Embed Size (px)
Citation preview

ACUTE INVASIVE FUNGAL SINUSITIS B Y: H A M E D B A S S E R I , P G Y- 2
Case of the Month

C L I N I C A L P R E S E N TAT I O N :
• An 80 yo male patient is brought to the ER with altered level of consciousness with limited available history.
• On Examination: the patient is febrile at 39.8oC. Right-sided proptosis with periorbital swelling and erythema is noted
• A CT Head is ordered by the medical team

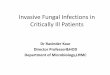
U N E N H A N C E D C T H E A D F I N D I N G S :
• Representative axial non-contrast CT Head images at the level of base of skull.

U N E N H A N C E D C T H E A D F I N D I N G S :
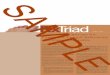
• Representative axial non-contrast CT Head image in bone window

• Representative coronal images from non-contrast CT Head. The right images is presented in bone window.
U N E N H A N C E D C T H E A D F I N D I N G S :

I M A G I N G F I N D I N G S
• CT demonstrates a lobulated heterogenous soft tissue mass centred in the right pterygopalatine fossa
• This mass involves the posterior nasal passage, ethmoid and sphenoid sinuses
• There is extensive bony destruction and evidence of minimal intracranial extension
• In addition, there is orbital extension of mass with resultant proptosis

D I F F E R E N T I A L C O N S I D E R AT I O N S :
• Acute Invasive Fungal Sinusitis
• Sinonasal squamous cell carcinoma
• Complicated Rhinosinusitis
• Sinonasal Wegner’s Granulomatosis
• Sinonasal Non-Hodgkin Lymphoma

D I A G N O S I S
• While CT features were suggestive, they were not sufficient to make the diagnosis
• Endoscopic biopsy was performed
• Pathology demonstrated high levels of fungal elements (Mucor sp.) favouring diagnosis of acute invasive fungal sinusitis
• No pathologic features to suggest of neoplasm

A C U T E I N VA S I V E F U N G A L S I N U S I T I S
T Y P I C A L I M A G I N G F E AT U R E S• Non-contrast CT:
• Soft tissue opacification with bony erosive changes
• Often unilateral with involvement of sphenoid and ethmoid sinuses [1]
• Can extend along vessels or intracranially with resultant complications such as cavernous sinus thrombosis, carotid artery invasion/occlusion or pseduoaneurysm [1]
• Contrast -enhanced study is optimal for evaluation of soft tissue infiltration as well as bony erosions [4]
• MR
• Better for assessment extent of intraocular extension [1]
• Leptomeningeal enhancement should be excluded in early intracranial extension [1]

A C U T E I N VA S I V E F U N G A L S I N U S I T I S
C L I N I C A L C O N S I D E R AT I O N S
• Most commonly occurs in immunocompromised patients, especially diabetics and elderly [5]
• Mucormycosis and Aspergillus are the most common causative organisms [5]
• Variable clinical presentation: acute fever, facial pain, nasal congestion, epistaxis, visual changes, altered LOC [2]

A C U T E I N VA S I V E F U N G A L S I N U S I T I S
M A N A G E M E N T
• Acute invasive fungal sinusitis is a source of significant morbidity and mortality [3]
• Histopathologic diagnosis is crucial to guide management
• Overall survival is poor with high risk of long term complications [2]
• Treatment includes empiric IV antifungal therapy (ie. Amphotericin B) [2]
• Surgical consultation for radical debridement is often necessary [2]

R E F E R E N C E S
[1] Aribandi M, McCoy VA, Bazan C 3rd. Imaging Features of Invasive and Noninvasive Fungal Sinusitis: A Review. Radiographics. 2007 Sep-Oct;27(5):1283-96.
[2] Cox, GM & Perfect, JR (2016) Fungal rhinosinusitis. In: UpToDate. UpToDate, Waltham, MA.
[3] Knipe H & Gaillard F. Acute Invasive Fungal Sinusitis. In: Radiopedia.org. rID: 9367
[4] Michel, MA. (2016). Invasive Fungal Sinusitis. In: StatDx.
[5] O’Brien, William T. Sr. (2010). Top 3 Differentials in Radiology. New York, NY: Thieme Medical Publishers Inc.