Embed Size (px)
DESCRIPTION
fungal
Citation preview
MarioF.Romagnoli-1993The literature does not seem to support any increased incidence of nasal or paranasal colonization or infection with fungi, although we have recently seen a healthy, immunocompetent man who presented with diplopia and sphenoid mass lesion.
A. T. Henrici - 1939
In man and mammals fungal infections are so rare as to be of little practical importance
FUNGAL SINUSITIS
Dr. Ajay George
Goals of today’s class TO GET ATTENDANCE. To understand the pathogenesis of fungal
sinusitis. To know about the causative agents. To know the principles of treatment.
Predisposing Factors:
•Uncontrolled diabetics.
•Chronic renal failure.
•Immuno compromised patients.
HIV
Leukaemias
Drugs
Chronic debilitating illness.
Conidiobolus coronatus(Rhinophycomycosis)
Cases seen in Central Africa, Brazil, West Indies.
Presents as polyps/ granulomas. Lesions spread submucosally. Treatment is removal of mass & amphotericin.
Rhinocerebral phycomycosis
Caused by Rhizopus oryzae, Mucor javanicus, Mucor circinelloides, Absidia corymbitera.
Usually a saprophyte. Marked affinity for blood vessels. Involves Nose, PNS, Orbit, Brain. Disease is confirmed by biopsy. Local drainage & debridement & Amphotericin
Aspergillosis
Caused by A. fumigatus, A. niger, A. flavus. Causes all forms of fungal sinusitis. Diagnosis is from fresh scrappings, Treatment depends on manifestation.
Blastomycosis
Caused by thermally diamorphic fungus Blastomyces dermatidis.
Common in North America – Ohio & Mississippi river valley areas.
Confirmation by special staining and serology. It is rarely fatal. Treatment depends on severity.
Cryptococcosis
Caused by Cryptococcus neoformans. Found in avian excreta. Predeliction for lung and brain. Usually completely treatable.
Actinomycosis
Actinomyces israelii is pathogenic for humans. Trauma predisposes for pathogenicity. Treatment is high dose penicillin.
Candidiasis
Caused by Candida albicans. Presents as small, discrete, pearly or dirty white
patches on red moist mucous membrane which can be easily removed without bleeding.
Treatment is by local application of 1% aqueous gentian violet or nystation.
Histoplasmosis
Caused by Histoplasma capsulatum. Common in central USA. Diagnosis is by biopsy and histoplasmin skin
test. Treatment is by amphotericin.
Sporotrichosis
Caused by Sporothrix schenckii. Infection of mucosa is usually by implantation. Treatment is by iodides or amphotericin.
FULMINANT FUNGAL SINUSITIS
Clinical Course :Acute Host :Immunocomprised Pathology :Tissue Invasion Organisms :Aspergillus, Mucor Sinus Involvement :Single or multiple Treatment :Radical
debridement&Anti-
fungal therapy
INDOLENT FUNGAL SINUSITIS Clinical Course :Chronic Host :Immunocompetent Pathology :Granuloma Organisms :Aspergillus,
Dematiaceous fungi Sinus Involvement :Single or multiple Treatment :Radical
debridement&Anti-
fungal therapy SOS
MYCETOMA
Clinical Course :Chronic Host :Immunocompetent Pathology :Fungal ball Organisms :Aspergillus Sinus Involvement :Single Treatment :Debridement&
Aeration

ALLERGIC FUNGAL SINUSITIS
Clinical Course : Chronic Host : Atopic Pathology : Allergic mucin Organisms : Aspergillus,
Dematiaceous fungi Sinus Involvement : Multiple Treatment : Debridement,
Steroids& Immunotherapy
DIAGNOSTIC CRITERIAdeShazo Criteria (1995) Typical radiographic picture of sinusitis Macroscopic/histopathological demonstration of
allergic mucin Positive fungal stain/culture from surgery specimen No immunocompromise No evidence of tissue invasion
Bent & Kuhn Modification Positive skin tests to fungal antigens
ETIOLOGYAge : Young adultsGender : No marked trendsEnvironment : Moist & dustyCausative Agents :
Mainly dematiaceous fungi like Bipolaris, Curvularia, Exserohilum, Alternaria, Drechslera, Helminthosporium, and Fusarium,
Sometimes aspergillus
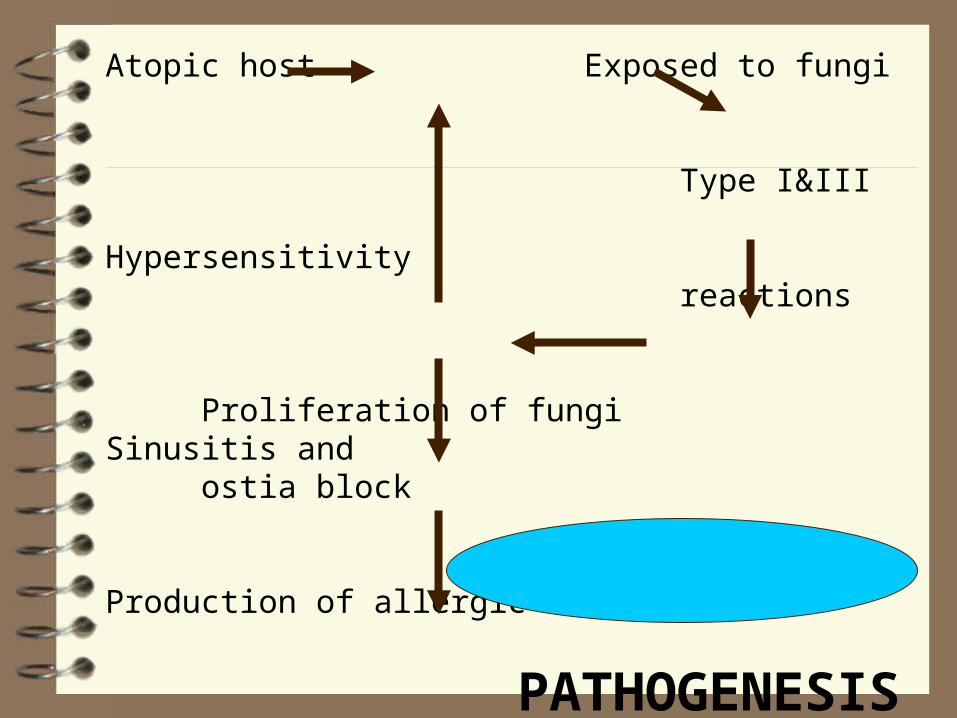
Atopic host Exposed to fungi
Type I&III Hypersensitivity
reactions
Proliferation of fungi Sinusitis and ostia block
Production of allergic mucin
PATHOGENESIS Polyposis and bony expansion
PRESENTING COMPLAINTS
Nasal ObstructionAllergic RhinitisPurulent RhinorrhoeaPost Nasal DripHeadacheFacial DeformityLoss of Vision
EXAMINATION FINDINGS
Intranasal inflammationPolyposisFacial Dysmorphism
Proptosis
Telecanthus
Malar flattening
Optic Nerve Compression

SPECIFIC INVESTIGATIONS
Serum Total IgEFungal Specific IgE, IgG, IgMSkin TestingRadioallergosorbent TestC T ScanHistopathology

TREATMENT
SurgeryCorticosteroidsImmunotherapyAnti-fungal agents






TAKE HOME MESSAGE
Fungal infestations of paranasal sinuses are relatively common
Even immunocompetent persons can get affected High degree of suspicion is necessary for diagnosis CT Scan, fungal serology and proper
microbiological study are very important for diagnosis
Standard therapy protocol with long term follow-up is necessary for good cure rates
FEEDBACK
Q.1 Did you get to learn anything new today which you can recollect ?
Q.2 Was information given more than necessary?
Q.3 Rate the lecture on a scale of 0 – 10.
Q.4 Any other comments or suggestions.
SMS – 9866236046SMS – 9866236046
Mail – [email protected] – [email protected]