Embed Size (px)
Citation preview
AETIOLOGY: PART 1
Mike Akroyd, 9th May 2014
Aims
Illustrate how aetiology fits into MRCPsych: Paper 1 and beyond
Explore aetiological factors of general adult psychiatric illness (Old age and child in part 2, in 2 weeks)

Objectives
“By the end of this session I will be able to...” Describe basic aetiological concepts Apply aetiological factors to the
biopsychosocial model Identify aetiological factors involved in
general adult psychiatric disorder Answer some exam questions on the above
Why aetiology?
We want to understand causes of mental disorder Identification of at-risk individuals Suggestion of management approaches Possibility of preventive interventions Patients (or parents...) want to know “am I
to blame?”
...and it accounts for c.12/200 questions in Paper 1...
Aetiological theory
Two broad categories of explanatory model Reductionist
Understand causation by tracing back to simpler stages
E.g. schizophrenia caused by faulty neurotransmission in specific part of brain
(narrow) medical models Non-reductionist
Problems relate to wider issues E.g. schizophrenia caused by patient’s family Sociological models
Aetiological factors
Genetic Psychological Psychodynamic Social Political Environmental Behavioural Developmental

Biopsychosocial formulation
Bio Psycho Social
Predisposing Genetics IQPersonality
FamilySocial class
Marital status
Precipitating IllnessDrugs
Traumatic event
UnemploymentDivorce
Perpetuating Chronic illness WithdrawalHopelessness
Ongoing unemployment
Basic aetiological terms
Heritability “Proportion of liability to a disorder in a
population that is accounted for by genetic effects”
How much of the aetiology is likely to be accounted for by genetics? (As opposed to environment) Expressed in percentage term Applied to population, not individual Derived from difference in concordance
between MZ and DZ twins
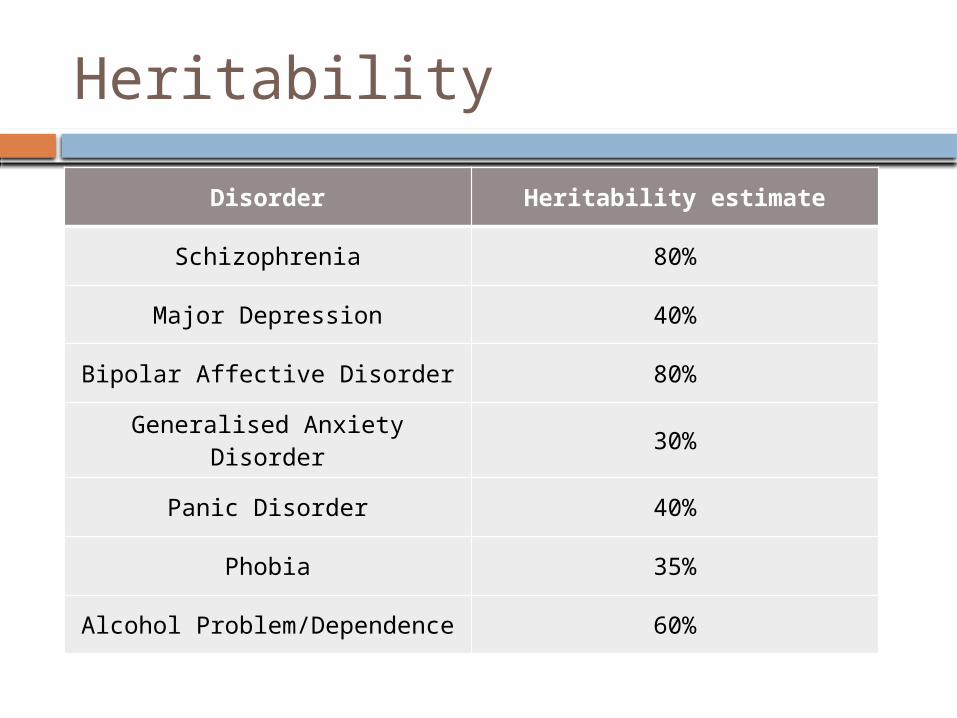
Heritability
Disorder Heritability estimate
Schizophrenia 80%
Major Depression 40%
Bipolar Affective Disorder 80%
Generalised Anxiety Disorder 30%
Panic Disorder 40%
Phobia 35%
Alcohol Problem/Dependence 60%

Basic aetiological terms
Not everything that runs in families is genetic... Religion, Football team
Equally, not everything passed on shows itself Concept of penetrance
Likelihood that having a particular genotype results in manifestation of associated characteristic.
Relatively few conditions fully penetrant.

Basic statistical concepts
Lifetime prevalence Risk Relative risk
Lifetime prevalence
What proportion of people will develop a given illness in their lifetime? Lifetime prevalence of schizophrenia = 1% 1 in 100 will develop schizophrenia in their
lifetime

Risk
Risk = Chance = Probability Probability that a given event will occur
In a given timeframe What is the probability that a person will
develop schizophrenia across their lifetime? 1/100 develop schizophrenia Risk = 0.01
Relative risk
Ratio of risk in a group exposed to a certain risk, compared to a group not exposed. i.e. Risk in exposed group Risk in unexposed group
If relative risk =1, no difference between groups
If relative risk >1, exposed group more likely to develop disorder
If relative risk <1, exposed group less likely
Relative risk
Cannabis use and schizophrenia Lifetime prevalence (risk) of
schizophrenia = 1/100 Risk in cannabis users = 5/200 Relative risk of schizophrenia in cannabis
users?
5/200 = 5/200 = 5 = 2.5 1/100 2/200 2

General Adult Aetiology
Schizophrenia Bipolar affective disorder Depression Anxiety disorders Dependency
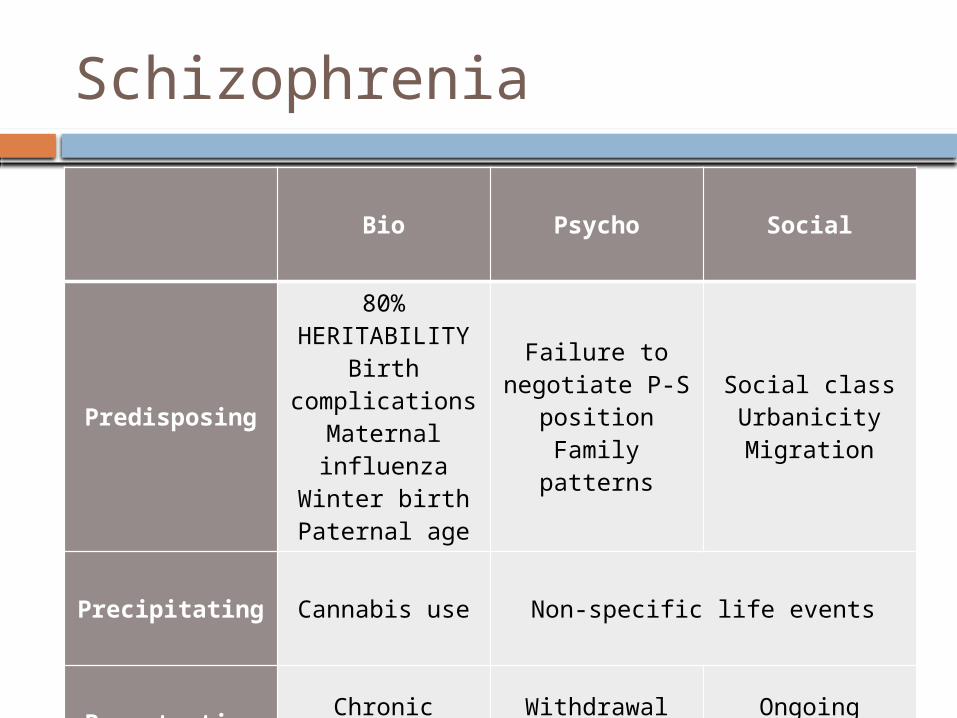
Schizophrenia
Bio Psycho Social
Predisposing
80% HERITABILITY
Birth complications
Maternal influenza
Winter birthPaternal age
Failure to negotiate P-S
positionFamily patterns
Social classUrbanicityMigration
Precipitating Cannabis use Non-specific life events
Perpetuating Chronic illness WithdrawalHopelessness
Ongoing unemployment
Schizophrenia – Genetics
80% heritability Complex genetic disorder Or group of disorders
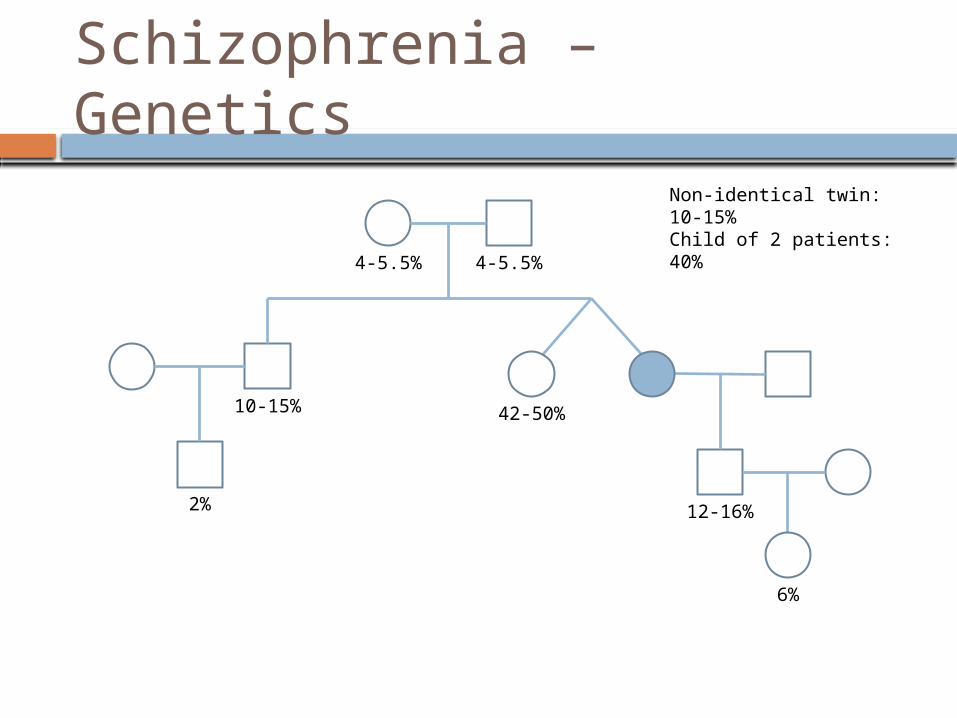
Schizophrenia – Genetics
12-16%
42-50%10-15%
2%
4-5.5% 4-5.5%
Non-identical twin: 10-15%Child of 2 patients: 40%
6%
Schizophrenia – Genetics
Susceptibility genes Neuregulin (NRG1) – strong evidence Dysbindin (DTNBP) – strong evidence D-Amino acid oxidase activator (G72) Regulator of G-protein signalling-4 (RGS-4) Disrupted in schizophrenia (DISc-1) Metabotropic glutamate receptor 3 (GRM3) Catechol-O-methyl transferase (COMT) (also
implicated in velocardiofacial syndrome) D-aminoacid oxidase (DAAO) 5-HT2A receptor (HTR2A) Dopamine D3 receptor (DRD3)

Schizophrenia – Genetics
1st degree relatives of patients with schizophrenia Risk of schizophrenia Risk of schizoaffective disorder Risk of schizotypal personality disorder
1st degree relatives of patients with schizoaffective Risk of schizophrenia
Schizophrenia – Social
Lower social class Competing hypotheses
Low predisposing IQ, hardship? Social drift in prodrome/illness?
Urbanicity Migration
Higher risk in migrants Particularly 2nd generation
UK migrants from Afro-Caribbean higher risk than indigenous UK population or non-migrating Afro-Caribbean
Schizophrenia – Environmental Obstetric complications
Reported in retrospective studies Not consistently replicated in prospective studies
Maternal influenza 2nd trimester influenza exposure
Mixed evidence Winter birth
Effect shown in N+S hemispheres Cannabis use
Andreasson’s Swedish military conscripts Dose-dependent relationship
Paternal age Some evidence

Schizophrenia – Organic
Metachromatic leucodystrophy 35% develop schizophrenia
Velocardiofacial syndrome (aka Di George) Schizophreniform and affective psychosis in
30% Huntington’s disease
Associated with schizophreniform/affective psychosis
Increased risk in epilepsy (birth of ECT...)

Schizophrenia – Neurological Developmental
Distinguishable from peers at c.11 Hostility toward adults Language delays Poor rapport Isolation from peers
Low IQ Prevalence of schizophrenia in LD = 3%
Schizophrenia – Psychological Psychodynamic
Freud – Narcissism Klein – Failure to negotiate paranoid-
schizoid position

Schizophrenia – Psychological Family
Fromm-Reichmann - Deviant role relationships (“schizophrenogenic mother”)
Lidz – Abnormal family patterns “Marital skew” – one parent yields to other’s
eccentricity “Marital schism” – contrary views, divided loyalties
Bateson & Wynee – Disordered communication “Double bind” – instruction contradicted by covert
instruction Not routinely used
Scarce data, induction of guilt

Schizophrenia – Precipitants
Non-specific life events precede first onset & relapses
Increased rate in preceding 3 weeks

Schizophrenia – Relative risks
Factor Relative risk
Cannabis use (heavy) 6
Epilepsy 2.4 (or 9...)
Migrants 2.7
In 6 months post ‘Life Event’ 2
Winter birth 1.1
Urban birth 2.4
Cannabis use (overall) 2.5
Maternal influenza (Up to 7...)

Schizophrenia – Aetiological theory Neurodevelopmental
Leading hypothesis Structural brain abnormalities precede symptom onset Cognitive/social impairment in childhood “Soft” neurological signs Perinatal risk factors
Abberant connectivity Inadequate integration of brain regions
Stress-diathesis model Vulnerability from early factors Later stressors trigger onset, determine course
BPAD
Lifetime prevalence = c.1% Heritability = 80-85% First degree relatives:
Risk of BPAD (7-10% vs 1%) Risk of unipolar depression (20-30% vs
10-20%) Risk of schizoaffective disorder
And risk of BPAD if first degree relative has: Unipolar depression (2%) (some dispute) Schizoaffective disorder (4.8%)

BPAD
Genetics Tyrosine hydroxylase; COMT; 5HT
transporter; BDNF Social
Higher socioeconomic class; divorced/single Psychological
Cyclothymic personality predisposes Precipitating factors
Life events “Kindling effect”

Depression
Lifetime prevalence = c.10-20% Heritability estimates vary (40-75%)
Lower MZ concordance First degree relatives:
Risk of unipolar depression (20-30%) Risk of BPAD 2%? 1%?

Depression
Genetics 5HT transporter gene
Social Risk in unemployed, divorced, separated Risk if poor social support, isolation Brown & Harris – 3 factors in women
Not working outside the home Lack of confiding relationship 3+ children under 14
Depression
Environmental Loss of parent before 11 Family discord, separation, divorce Childhood sexual abuse
Organic Risk in HIV, MS, endocrine disorders Iatrogenic: L-Dopa, methyldopa, ß-blockers,
steroids Precipitating factors
Kindling
Depression – Psychological
Relationship with parents Non-caring/overprotective Attachment problems (e.g. maternal
depression) Personality
High need for approval Neuroticism (Eysenck)
Beck’s cognitive triad 1. Self: negative self-perception 2. World: hostile, demanding 3. Future: expectation of suffering, failure
Depression – Psychological
Freud, Abraham Disturbance of oral phase predisposes Real/imagined loss of an object
Object introjected (defence) Invokes love and hate Anger toward lost object directed inwards
Seligman Learned helplessness
Suicide
UK suicide rate c.1/10,000 Men (17/100,000) > Women (5/100,000)
Genetics Positive family history increases risk
Organic Associated with: Epilepsy; MS; AIDS;
Huntington’s Low 5-HIAA in CSF of completed suicide
Presynaptic marker of 5HT function
Suicide – Social
Risk in: Males, unemployed, Caucasian, migrants Low social class, professionals, fall in status
Risk in: Married, with children Wartime
Durkheim: 4 types of suicide Egoistic – Not integrated Altruistic – Excessive integration Anomic – Disrupted integration Fatalistic – Escape from oppression

Suicide
50%
17%
8%
8%
3%
14%
Mental heath diagnoses associated with suicide
AffectiveSchizophreniformPersonality disorderAlcohol dependenceDrug dependenceOther

Anxiety disorders
OCD Prevalence = c.2-3%; 35% in 1st degree Risk in single 35% premorbidly anankastic Freud: Regression to anal phase
PTSD Women > Men Risk in single/divorced/widowed; withdrawn, low SE Risk in alcohol misuse, previous childhood trauma Precipitated by
Interpersonal violence (assault, rape, combat) External locus of control (natural disaster)
Anxiety disorders
Phobias 31% of 1st degree relatives will have a
phobia ‘Prepared learning’ – some evolutionary
benefit E.g. snakes
Conditioning Development of phobia following stressor
Panic disorder Heritability = c.30-40% 1st degree relatives c.3x more likely

Alcohol
Alcohol dependence Heritability = c.60%
Biological sons adopted away retain risk Social learning theory Comorbid psychiatric disorder is common Rate of dependence mirrors rate of
consumption
Drugs
4 factors contribute to drug use 1. Availability of drugs 2. Vulnerable personality
School record, truancy, thrill-seekers, impulsivity
3. Social environment Condoned use, unemployment, homelessness
4. Pharmacological factors Not every user becomes an abuser Risk if create positive feeling or alleviate
stress
Which of the following theories suggests that schizophrenia occurs when individuals who are vulnerable to the disease undergo a life stress which precipitates the initial episode ?
a. Kindling effect
b. Abberant connectivity
c. Neurodevelopmental hypothesis
d. Stress-diathesis model
e. Social model

A mother wants to know what is the risk of schizophrenia in her son who smokes cannabis?
a. Four-fold increase in risk
b. Two-fold increase in risk
c. Four-fold decrease in risk
d. Two-fold decrease in risk
e. No association between cannabis and schizophrenia
Which of the following does not increase the risk of developing bipolar disorder?
a. Family history of depression
b. Family history of schizoaffective disorder
c. Family history of schizophrenia
d. Cyclothymic personality
e. Family history of bipolar disorder
Which of the following is not a vulnerability factor for depression as described by Brown and Harris?
a. Lack of confiding relationship
b. Loss of parent before age of 11
c. Not working outside the home
d. Having 3 or more children under the age of 14
e. None of the above

A person who feels like he has lost his place is society due to being made redundant goes on to commit suicide. According to Emile Durkheim what type of suicide would that be?
a. Anomic
b. Altruistic
c. Egoistic
d. Fatalistic
e. Holistic
Which of the following risk factor is likely to be causative in a young man diagnosed with schizophrenia?
a. Alcoholism
b. HLADR2 gene
c. Being a migrant
d. Having lost his mother before the age of 14
e. Living alone