Embed Size (px)
Citation preview

Adapted from:
Treatment of Schizophrenia (and Related Psychotic Disorders)
Scott Stroup, MD, MPH
2004

Psychosis
• Generally equated with positive symptoms and disorganized or bizarre speech/behavior
• Impaired “reality testing”• A syndrome present in many illnesses
– remove known cause or treat underlying illness
– treat symptomatically with antipsychotic medications

Schizophrenia is a heterogeneous illness
• Defined by a constellation of symptoms, including psychosis
• Multifactorial etiology, variable course• Social/occupational dysfunction a
required diagnostic criterion• Good treatment must address
symptoms and social/occupational dysfunction

DSM-IV Schizophrenia• 2 or more of the following for most of 1 month:
– Delusions– Hallucinations– Disorganized speech– Grossly disorganized or catatonic behavior– Negative symptoms
• Social/occupational dysfunction• Duration of at least 6 months• Not schizoaffective disorder or a mood disorder
with psychotic features• Not due to substance abuse or a general
medical disorder

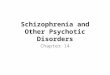
Features of SchizophreniaPositive symptomsDelusionsHallucinations
Cognitive deficitsAttentionMemoryVerbal fluencyExecutive function (eg, abstraction)
Functional ImpairmentsWork/school
Interpersonal relationshipsSelf-care
Negative symptomsAnhedoniaAffective flatteningAvolitionSocial withdrawalAlogia
Mood symptomsDepression/AnxietyAggression/HostilitySuicidality
DisorganizationSpeech
Behavior

Common needs of people with schizophrenia
• Symptom control• Housing • Income• Work• Social skills• Treatment of comorbid conditions

Challenges in the Treatment of Schizophrenia
• Stigma• Impaired “insight”– no agreement on problem• Treatment “compliance”• Substance abuse very common• Violence risk• Suicide risk• Medical problems common, often
unrecognized

Schizophrenia Treatment
• Therapeutic Goals• minimize symptoms• minimize medication side effects• prevent relapse• maximize function• “recovery”
• Types of Treatment• pharmacotherapy• psychosocial/psychotherapeutic

Treatments for schizophrenia:Strong evidence for effectiveness
• Antipsychotic medications• Family psychoeducation• Assertive Community Treatment
(ACT teams)

The First Modern AntipsychoticChlorpromazine (Thorazine)
• Antipsychotic properties discovered in 1952
• Studied originally for usefulness as a sedative
• Found to be useful in controlling agitation in patients with schizophrenia
• Introduced in U.S. in 1953

Show Video Tape
Augustine

The Dopamine Hypothesis of Schizophrenia
• All conventional antipsychotics block the dopamine D2 receptor
• Dopamine enhancing drugs can induce psychosis (e.g., chronic amphetamine use)

“Typical” antipsychotic medications(aka first-generation, conventional, neuroleptics, major tranquilizers)
• High Potency (2-20 mg/day)(haloperidol, fluphenazine)
• Mid Potency (10-100 mg/day)(loxapine, perphenazine)
• Low Potency (300-800+ mg/day)(chlorpromazine, thioridizine)

Dopamine blockade effects
• Limbic and frontal cortical regions: antipsychotic effect
• Basal ganglia: Extrapyramidal side effects (EPS)
• Hypothalamic-pituitary axis: hyperprolactinemia

Typical Antipsychotic limitation:
Extrapyramidal side effects (EPS)• Parkinsonism• Akathisia• Dystonia• Tardive dyskinesia (TD)-- the worst form
of EPS-- involuntary movements

Parkinsonian side effects
• Rigidity, tremor, bradykinesia, masklike facies
• Management: – Lower antipsychotic dose if feasible– Change to different drug (i.e., to an atypical
antipsychotic)– Anticholinergic medicines:
• benztropine (Cogentin)• trihexylphenidine (Artane)

Akathisia
• Restlessness, pacing, fidgeting; subjective jitteriness; associated with suicide
• Resembles psychotic agitation, agitated depression
• Management: – lower antipsychotic dose if feasible– Change to different drug (i.e., to an atypical
antipsychotic)– Adjunctive medicines:
• propanolol (or another beta-blocker)• benztropine (Cogentin)• benzodiazepines

Acute dystonia
• Muscle spasm: oculogyric crisis, torticollis, opisthotonis, tongue protrusion
• Dramatic and painful• Treat with intramuscular (or IV)
diphenhydramine (Benadryl) or benztropine (Cogentin)

Tardive Dyskinesia (TD)
• Involuntary movements, often choreoathetoid
• Often begins with tongue or digits, progresses to face, limbs, trunk
• Etiologic mechanism unclear• Incidence about 3% per year with
typical antipsychotics– Higher incidence in elderly

Show Tardive Dyskinesia Videotape
Abnormal Involuntary Movement Scale (AIMS) training tape

Neuroleptic Malignant Syndrome
(NMS)• Fever, muscle rigidity, autonomic instability,
delirium• Muscle breakdown indicated by increased CK• Rare, but life threatening• Risk factors include:
– High doses, high potency drugs, parenteral administration
• Management: – stop antipsychotic, supportive measures (IV fluids,
cooling blankets, bromocriptine, dantrolene)

Typical Antipsychotic limitation: Other common side effects
• Anticholinergic side effects: dry mouth, constipation, blurry vision, tachycardia
• Orthostatic hypotension (adrenergic)• Sedation (antihistamine effect)• Weight gain
• “Neuroleptic dysphoria”

Typical Antipsychotic limitation: Treatment Resistance
• Poor treatment response in 30% of treated patients
• Incomplete treatment response in an additional 30% or more