Embed Size (px)
Citation preview

Agenda 7:00 AM Optional Breakfast and Registration
8:00 AM Welcome & Introductions Dr. Bresee
8:10AM
Why Regionalization is Important Lessons from Regional System Models Elements of the Ideal System Guideline Review of Reperfusion Strategy Data Solutions Shock
Dr. Hadley Wilson Stephanie Starling
9:45 AM BREAK Accelerator
10:00 AM Regional Systems of Care Demonstration Project: Mission: Lifeline STEMI ACCELERATOR
Hadley Wilson, MD, FACC Stephanie Starling
10:30 AM Assessing the Landscape Mapping the Region Regional Faculty/AHA Staff
11:30 AM Challenging Case Studies from the Region EMS/Transfer/Shock Cases
Sunil T. Ramaprasad, MD FACC Mukesh K. Sarma, MD, FACC
12:00 PM LUNCH
1:00 PM Challenging Case Studies Stuart J. Breese, MD
1:30 PM Next Steps Group Discussion
2:00 PM Adjourn
AGENDA
Regionalization of STEMI Systems
Hadley Wilson, MD, FACC Chief of Cardiology, Sanger Heart and Vascular Institute, Charlotte, NC Physician and Regional STEMI System Implementer
Stephanie Starling, RN, BSN, MHA Director of Nursing at Forsyth Medical Center, Winston-Salem, NC Nurse and Regional STEMI System Implementer

Welcome & Introductions
• Regional Leadership
• AHA Local Staff & Affiliate Staff

Welcome
• Blount Memorial
• Fort Sander Regional
• LeConte Medical Center
• Methodist Medical Center
• Morristown Hamblen Healthcare
• Parkwest Medical Center
• Tennova Healthcare
• Turkey Creek Medical Center
• UT Medical Center
• First Call Ambulance Service • Morristown Hablen EMS • Rural Metro EMS – Knox County
Regional Systems of Care CME Objectives
• Describe existing successful STEMI regional plans that are pertinent to a wide array of geographical and political realities.
• Identify collaborative solutions to overcome existing barriers to coordinated regional STEMI care.
• Establish a framework for the accelerated development, enhancement and training of multidisciplinary STEMI teams in their regional practice areas.
• Agree upon best data tool to establish a baseline data for the region and monitor process and outcomes improvement on a quarterly basis.
• Discuss pros and cons of the current system practices.
• Identify available tools to provide feedback for necessary quality improvement for STEMI care.

Why Regionalize?
We already have a system, why regionalize?
• Most effective approach to modifying the system, particularly
EMS and hospitals that refer to more than one PCI center.
If every PCI hospital is has the same message, protocols
change.
• Fill in the existing gaps / chasm in healthcare
Competing hospitals
Loose EMS – hospital affiliations
• Only possible way to overcome the “longest breath hold”… two
hour transfer device times.
Two hours is a long time for a myocyte to hold its breath.
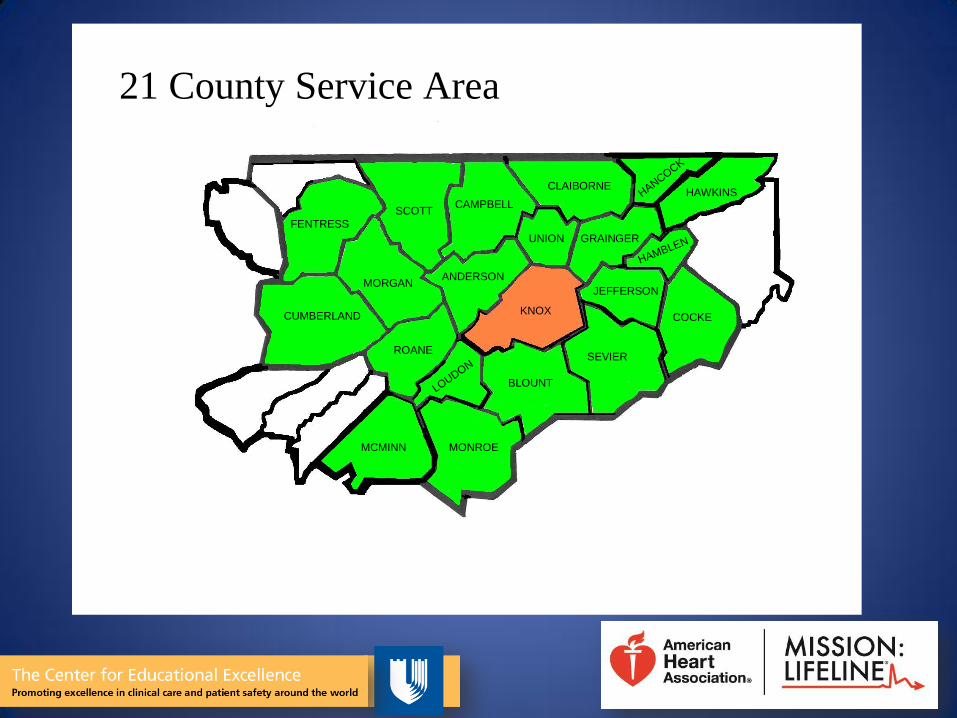
CUMBERLAND
FENTRESS
SCOTT
MORGAN
ROANE
MCMINN MONROE
BLOUNTLOUDON
SEVIER
COCKE
ANDERSON
CAMPBELL
CLAIBORNE
UNION
JEFFERSON
GRAINGER
HAMBLEN
HANCOCK
HAWKINS
KNOX
21 County Service Area
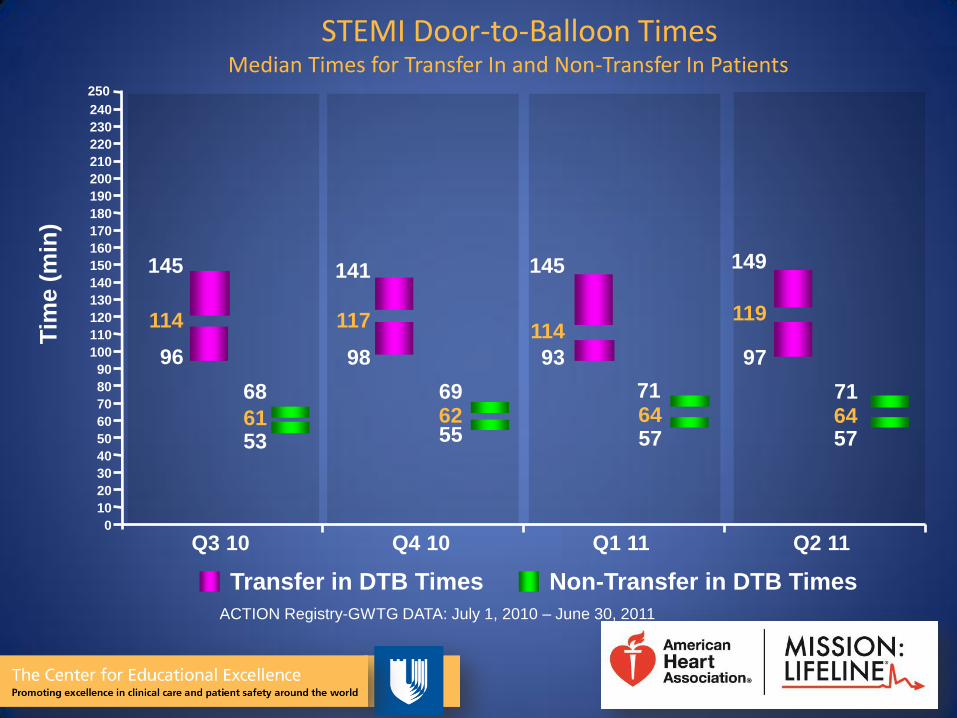
STEMI Door-to-Balloon Times Median Times for Transfer In and Non-Transfer In Patients
Transfer in DTB Times Non-Transfer in DTB Times
96
114
145
53 61
68
Q3 10
98
117
141
55 62 69
Q4 10
93
114
145
57 64
Q1 11
97
119
149
57 64 71
Q2 11
Tim
e (
min
)
50
220
210
60
70
80
90
110
100
120
130
140
150
160
170
200
180
190
240
230
71
40
30
20
250
10
0
ACTION Registry-GWTG DATA: July 1, 2010 – June 30, 2011
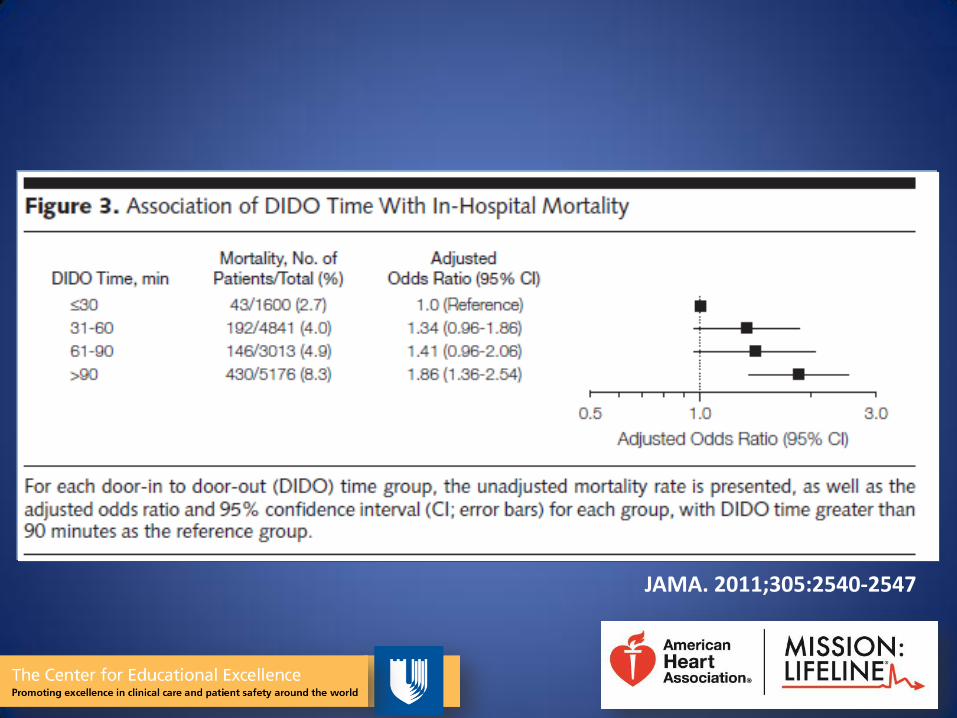
JAMA. 2011;305:2540-2547

We already have a system, why regionalize?
• Without regional approach to data collection, impossible to improve system coordination.
• Provide a platform for regional care of other cardiovascular emergencies… cardiac arrest, stroke, aortic dissection….

We already have a system, why regionalize?
# 1 Reason- Save lives
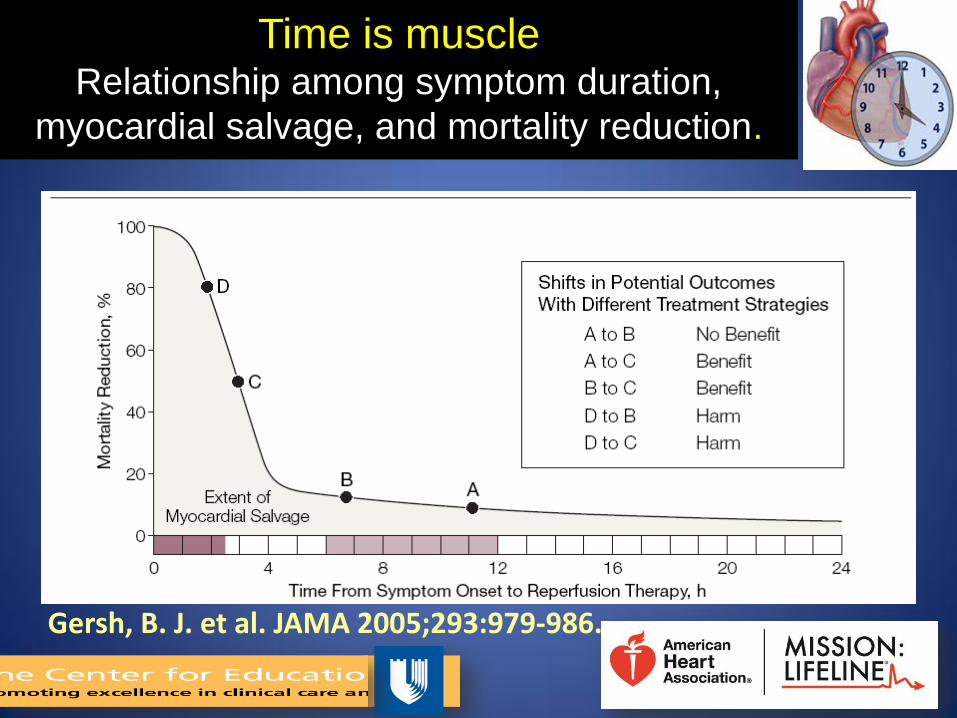
Time is muscle Relationship among symptom duration,
myocardial salvage, and mortality reduction.
Gersh, B. J. et al. JAMA 2005;293:979-986.
Levels of organization
Hub and spoke model
Regional system
Every hospital and EMS Agency
Individual hospital
Journal of Invasive Cardiology 2011; 23 A:8-12
A system that includes all hospitals within a region,
establishes common hospital and EMS protocols, and shares
common data
Regional system
• Patients walk in to every hospital and call every EMS agency… all need a plan.
• Regional leadership involving all major hospitals is more effective at influencing referring hospitals and EMS agencies.
– If all leading professionals and institutions in a region agree, recommendations more likely to be adopted.
• Single approach enhances rapid treatment.
– everyone knows their role, no hesitation to find out who is on call…. Journal of Invasive Cardiology 2011; 23 A:8-12
Regional system Advantages
Regional System
Barriers / Opportunities • Competition
– most commonly cited reason
• Apathy in Leadership
• Conflicting management plans
– “5 doctors will give you 6 different plans”
• Resources
– “Feet on the street” system coordinators
• Lack of comparable regional data for ongoing quality improvement and immediate feedback loop for all members of the team
Circ Cardiovasc Qual Outcomes. 2012;5:423-428
Regional Cardiovascular Emergency System
• How are we doing
– EMS to device
– Hospital transfer
• Regionalization
• Building regional system
• Mission: Lifeline STEMI SYSTEMS ACCELERATOR Intervention

How patients present • Call 911 EMS
(~50%)
• Walk-in
(~50%)
• Hospital transfer
• - Walk in or EMS to 1st
hospital
(~60% of PCI hospital)
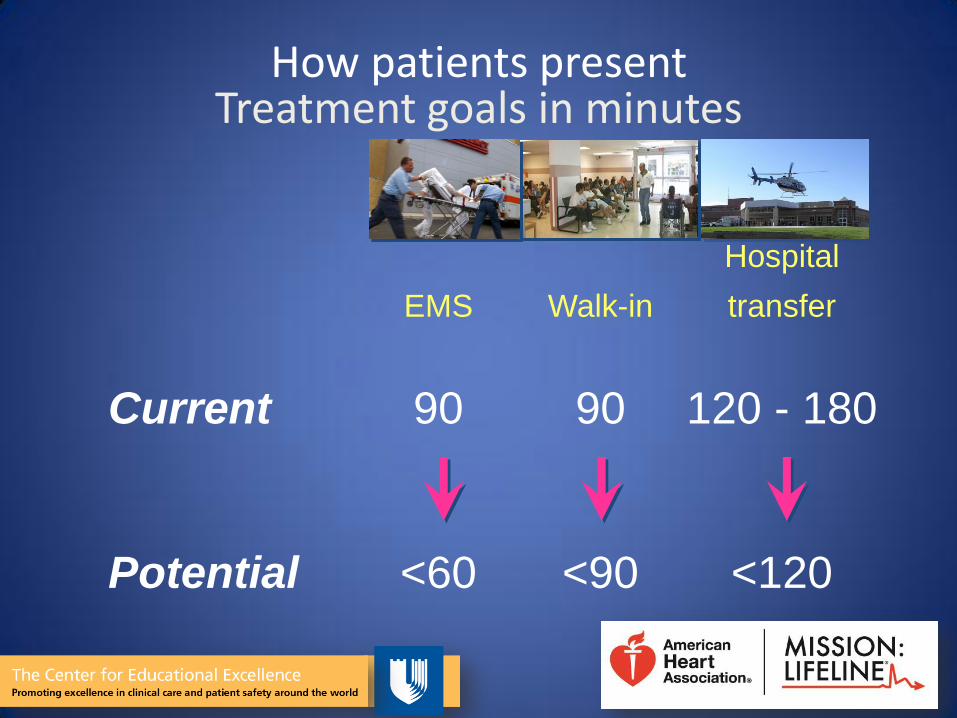
How patients present Treatment goals in minutes
EMS
Walk-in
Hospital
transfer
Current 90 90 120 - 180
Potential <60 <90 <120
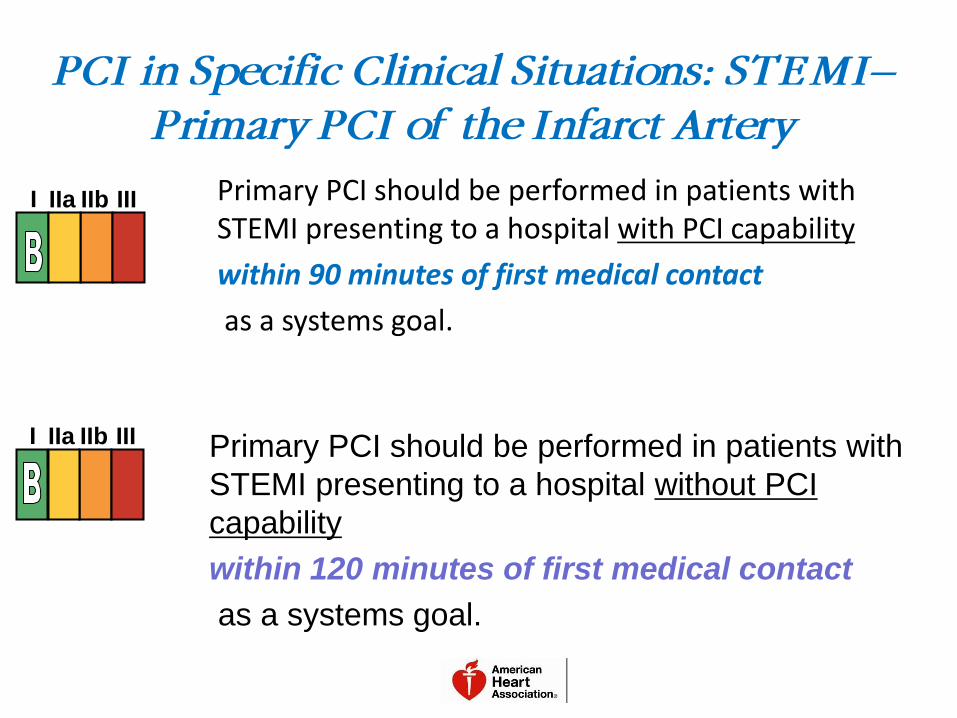
Primary PCI should be performed in patients with STEMI presenting to a hospital with PCI capability
within 90 minutes of first medical contact
as a systems goal.
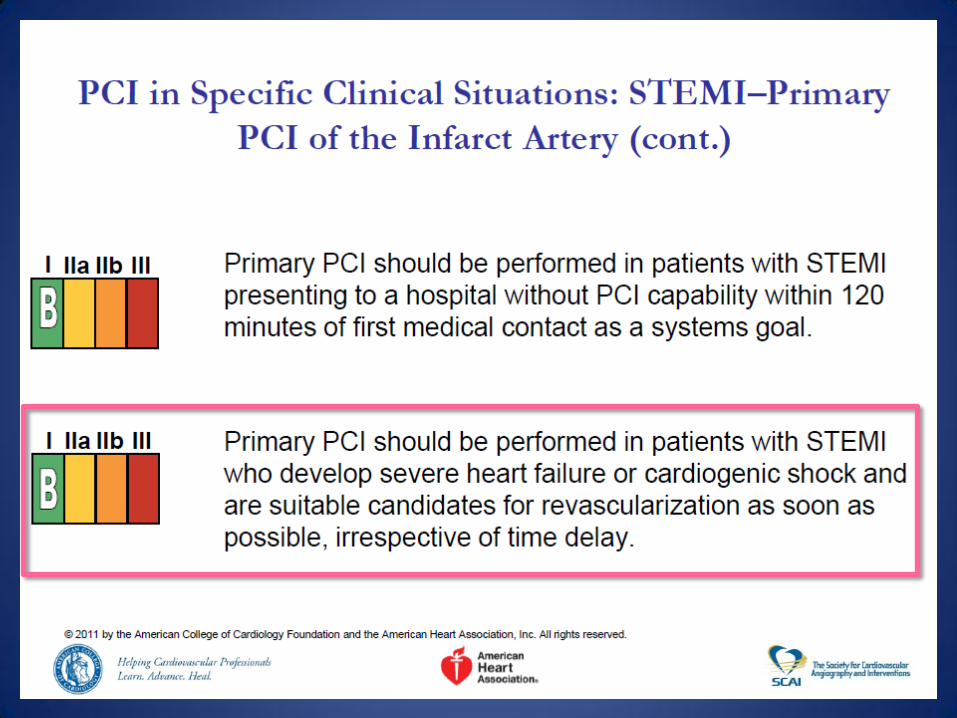
PCI in Specific Clinical Situations: STEMI–
Primary PCI of the Infarct Artery
I IIa IIb III
Primary PCI should be performed in patients with
STEMI presenting to a hospital without PCI
capability
within 120 minutes of first medical contact
as a systems goal.
I IIa IIb III
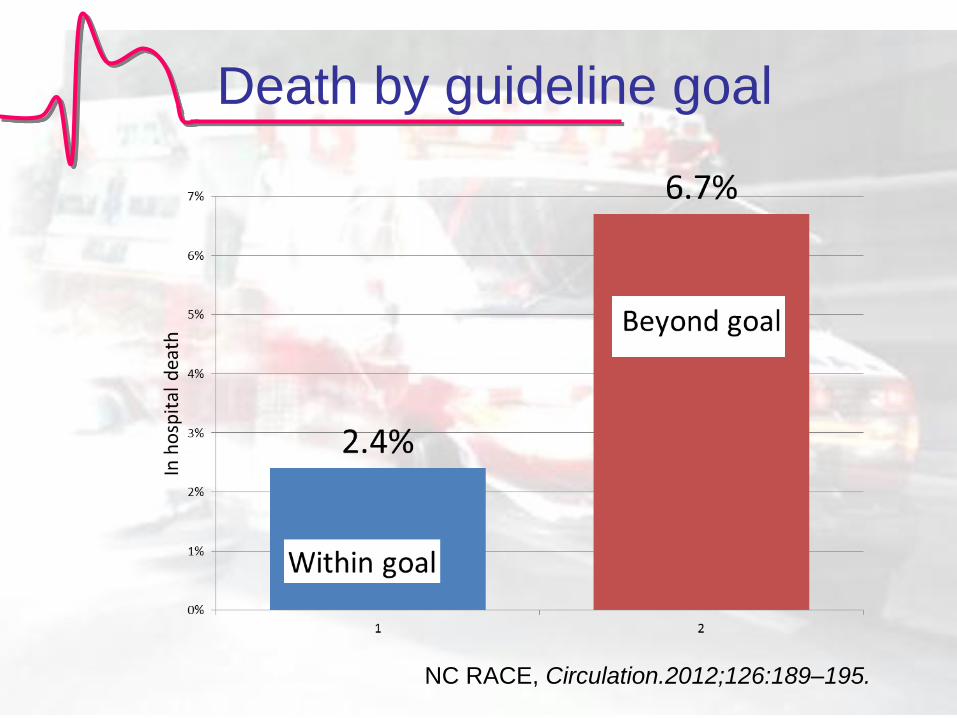
Death by guideline goal
NC RACE, Circulation.2012;126:189–195.
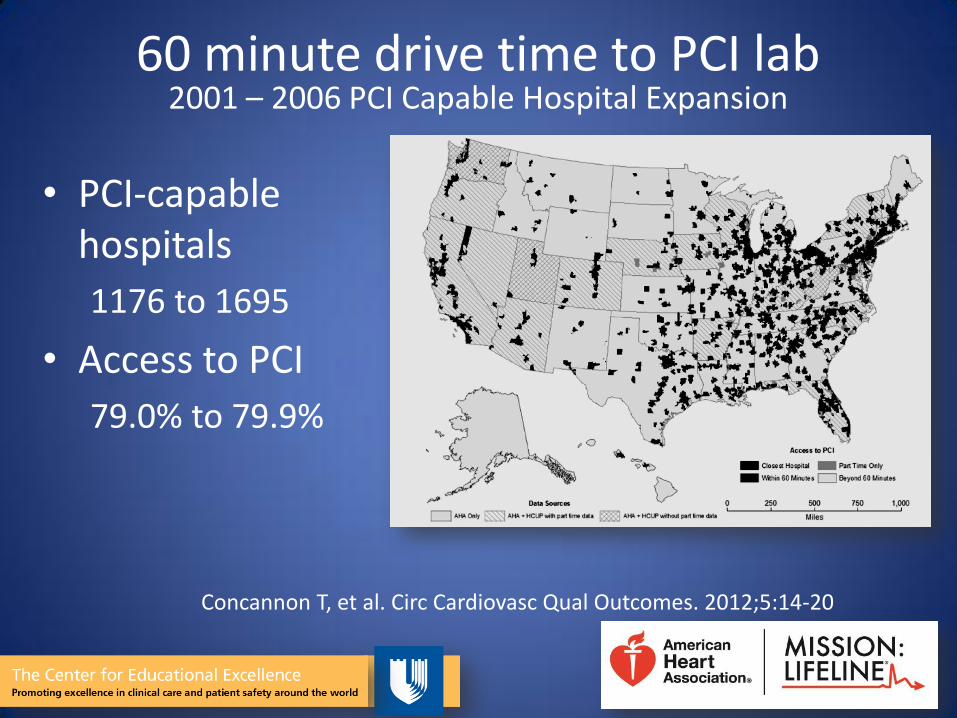
60 minute drive time to PCI lab 2001 – 2006 PCI Capable Hospital Expansion
• PCI-capable hospitals
1176 to 1695
• Access to PCI
79.0% to 79.9%
Concannon T, et al. Circ Cardiovasc Qual Outcomes. 2012;5:14-20
10/8/2012
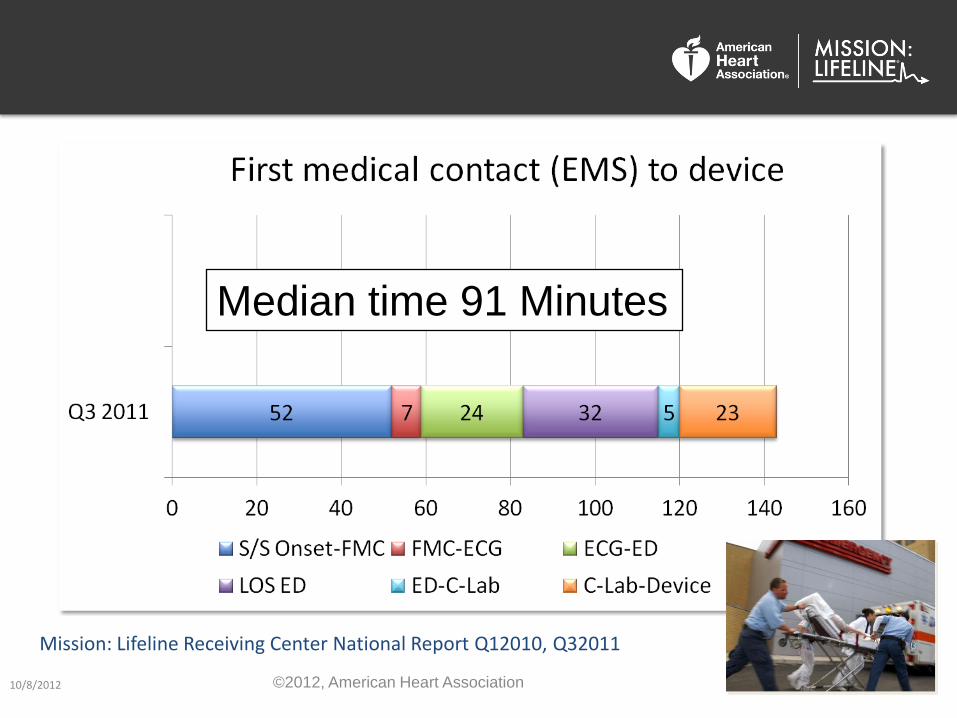
Mission: Lifeline Receiving Center National Report Q12010, Q32011
25
Median time 91 Minutes
©2012, American Heart Association

Regional Cardiovascular Emergency System How are we doing?
• Door to balloon largely solved • Major targets remain
1. Hospital transfer patients (roughly half or all STEMI patients)
First door to device
2. EMS diagnosed patients (roughly half of patients presenting directly to PCI hospitals
First medical contact to device
Regionalization Can Look Very Different Across the Country…….Depending on
Where you are living
RACE
Reperfusion in AMI in Carolina
Emergency Departments
Regionalization of Emergency Cardiac Care
“Most of the important decisions that
impact patient outcomes occur long
before the patients reaches the
cardiologist”
Regionalization of Emergency Cardiac Care
Move care forward…
• EMS does emergency department job
• Emergency department does cardiology
job
• Cardiology lives in the cath. lab / intensive
care unit
Diagnose quickly
Reperfuse quickly
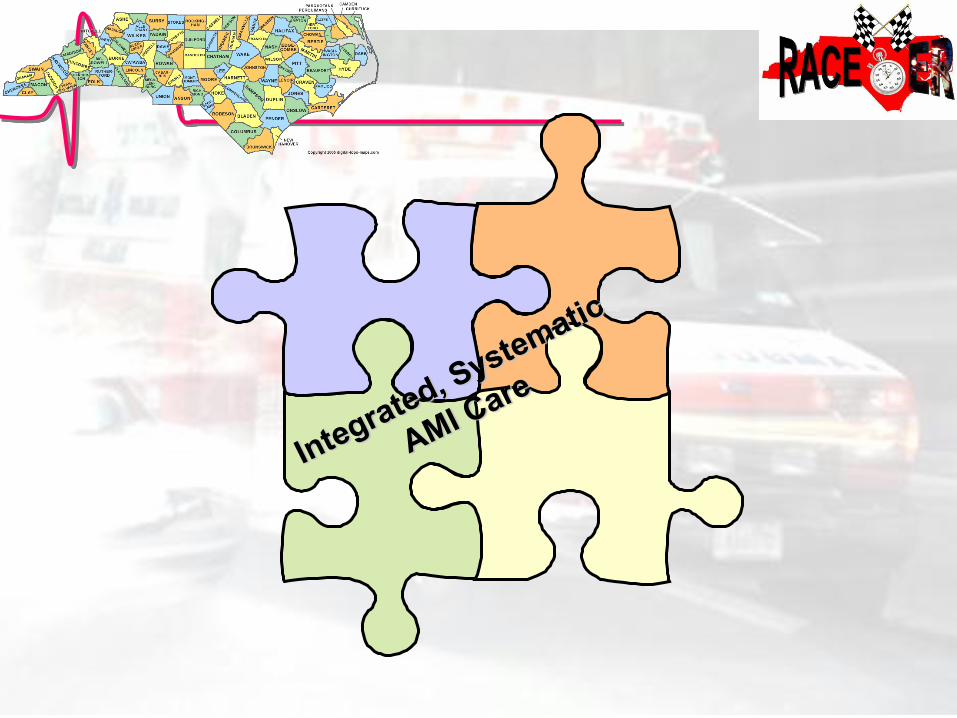
ST Elevation Myocardial Infarction
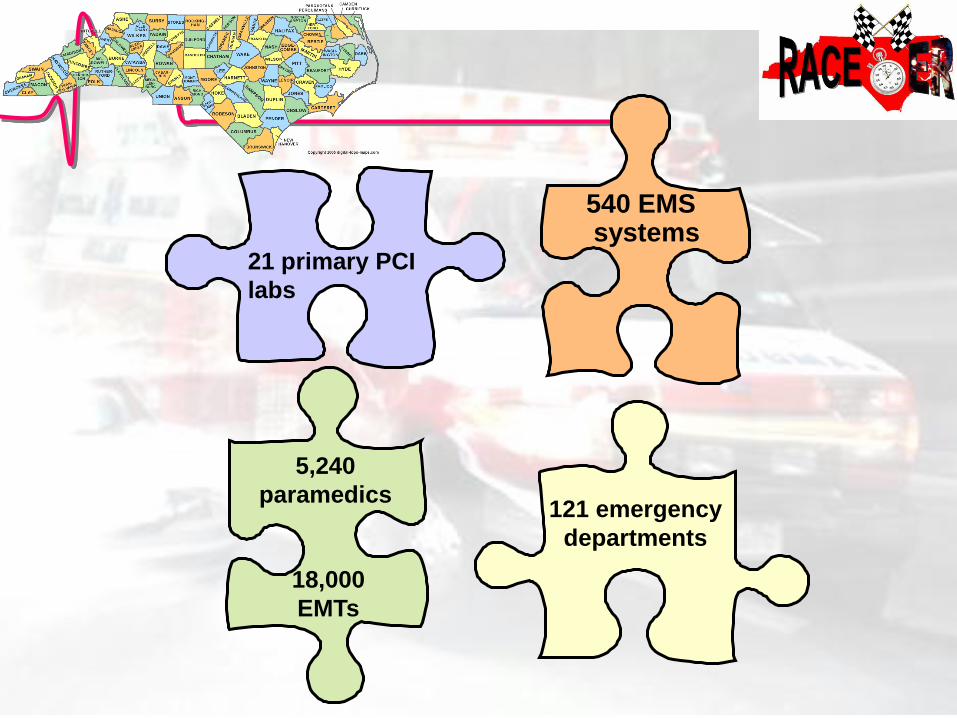
121 emergency
departments
540 EMS systems
5,240
paramedics
18,000
EMTs
21 primary PCI
labs
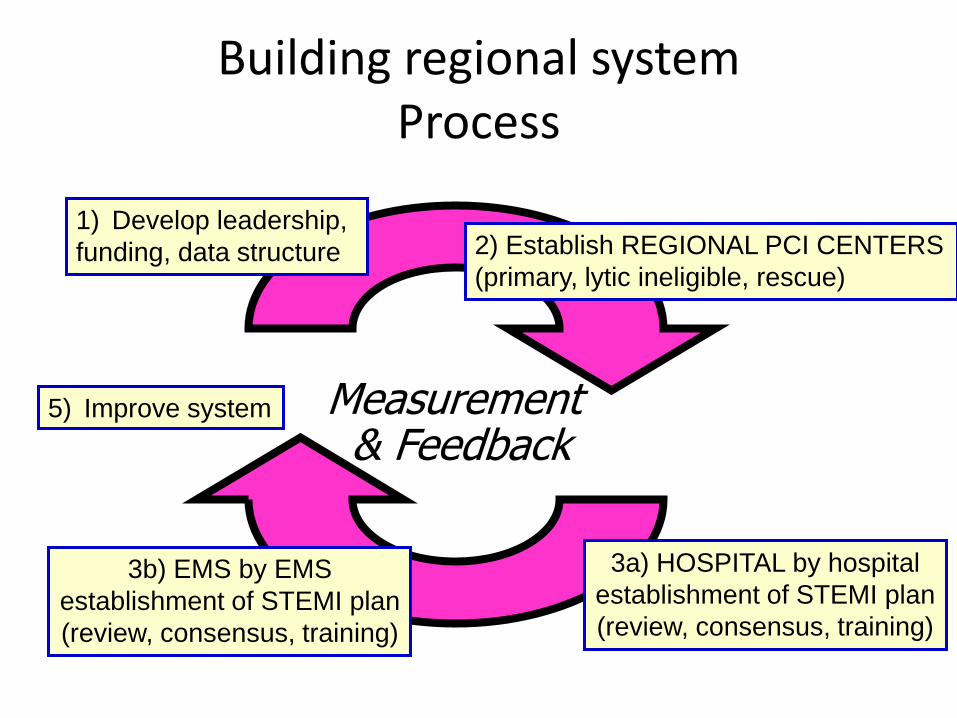
Building regional system Process
2) Establish REGIONAL PCI CENTERS
(primary, lytic ineligible, rescue)
Measurement & Feedback
3a) HOSPITAL by hospital
establishment of STEMI plan
(review, consensus, training)
3b) EMS by EMS
establishment of STEMI plan
(review, consensus, training)
5) Improve system
1) Develop leadership,
funding, data structure
Regional Coordinator(s)
Directed by regional leadership to implement
emergency care plans.
Lead establishment of STEMI plan in every hospital
and EMS agency.
Day to day oversight and coordination of system.
Training of EMS, ED, catheterization lab, and QI
personnel
Regular data feedback to hospitals, EMS agencies,
and regional meetings.
Establish a STEMI plan
• Optimal system specifications
by point of care
– EMS
– ED
– Transfer
– Receiving hospital
– Cath. Lab
– Other system issues –
payers, regulations
Develop a regional plan
Available at http://www.nccacc.org/news/news1.html
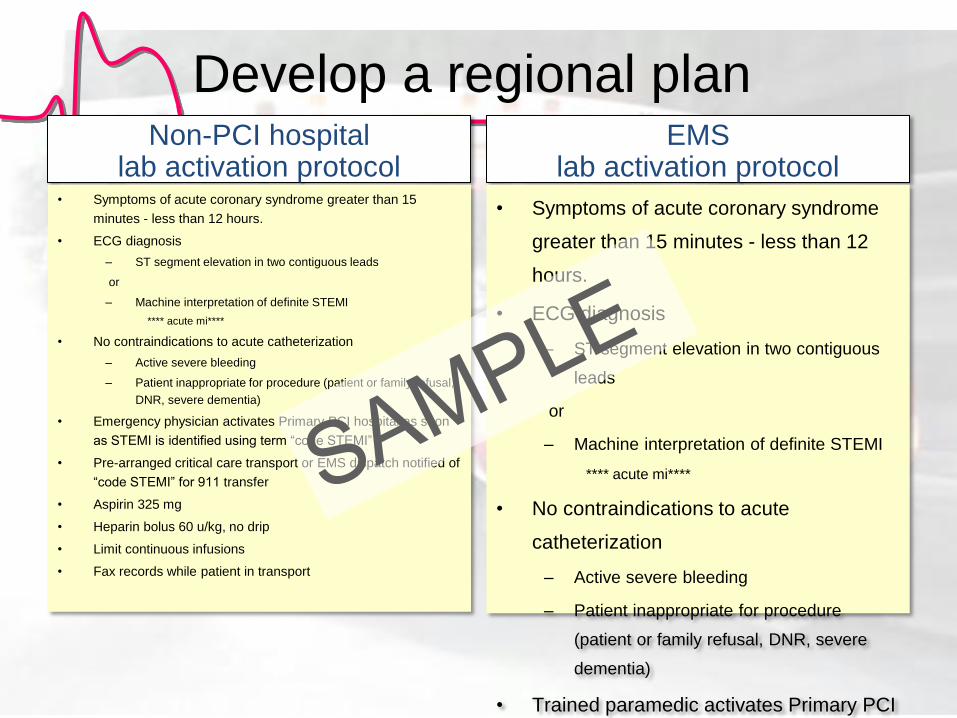
Non-PCI hospital lab activation protocol
• Symptoms of acute coronary syndrome greater than 15
minutes - less than 12 hours.
• ECG diagnosis
– ST segment elevation in two contiguous leads
or
– Machine interpretation of definite STEMI
**** acute mi****
• No contraindications to acute catheterization
– Active severe bleeding
– Patient inappropriate for procedure (patient or family refusal,
DNR, severe dementia)
• Emergency physician activates Primary PCI hospital as soon
as STEMI is identified using term “code STEMI”
• Pre-arranged critical care transport or EMS dispatch notified of
“code STEMI” for 911 transfer
• Aspirin 325 mg
• Heparin bolus 60 u/kg, no drip
• Limit continuous infusions
• Fax records while patient in transport
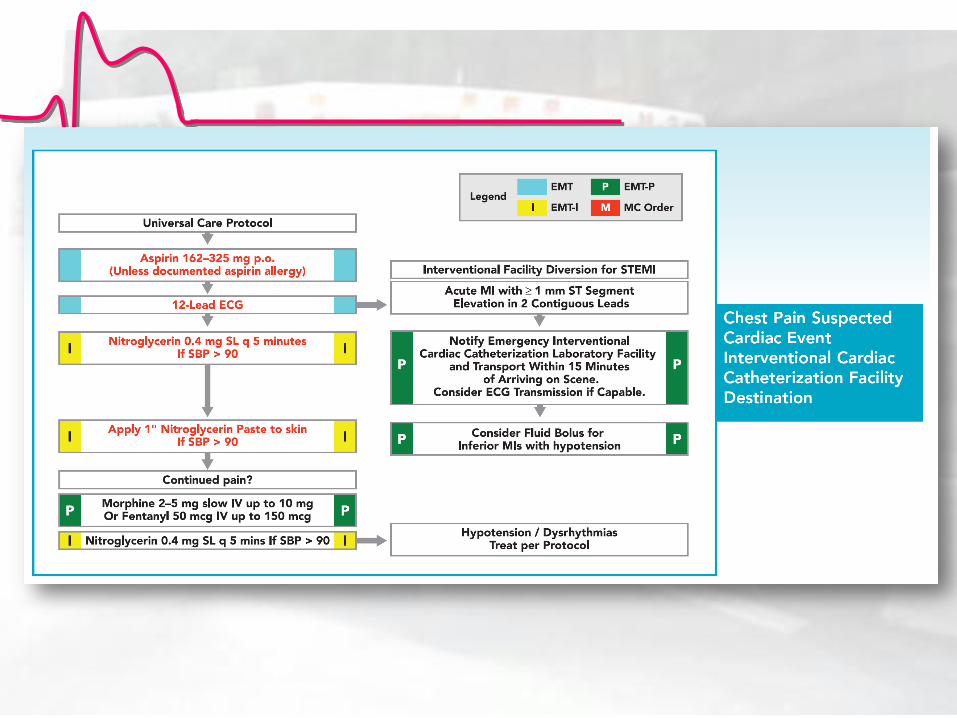
EMS lab activation protocol
• Symptoms of acute coronary syndrome
greater than 15 minutes - less than 12
hours.
• ECG diagnosis
– ST segment elevation in two contiguous
leads
or
– Machine interpretation of definite STEMI
**** acute mi****
• No contraindications to acute
catheterization
– Active severe bleeding
– Patient inappropriate for procedure
(patient or family refusal, DNR, severe
dementia)
• Trained paramedic activates Primary PCI
hospital as soon as STEMI is identified
using term “code STEMI”
• Aspirin 325 mg
Develop a regional plan
PCI Hospitals RACE Criteria
Single number cath. lab activation
Accept all STEMI patients regardless of
bed availability
30 minute lab availability 24/7
On site surgery
Ongoing QI and data feedback– AR-G
database
Partial support of a Regional Coordinator
Emergency departments
Establish a STEMI plan
Nurse first triage
10 minutes to ECG
— Typical symptoms, over age 30
— Atypical symptoms, over age 50
Emergency physician makes reperfusion
decision
Activate lab or initiate fibrinolysis
Care Processes Associated With Quicker
Door-In–Door-Out Times
Hospital processes
Dedicated STEMI reperfusion team with committed leadership
Hospital-specific reperfusion protocol
ED processes
System for obtaining ECGs within 10 min of ED arrival
Single call No. to activate PCI center cardiac catheterization lab
EMS processes
EMS has equipment to perform pre-hospital ECGs
Program for paramedics to recognize STEMI on 12-lead ECGs
Program for paramedics to recognize STEMI on 12-lead ECGs
Keep patient on local stretcher as part of AMI
Circ Cardiovasc Qual Outcomes. 2011;4:382-388.)
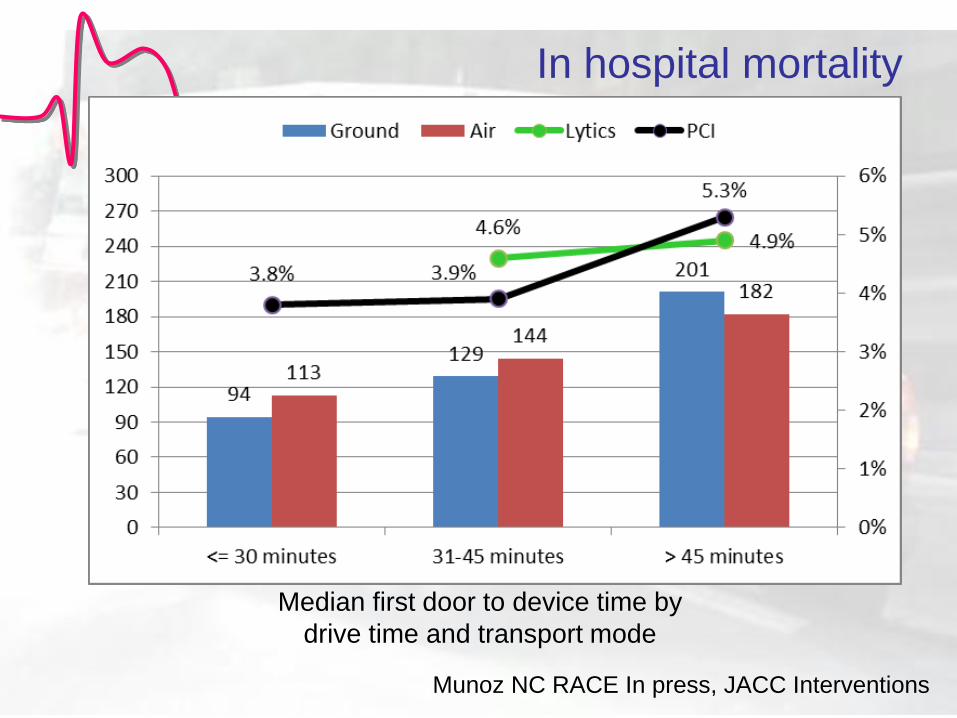
Median first door to device time by
drive time and transport mode
In hospital mortality
Munoz NC RACE In press, JACC Interventions
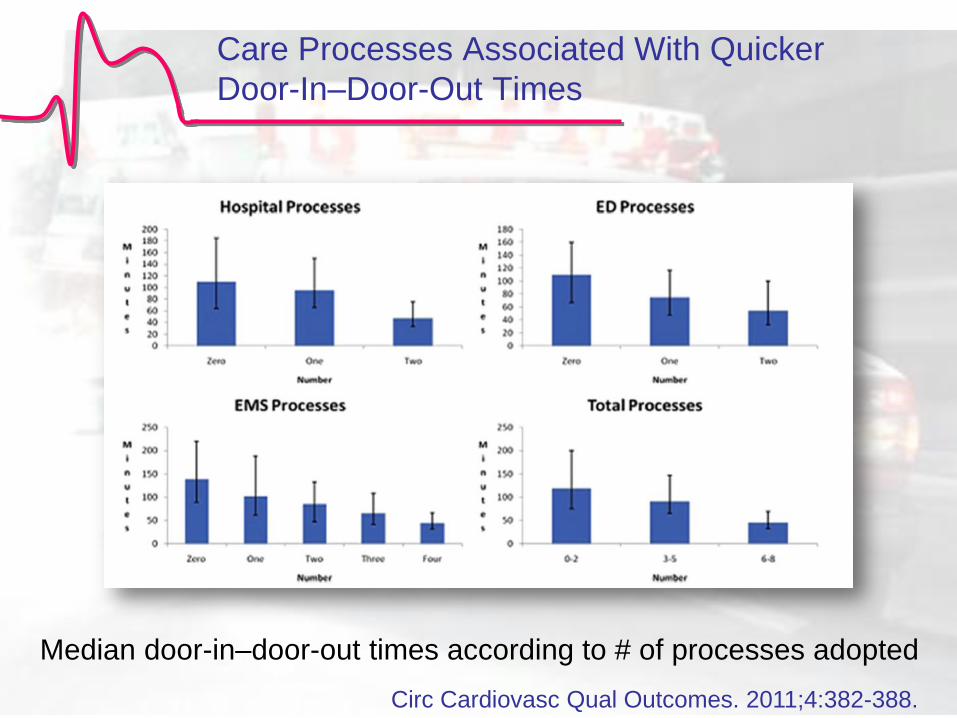
Care Processes Associated With Quicker
Door-In–Door-Out Times
Circ Cardiovasc Qual Outcomes. 2011;4:382-388.
Median door-in–door-out times according to # of processes adopted
EMS
Establish a STEMI plan
ECG for all possible STEMI patients
— Typical symptoms, over age 30
— Atypical symptoms, over age 50
Paramedic interpretation and cath. lab
activation
— Paramedic read, machine read, or
transmission.
Diversion plan to PCI hospital — Lytic ineligible
— Hospital within 30 to 40 minutes
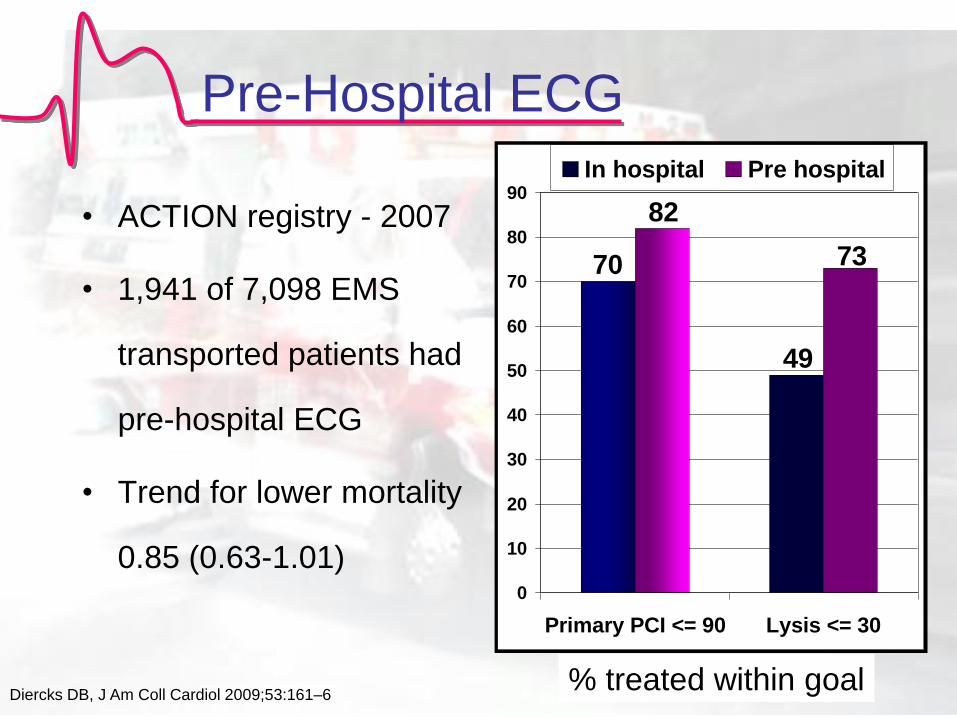
Pre-Hospital ECG
• ACTION registry - 2007
• 1,941 of 7,098 EMS
transported patients had
pre-hospital ECG
• Trend for lower mortality
0.85 (0.63-1.01)
49
70
82
73
0
10
20
30
40
50
60
70
80
90
Primary PCI <= 90 Lysis <= 30
In hospital Pre hospital
Diercks DB, J Am Coll Cardiol 2009;53:161–6 % treated within goal
4 ways to activate
1)Paramedic read
2)Machine read
3)ECG transmission
4)Walk in with ECG
EMS ECG Cath lab activation
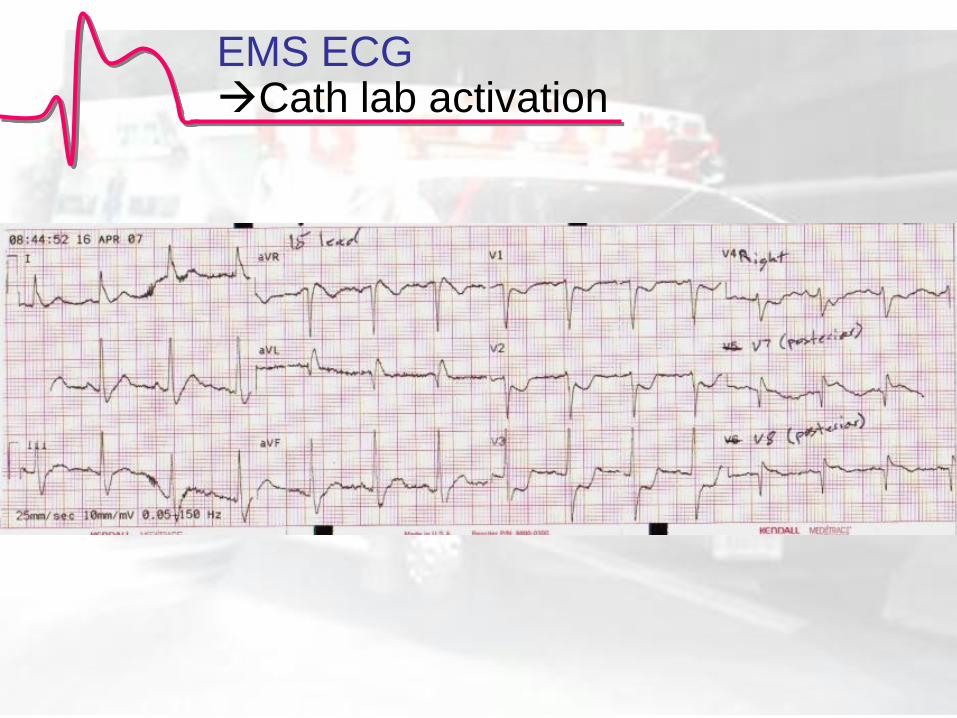
EMS ECG Cath lab activation
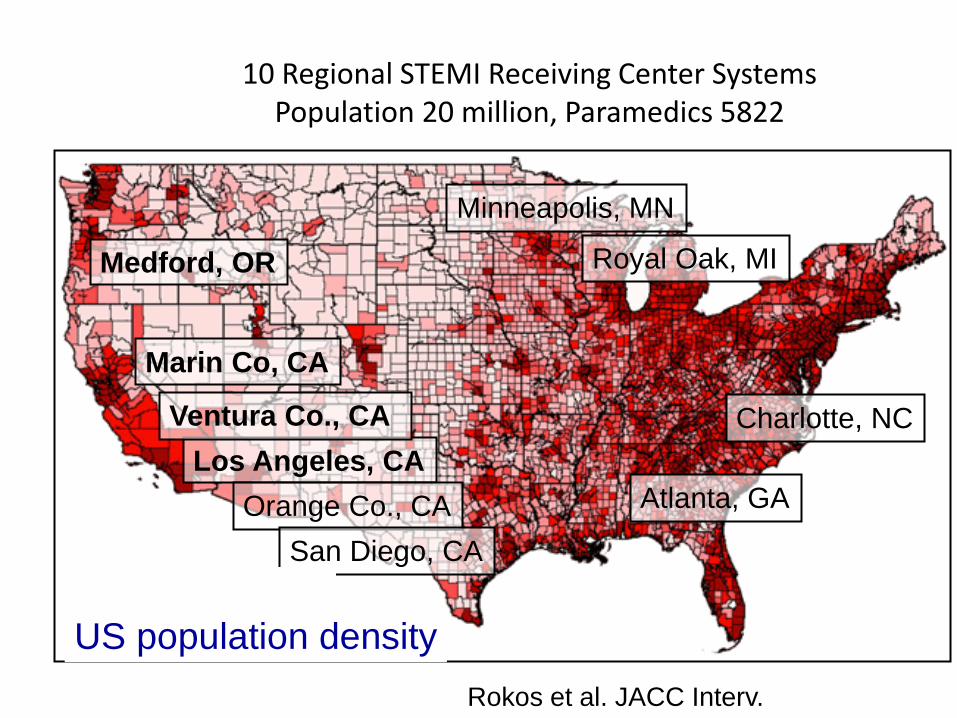
10 Regional STEMI Receiving Center Systems Population 20 million, Paramedics 5822
Royal Oak, MI
Minneapolis, MN
Medford, OR
Marin Co, CA
Los Angeles, CA
Orange Co., CA
San Diego, CA
Ventura Co., CA Charlotte, NC
Atlanta, GA
US population density
Rokos et al. JACC Interv.
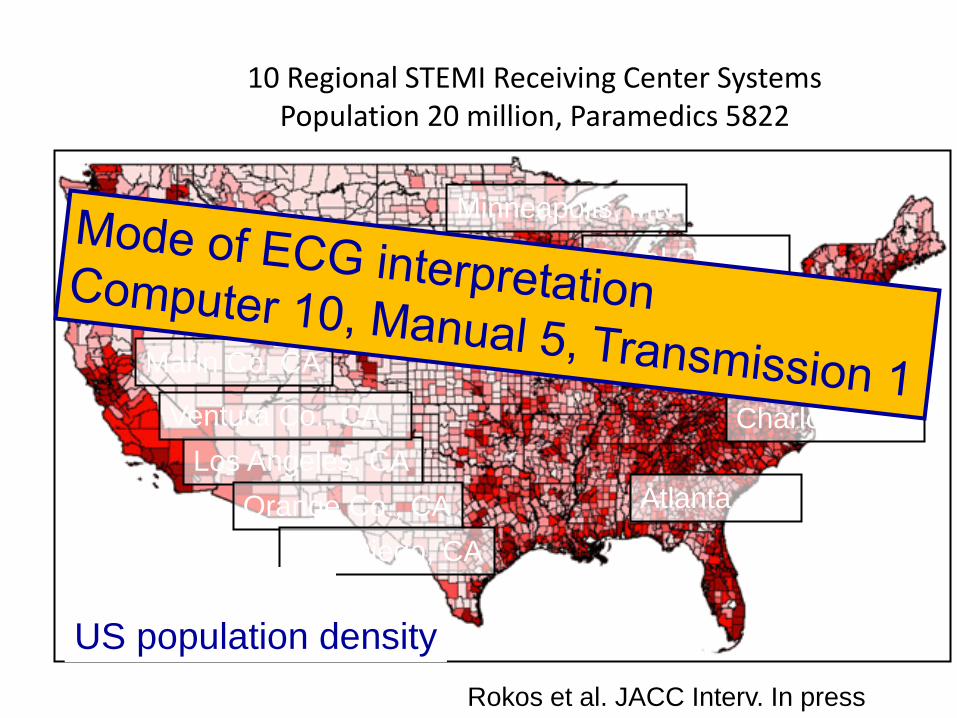
10 Regional STEMI Receiving Center Systems Population 20 million, Paramedics 5822
Royal Oak, MI
Minneapolis, MN
Medford, OR
Marin Co, CA
Los Angeles, CA
Orange Co., CA
San Diego, CA
Ventura Co., CA Charlotte, NC
Atlanta, GA
US population density
Rokos et al. JACC Interv. In press
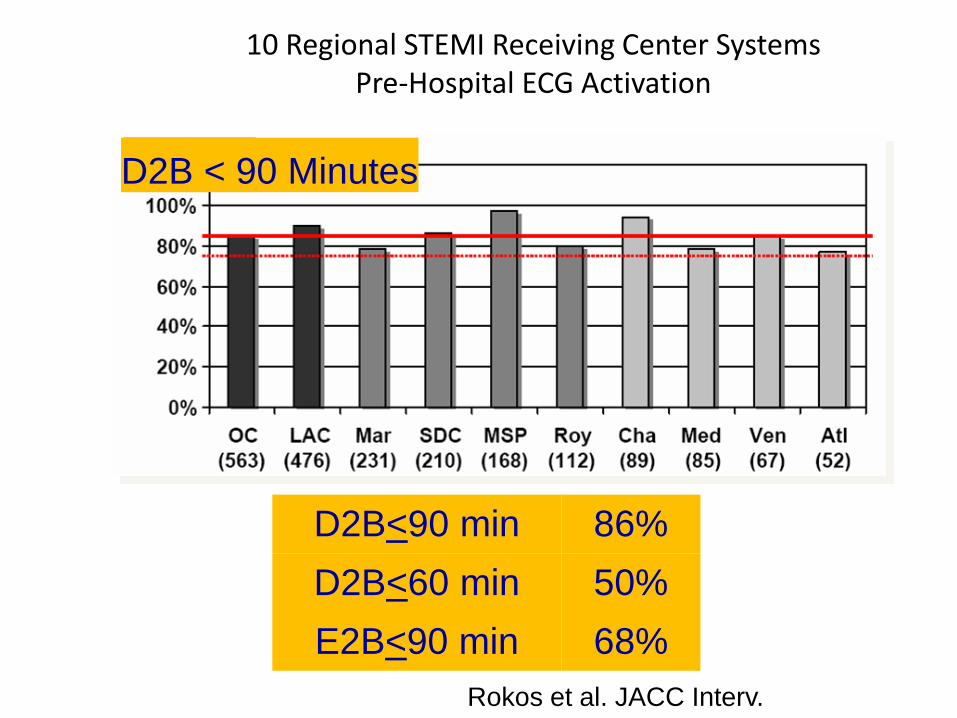
10 Regional STEMI Receiving Center Systems Pre-Hospital ECG Activation
Rokos et al. JACC Interv.
D2B < 90 Minutes
D2B<90 min 86%
D2B<60 min 50%
E2B<90 min 68%
Critical Success Factors for Regionalization
• Place patient first, not competition or $$
• Have a “neutral” party coordinate competitive regions (Key-> funding the neutral body)
• Cardiology, ED Medicine, Nursing, EMS leadership, CV Administration & QI
• Empower ED Medicine and EMS to be decision makers & activate the reperfusion plan
• Keep Reperfusion plan simple, parallel processing
• Data drives change-> both immediate and QI quarterly monitoring important
• Nurse or paramedic coordinators / Mission: Lifeline Directors essential to success
Guideline Review of Reperfusion Strategy &
other Important Statements
Primary PCI should be performed in patients
with STEMI presenting to a hospital with PCI
capability
within 90 minutes of first medical contact
as a systems goal.
PCI in Specific Clinical Situations: STEMI–
Primary PCI of the Infarct Artery
I IIa IIb III
Primary PCI should be performed in patients
with STEMI presenting to a hospital without
PCI capability
within 120 minutes of first medical contact
as a systems goal.
PCI in Specific Clinical Situations: STEMI–Primary
PCI of the Infarct Artery
I IIa IIb III
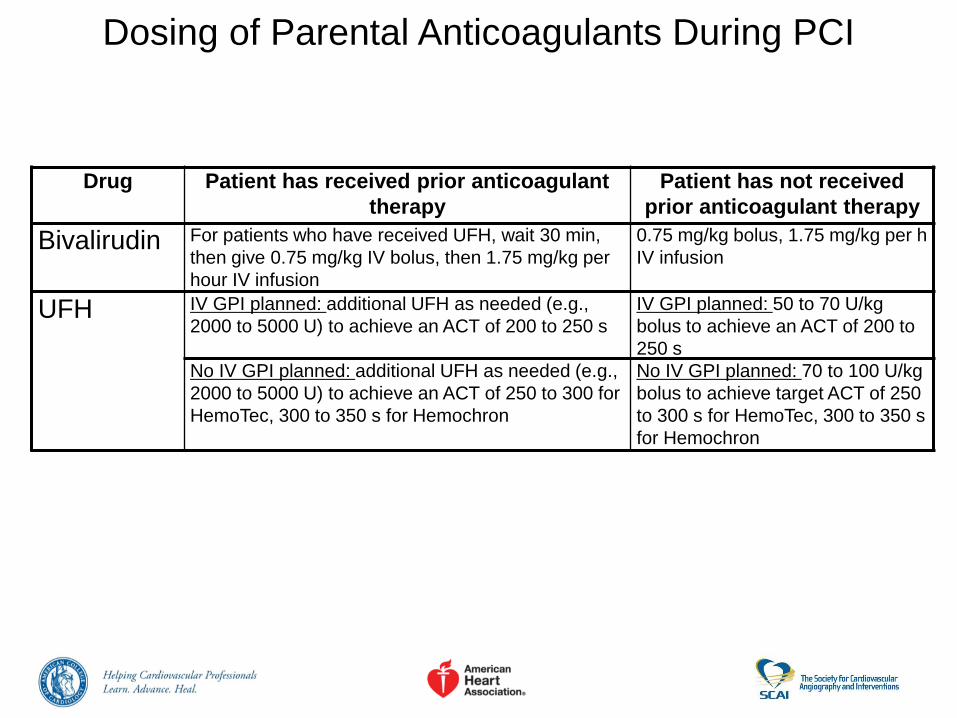
Drug Patient has received prior anticoagulant
therapy
Patient has not received
prior anticoagulant therapy
Bivalirudin For patients who have received UFH, wait 30 min,
then give 0.75 mg/kg IV bolus, then 1.75 mg/kg per
hour IV infusion
0.75 mg/kg bolus, 1.75 mg/kg per h
IV infusion
UFH IV GPI planned: additional UFH as needed (e.g.,
2000 to 5000 U) to achieve an ACT of 200 to 250 s
IV GPI planned: 50 to 70 U/kg
bolus to achieve an ACT of 200 to
250 s
No IV GPI planned: additional UFH as needed (e.g.,
2000 to 5000 U) to achieve an ACT of 250 to 300 for
HemoTec, 300 to 350 s for Hemochron
No IV GPI planned: 70 to 100 U/kg
bolus to achieve target ACT of 250
to 300 s for HemoTec, 300 to 350 s
for Hemochron
Dosing of Parental Anticoagulants During PCI
Cardiogenic Shock
Definition of shock • Decreased CO with evidence of insufficient
tissue perfusion in the presence of adequate intravascular volume
– Hemodynamic criteria : SBP < 90, PWP > 18, CI < 1.8
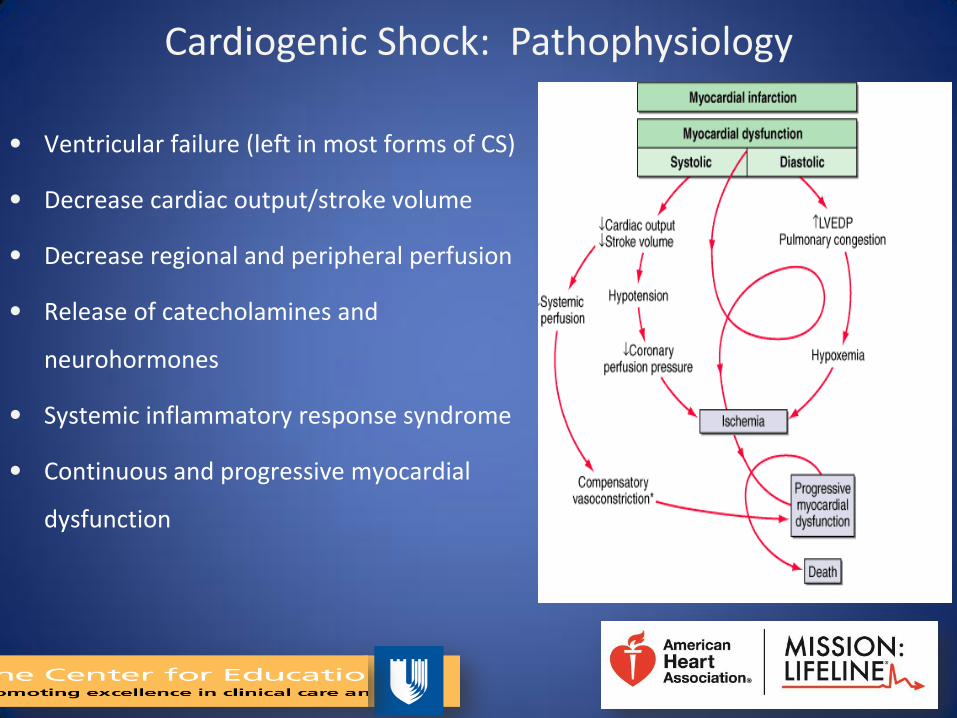
Cardiogenic Shock: Pathophysiology
• Ventricular failure (left in most forms of CS)
• Decrease cardiac output/stroke volume
• Decrease regional and peripheral perfusion
• Release of catecholamines and
neurohormones
• Systemic inflammatory response syndrome
• Continuous and progressive myocardial
dysfunction
Clinical signs
• Oliguria, cool, pale and clammy extremities, altered mental status, pulmonary congestion, tachycardia, elevated lactate, mixed venous saturation of less than 65%
• Pre shock – higher HR, lower BP among patients on
presentation among those who develop CS • STEMI
– Systolic blood pressure <= 90 on presentation
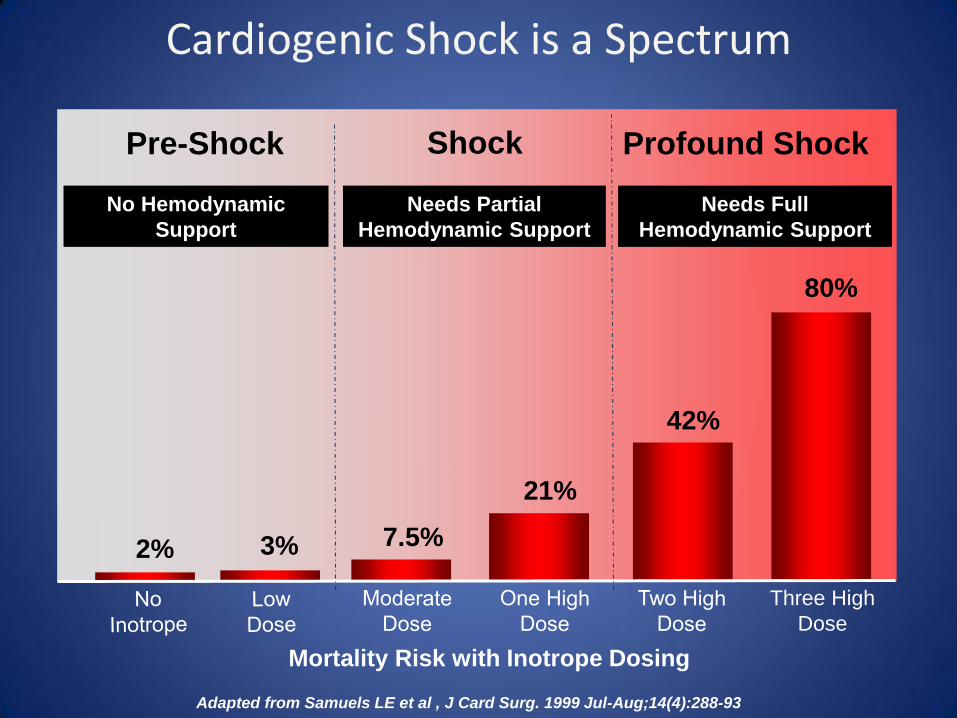
Cardiogenic Shock is a Spectrum
Three High
Dose
2% 3% 7.5%
21%
42%
80%
Pre-Shock
Profound Shock Shock
No Hemodynamic
Support
Needs Partial
Hemodynamic Support
Needs Full
Hemodynamic Support
Mortality Risk with Inotrope Dosing
Adapted from Samuels LE et al , J Card Surg. 1999 Jul-Aug;14(4):288-93
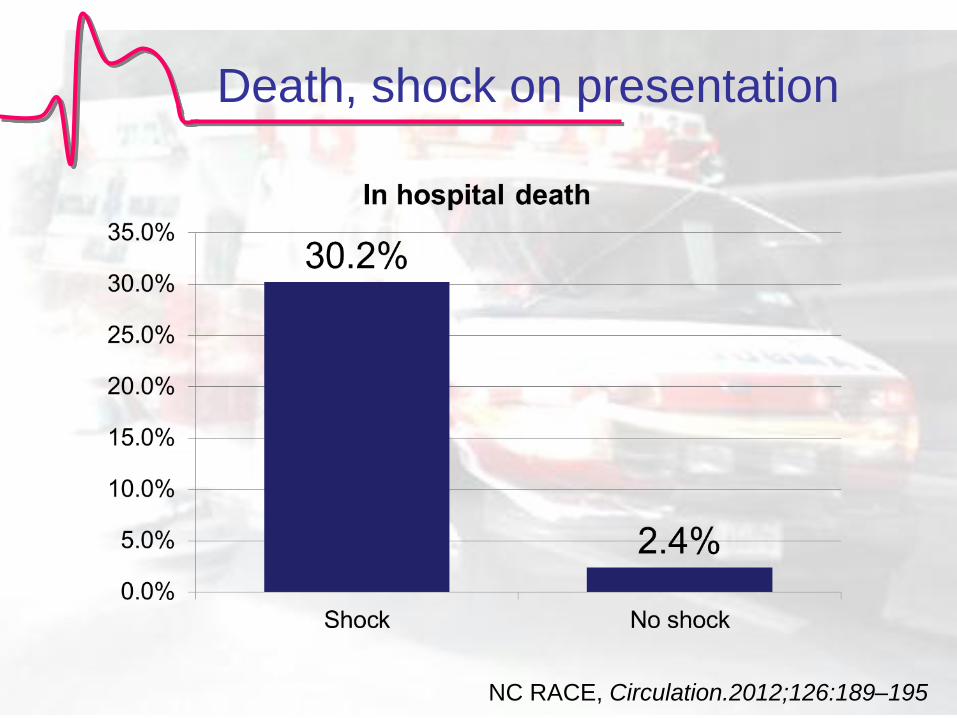
Death, shock on presentation
NC RACE, Circulation.2012;126:189–195
Cardiogenic Shock: Potential Treatment
• Revascularization: PCI / CABG
• Pressors
– Dobutamine, Nitroprusside, ….
• Mechanical support
– IABP / Impella 2.5
• Refractory shock: ventricular assist device, cardiac
transplantation
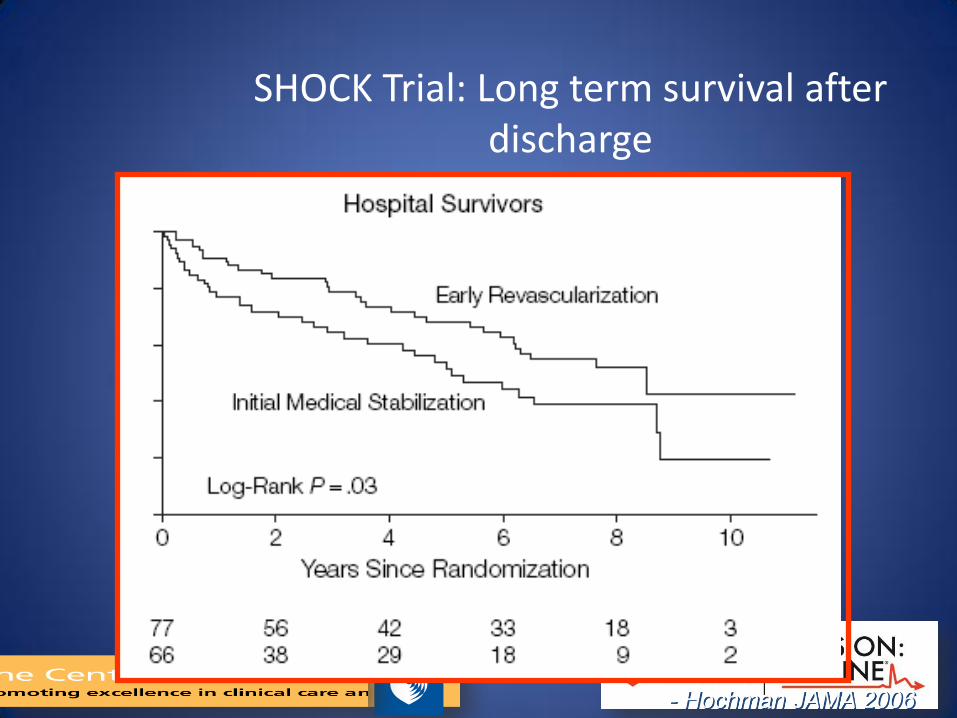
SHOCK Trial: Long term survival after discharge
- Hochman JAMA 2006
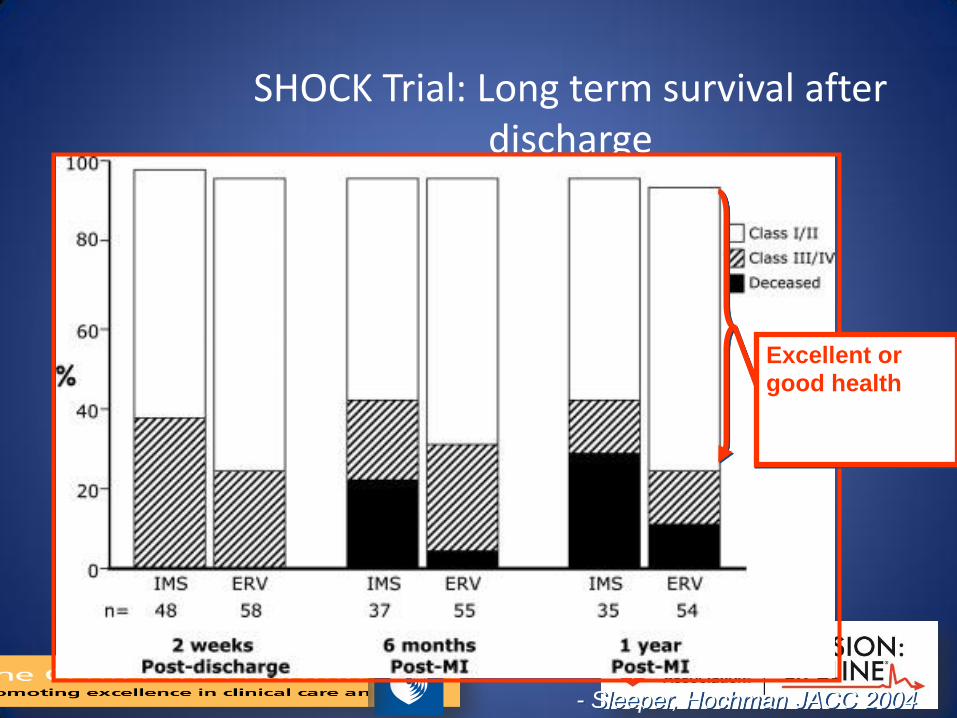
SHOCK Trial: Long term survival after discharge
Excellent or
good health
- Sleeper, Hochman JACC 2004

Most Commonly Used Mechanical Devices
IABP
TandemHeart
Impella

Current Pharmacology & Devices
Inotropes IABP ECMO Tandem-
Heart Impella
Surgical VAD
Advantages
Flow (L/min.)
Coronary Perfusion
LVEDP
<0.5
↑
↑
0.5
↑↑
↓
4
-
↑↑↑↑
3.5
-
↓↓
2.5 - 5.0
↑↑
↓↓↓
6.0
↑↑
↓↓↓↓
Limitations
Arrhythmia
Stroke
Limb ischemia
Bleeding
Cost
+++
-
N.A
N.A
$
-
++
+
++
$
-
++
+++
++++
$$$
-
+
++
+++
$$$
-
+
+
+ / ++
$$$
-
+++
N.A
++++
$$$$$

Data Solutions
Data Ongoing measurement and feedback to
entire team
Focus on benchmarks most amenable to
improvement
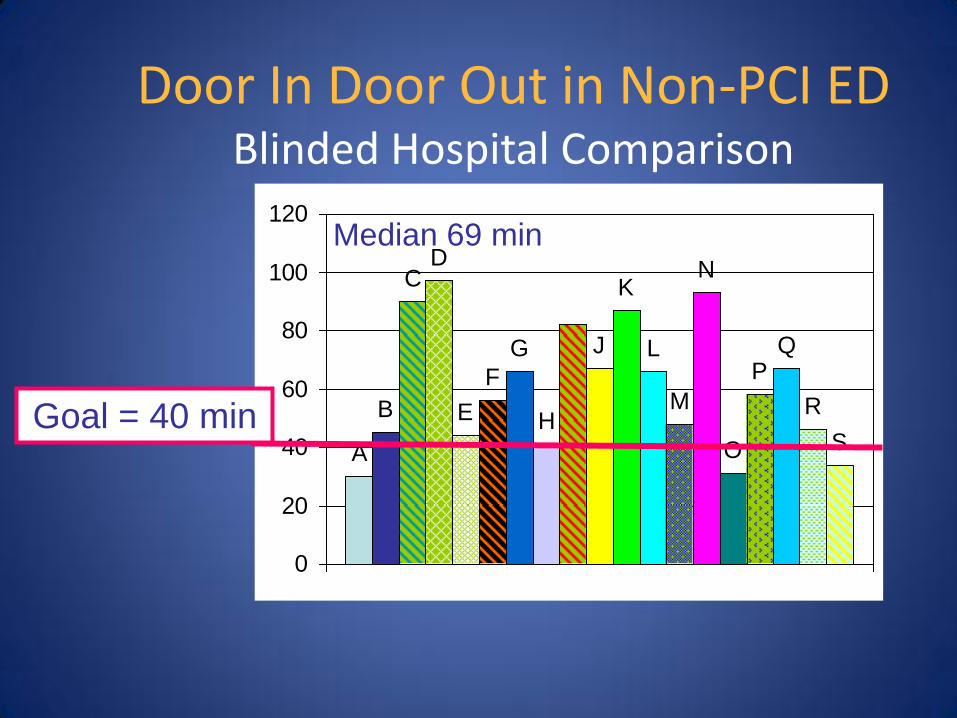
Door In Door Out in Non-PCI ED Blinded Hospital Comparison
A
B
G
H
J
K
L
N
O
Q
CD
E
FM
P
R
S
0
20
40
60
80
100
120
Goal = 40 min
Median 69 min
Data Participation in Regional Reports / System
Requirements
1. Regional PCI hospitals enroll in
NCDR ACTION-GWTG Registry
2. PCI hospitals sign up with
Mission: Lifeline
3. PCI hospitals complete
• ML System DCRF
• Accelerator Project DCRF
Regional Systems of Care Demonstration Project:
Mission: Lifeline STEMI Accelerator
National Program Sponsors Through Educational Grants
THE MEDICINES COMPANY
Philips Healthcare
ABIOMED, Inc.
Objectives • Establish a regional standard of emergency
cardiovascular care that includes every hospital and EMS agency.
• Lower cardiovascular mortality by broadly improving the timely treatment of ST elevation myocardial infarction (STEMI) patients.
• Create a sustainable system for treating cardiovascular emergencies including STEMI, cardiac arrest, stroke and aortic dissection.
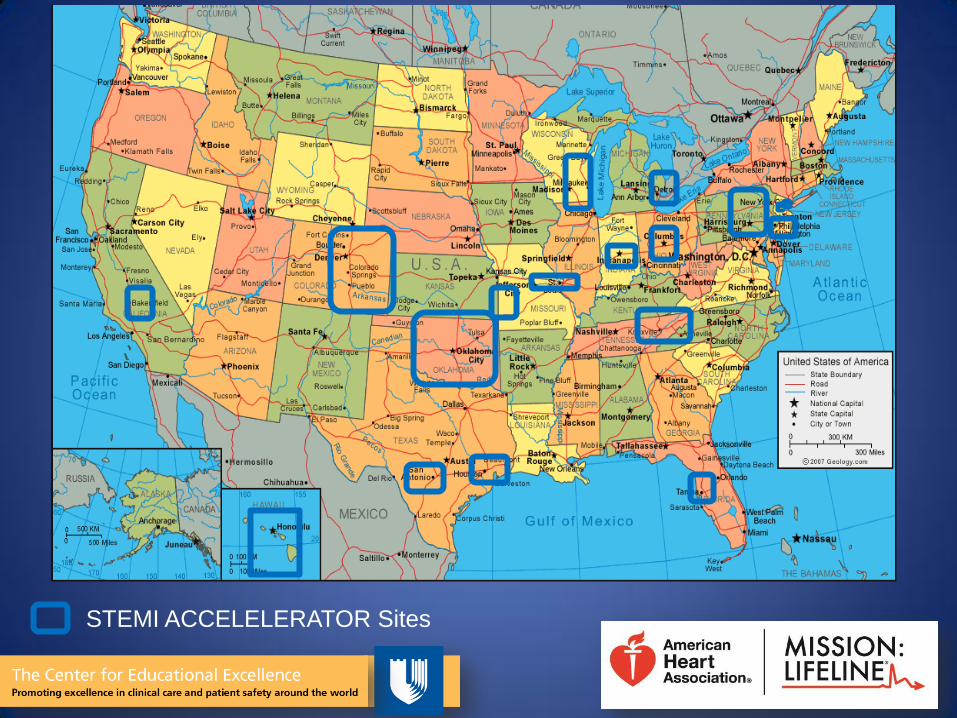
STEMI ACCELELERATOR Sites
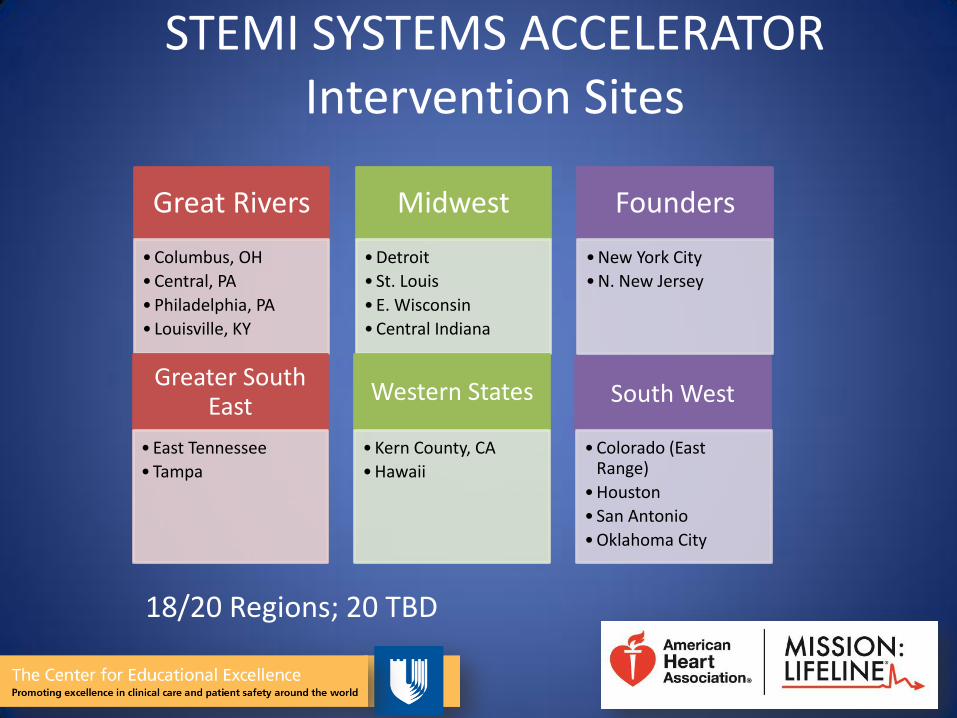
STEMI SYSTEMS ACCELERATOR Intervention Sites
Great Rivers
• Columbus, OH
• Central, PA
• Philadelphia, PA
• Louisville, KY
Midwest
• Detroit
• St. Louis
• E. Wisconsin
• Central Indiana
Founders
• New York City
• N. New Jersey
Greater South East
• East Tennessee
• Tampa
Western States
• Kern County, CA
• Hawaii
South West
• Colorado (East Range)
• Houston
• San Antonio
• Oklahoma City
18/20 Regions; 20 TBD
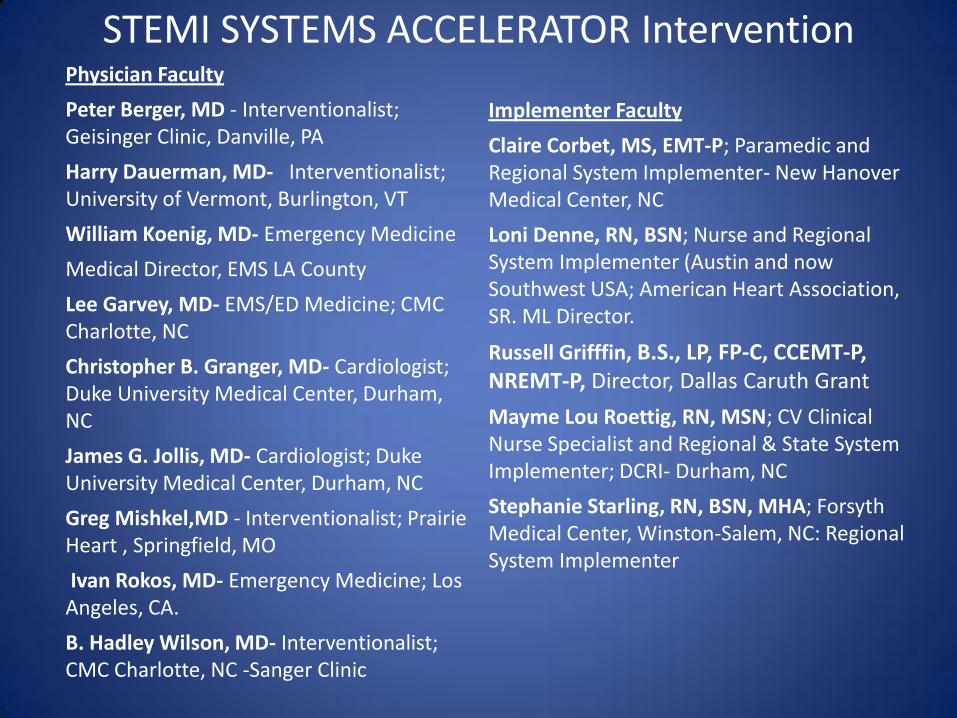
STEMI SYSTEMS ACCELERATOR Intervention Physician Faculty
Peter Berger, MD - Interventionalist; Geisinger Clinic, Danville, PA
Harry Dauerman, MD- Interventionalist; University of Vermont, Burlington, VT
William Koenig, MD- Emergency Medicine
Medical Director, EMS LA County
Lee Garvey, MD- EMS/ED Medicine; CMC Charlotte, NC
Christopher B. Granger, MD- Cardiologist; Duke University Medical Center, Durham, NC
James G. Jollis, MD- Cardiologist; Duke University Medical Center, Durham, NC
Greg Mishkel,MD - Interventionalist; Prairie Heart , Springfield, MO
Ivan Rokos, MD- Emergency Medicine; Los Angeles, CA.
B. Hadley Wilson, MD- Interventionalist; CMC Charlotte, NC -Sanger Clinic
Implementer Faculty
Claire Corbet, MS, EMT-P; Paramedic and Regional System Implementer- New Hanover Medical Center, NC
Loni Denne, RN, BSN; Nurse and Regional System Implementer (Austin and now Southwest USA; American Heart Association, SR. ML Director.
Russell Grifffin, B.S., LP, FP-C, CCEMT-P, NREMT-P, Director, Dallas Caruth Grant
Mayme Lou Roettig, RN, MSN; CV Clinical Nurse Specialist and Regional & State System Implementer; DCRI- Durham, NC
Stephanie Starling, RN, BSN, MHA; Forsyth Medical Center, Winston-Salem, NC: Regional System Implementer
• Using national level system faculty and local AHA staff to broker competitive entities to regionalize STEMI care for a community.
• Success based on regional local leadership owning the program.
• Unbiased staff to recruit all hospitals to join centralized database.
• Regional Intervention Day – CME/CNE event
• Data- Baseline, Quarterly for 1 year, Post Intervention • Quarterly meetings to share best practices, data review
across the region and identify strategies to improve process
STEMI SYSTEMS ACCELERATOR Intervention
• Voluntary.
• Intervention does not change referral lines.
• Augments existing systems / leaves regional leadership entirely in charge of system.
STEMI SYSTEMS ACCELERATOR Intervention
STEMI SYSTEMS ACCELERATOR Intervention
Data All primary PCI hospitals in the Accelerator Region
> enroll in AR-G (minimal requirement- STEMI only for duration of the project timeline)
> Agree to “systems release” ₋ Hospitals ID’s are blinded
₋ Data may be aggregated (combined) for regional report (M:L Systems Report) and with 19 additional regions in the program.
System data consent release form (DCRF) must be signed and returned to AHA for assignment of a system ID #
Timelines: > July 2012 – enroll and complete release forms > Baseline regional Data July 1, 2012 discharges through
September 31st, 2012 > Quarterly Data through December 31, 2013
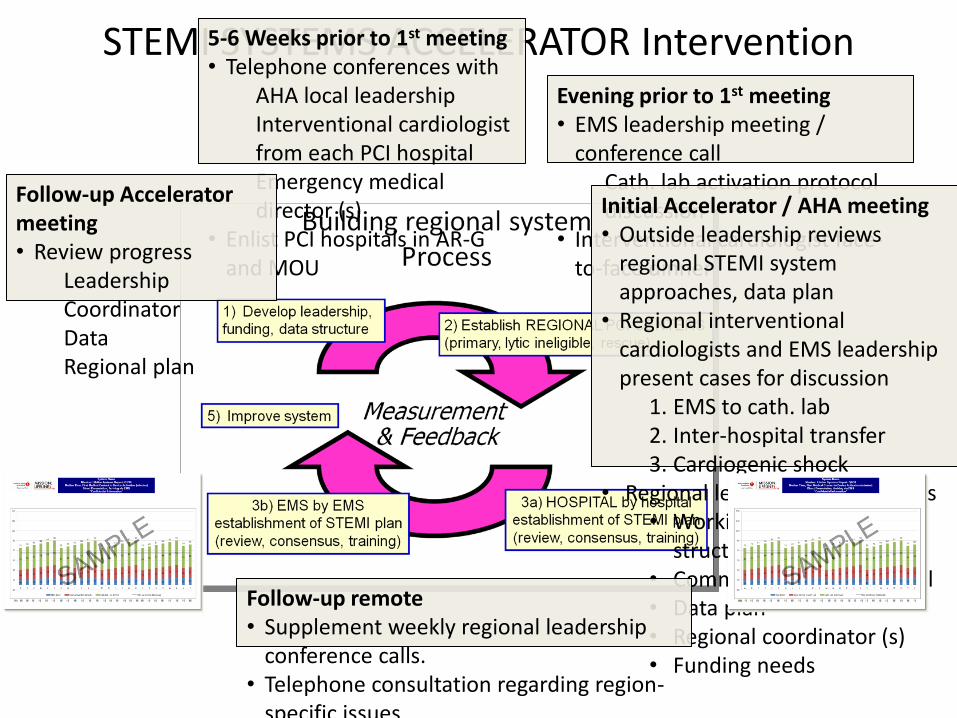
STEMI SYSTEMS ACCELERATOR Intervention 5-6 Weeks prior to 1st meeting • Telephone conferences with
AHA local leadership Interventional cardiologist from each PCI hospital Emergency medical director (s)
• Enlist PCI hospitals in AR-G and MOU
Evening prior to 1st meeting • EMS leadership meeting /
conference call Cath. lab activation protocol discussion
• Interventional cardiologist face-to-face dinner
Initial Accelerator / AHA meeting • Outside leadership reviews
regional STEMI system approaches, data plan
• Regional interventional cardiologists and EMS leadership present cases for discussion
1. EMS to cath. lab 2. Inter-hospital transfer 3. Cardiogenic shock
• Regional leaders plan next steps • Working leadership
structure • Common regional protocol • Data plan • Regional coordinator (s) • Funding needs
Follow-up remote • Supplement weekly regional leadership
conference calls. • Telephone consultation regarding region-
specific issues
Follow-up Accelerator meeting • Review progress
Leadership Coordinator Data Regional plan
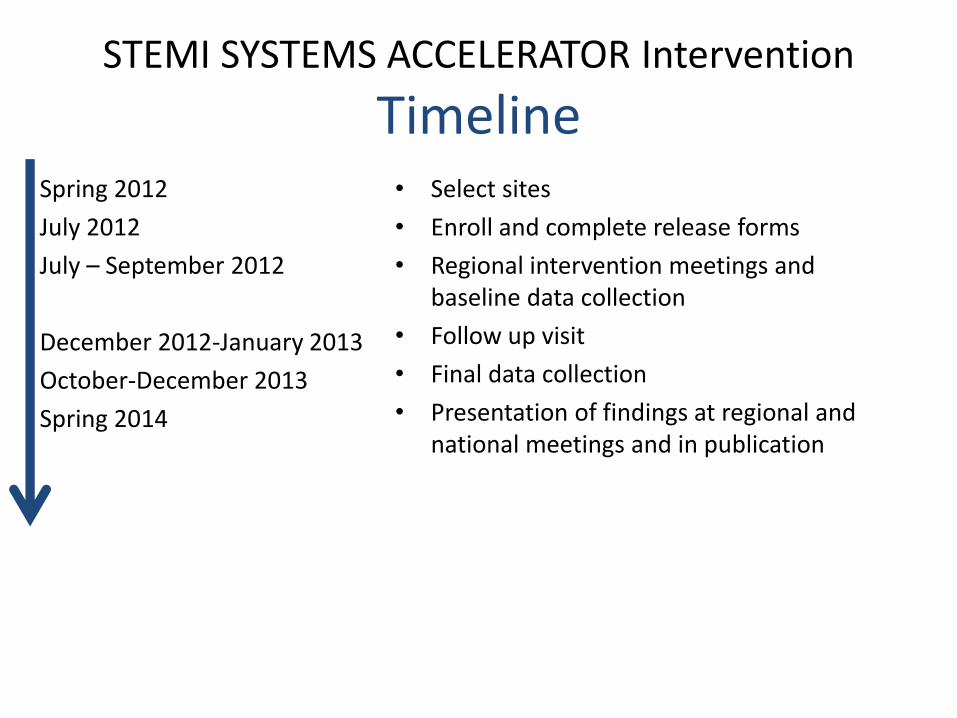
STEMI SYSTEMS ACCELERATOR Intervention
Timeline Spring 2012
July 2012
July – September 2012
December 2012-January 2013
October-December 2013
Spring 2014
• Select sites
• Enroll and complete release forms
• Regional intervention meetings and baseline data collection
• Follow up visit
• Final data collection
• Presentation of findings at regional and national meetings and in publication




























