of tryptase-chymase double connec-tive tissue mast cells remains static.50 A mast cell gene profile is increased in pediatricpatients with EoE.7,51 Mast cells are increased in number in the esophageal muscularismucosa and their products are able to affect esophageal smooth-muscle function invitro, suggesting an important function of mast cells in EoE pathogenesis.50 A localcapacity for immunoglobulin class switch occurs in the esophagus but whether localIgE production represents a mucosal food-specific antigen response remains to beshown.47 Increased levels of esophageal IL-13 could promote local immunoglobulinclass switch to IgE production in EoE.

Wolfe & Aceves394
The role of systemic food-specific IgE remains to be further elucidated in EoE.Although most patients have sensitization to food antigens, the role of IgE in predictingfoods that instigate or propagate EoE is unclear and SPT or serum IgE-based dietaryeliminations are variably successful.
Pathogenesis of Complications
The most severe consequence of EoE is fixed esophageal stenosis requiring repeateddilation. Subepithelial sclerosis was first reported in adult patients with long-standingEoE.17 Children, both with and without stricture-associated EoE, have subepithelialremodeling, an esophageal process with a pathogenesis akin to asthmatic airwayremodeling.52 Increases in TGFb1 and its signaling pathway, phosphorylatedSmad2/3, are found in the subepithelium of individuals with EoE. Increased angiogen-esis, a component of esophageal remodeling, and vascular activation with vascularcell adhesion molecule 1 form adhesive conduits for inflammatory cell trafficking.52
In addition to increased collagen deposition, increased amounts of matrix proteinssuch as periostin allow eosinophil accumulation.53 Animal models have shown thatIL-5 and eosinophils are necessary for tissue remodeling, whereas in vitro studiesshow that TGFb1 and eotaxin-3 increase periostin expression in esophagealfibroblasts.38
Food Allergy Testing in EoE
Immediate hypersensitivityFood testing that evaluates immediate hypersensitivity reactions evaluates the pres-ence of specific IgE. SPT is performed by placing food extracts or fresh foods onthe skin and pricking the skin. Cutaneous mast cells carrying food-specific IgE arestimulated to degranulate, which causes a cutaneous urticarial reaction. SPT gaugesboth the presence and function of specific IgE.Serum IgE testing assesses the levels of food-specific IgE. In the context of a clinical
history of anaphylaxis or immediate food hypersensitivity reaction (urticaria, vomiting,angioedema), the quantity of serum specific IgE can have predictive values for thereaction to specific foods. However, it is critical to understand that although manypeople generate food-specific IgE that is detectable by SPT or in vitro testing theycan be clinically tolerant to the food and have no reaction on ingestion. In some cases,removal of IgE-positive foods in a clinically tolerant person can result in immediatehypersensitivity on food reintroduction, implying that continued food ingestion isimportant for maintaining tolerance. Although most patients with EoE have detectablelevels of food-specific IgE, they do not have anaphylaxis. The reason for this remainsunclear.Serum or skin testing for foods in EoE reveals that 70% to 80% of patients with EoE
have positive food testing.2 Serum IgE testing detects more foods than SPT but theclinical implication and usefulness of low-level sensitization to foods (in the range of1–5 IU/mL) is unclear.54 The most commonly positive foods in patients with EoEwho undergo SPT or serum IgE testing are cow’s milk, hen’s egg, soy, wheat, corn,rice, oat, beef, chicken, peanuts, and white potato.54,55
Delayed hypersensitivityDelayed hypersensitivity testing evaluates the presence of cellular inflammation inresponse to foods. T-cell memory is critical to the onset of delayed-type hypersensi-tivity. The use of atopy patch testing has been validated, standardized, and shown toprovoke a cutaneous cellular immune response in diseases such as contact dermatitisand eczema. The usual antigens in these cases are metals, occupational chemicals,

Gastrointestinal Manifestations of Food Allergies 395
and aeroallergens such as house dust mite. Food patch testing has been evaluated inEoE in order to assess foods that cause a delayed reaction. Single food extracts inFinn chambers are placed on the back for 48 hours. The reactions are read at 72 hoursand graded using a scoring system that evaluates the presence and severity oferythema, induration, papules, and vesicles. The most commonly positive foods onpatch testing of patients with EoE are cow’s milk, hen’s egg, wheat, soy, corn, barley,oat, rice, beef, and potato.55 Positive predictive values from 1 center range from 54%(potato) to 94% (beef), whereas negative predictive values range from 59% to 97%.55
The presence of a cutaneous cellular immune response has not yet been shown inEoE, large numbers of non-EoE control patients have not been evaluated, and theinterpretation of food patch tests has not been standardized or validated yet in EoE.Food patch testing remains a research tool in EoE.
Evidence that EoE is a Food Allergic GI Disease
Murine models of esophageal eosinophilia can be promoted by food antigens, specif-ically ovalbumin.35 Human data invoking foods as triggers of EoE come from thesuccess of elimination diets as EoE therapy. Elemental formulas are the mostsuccessful dietary intervention, with histologic resolution in more than 94% ofpatients.56,57 However, unpalatable taste requiring nasogastric or gastric tube inser-tions, lack of insurance coverage in many states, and difficulty with adherence limitthe use of elemental diets.In vitro studies looking at dendritic cells from patients with EoE and food allergic
patients show increased levels of Th2 cytokine production when cultured in vitrowith autologous CD41 cells and increased serum levels of IL-5 and IL-13.58 It ispossible that, similar to patients with eosinophilic gastroenteritis (EGE), patientswith EoE have increased numbers of CD41, IL-51, and IL-4� cells but this remainsto be evaluated.59
Kagalwalla and colleagues60 first described the use of an empiric 6-food eliminationdiet in children. Avoidance of cow’s milk, hen’s egg, soy, wheat, fish, shellfish,peanuts, and tree nut resulted in histologic remission in 74% of pediatric patients,again invoking immunologic food reactions in the esophagus as the basis for EoE.Consistent with atopy patch test and SPT-based diets, the most common food anti-gens in children were cow’s milk and hen’s egg. The same avoidance diet in adultsleads to 70% resolution or improvement, with disease recurrence on food reintroduc-tion. Milk and wheat were the most common adult EoE triggers (Nirmala Gonsalves,MD, personal communication, 2010).The long-term induction of tolerance to EoE triggering foods and the potential impli-
cations for loss of tolerance and onset of IgE-mediated allergy when using diets thateliminate IgE-positive foods remain to be studied in EoE.
EoE Therapy
As a food-triggered disease, EoE can be successfully managed using eliminationdiets, as detailed earlier. Other mainstays of EoE management are the use ofswallowed corticosteroids that deposit topically on the esophagus. By treating inflam-mation locally, topical corticosteroids control allergic inflammation and allow a widediet to be consumed. Success rates vary but randomized placebo-controlled trialsin children show that puff and swallowed fluticasone can be as effective as oral pred-nisone and significantly superior to placebo.49,61 Oral viscous budesonide in combina-tion with acid blockade daily is an effective EoE therapy, with response rates of 87%compared with placebo.62 Repeat endoscopy with biopsy should be performed afterchanging therapy or foods, because documentation of histologic resolution is required

Wolfe & Aceves396
in disease management. There are no surrogate markers, including symptoms, thatobviate repeated endoscopy in patients with EoE.
Therapeutic Maneuvers in EoE
Dilation therapy and food disimpaction are required less frequently in children than inadults with EoE. However, when dilation is required, care must be taken to avoidperforation. Several case studies in the literature support a higher perforation risk inEoE, believed to be caused by mucosal remodeling and fibrosis leading to a lesscompliant or fragile esophageal wall.63,64 However, recent studies have reportedthat perforation caused by dilation in patients with EoE may be safer than previouslybelieved.63,65,66 The role of antiinflammatory therapy in reducing or obviating dilationswarrants further study.
EOSINOPHILIC GASTROENTERITISClinical, Histologic, and Endoscopic Features
First described more than 50 years ago by Kaijser,67 EGE is a clinicopathologic enti-ty characterized by increased eosinophils in the stomach and small intestine, andless commonly the colon. It is rare, and the underlying pathophysiology is not clear.It is diagnosed primarily in the third to fifth decade of life, and affects both gendersequally. The incidence is not clear, likely because of lack of recognition andunderreporting.68
The definition of EGE is complicated by the baseline, normal eosinophilia of the non-esophageal regions of the GI tract. They are highest in the cecum, ascending colon,and terminal ileum.69,70 There is no consensus guideline regarding the number ofeosinophils required for diagnosis, but rather the combination of eosinophil location,depth, other histologic findings or lack thereof, the clinical context, and lack of signsof other diseases with eosinophilia help to direct diagnosis.71
Primary EGE can be atopic or nonatopic but is often believed be a food allergicdisorder, potentially with a genetic susceptibility.72 The most common cause ofsecondary EGE is parasitic infection but inflammatory bowel disease, celiacdisease, and connective tissue diseases such as scleroderma can also be associ-ated with EGE. Peripheral eosinophilia may be seen in more than 50%, but notconsistently, and its significance in terms of diagnostic criteria has not beenestablished.73
The stomach has been reported to be involved in 26% to 81% of cases, and thesmall intestine in 28% to 100% of cases.74,75 The most frequently described symp-toms are abdominal pain, diarrhea, nausea, vomiting, and weight loss.74–77 Symptomsmay wax and wane, and it is not uncommon for diagnosis to be delayed because oflack of consistency in symptoms. The most commonly accepted classification systemwas developed by Klein and colleagues78 in 1970, in which the disorder was dividedinto 3 subtypes: mucosal, muscularis, and serosal.Mucosal disease is the most frequently encountered, which is likely in part because
of the technical limitation in obtaining deep-layer biopsies via standard endoscopy.Individuals with mucosal-type disease tend to have IgE-mediated food allergy or otheratopy.79 Other presentations of mucosal disease include anemia caused byGI bleeding, gastric and duodenal ulcers, or protein-losing enteropathy caused bymalabsorption.71,73,80–83
Muscular disease tends to present with obstructive symptoms, and several uniquepresentations have been reported. Infants may present with gastric outlet obstruction,mimicking hypertrophic pyloric stenosis. Thickening of the intestinal wall, strictures,

Gastrointestinal Manifestations of Food Allergies 397
pancreatitis, intussusception, and obstruction by a cecal mass have also beendescribed.75,77,84,85 Diagnosis of muscular and serosal types may require laparotomyand full-thickness biopsy.Serosal disease is associated with abdominal bloating, marked increase in eosino-
phils, ascites, increased peripheral eosinophilia, and better response to steroids.Talley and colleagues74 published one of the largest experiences with EGE, in whichthey compared symptoms, allergic history, and serum parameters among patientswith EGE and control individuals and reported that abdominal bloating and peripheraleosinophil count were the only parameters found to be statistically different. However,obstructive jaundice, acute abdomen, intussusception, and bowel obstruction havealso been described.86–91
Diagnosis
Endoscopy and histology are required for diagnosis. Endoscopic findings vary fromnormal to nodular with friability, erythema, polypoid lesions, or ulcerations.72 Biopsiesshow increased eosinophils but the histologic finding of eosinophilia must be evalu-ated in the clinical context, and secondary causes such as inflammatory boweldisease and celiac disease that can also be associated with intestinal eosinophiliamust be evaluated. Like EoE, EGE disease is patchy and therefore multiple biopsiesshould be obtained.Diagnosis is made more difficult by the technical limitation of standard endoscopy.
The distal limit of upper endoscopic biopsies is the third portion of the duodenum,whereas the proximal limit of colonic endoscopies is the terminal ileum. With newerendoscopic techniques such as balloon enteroscopy, more distal small bowel biop-sies may be obtained and aid in EGE recognition.There are no radiographic findings specific to EGE, although computed tomography
of the abdomen may show nodular and irregular thickening of gastric folds.91
Ultrasound may also be helpful in assessing antral and bowel wall thickness.92 Bariumcontrast may show bowel wall thickening or strictures.
Pathogenesis
Patients with atopic EGE often have multiple food sensitizations with positive SPT.However, elimination diets based on SPT results have variable success. However,elemental formula can have significant success.93 Together the success of theseinterventions speaks to the important role of food intolerance in EGE.Because the usual response of the GI tract is tolerogenic, shifts in sensitization
to foods can lead to significant intestinal disease, and the role of food antigens inEGE continues to be investigated. Most recently Prussin and colleagues59
reported that peripheral, food-specific CD41 T cells in allergic patients withanaphylaxis produce both IL-4 and IL-5, whereas allergic EGE was singularlyassociated with a Th2 population that was IL-4�/IL-51 cells. The numbers ofIL-41,51 cells in peanut-allergic patients directly correlated with IgE levels.However, the link between the presence of peripheral IL-4�,51 cells and GIT cells and eosinophils remains ambiguous. In addition, earlier work showedthat patients with allergic EGE had duodenal CD41/IL-41 cells that proliferatedto milk.94 These cells were also noted to release IL-5 and IL-13 but not IL-4 inresponse to antigen, again implicating the importance of these interleukins tofood-related GI disease. Together, these studies provide evidence for a mechanismof eosinophil chemoattraction and activation via IL-5 in patients with a GI Th2phenotype and EGE.

Wolfe & Aceves398
Treatment
Patients with cow’s milk allergy and EGE can have IgE to casein and whey proteins. Itis reasonable to perform SPT to foods and, if not limited by the numbers of positivefoods, to trial an elimination diet. Amino acid-based formulas can be trialed for EGEif there are multiple positive foods on IgE testing or if no food triggers can be foundon IgE testing but the patient wishes to pursue dietary management. Although prolif-erative responses of peripheral blood mononuclear cells have been reported for milk,peanut, and soy proteins in patients with EGE, the extension of this disease mecha-nism to food patch testing has not been studied rigorously.A recent clinical trial reported that the biologic agent anti-IgE was successful in
decreasing eosinophil counts and symptoms in patients with EGE, underscoringa role for IgE in EGE.95 Although IL-5 can drive esophageal eosinophilia, its role inthe pathogenesis of EGE remains less clear and trials that were geared to assessthe role of anti-IL-5 therapy in EoE showed that there were no changes in the levelsof T cells, eosinophils, or mast cells in the duodenal or gastric mucosa of patientswith EoE treated with anti-IL-5.96
The treatment of EGE can be complex, requiring systemic immunomodulatorytherapy with prednisone, 6-mercaptopurine, and azathioprine.97 Because EGE ischaracterized by relapses and remissions, patients often require recurrent steroidcourses, with serosal disease having been reported to respond to systemic corticoste-roids. Long-term remission may be possible with the use of the leukotriene receptorantagonist montelukast.98 Because EGE has been associated with infections fromhelminths and Helicobacter pylori as well as systemic processes such as lupus eryth-ematosis and posttransplantation syndrome, it is of paramount importance to deter-mine if the disease is primary or secondary EGE before embarking on therapy.Depending on the location of intestinal involvement, topical corticosteroids such asentocort, a formulation of budesonide that targets right-sided intestinal disease, canbe instituted.
EOSINOPHILIC COLITIS/PROCTOCOLITIS
Most commonly a benign disease of infancy, milk and soy trigger proctocolitis mani-fests as bloody, mucus-containing stools in infancy and is easily treated by theremoval of the triggering antigen. Up to 60% of cases occur in breastfed babies,with onset during the first 6 months of life, and resolution by age 2 years old, withmany children tolerating regular diets by 1 year of age.99,100 Dietary elimination leadsto rapid resolution of symptoms within 72 to 96 hours.99 Because the diagnosis isbased on clinical history and improvement with elimination of cow’s milk in the breast-feeding mother, or with a semihydrolyzed or extensively hydrolyzed formula, neitherflexible sigmoidoscopy nor colonoscopy is routinely indicated. Gross visual findingsin the rectosigmoid colon may reveal erythema or erosions, whereas histologicallyone may see acute inflammation and eosinophilia. Although T cells are likely thesource of immunologic memory, the use of food patch testing is not warranted in theseinfants.
FOOD PROTEIN-INDUCED ENTEROCOLITIS SYNDROME
Food protein–induced enterocolitis syndrome (FPIES) is a non–IgE-mediated foodallergic disorder characterized by severe GI or systemic reactions to a food trigger,particularly milk or soy. Symptoms resolve with elimination of exposure to the incitingfood. After the first case series in 1967 of 21 infants with diarrhea and variable

Gastrointestinal Manifestations of Food Allergies 399
hemodynamic instability with exposure to milk protein,101 the diagnostic criteria havebeen formalized to include: (1) onset of symptoms typically at age less than 2 months,(2) diagnosis at age younger than 9 months; and (3) resolution of symptoms when thefood antigen is eliminated.102
FPIES typically presents with significant GI symptoms, primarily vomiting and diar-rhea within 4 hours of food ingestion.103 More than 75% of infants appear ill, and insome patients, systemic signs such as hypotension necessitate hospitalization.103
Common presentation in infants includes a septic appearance with a metabolicacidosis, dehydration, lethargy, and bloody stools. Because of this, children are oftenevaluated first for sepsis, metabolic disorders, or acute abdominal processes beforethe recognition of the triggering food antigen. Other signs such as hypoalbuminemia,poor weight gain, hypothermia, thrombocytosis, peripheral polymorphonuclearlymphocytosis, and methemoglobinemia have also been reported.102–105 The severityof symptoms and lack of awareness of FPIES often delay the diagnosis.Milk and soy are the most common food triggers, with as high as a 50% cross-
reactivity between milk and soy.102,106 Solid foods have also been implicated, partic-ularly rice.105,107,108 Most patients have negative SPTs and serum IgE test results.102
Patch testing may be a promising modality to aid in diagnosis.109
FPIES is a clinical diagnosis. The gold standard for diagnosis is a positive oral foodchallenge but this is often not necessary and can be dangerous if the reaction involveshypotension. When challenges are done, intravenous access and a minimum of4 hours of observation are necessary. Endoscopy is not routine because the diagnosiscan often be made clinically based on symptoms with exposure to the food trigger,and improvement with removal of the causative food. Histologic changes includeincreased eosinophils in the lamina propria and focal cryptitis, with overall preserva-tion of architecture.110–112
SUMMARY
Food reactions can have GI manifestations that cause significant tissue disease andpatient morbidity. It is essential to use the proper diagnostic testing, including endos-copy with biopsy and food allergy testing, and to interpret test results appropriately inorder to choose the best therapeutic intervention. New manifestations of food aller-gies, especially EoE, are increasing in prevalence and constitute a new and significanthealth care burden.
REFERENCES
1. Noel RJ, Putnam PE, Rothenberg ME. Eosinophilic esophagitis. N Engl J Med2004;26(351):940–1.
2. Furuta GT, Liacouras CA, Collins MH, et al. Eosinophilic esophagitis in childrenand adults: a systematic review and consensus recommendations for diagnosisand treatment. Gastroenterology 2007;133:1342–63.
3. Dobbins JW, Sheahan DG, Behar J. Eosinophilic gastroenteritis with esophagealinvolvement. Gastroenterology 1977;72(6):1312–6.
4. Landres RT, Kuster GG, Strum WB. Eosinophilic esophagitis in a patient withvigorous achalasia. Gastroenterology 1978;74(6):1298–301.
5. Attwood SE, Smyrk TC, Demeester TR, et al. Esophageal eosinophilia withdysphagia.Adistinct clinicopathologic syndrome.DigDisSci 1993;38(1):109–16.
6. Orenstein SR, Shalaby TM, Di Lorenzo C, et al. The spectrum of pediatric eosin-ophilic esophagitis beyond infancy: a clinical series of 30 children. Am J Gastro-enterol 2000;95(6):1422–30.

Wolfe & Aceves400
7. Blanchard C, Wang N, Stringer KF, et al. Eotaxin-3 and a uniquely conservedgene-expression profile in eosinophilic esophagitis. J Clin Invest 2006;116:536–47.
8. Rothenberg ME, Spergel JS, Sherrill JD, et al. Common variants at 5q22 asso-ciate with pediatric eosinophilic esophagitis. Nat Genet 2010;42:289–91.
9. Aceves SS, Newbury RO, Chen D, et al. Resolution of remodeling in eosinophilicesophagitis correlates with epithelial response to topical corticosteroids. Allergy2010;65:109–15.
10. Pentiuk S, Putnam PE, Collins MH, et al. Dissociation between symptoms andhistological severity in pediatric eosinophilic esophagitis. J Pediatr GstroenterolNutr 2009;48:152–60.
11. Putnam PE. Eosinophilic esophagitis in children: clinical manifestations. Gastro-enterol Clin North Am 2008;37:369–81.
12. Sgouros SN, Bergele C, Mantides A. Eosinophilic esophagitis in adults:a systematic review. Eur J Gastroenterol Hepatol 2006;18:211–7.
13. Desai TK, Stecevic V, Chang CH, et al. Association of eosinophilic inflammationwith esophageal food impaction in adults. Gastrointest Endosc 2005;61:795–801.
14. Kapel RC, Miller JK, Torres C, et al. Eosinophilic esophagitis: a prevalentdisease in the United States that affects all age groups. Gastroenterology2008;134:1316–21.
15. Fox VL, Nurko S, Teitelbaum JE, et al. High-resolution EUS in children with eosin-ophilic “allergic” esophagitis. Gastrointest Endosc 2003;57:30–6.
16. Nurko S, Rosen R, Furuta GT. Esophageal dysmotility in children with eosino-philic esophagitis: a study using prolonged manometry. Am J Gastroenterol2009;104:3050–7.
17. Straumann A, Spichtin HP, Grize L, et al. Natural history of primary eosinophilicesophagitis: a follow-up of 30 adult patients for up to 11.5 years. Gastroenter-ology 2003;125:1660–9.
18. Onbasi K, Sin AZ, Doganavsargil B, et al. Eosinophil infiltration of the oesopha-geal mucosa in patients with pollen allergy during the season. Clin Exp Allergy2005;35:1423–31.
19. Gonsalves N, Policarpio-Nicolas M, Zhang Q, et al. Histopathologic variabilityand endoscopic correlates in adults with eosinophilic esophagitis. GastrointestEndosc 2006;64:313–9.
20. Vasilopoulos S, Murphy P, Auerbach A, et al. The small-caliber esophagus: anunappreciated cause of dysphagia for solids in patients with eosinophilicesophagitis. Gastrointest Endosc 2002;55(1):99–106.
21. Winter HS, Madara JL, Stafford RJ, et al. Intraepithelial eosinophils: a new diag-nostic criterion for reflux esophagitis. Gastroenterology 1982;83:818–23.
22. Ruchelli E, Wenner W, Voytek T, et al. Severity of esophageal eosinophiliapredicts response to conventional gastroesophageal reflux therapy. PediatrDev Pathol 1999;2(1):15–8.
23. Steiner SJ, Gupta SK, Croffie JM, et al. Correlation between number of eosino-phils and reflux index on same day esophageal biopsy and 24 hour esophagealpH monitoring. Am J Gastroenterol 2004;99:801–5.
24. Liacouras C, Wenner WJ, Brown K, et al. Primary eosinophilic esophagitis inchildren: successful treatment with oral corticosteroids. J Ped Gastro Nutr1998;26:380–5.
25. Dellon ES, Gibbs WB, Fritchie KJ, et al. Clinical, endoscopic, and histologic find-ings distinguish eosinophilic esophagitis from gastroesophageal reflux disease.Clin Gastroenterol Hepatol 2009;7:1305–13.

Gastrointestinal Manifestations of Food Allergies 401
26. Parfitt JR, Gregor JC, Suskin NG, et al. Eosinophilic esophagitis in adults: dis-tinguishing features from gastroesophageal reflux disease: a study of 41patients. Mod Pathol 2006;19:90–6.
27. Aceves SS, Newbury RO, Dohil R, et al. Distinguishing eosinophilic esophagitisin pediatric patients: clinical, endoscopic, and histologic features of anemerging disorder. J Clin Gastroenterol 2007;41:252–6.
28. Aceves SS, Newbury RO, Dohil MA, et al. A symptom scoring tool for identifyingpediatric patients with eosinophilic esophagitis and correlating symptoms withinflammation. Ann Allergy Asthma Immunol 2009;103:401–6.
29. Krarup AL, Villadsen GE, Mejlgaard E, et al. Acid hypersensitivity in patients witheosinophilic esophagitis. Scan J Gastroenterol 2010;45:273–81.
30. Spechler SJ, Genta RM, Souza RF. Thoughts on the complex relationshipbetween gastroesophageal reflux disease and eosinophilic esophagitis. Am JGastroenterol 2007;102:1301–6.
31. Ngo P, Furuta GT, Antonioli DA, et al. Eosinophils in the esophagus–peptic orallergic eosinophilic esophagitis? Case series of three patients with esophagealeosinophilia. Am J Gastroenterol 2006;101:1666–70.
32. Walsh SV, Antonioli DA, Goldman H, et al. Allergic esophagitis in children: a clin-icopathological entity. Am J Surg Pathol 1999;23:390–6.
33. Mishra A, Hogan SP, Brandt EB, et al. An etiological role for aeroallergens andeosinophils in experimental esophagitis. J Clin Invest 2001;107:83–90.
34. Rayapudi M, Mavi P, Zhu X, et al. Indoor insect allergens are potent inducersof experimental eosinophilic esophagitis in mice. J Leukoc Biol 2010;88:337–46.
35. Song DJ, Cho JY, Lee SY, et al. Anti-Siglec-F antibody inhibits oral egg allergen-induced intestinal eosinophilic inflammation in a mouse model. Clin Immunol2009;131:157–69.
36. Mishra A, Schlotman J, Wang M, et al. Critical role for adaptive T-cell immu-nity in experimental eosinophilic esophagitis in mice. J Leukoc Biol 2007;81:916–24.
37. Xiang Z, Wang M, Mavi P, et al. Interleukin-15 expression is increased in humaneosinophilic esophagitis and mediates pathogenesis in mice. Gastroenterology2010;139:182–93.
38. Mishra A, Wang M, Pemmaraju VR, et al. Esophageal remodeling develops asa consequence of tissue specific IL-5-induced eosinophilia. Gastroenterology2008;134:204–14.
39. Blanchard C, Mingler MK, Vicario M, et al. IL-13 involvement in eosinophilicesophagitis: transcriptome analysis and reversibility with glucocorticoids.J Allergy Clin Immunol 2007;120:1292–300.
40. Lucendo AJ, Navarro M, Comas C, et al. Immunophenotypic characterizationand quantification of the epithelial inflammatory infiltrate in eosinophilic esopha-gitis through stereology: an analysis of the cellular mechanisms of the diseaseand the immunologic capacity of the esophagus. Am J Surg Pathol 2007;31:598–606.
41. Teitelbaum J, Fox V, Twarog F, et al. Eosinophilic esophagitis in children: immu-nopathological analysis and response to fluticasone propionate. Gastroenter-ology 2002;122:1216–25.
42. Mueller S, Aigner T, Neureiter D, et al. Eosinophil infiltration and degranulation inoesophageal mucosa from adult patients with eosinophilic oesophagitis: a retro-spective and comparative study on pathological biopsy. J Clin Pathol 2006;59:1175–80.

Wolfe & Aceves402
43. Kephart GM, Alexander JA, Arora AS, et al. Marked deposition of eosinophilderived neurotoxin in adult patients with eosinophilic esophagitis. Am J Gastro-enterol 2010;105:298–307.
44. Protheroe C, Woodruff SA, dePetris G, et al. A novel histologic scoring system toevaluate mucosal biopsies from patients with eosinophilic esophagitis. Clin Gas-troenterol Hepatol 2009;7:749–55.
45. Mulder DJ, Pacheco I, Hurlbut DJ, et al. FGF-9 induced proliferative response toeosinophilic inflammation in oesophagitis. Gut 2009;58:166–73.
46. Kirsch R, Bokhary R, Marcon MA, et al. Activated mucosal mast cells differen-tiate eosinophilic (allergic) esophagitis from gastroesophageal reflux disease.J Pediatr Gastroenterol Nutr 2007;44:20–6.
47. Vicario M, Blanchard C, Stringer KF, et al. Local B cells and IgE production inoesophageal mucosa in eosinophilic oesophagitis. Gut 2010;59:12–20.
48. Yen EH, Hornick JL, Dehlink E, et al. Comparative analysis of FcER1 expressionpatterns in patients with eosinophil and reflux esophagitis. J Pediatr Gastroen-terol Nutr 2010;51(5):584–92.
49. Konikoff MR, Noel RJ, Blanchard C, et al. A randomized, double blind, placebo-controlled trial of fluticasone propionate for pediatric eosinophilic esophagitis.Gastroenterology 2006;131:1381–91.
50. Aceves SS, Chen D, Newbury RO, et al. Mast cells infiltrate the esophagealsmooth muscle in patients with eosinophilic esophagitis, express TGFb1 andincrease esophageal smooth muscle contraction. J Allergy Clin Immunol2010;126:1198–204.
51. Albonia JP, Blanchard C, Butz BB, et al. Involvement of mast cells in eosinophilicesophagitis. J Allergy Clin Immunol 2010;126:140–9.
52. Aceves SS, Newbury RO, Dohil R, et al. Esophageal remodeling in pediatriceosinophilic esophagitis. J Allergy Clin Immunol 2007;119:206–12.
53. Blanchard C, Mingler MK, McBride M, et al. Periostin facilitates eosinophil tissueinfiltration in allergic lung and esophageal responses. Mucosal Immunol 2008;1:289–96.
54. Erwin EA, James HR, Gutekunst HM, et al. Serum IgE measurement and detec-tion of food allergy in pediatric patients with eosinophilic esophagitis. AnnAllergy Asthma Immunol 2010;104:496–502.
55. Spergel JM, Brown-Whitehorn T, Beausoleil JL, et al. Predictive values for skinprick test and atopy patch test for eosinophilic esophagitis. J Allergy Clin Immu-nol 2007;119:509–11.
56. Markowitz JE, Spergel JM, Ruchelli E, et al. Elemental diet is an effective treat-ment for eosinophilic esophagitis in children and adolescents. Am J Gastroen-terol 2003;98:777–82.
57. Liacouras CA, Spergel JM, Ruchelli E, et al. Eosinophilic esophagitis:a 10-year experience in 381 children. Clin Gastroenterol Hepatol 2005;3:1198–206.
58. Frischmeyer-Guerrerio PA, Guerrerio AL, Chichester KL, et al. Dendritic celland T cell responses in children with food allergy. Clin Exp Allergy 2011;41(1):61–71.
59. Prussin C, Lee J, Foster B. Eosinophilic gastrointestinal disease and peanutallergy are alternatively associated with IL-51 and IL-5-Th2 responses.J Allergy Clin Immunol 2009;124:1326–32.
60. Kagalwalla AF, Sentongo TA, Ritz S, et al. Effect of six-food elimination diet onclinical and histologic outcomes in eosinophilic esophagitis. Clin GastroenterolHepatol 2006;4:1097–102.

Gastrointestinal Manifestations of Food Allergies 403
61. Schaefer ET, Fitzgerald JF, Molleston JP, et al. Comparison of oral prednisoneand topical fluticasone in treatment of eosinophilic esophagitis: a randomizedtrial in children. Clin Gastroenterol Hepatol 2008;6:165–73.
62. Dohil R, Newbury R, Fox L, et al. Oral viscous budesonide is effective in childrenwith eosinophilic esophagitis in a randomized placebo controlled trial. Gastro-enterology 2010;139:418–29.
63. Dellon ES, Gibbs WB, Rubinas TC, et al. Esophageal dilation in eosinophilicesophagitis: safety and predictors of clinical response and complications. Gas-trointest Endosc 2010;71:706–12.
64. Straumann A, Bussmann C, Zuber M, et al. Eosinophilic esophagitis: analysis offood impaction and perforation in 251 adolescent and adult patients. Clin Gas-troenterol Hepatol 2008;6:598–600.
65. Schoepfer AM, Gonsalves N, Bussmann C, et al. Esophageal dilation in eosin-ophilic esophagitis: effectiveness, safety, and impact on the underlying inflam-mation. Am J Gastroenterol 2010;105:1062–70.
66. Jacobs JW Jr, Spechler SJ. A systematic review of the risk of perforation duringesophageal dilation for patients with eosinophilic esophagitis. Dig Dis Sci 2010;55:1512–5.
67. Kaijser R. Allergic disease of the gut from the point of view of the surgeon. ArchKlin Chir 1937;188:36–64, 183:195–201.
68. Oh HE, Chetty R. Eosinophilic gastroenteritis: a review. J Gastroenterol 2008;43:741–50.
69. Lowichik A, Weinberg AG. A quantitative evaluation of mucosal eosinophils inthe pediatric gastrointestinal tract. Mod Pathol 1996;9(2):110–4.
70. DeBrosse CW, Case JW, Putnam PE, et al. Quantity and distribution of eosin-ophils in the gastrointestinal tract of children. Pediatr Dev Pathol 2006;9(3):210–8.
71. Kelly KJ. Eosinophilic gastroenteritis. J Pediatr Gastroenterol Nutr 2000;30:S28–35.
72. Simon D, Wardlaw A, Rothenberg ME. Organ specific eosinophilic disorders ofthe skin, lung, and gastrointestinal tract. J Allergy Clin Immunol 2010;126:3–13.
73. Redondo-Cerezo E, Cabello MJ, Gonzalez Y, et al. Eosinophilic gastroenteritis:our recent experience: one-year experience of atypical onset of an uncommondisease. Scand J Gastroenterol 2001;36:1358–60.
74. Talley NJ, Shorter RG, Phillips SF, et al. Eosinophilic gastroenteritis: a clinico-pathological study of patients with disease of the mucosa, muscle layer, andsubserosal tissues. Gut 1990;31:54–8.
75. Lee CM, Changchien CS, Chen PC, et al. Eosinophilic gastroenteritis: 10 yearsexperience. Am J Gastroenterol 1993;88:70–4.
76. Guajardo JR, Plotnick LM, Fende JM, et al. Eosinophil-associated gastrointes-tinal disorders: a world-wide-web based registry. J Pediatr 2002;141(4):576–81.
77. Chen MJ, Chu CH, Lin SC, et al. Eosinophilic gastroenteritis: clinical experiencewith 15 patients. World J Gastroenterol 2003;9(12):2813–6.
78. Klein NC, Hargrove RL, Sleisenger MH, et al. Eosinophilic gastroenteritis. Medi-cine 1970;40:299–319.
79. Gonsalves N. Food allergies and eosinophilic gastrointestinal illness. Gastroen-terol Clin North Am 2007;36:75–91.
80. Siaw EK, Sayed K, Jackson RJ. Eosinophilic gastroenteritis presenting as acutegastric perforation. J Pediatr Gastroenterol Nutr 2006;43:691–4.
81. Markowitz JE, Russo P, Liacouras CA. Solitary duodenal ulcer: a new presenta-tion of eosinophilic gastroenteritis. Gastrointest Endosc 2000;52:673–6.

Wolfe & Aceves404
82. Friesen CA. Clinical efficacy and pharmacokinetics of montelukast in dyspepticchildren with duodenal eosinophilia. J Pediatr Gastroenterol Nutr 2004;38:343–51.
83. Jacobson LB. Diffuse eosinophilic gastroenteritis: an adult form of allergic gas-troenteropathy. Report of a case with probable protein-losing enteropathy. Am JGastroenterol 1970;54:580–8.
84. Tursi A, Rella G, Inchingolo CD, et al. Gastric outlet obstruction due to gastro-duodenal eosinophilic gastroenteritis. Endoscopy 2007;39:E184.
85. Lyngbaek S, Adamsen S, Aru A, et al. Recurrent acute pancreatitis due to eosin-ophilic gastroenteritis. Case report and literature review. JOP 2006;9:211–7.
86. Whitaker IS, Gulati A, McDaid JO, et al. Eosinophilic gastroenteritis presentingas obstructive jaundice. Eur J Gastroenterol Hepatol 2004;16:407–9.
87. Tran D, Salloum L, Tshibaka C, et al. Eosinophilic gastroenteritis mimickingacute appendicitis. Am Surg 2000;66(10):990–2.
88. Shweiki E, West JC, Klena JW, et al. Eosinophilic gastroenteritis presenting asan obstructing cecal mass–a case report and review of the literature. Am J Gas-troenterol 1999;94:3644–5.
89. Yun MY, Cho YU, Park IS, et al. Eosinophilic gastroenteritis presenting as smallbowel obstruction: a case report and review of the literature. World J Gastroen-terol 2007;13:1758–60.
90. Siahanidou T, Mandyla H, Dimitriadis D, et al. Eosinophilic gastroenteritiscomplicated with perforation and intussusception in a neonate. J Pediatr Gas-troenterol Nutr 2001;32:335–7.
91. Vitellas KM, Bennett WF, Bova JG, et al. Radiographic manifestations of eosin-ophilic gastroenteritis. Abdom Imag 1995;20:406–13.
92. Maroy B. Nonmucosal eosinophilic gastroenteritis: sonographic appearance atpresentation and during follow-up of response to prednisone therapy. J ClinUltrasound 1998;26:483–6.
93. Chehade M, Magid MS, Mofidi S, et al. Allergic eosinophilic gastroenteritis withprotein losing enteropathy: intestinal pathology, clinical course, and long termfollow up. J Pediatr Gastroenterol Nutr 2006;42:516–21.
94. Beyer K, Castro R, Birnbaum A, et al. Human milk specific mucosal lymphocytesof the gastrointestinal tract display a Th2 cytokine profile. J Allergy Clin Immunol2002;109:707–13.
95. Foroughi S, Foster B, Kim NY, et al. Anti-IgE treatment of eosinophil associatedgastrointestinal disorders. J Allergy Clin Immunol 2007;120:594–601.
96. Conus S, Straumann A, Bettler E, et al. Mepolizumab does not alter levels ofeosinophils, T cells, and mast cells in the duodenal mucosa in eosinophilicesophagitis. J Allergy Clin Immunol 2010;120:175–6.
97. Netzer P, Gschossmann JM, Staumann A, et al. Corticosteroid dependent eosin-ophilic oesophagitis: azathioprine and 6-mercaptopurine can induce and main-tain long term remission. Eur J Gastroenterol Hepatol 2007;19:865–9.
98. Quack I, Sellin L, Buchner NJ, et al. Eosinophilic gastroenteritis in a young girl–long term remission under montelukast. BMC Gastroenterology 2005;5:24–9.
99. Garcia-Careaga M Jr, Kerner JA. Gastrointestinal manifestations of food aller-gies in pediatric patients. Nutr Clin Pract 2005;20:526–35.
100. Lake AM. Food-induced eosinophilic proctocolitis. J Pediatr Gastroenterol Nutr2000;30:S58–60.
101. Gryboski J. Gastrointestinal milk allergy in infancy. Pediatrics 1967;40:354–62.102. Sicherer SH, Eigenmann PA, Sampson HA. Clinical features of food protein-
induced enterocolitis syndrome. J Pediatr 1998;133(2):214–9.

Gastrointestinal Manifestations of Food Allergies 405
103. Nowak-Wegrzyn A, Muraro A. Food protein-induced enterocolitis syndrome.Curr Opin Allergy Clin Immunol 2009;9:371–7.
104. Hwang JB, Lee SH, Kang YN, et al. Indexes of suspicion of typical cow’s milkprotein-induced enterocolitis. J Korean Med Sci 2007;22:993–7.
105. Mehr S, Kakakios A, Frith K, et al. Food protein-induced enterocolitis syndrome:16-year experience. Pediatrics 2009;123:e459–64.
106. Burks AW, Casteel HB, Fiedorek SC, et al. Prospective oral food challenge studyof two soybean protein isolates in patients with possible milk or soy proteinenterocolitis. Pediatr Allergy Immunol 1994;5:40–5.
107. Nowak-Wegrzyn A, Sampson HA, Wood RA, et al. Food protein-induced entero-colitis syndrome caused by solid food proteins. Pediatrics 2003;111(4):829–35.
108. Levy Y, Danon YL. Food protein-induced enterocolitis syndrome–not only due tocow’s milk and soy. Pediatr Allergy Immunol 2003;14(4):325–9.
109. Fogg MI, Brown-Whitehorn TA, Pawlowski NA, et al. Atopy patch test for thediagnosis of food protein-induced entero-colitis syndrome. Pediatr Allergy Im-munol 2006;17(5):351–5.
110. Goldman H, Provjanksy R. Allergic proctitis and gastroenteritis in children. Am JSurg Pathol 1986;10:75–86.
111. Machida HM, Catto Smith AG, et al. Allergic colitis in infancy: clinical and path-ologic aspects. J Pediatr Gastroenterol Nutr 1994;19(1):22–6.
112. Arvola T, Ruuska T, Keranen J, et al. Rectal bleeding in infancy: clinical, allergo-logical, and microbiological examination. Pediatrics 2006;117(4):e760–8.