Embed Size (px)
Citation preview

Active TB Drug-Safety
Monitoring and Management
(aDSM)
National TB ProgrammeDepartment of Public HealthMinistry of Health and Sports
The Republic of the Union of Myanmar

ACKNOWLEDGEMENTS 5
ABBREVIATIONS 6
INTRODUCTION 7
DEFINITIONS 9
OBJECTIVES OF aDSM 9
PURPOSE AND SCOPE of the aDSM Manual 10
ESSENTIAL ELEMENTS OF aDSM 10
LEVELS OF aDSM MONITORING 13
IMPLEMENTATION STEPS OF aDSM 14
1. Create a national coordinating mechanism for aDSM 14
2. Develop a plan for aDSM 15
3. Definemanagementandsupervisionrolesandresponsibilities 15
4. Create standard data collection materials 16
5. Train staff for collection of data 17
6. Defineschedulesandroutesfordatacollectionandreporting 17
7. Consolidate data electronically 20
8. Develop capacity for signal detection and causality assessment 20
ROLES AND RESPONSIBILITIES 20
CAUSALITY ASSESSMENT 22
SIGNAL DETECTION 25
ANNEXES 26
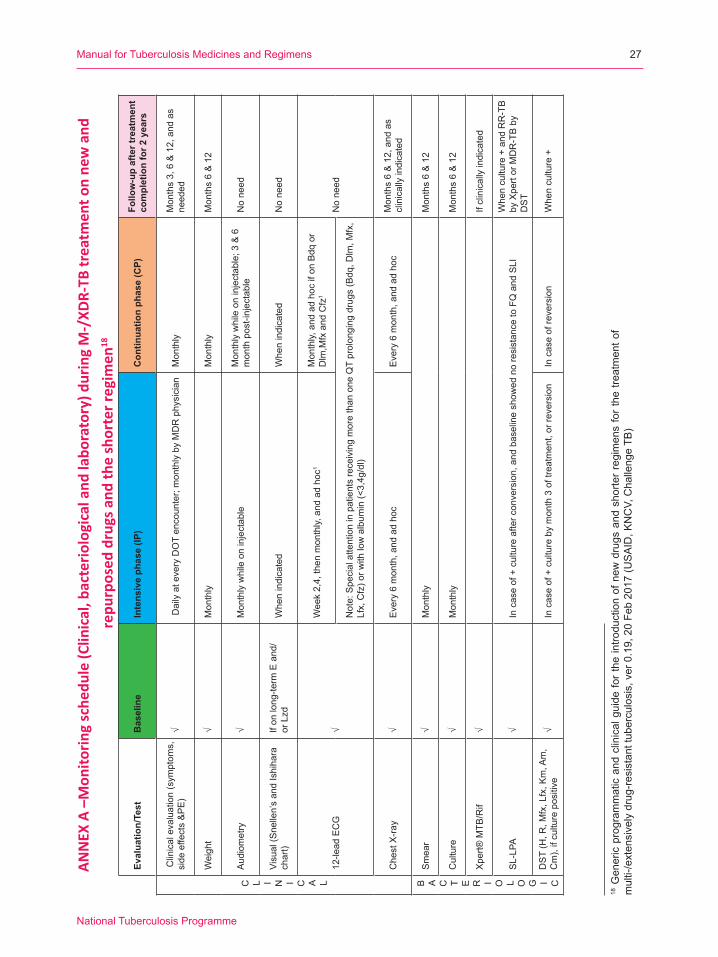
ANNEXA Monitoringschedule(Clinical,bacteriologicalandlaboratory)
during M-/XDR-TB treatment on new and repurposed drugs and
the shorter regimen 27
ANNEXB ProgrammaticindicatorsforaDSM(WHOGuidelines,2014) 29
ANNEXC MDR-TBTreatmentCard(DR-TBForm01)includingnewdrugs,and
new regimens 31
ANNEXD NTPFormforReportingSeriousAdverseEvent(SAE) 37
ANNEX E Severity grading scales and suggested action for common AEs 39
CONTENTS

ACKNOWLEDGEMENTS
The Ministry of Health and Sports, Myanmar would like to express its sincere thanks to Professor Tin Maung Cho, Professor Win Naing, Professor Ye Tun and Professor Yadanar Kyaw for their technicalsupportandtimeinwritingthisManual;MyanmarFoodandDrugAdministration(FDA),TBspecialistHospitalsfortheircollaborationandsupport,theWorldHealthOrganizationforitsinitiative in developing the national aDSM plan and providing technical assistance to this manual; MédecinsSansFrontières(MSF)foritscollaboration;andDr.MamelQuelapio,SeniorConsultantfromKNCVTuberculosisFoundationforhertechnicalsupportintheprocessofaDSMManualdevelopment. The development of this aDSM Manual was undertaken in 2017 with support from the USAID-funded Challenge TB project.
TheGlobalHealthBureau,OfficeofHealth,InfectiousDiseaseandNutrition(HIDN),UnitedStatesAgency for InternationalDevelopment,financiallysupports thisguide throughChal-lengeTBunderthetermsofAgreementNo.AID-OAA-A-14-00029.ThisfieldguideismadepossiblebythegeneroussupportoftheAmericanpeoplethroughtheUnitedStatesAgencyforInternationalDevelopment(USAID).ThecontentsaretheresponsibilityofChallengeTBanddonotnecessarilyreflecttheviewsofUSAIDortheUnitedStatesGovernment.
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
5
ADR/AR Adverse drug reaction/Adverse reaction
aDSM Active TB Drug-Safety Monitoring and Management
AE Adverse event
Bdq Bedaquiline
CA Causality assessment
Cfz Clofazimine
Dlm Delamanid
DR-TB Drug-resistanttuberculosis
FDA Food and Drug Administration
Gfx Gatifloxacin
MDR-TB Multidrug-resistanttuberculosis
Mfx Moxifloxacin
NTP NationalTuberculosisProgramme
PMDT ProgrammaticManagementofDrug-ResistantTuberculosis
PV Pharmacovigilance
SAE Serious adverse event
SLD Second-line drug
TB Tuberculosis
UMC Uppsala Monitoring Centre
WHO WorldHealthOrganization
XDR-TB Extensively drug-resistanttuberculosis
ABBREVIATIONS
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
6

INTRODUCTION
1WorldHealthOrganization.WHOGlobalTuberculosisReport,2016.WHO-Geneva.WHO/HTM/TB/2016.132NationalStrategicPlanforTuberculosis2016-2020,NationalTBProgramme,NTP,Myanmar.3Theuseofbedaquilineinthetreatmentofmultidrug-resistantTBWHO-Geneva.InterimPolicyGuidance,WHO-Geneva,2013. WHO/HTM/TB/2013.64 The use of delamanid in the treatment of multidrug-resistant TB WHO-Geneva. Interim Policy Guidance WHO- Geneva, 2014. WHO/HTM/TB/2014.235WHOtreatmentGuidelinesfordrug-resistanttuberculosis,2016update.WHO-Geneva,2016.WHO/HTM/TB/2016.046Active tuberculosis drug-safetymonitoring andmanagement: Framework for implementation.WHO-Geneva, 2015.WHO/HTM/TB/2015.28
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
7
Myanmarisoneofthe30highburdencountriesforTB,multidrug-resistant(MDR)TBandTB/HIV.1
ToimplementaneffectivestrategytocombatandcontrolTB/MDR-TB,theNTPhasdevelopeda5-yearNationalStrategicPlanforTuberculosis2016-2020(NSP)2 that includes the programmatic managementofdrug-resistantTB(PMDT)asoneofthekeyinterventions.Managementofdrug-resistantTB(DR-TB)ischallengingduetoprolongedtreatmentduration,costlyregimen,andsideeffects of the drugs that lead to poor treatment adherence. New and innovative strategies are needed to address these challenges.
Recently,WHOhasapprovedtheuseofnewanti-tuberculosis(TB)medicines,Bedaquiline(Bdq)andDelamanid(Dlm)undercertainconditions.3, 4 Moreover, a shorter regimen for MDR-TB that includesrepurposeddrugs,suchasclofazimine(Cfz)andmoxifloxacin(Mfx)hasbeenapprovedandrecommendedbyWHOintheDrug-resistantTBguidelines,2016update.5 The introduction of new and repurposed TB medicines, some given at higher dosages than previously used, and somedrugswith potentially additive toxicity given in combination, prompts the importance ofactivepharmacovigilance(PV)systemforpatientsonTBtreatment.Additionally,forHIVpatientsontreatment,someofthenewTBdrugshavebeenobservedtomanifestdrug-druginteractionswith certain anti-retroviral medicines.
Toaddressthisissue,theWHOGlobalTBProgramme(WHO/GTB)andtheEssentialMedicinesProducts department drew on the input of technical partners to develop the concept of active TB drug safety monitoring and management (aDSM), defined as the “active and systematicclinicaland laboratoryassessmentofpatientswhileon treatment.” aDSMapplies topatientson treatment with new anti-TB drugs, new MDR-TB regimens, including the shorter treatment regimen, andextensively drug-resistantTB (XDR-TB) regimens.6 The purpose of aDSM is to detect,manage,andreportsuspectedorconfirmeddrugtoxicitiesinatimelyfashion.Afeedbackmechanism tocareprovidersneeds tobe inplace for theirknowledgeandneededaction forpatient management.

7ActiveTBdrug-safetymonitoringandmanagement (aDSM) for treatmentofMDR/XDR-TBusingnewor repurposeddrugsinMyanmar:Debriefing,aDSMmission,Myanmar2-6May2016,WHO.
UpontherequestoftheNTP,theTechnicalOfficer,TechnicalSupportCoordination(TSC)GlobalTBProgramme (GTB),WHO (Geneva) conducted an aDSMmission on 2-6May 2016.7 The current national PV system in Myanmar for all diseases involves spontaneous reporting of adverse events(AEs)byvoluntaryreportingofhealthcareworkers.ThishasbeenmanagedbytheFoodandDrugAdministration(FDA)/Drugcontrolsectionalthoughwithlimitedhumanresources.AnAEReportingForm(inMyanmarlanguage)isinplacebutwithlimitedimplementation,andwithnoTB-relatedAEreportssubmittedasofyet.BdqandDlmwere introduced in thecountry inMarch2016 through theEndTBproject implementedby theNTP,AungSanTBHospital andMSF-Holland. The PV system of the EndTB project is an advanced package with reporting of seriousAEs(SAEs)plusAEsofspecialinterestandclinicalsignificance(seeDefinitions).Whilean advanced package is relevant in a project or research study context, programmatic aDSM implementationwithamoresimplifiedsystemismoreappropriateintheNTPwhereresourcesare limited, in order to scale it up more widely.
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
8

DEFINITIONS 1. Active drug-safety monitoring and management (aDSM): active and systematic
clinical and laboratory assessment of patients while on treatment. aDSM applies topatientsontreatmentwith(a)newanti-TBdrugs,suchasBdqandDlm;(b)newDR-TBregimens,suchastheshorter(or9-month)MDR-TBregimen;or(c)XDR-TBregimensonnew/repurposeddrugs,inordertodetect,manageandreportsuspectedorconfirmeddrug toxicities.
2. Adverse event (AE): any untoward medical occurrence that may present in a TB patient duringtreatmentwithapharmaceuticalproduct,butwhichdoesnotnecessarilyhaveacausal relationship with this treatment.
3. Adverse drug reaction (ADR): a response to a TB medicine that is noxious and unintended, and which occurs at doses normally used in humans.
4. Causality assessment: the evaluation of the likelihood that a TB medicine was the causativeagentofanobservedadversereaction.
5. Serious adverse event (SAE): an AE which either leads to death or a life-threatening experience;tohospitalizationorprolongationofhospitalization;topersistentorsignificantdisability;ortoacongenitalanomaly.SAEsthatdonotimmediatelyresultinoneoftheseoutcomesbutwhichrequireaninterventiontoprevent it fromhappeningareincluded.SAEs may require a drastic intervention, such as termination of the drug suspected of having caused the event.
6. AE of special interest: AE documented to have occurred during clinical trials and for which themonitoring program is specifically sensitized to report regardless of itsseriousness, severity or causal relationship to the TB treatment
7. AE of clinical significance:AE that iseithera)serious (SAE),b)ofspecial interest,c) leads toadiscontinuationorchange in the treatment,or,d) is judgedasotherwiseclinicallysignificantbytheclinician
8. Signal: reported information on a possible causal relationship between an adverseeventandaTBmedicine,therelationshipbeingunknownorincompletelydocumentedpreviously or representing a new aspect of a known association
OBJECTIVES OF aDSMTheoverallobjectivesofaDSMaretoreducerisksfromdrug-relatedharmsinpatientsonsecond-line(SL)treatmentforDR-TBandtogeneratestandardizedaDSMdatatoinformfuturepolicyupdates on the use of such medicines. aDSM aims to detect, manage, and report suspected or confirmeddrugtoxicitiesinatimelyfashion.
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
9
PURPOSE AND SCOPE of the aDSM ManualThe purpose of this aDSM Manual is to provide a step-by-step guide to programmaticallyimplementasustainableaDSMsysteminlinewiththeWHO-recommendedaDSMFramework.8
ThisManualwillbeapplicable topatientson1) new and repurposed drugs, 2) new DR-TB regimens such as the shorter treatment regimen, and 3) XDR-TB regimens. This document willdescribethedetection,activemonitoringandmanagementofDR-TBpatientsusingclinicalandlaboratoryassessment,aswellasrecordingandreportingofSAEs.
ESSENTIAL ELEMENTS OF aDSMTherearethreeessentialelementsofaDSMtoachievetheaboveobjectives:
1. Active and systematic clinical and laboratory assessment during treatment to detect drug toxicity and AEs. There are ways to help health providers do this step.
a. Observe and listen to patients. The detection of AEs is primarily dependent upon reporting from patients, nurses, doctors, counsellors, etc. At every DOT encounter, healthworkersshouldaskthepatientandfamilymembersaboutclinicalsymptomsof common AEs including nausea, vomiting, peripheral neuropathy, skin rash, psychiatricdisturbance(headache,anxiety,depression,irritability,behaviorchange),hearingloss,jaundice,vestibulartoxicity(vertigo,ataxia,hearingloss),andsymptomsofelectrolytewasting (musclecramping,palpitations).Allhealthcareprofessionalsinvolvedmustbetrainedonadverseeventscreening.
b. Performroutine clinical assessments, e.g., for treatment adherence and tolerance, psychosocial support and consults with the psychiatrist, ophthalmologist, HIV specialist, etc. Clinical follow-up with the MDR-TB physician for all patients is at a minimum of 2 weeks after the start of MDR-TB treatment, then monthly until the treatment completion.
c. Scheduleregularlaboratoryscreening,evenifthepatienthasnospecificcomplaints,e.g.,creatinine,ECG,liverfunctiontests,etc.Regularlaboratorymonitoringdetectsoccultadverseeffects.Laboratorytestsandproceduresrelatedtotreatmentshouldbeavailableandaccessibletopatients,freeofcharge.
8Active tuberculosis drug-safetymonitoring andmanagement: Framework for implementation.WHO-Geneva, 2015.WHO/HTM/TB/2015.28
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
10
Annex Ashowsthescheduleofclinicalandlaboratorytestsforpatientsonnewandrepurposeddrugsandtheshortertreatmentregimen(STR).AsBdqandDlm,Mfx,andCfzmay induceQTprolongation,ECGmonitoring isessential.ChallengeTBrecentlyissuedrecommendationsonthemeasurementofQTprolongation.9
2. Management of AEs in a timely manner. Early detection of signs and symptoms is key to proper management of AEs that significantly impacts patient well-being,overall treatment acceptance, and adherence. Management includes measures taken to alleviate the signs and symptoms of adverse reactions with careful individual case review, suchas:a) reassurance, ifAE isminorb) lowering thedoseof theoffendingdrug,c)stoppingthedrug,d)drugreplacement;e)providingancillarymedicationsandf)otherinterventions(surgery,transfusion,psychologicalsupport,etc.).Ancillarymedicinesshouldbeavailableandaccessibletopatients,freeofcharge.
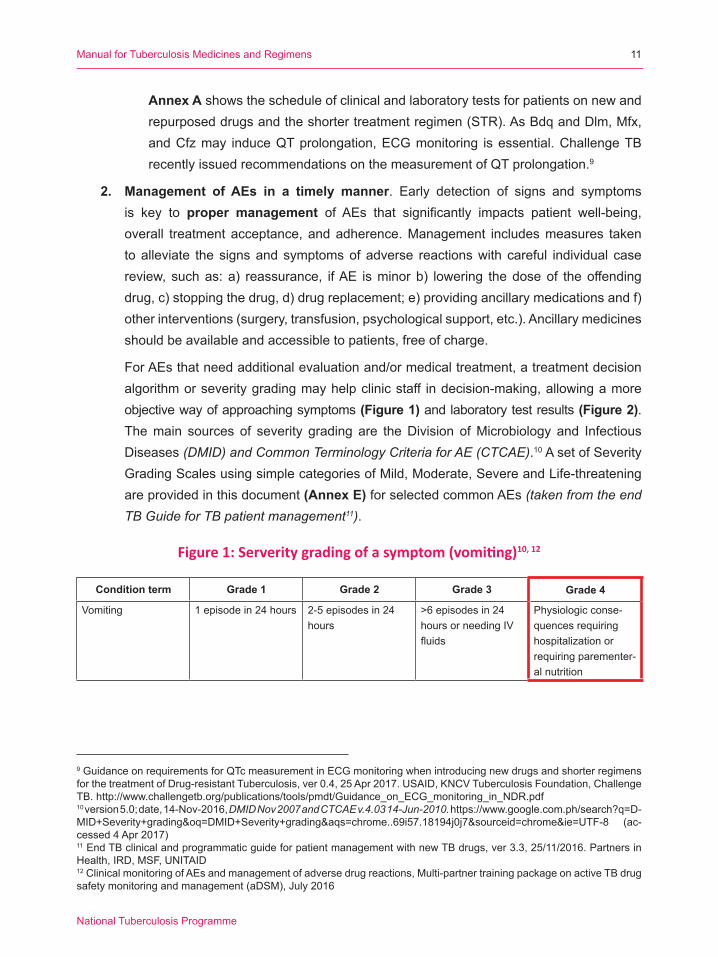
For AEs that need additional evaluation and/or medical treatment, a treatment decision algorithm or severity grading may help clinic staff in decision-making, allowing a more objectivewayofapproachingsymptoms(Figure 1)andlaboratorytestresults(Figure 2). Themain sources of severity grading are theDivision ofMicrobiology and InfectiousDiseases (DMID) and Common Terminology Criteria for AE (CTCAE).10 A set of Severity Grading Scales using simple categories of Mild, Moderate, Severe and Life-threatening are provided in this document (Annex E) for selected common AEs (taken from the end TB Guide for TB patient management11).
Figure 1: Serverity grading of a symptom (vomiting)10, 12
Condition term Grade 1 Grade 2 Grade 3 Grade 4
Vomiting 1 episode in 24 hours 2-5 episodes in 24 hours
>6 episodes in 24 hours or needing IV fluids
Physiologic conse-quences requiring hospitalizationorrequiring parementer-al nutrition
9GuidanceonrequirementsforQTcmeasurementinECGmonitoringwhenintroducingnewdrugsandshorterregimensforthetreatmentofDrug-resistantTuberculosis,ver0.4,25Apr2017.USAID,KNCVTuberculosisFoundation,ChallengeTB.http://www.challengetb.org/publications/tools/pmdt/Guidance_on_ECG_monitoring_in_NDR.pdf10 version 5.0; date, 14-Nov-2016, DMID Nov 2007 and CTCAE v.4.03 14-Jun-2010.https://www.google.com.ph/search?q=D-MID+Severity+grading&oq=DMID+Severity+grading&aqs=chrome..69i57.18194j0j7&sourceid=chrome&ie=UTF-8 (ac-cessed4Apr2017)11 End TB clinical and programmatic guide for patient management with new TB drugs, ver 3.3, 25/11/2016. Partners in Health, IRD, MSF, UNITAID 12 Clinical monitoring of AEs and management of adverse drug reactions, Multi-partner training package on active TB drug safetymonitoringandmanagement(aDSM),July2016
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
11
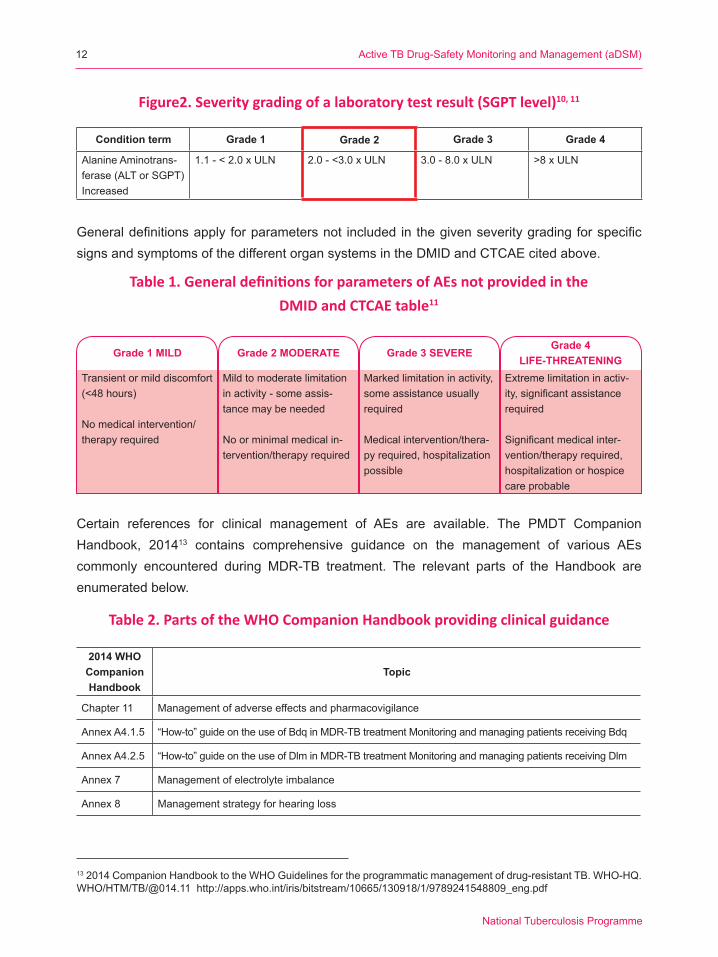
Generaldefinitionsapplyforparametersnot included inthegivenseveritygradingforspecificsignsandsymptomsofthedifferentorgansystemsintheDMIDandCTCAEcitedabove.
Certain references for clinical management of AEs are available. The PMDT CompanionHandbook, 201413 contains comprehensive guidance on the management of various AEs commonly encountered during MDR-TB treatment. The relevant parts of the Handbook areenumeratedbelow.
Figure2. Severity grading of a laboratory test result (SGPT level)10, 11
Condition term Grade 1 Grade 2 Grade 3 Grade 4
Alanine Aminotrans-ferase(ALTorSGPT)Increased
1.1 - < 2.0 x ULN 2.0 - <3.0 x ULN 3.0 - 8.0 x ULN >8 x ULN
Table 1. General definitions for parameters of AEs not provided in theDMID and CTCAE table11
Grade 1 MILD Grade 2 MODERATE Grade 3 SEVEREGrade 4
LIFE-THREATENINGTransient or mild discomfort (<48hours)
No medical intervention/therapy required
Mild to moderate limitation in activity - some assis-tancemaybeneeded
No or minimal medical in-tervention/therapy required
Marked limitation in activity, some assistance usually required
Medical intervention/thera-pyrequired,hospitalizationpossible
Extreme limitation in activ-ity,significantassistancerequired
Significantmedicalinter-vention/therapy required, hospitalizationorhospicecareprobable
132014CompanionHandbooktotheWHOGuidelinesfortheprogrammaticmanagementofdrug-resistantTB.WHO-HQ.WHO/HTM/TB/@014.11http://apps.who.int/iris/bitstream/10665/130918/1/9789241548809_eng.pdf
Table 2. Parts of the WHO Companion Handbook providing clinical guidance
2014 WHO Companion Handbook
Topic
Chapter 11 Management of adverse effects and pharmacovigilance
Annex A4.1.5 “How-to”guideontheuseofBdqinMDR-TBtreatmentMonitoringandmanagingpatientsreceivingBdq
Annex A4.2.5 “How-to”guideontheuseofDlminMDR-TBtreatmentMonitoringandmanagingpatientsreceivingDlm
Annex 7 Managementofelectrolyteimbalance
Annex 8 Management strategy for hearing loss
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
12
14 EndTB clinical and programmatic guide for the patient management with new TB drugs, version 3.3, 25/11/2016. Part-ners in Health, Medecins sans Frontieres, IRD, UNITAID
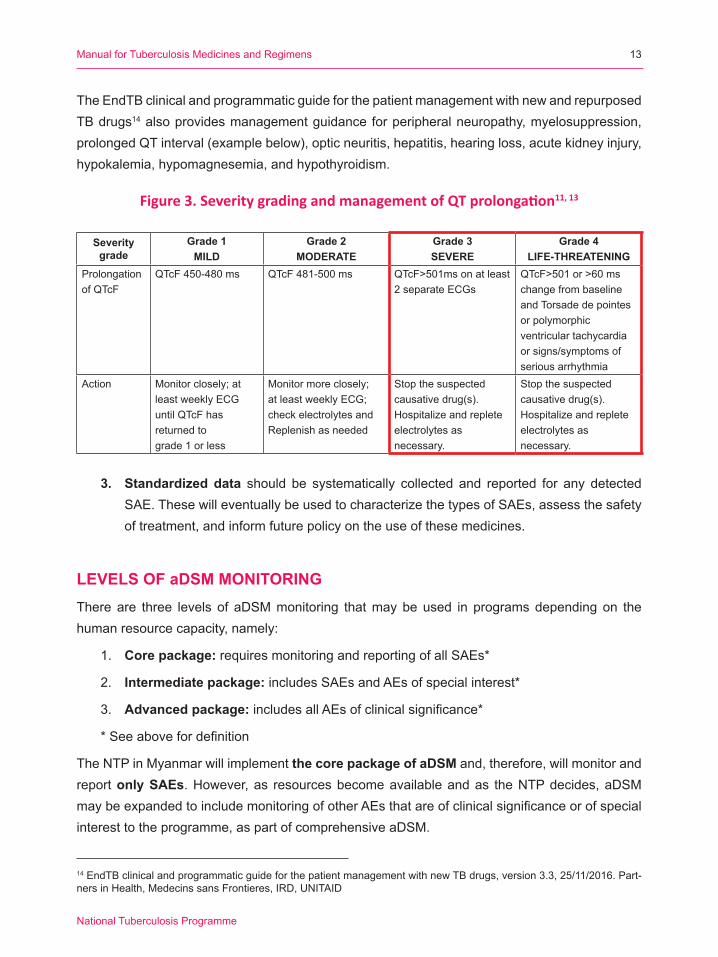
The EndTB clinical and programmatic guide for the patient management with new and repurposed TB drugs14 also provides management guidance for peripheral neuropathy, myelosuppression, prolongedQTinterval(examplebelow),opticneuritis,hepatitis,hearingloss,acutekidneyinjury,hypokalemia, hypomagnesemia, and hypothyroidism.
Figure 3. Severity grading and management of QT prolongation11, 13
Severity grade
Grade 1MILD
Grade 2MODERATE
Grade 3SEVERE
Grade 4LIFE-THREATENING
Prolongation ofQTcF
QTcF450-480ms QTcF481-500ms QTcF>501msonatleast2 separate ECGs
QTcF>501or>60mschangefrombaselineand Torsade de pointes or polymorphic ventricular tachycardia or signs/symptoms of serious arrhythmia
Action Monitor closely; at least weekly ECG untilQTcFhasreturned tograde 1 or less
Monitor more closely; at least weekly ECG; check electrolytes and Replenish as needed
Stop the suspected causativedrug(s).Hospitalizeandrepleteelectrolytes asnecessary.
Stop the suspected causativedrug(s).Hospitalizeandrepleteelectrolytes as necessary.
3. Standardized data should be systematically collected and reported for any detectedSAE.ThesewilleventuallybeusedtocharacterizethetypesofSAEs,assessthesafetyof treatment, and inform future policy on the use of these medicines.
LEVELS OF aDSM MONITORINGThereare three levels of aDSMmonitoring thatmaybeused in programsdepending on thehumanresourcecapacity,namely:
1. Core package: requires monitoring and reporting of all SAEs*
2. Intermediate package: includes SAEs and AEs of special interest*
3. Advanced package:includesallAEsofclinicalsignificance*
*Seeabovefordefinition
The NTP in Myanmar will implement the core package of aDSM and, therefore, will monitor and report only SAEs.However,as resourcesbecomeavailableandas theNTPdecides,aDSMmaybeexpandedtoincludemonitoringofotherAEsthatareofclinicalsignificanceorofspecialinterest to the programme, as part of comprehensive aDSM.
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
13
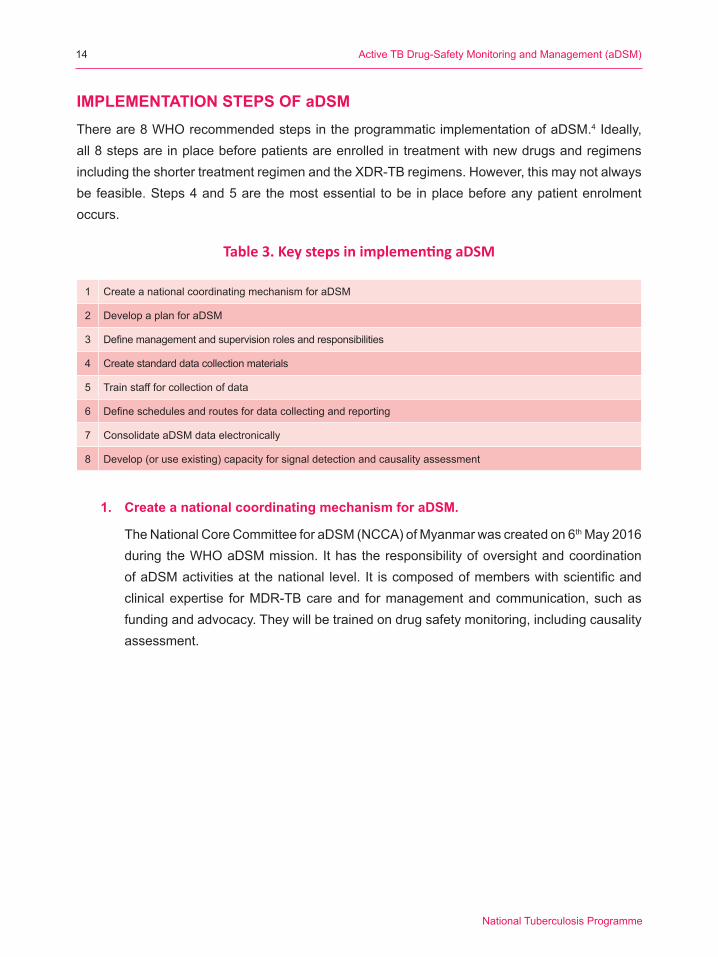
IMPLEMENTATION STEPS OF aDSMThere are 8 WHO recommended steps in the programmatic implementation of aDSM.4 Ideally, all8stepsareinplacebeforepatientsareenrolledintreatmentwithnewdrugsandregimensincluding the shorter treatment regimen and the XDR-TB regimens. However, this may not always befeasible.Steps4and5arethemostessential tobe inplacebeforeanypatientenrolmentoccurs.
1. Create a national coordinating mechanism for aDSM.
TheNationalCoreCommitteeforaDSM(NCCA)ofMyanmarwascreatedon6th May 2016 duringtheWHOaDSMmission. IthastheresponsibilityofoversightandcoordinationofaDSMactivitiesat thenational level. It iscomposedofmemberswithscientificandclinical expertise for MDR-TB care and for management and communication, such as fundingandadvocacy.Theywillbetrainedondrugsafetymonitoring,includingcausalityassessment.
Table 3. Key steps in implementing aDSM
1 Create a national coordinating mechanism for aDSM
2 Develop a plan for aDSM
3 Definemanagementandsupervisionrolesandresponsibilities
4 Create standard data collection materials
5 Train staff for collection of data
6 Defineschedulesandroutesfordatacollectingandreporting
7 Consolidate aDSM data electronically
8 Develop(oruseexisting)capacityforsignaldetectionandcausalityassessment
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
14
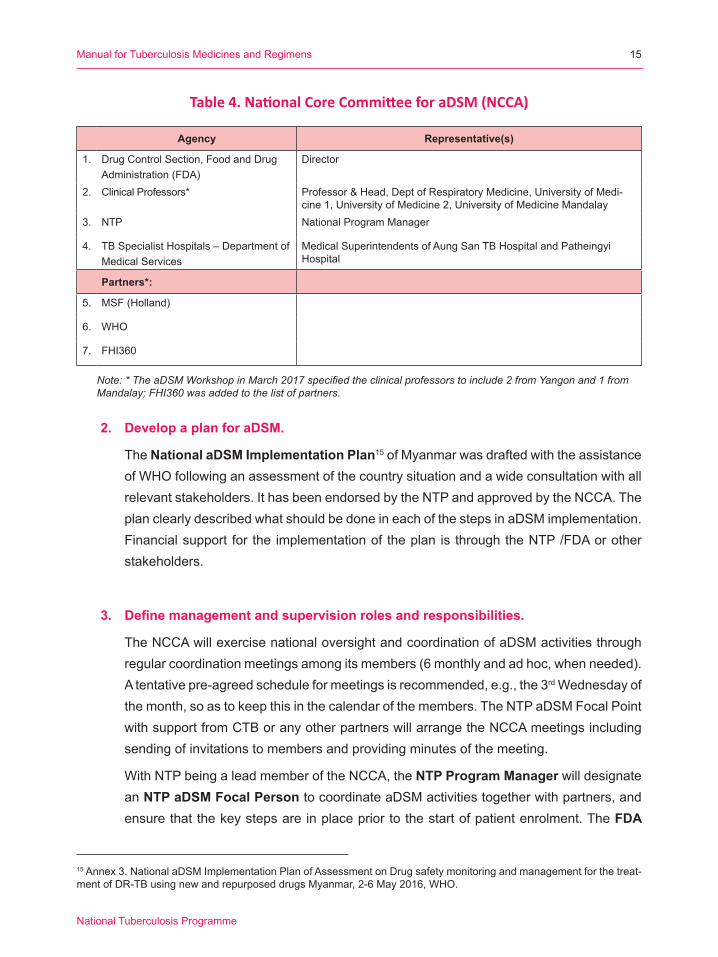
Table 4. National Core Committee for aDSM (NCCA)
Agency Representative(s)
1. Drug Control Section, Food and Drug Administration(FDA)
Director
2. Clinical Professors* Professor & Head, Dept of Respiratory Medicine, University of Medi-cine 1, University of Medicine 2, University of Medicine Mandalay
3. NTP National Program Manager
4. TB Specialist Hospitals – Department of Medical Services
Medical Superintendents of Aung San TB Hospital and Patheingyi Hospital
Partners*:
5. MSF(Holland)
6. WHO
7. FHI360
Note: * The aDSM Workshop in March 2017 specified the clinical professors to include 2 from Yangon and 1 from Mandalay; FHI360 was added to the list of partners.
2. Develop a plan for aDSM.
The National aDSM Implementation Plan15 of Myanmar was drafted with the assistance of WHO following an assessment of the country situation and a wide consultation with all relevantstakeholders.IthasbeenendorsedbytheNTPandapprovedbytheNCCA.TheplanclearlydescribedwhatshouldbedoneineachofthestepsinaDSMimplementation.Financial support for the implementation of the plan is through the NTP /FDA or other stakeholders.
3. Define management and supervision roles and responsibilities.
The NCCA will exercise national oversight and coordination of aDSM activities through regularcoordinationmeetingsamongitsmembers(6monthlyandadhoc,whenneeded).A tentative pre-agreed schedule for meetings is recommended, e.g., the 3rd Wednesday of themonth,soastokeepthisinthecalendarofthemembers.TheNTPaDSMFocalPointwith support from CTB or any other partners will arrange the NCCA meetings including sendingofinvitationstomembersandprovidingminutesofthemeeting.
WithNTPbeingaleadmemberoftheNCCA,theNTP Program Manager will designate an NTP aDSM Focal Person to coordinate aDSM activities together with partners, and ensure that the key steps are in place prior to the start of patient enrolment. The FDA
15 Annex 3. National aDSM Implementation Plan of Assessment on Drug safety monitoring and management for the treat-ment of DR-TB using new and repurposed drugs Myanmar, 2-6 May 2016, WHO.
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
15
Director will likewise designate an FDA aDSM Focal Person to work together with the NTP aDSM Focal Person in coordinating aDSM activities. The current NTP and FDA aDSMFocalPersonshavebeentrainedonPVduringtheAsia-PacificPVCourseinIndiain January 2017.Other opportunities for training should further strengthen the capacity of NCCAmembers.
The Clinical ProfessorswhoaremembersoftheNationalDR-TBExpertCommittee,andotherdesignatedmembers,willprovideclinicaladviceforAEsthatcannotbemanagedintheMDR-TBCentres,andwillberesponsibleforcausalityassessment,afterundergoingtrainingbyexpertsinthisfield.
Monitoring and supervision of the programmatic implementation of aDSM is an important task for the NCCA. The committee will oversee the monitoring of the two essential indicatorsoutoffouraDSMindicatorssuggestedbyWHO(Annex B).Thetwoessentialindicators,namelya)coverage(rateofenrolledpatientscoveredbyaDSM);andb)SAErate among patients treated andmonitored for aDSMwill be used tomonitor aDSMprogrammatic implementation given the current limited resources.
4. Create standard data collection materials
WHO,theClintonHealthAccessInitiative(CHAI),andotherpartnerswillprovidesupportin data collection and M & E.
TheformsrelatedtoaDSMareasfollows:
a. Modified NTP MDR-TB Treatment Card (DR-TB Form 01) (Annex C)
The six-page NTPMDR-TB Treatment Card, based on theWHO recommendedtemplate, is the standard card used for all DR-TB patients enrolled in treatment. For aDSMpurposes,somerevisionshavebeenmadeontheoriginalTreatmentCard,whichareasfollows:
• Page1: Addedabbreviationsfornewandrepurposeddrugs;modifiedtableforDST
• Page2: Provided 4 columns for liver function tests (LFT) [bilirubin, alkalinephosphatase, aspartate aminotransferase (AST) and alanineaminotransferase(ALT)]
• Page3: Providedseparate tables; thefirst table (ascontinuationof the tableonpage2),3columnsforelectrolytes,addedcolumnsforalbuminandlipase,andanewtableforECG/QTc,andaudiometryforfollow-up.
• Page4: addedonecolumnforfollow-upmonthandyear(mm-yy).
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
16
• Page5: Updatedthecolumnheadingwithnewandrepurposeddrugs;anewtabletorecordtheissues,discussionanddecisionbyExpertPanel.
• Page6: Included a comment box, outcome categories with new categories(moved to either conventional regimen or individualized regimen);added a table to record patients’ information during 2 years aftercompletion of treatment.
b. Form for Reporting of Serious Adverse Event
This form is a simplified version of theMSFSAEFormdeveloped byWHOwithinputsfromtheNCCAmembers,andisnowbeingusedbythefocalMSF-HdoctorfortheEndTBProjectinAungSanTBSpecialistsHospital(ASTSH).ThisformistobefilledoutbytheMDR-TBHospitalphysicianeverytimeanSAEisdetectedduringthecourseoftreatment.ThisformwillbeusedtoalerttheNTPandtheNCCA,andwill also be sent to theRegion/StateDR-TBCommittee for their information andclinical inputs. TheReporter/ the attending (on duty) clinician from theHospital /MDR-TBcentrewillenterallavailableinformationatthetimeofreporting,andwillsubmittheformwithin24hoursfromSAEdetection.AllothermissinginformationinthisformwillbefilledoutandtransmittedtotheNCCAwithin72hours.
Fornow,alldatacollectionformsarepaper-based,andshouldbekepton-site,andfiledforelectronicdataentryinthefuture(whenanaDSMelectronicdatabaseisdeveloped).
5. Train staff for collection of data
Thetrainingwillcover,mostimportantly,datacollection(whichhappensbothinthehospitalwhenthepatientisstillconfined,andintheout-patientsettingafterdischarge),reportingflow, as well as the basics of aDSM, clinical monitoring and management, causalityassessment, and signal detection. Training participants will include those involved in direct patient care, in providing clinical advice, performing causality assessment and signaldetection,andinsupervisionandmonitoringofbothhospitalizedandambulatoryphases of treatment.
6. Define schedules and routes for data collection and reporting
UnderthecoreaDSMpackage,reportingismainlyforSAEsdetectedandidentifiedwhileontreatmenteitherintheMDR-TBhospitalorinthecommunityduringtheambulatoryphase.
A. ThehospitalorMDR-TBCentresubmitstheSAEReportingForm(Annex D) within 24 hours of SAE detectionbyemailtothefollowing:
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
17
a. Region/StateDR-TBCommittee:This is to inform theCommitteeof theSAE,andtoseektechnicalassistance,beitforprogrammaticorclinicalmanagementpurposes.
b. NCCA:TheNTPProgramManagerneedstoknowtheSAE,andwillsupervisetheNTPaDSMFocalPoint(whoiscopyfurnishedwiththeSAEForm)inquicklyreviewing the entries of the SAE Form for completion, consistency and accuracy.
B. TheNTPaDSMFocalPointverifieswiththehospitalreporteranyunclearinformation.Within 72 hours,all information in theSAEFormmusthavebeencompletedandreceivedbytheNTPaDSMFocalPoint.
C. TheNPTaDSMFocalPointwill forwardthecompletedSAEFormbyemail tothefollowing:
a. Clinical Professors who aremembers of the NCCA and the National DR-TBExpertCommitteeandtotheothermembersoftheNCCAfortheirinformation,their review and clinical inputs, if and when necessary.
b. AllmembersofNCCA
c. The FDA Director with a copy furnished to the FDA aDSM Focal Point. The Director and/or theFDAFocalPointmayask questions or clarification to theNTPaDSMFocalpointabouttheSAE.
d. The Department of Medical Services
D. The NTP aDSM Focal Point will then schedule and convene a meeting among the Clinical Professors to perform causality assessment on the SAE within 15 days from SAE detection.
E. TheNTPaDSMFocalPointentersthedatatotheNationalaDSMDatabasewithin72hoursassoonasalldetailsareverifiedfromthehospitalorMDR-TBCenter.
F. TheNTPaDSMFocalPoint transmits the data to theGlobal aDSMDatabase [email protected].
G. TheGlobalaDSM teamwillmakeverifications to theNTPaDSMFocalPoint, asneed,andwillenterthedatatotheGlobalDatabase.Feedbackwillbegiventothecountry, after a certain agreed period of time.
H. Two-way communication is maintained between the FDA and the Department ofMedicalServices,andbetweentheNTPandDepartmentofMedicalServices.
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
18
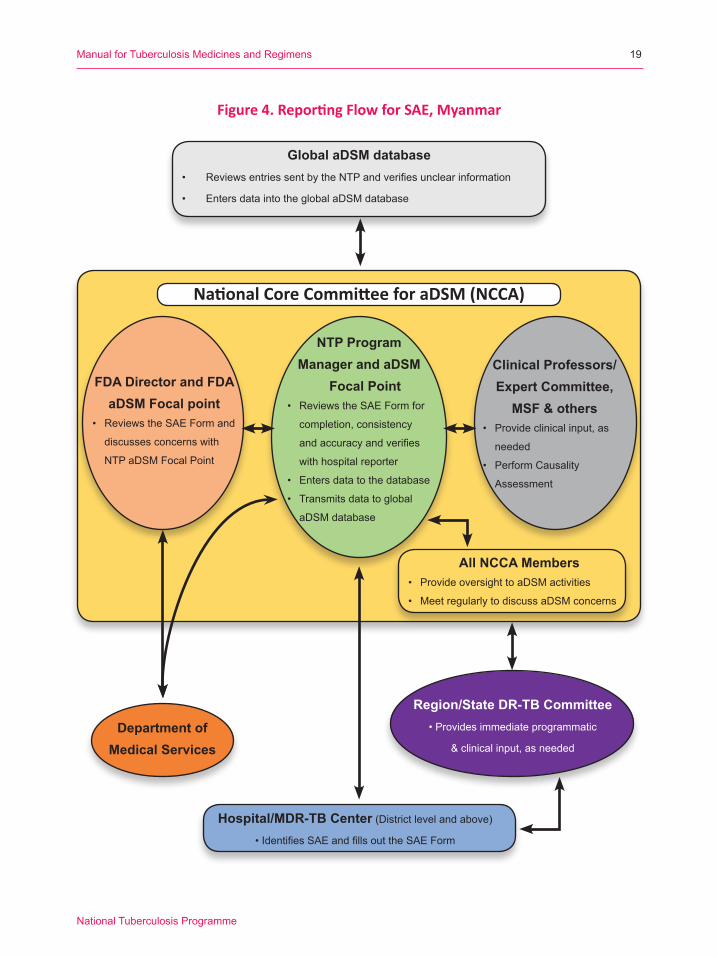
Figure 4. Reporting Flow for SAE, Myanmar
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
19
National Core Committee for aDSM (NCCA)
Global aDSM database• ReviewsentriessentbytheNTPandverifiesunclearinformation
• EntersdataintotheglobalaDSMdatabase
FDA Director and FDA aDSM Focal point
• Reviews the SAE Form and
discusses concerns with
NTP aDSM Focal Point
Department ofMedical Services
Clinical Professors/Expert Committee,
MSF & others• Provide clinical input, as
needed
• Perform Causality
Assessment
Region/State DR-TB Committee• Provides immediate programmatic
& clinical input, as needed
Hospital/MDR-TB Center(Districtlevelandabove)•IdentifiesSAEandfillsouttheSAEForm
NTP ProgramManager and aDSM
Focal Point• Reviews the SAE Form for
completion, consistency
andaccuracyandverifies
with hospital reporter
• Entersdatatothedatabase
• Transmitsdatatoglobal
aDSMdatabase
All NCCA Members• Provide oversight to aDSM activities
• Meet regularly to discuss aDSM concerns
7. Consolidate data electronically
TheClintonHealthAccessInitiative(CHAI)forDR-TBpatients isassistingtheNTPincreatinganationalelectronicdatabaseforDR-TBpatients.TheelementsoftheaDSMdatabaseare tobe incorporated into thisDR-TBDatabase, rather thanbedevelopedindependentlyasaseparateone.ThecreationoftheelectronicaDSMdatabaseshouldnotduplicatetheworkbeingdonefortheexistingdatabases,andshouldbeinteroperablewiththeexistingdatamanagementsystem.TheelectronicaDSMdatabasewillensurestandardizationandsafekeepingofdata.
Thepaper-basedSAEForm received by theNTP should be entered regularly to theNational Database by theNTP Focal Point in a format linkedwith theGlobal aDSMDatabasesharingthesamekeyvariablestofacilitatedatatransmissionandcontributionofthedatafromthecountrytotheGlobalDatabase.
AlistofkeyvariablestobecollectedfortheWHOcentralaDSMdatabaseandadatadictionarymay be found at http://www.who.int/tdr/research/tb_hiv/adsm/en/. It collectsanonymizedindividualpatientdataforallSAEsfromPMDT.WHOandCTBarehelpingfacilitatethelinkbetweenthegroupworkingontheNationalDatabasewiththeGlobalDatabase.
Management of data in electronic form is necessary and will facilitate sharing of data as wellasgenerationofindicatorsandanalysisthatwillbeusefultoassessthecoverageofaDSMactivitiesandtosummarizetheoverallAEexperienceofmonitoredpatients.
8. Develop capacity for signal detection and causality assessment
TheultimatepurposeofsystematicdatacollectionwithinaDSMis toenablecausalityassessment for the SAEs, determine the frequency and rates of occurrence and detect signals.ClinicalexpertsinM/XDR-TBmanagementmayattempttoestablishrelationshipsbetween drugs andADRs; however, performing causality assessment is a separateprocess requiring expertise. The physicians involved in M/XDR care will undergo training on causality assessmentwhichwill enable them to conduct causality assessment foreverySAEreported.Signaldetectionwillbeafunctionthatwillberequestedfromexternalexperts.
ROLES AND RESPONSIBILITIESThe roles and responsibilities in aDSM focus on key stakeholders involved in the clinicalmanagementandpublichealthmanagement forDR-TBpatientsat thenational, regionalandhospitallevels.ThesearediscussedinStep#2aboveandsummarizedinthenext2tables.
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
20
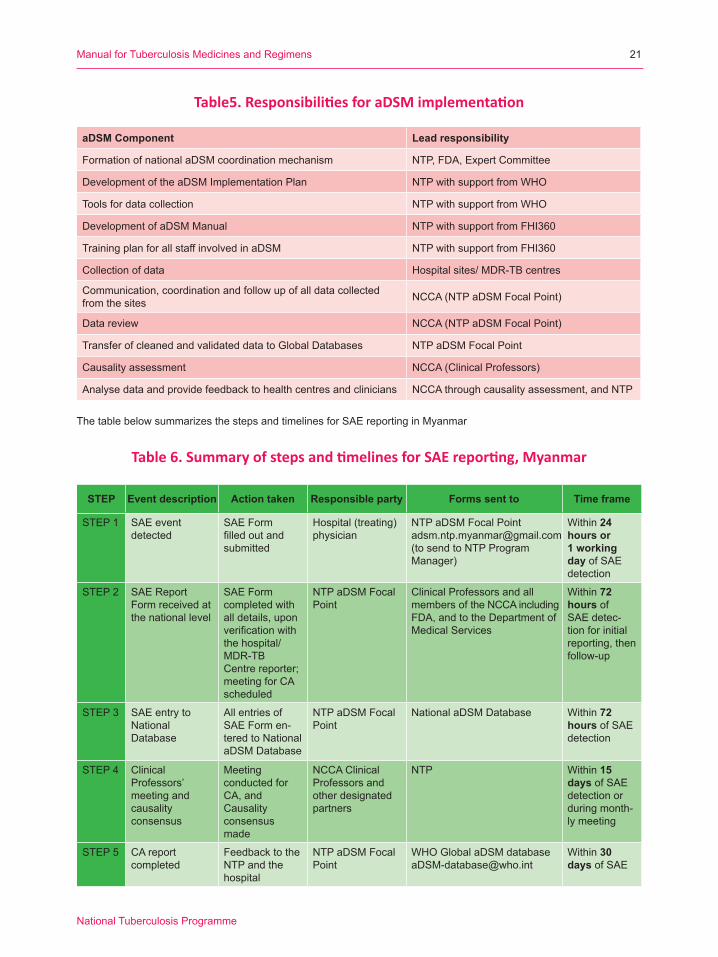
aDSM Component Lead responsibility
Formation of national aDSM coordination mechanism NTP, FDA, Expert Committee
Development of the aDSM Implementation Plan NTP with support from WHO
Tools for data collection NTP with support from WHO
Development of aDSM Manual NTP with support from FHI360
Training plan for all staff involved in aDSM NTP with support from FHI360
Collection of data Hospital sites/ MDR-TB centres
Communication, coordination and follow up of all data collected from the sites NCCA(NTPaDSMFocalPoint)
Data review NCCA(NTPaDSMFocalPoint)
TransferofcleanedandvalidateddatatoGlobalDatabases NTP aDSM Focal Point
Causality assessment NCCA(ClinicalProfessors)
Analysedataandprovidefeedbacktohealthcentresandclinicians NCCA through causality assessment, and NTP
Table5. Responsibilities for aDSM implementation
ThetablebelowsummarizesthestepsandtimelinesforSAEreportinginMyanmar
Table 6. Summary of steps and timelines for SAE reporting, Myanmar
STEP Event description Action taken Responsible party Forms sent to Time frame
STEP 1 SAE event detected
SAE Form filledoutandsubmitted
Hospital(treating)physician
NTP aDSM Focal Point [email protected](to send to NTP Program Manager)
Within 24 hours or 1 working day of SAE detection
STEP 2 SAE Report Form received at the national level
SAE Form completed with all details, upon verificationwiththe hospital/MDR-TB Centre reporter; meeting for CA scheduled
NTP aDSM Focal Point
Clinical Professors and all membersoftheNCCAincludingFDA, and to the Department of Medical Services
Within 72 hours of SAE detec-tion for initial reporting, then follow-up
STEP 3 SAE entry to National Database
All entries of SAE Form en-tered to National aDSMDatabase
NTP aDSM Focal Point
NationalaDSMDatabase Within 72 hours of SAE detection
STEP 4 Clinical Professors’meeting andcausality consensus
Meeting conducted for CA, and Causality consensus made
NCCA Clinical Professors and other designated partners
NTP Within 15 days of SAE detection or during month-ly meeting
STEP 5 CA reportcompleted
FeedbacktotheNTP and the hospital
NTP aDSM Focal Point
Within 30 days of SAE
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
21

CAUSALITY ASSESSMENTCausality assessment (CA) is an integral part of clinical management. In TB, evaluating thelikelihoodthataTBmedicinewasthecausativeagentofanobservedadversereactionformspart of clinical evaluation. While the details of the systematic method of conducting CA may not befamiliartothepractitioner,theoverallapproachisnottoodifferentfromtheclinicalpracticefollowed when evaluating any patient on treatment.16
CAinvolvesmakinganattributionordescribingtherelationshipbetweentheAEandanexposurebyaphysicianoranyotherhealthcareprofessionalwiththerightexpertisewhichformspartofclinicalmonitoringandmanagement.Thisdeterminationmustberecordedbothinthepatient’smedicalrecordaswellasinacasereportform.ForaDSM,CAshouldbemadeprimarilyatthecountry levelandbyconsulting the relevantdatasourcesclose towhere theeventoccurred.AttributingarelationshiprequiresasystematicprocessandisoneofthemainreasonswhydataarecollectedinaDSM.CAoncedoneattributesalevelofcertaintybetweentheeventandtheexposure, ranging from certain to unrelated.
CAisconductedbytheClinicalprofessorsoftheNCCA,whoalsocomprisetheNationalDR-TBExpertCommittee,withtheparticipationofotherdesignatedmembers.CAshouldbeconductedusing a systematic tool provided later in this section, involving inputs from the panel of experts beyondthetreatingphysician.ThestepsindoingCAareasfollows:
- The hospital site provides all details relevant to the SAE to the national level (within 24 hourstotheNTPandFDAaDSMfocalpoints)
- The hospital site will forward all other details to the NTP aDSM Focal Point (within 72 hoursfromSAEdetection)intheCaseSummarysectionoftheSAEForm,includingthefollowingkeydataelements:
a) medicalhistory(includingconcomitantdisease),
b) otherriskfactors(socialfactors,alcoholuse,substanceabuse,etc.),
c) detailsofdrugstaken:names,doses,routes,
d) startandstopdatesandindicationsforuse,
e) descriptionofadverseevent,includingclinicaldescription,baseline,monthlyandadhoclaboratoryresults,anddateofonset/endand
f) evolutionofevent,severity,seriousness,andoutcome.
- The NTP aDSM Focal Point forwards the completed SAE Form to the Clinical Professors andallwhoareinvolvedinCA,andotherNCCAmembers
16aDSMtrainingpackage(trainingslidespreparedbyKNCVTuberculosisFoundation,ManagementSciencesforHealth(SIAPS),MédecinssansFrontières,WorldHealthOrganization/GlobalTBProgrammeSpecialProgrammeforResearchandTraininginTropicalDiseases(TDR)atWHOHeadquarters,July2016http://www.who.int/tdr/research/tb_hiv/adsm/training_adsm/en/((accessedon2Feb2017)
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
22
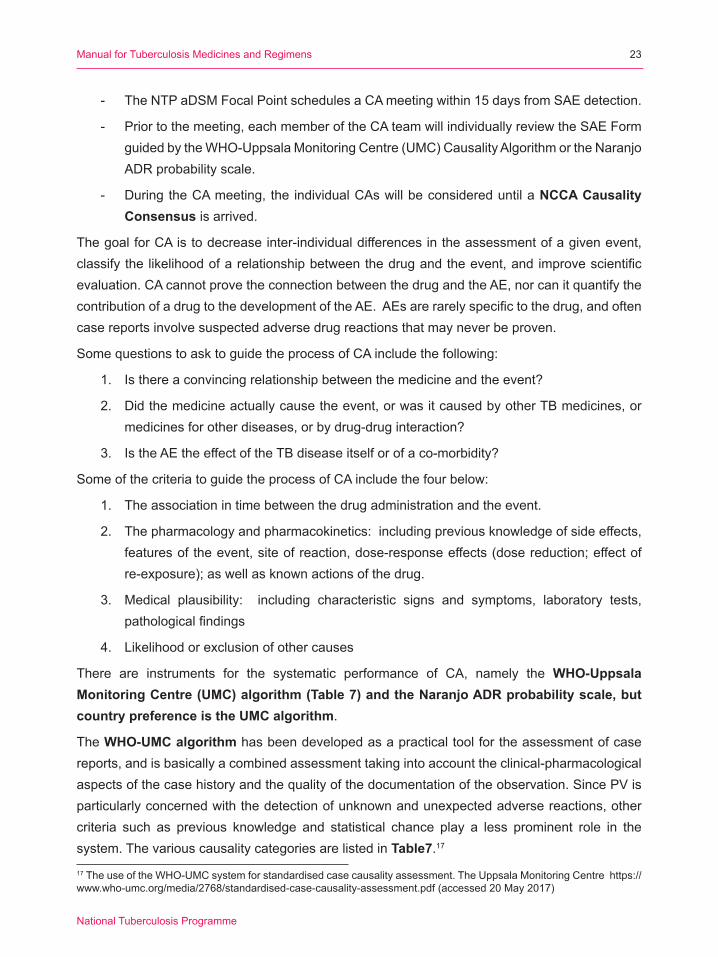
- The NTP aDSM Focal Point schedules a CA meeting within 15 days from SAE detection.
- Priortothemeeting,eachmemberoftheCAteamwillindividuallyreviewtheSAEFormguidedbytheWHO-UppsalaMonitoringCentre(UMC)CausalityAlgorithmortheNaranjoADRprobabilityscale.
- DuringtheCAmeeting, the individualCAswillbeconsidereduntilaNCCA Causality Consensus is arrived.
The goal for CA is to decrease inter-individual differences in the assessment of a given event, classifythelikelihoodofarelationshipbetweenthedrugandtheevent,andimprovescientificevaluation.CAcannotprovetheconnectionbetweenthedrugandtheAE,norcanitquantifythecontributionofadrugtothedevelopmentoftheAE.AEsarerarelyspecifictothedrug,andoftencasereportsinvolvesuspectedadversedrugreactionsthatmayneverbeproven.
SomequestionstoasktoguidetheprocessofCAincludethefollowing:
1. Isthereaconvincingrelationshipbetweenthemedicineandtheevent?
2. Didthemedicineactuallycausetheevent,orwasitcausedbyotherTBmedicines,ormedicinesforotherdiseases,orbydrug-druginteraction?
3. IstheAEtheeffectoftheTBdiseaseitselforofaco-morbidity?
SomeofthecriteriatoguidetheprocessofCAincludethefourbelow:
1. Theassociationintimebetweenthedrugadministrationandtheevent.
2. Thepharmacologyandpharmacokinetics:includingpreviousknowledgeofsideeffects,features of the event, site of reaction, dose-response effects (dose reduction; effect of re-exposure);aswellasknownactionsofthedrug.
3. Medical plausibility: including characteristic signs and symptoms, laboratory tests,pathologicalfindings
4. Likelihood or exclusion of other causes
There are instruments for the systematic performance of CA, namely the WHO-Uppsala Monitoring Centre (UMC) algorithm (Table 7) and the Naranjo ADR probability scale, but country preference is the UMC algorithm.
The WHO-UMC algorithmhasbeendevelopedasapracticaltoolfortheassessmentofcasereports,andisbasicallyacombinedassessmenttakingintoaccounttheclinical-pharmacologicalaspectsofthecasehistoryandthequalityofthedocumentationoftheobservation.SincePVisparticularly concerned with the detection of unknown and unexpected adverse reactions, other criteria such as previous knowledge and statistical chance play a less prominent role in the system. The various causality categories are listed in Table7.17
17TheuseoftheWHO-UMCsystemforstandardisedcasecausalityassessment.TheUppsalaMonitoringCentrehttps://www.who-umc.org/media/2768/standardised-case-causality-assessment.pdf(accessed20May2017)
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
23

Tabl
e 7.
The
WHO
-UM
C Cl
assi
ficati
on S
yste
m fo
r cau
salit
y as
sess
men
t
Cau
salit
y te
rmD
efini
tion
Ass
essm
ent c
riter
ia*
Cer
tain
Cle
arly
cau
sed
by th
e ex
posu
reTh
ere
is c
lear
evi
denc
e to
sug
gest
a c
ausa
l rel
atio
nshi
p an
d ot
her p
ossi
ble
cont
ribut
ing
fact
ors
can
be ru
led
out.
• • • • •
Eventorlaboratorytestabnormality,w
ithp
laus
ible
tim
e re
latio
nshi
p to
dru
g in
take
Can
notbeexplainedbydiseaseorotherdrugs
Res
pons
e to
with
draw
al p
laus
ible
(pha
rmac
olog
ical
ly, p
atho
logi
cally
)Eventdefinitivepharmacologicallyorphenomenologically(i.e.,anobjective
andspecificmedicaldisorderorarecognizedpharmacologicalphenomenon)
Re-
chal
leng
e sa
tisfa
ctor
y, if
nec
essa
ry
Probable/Likely
Like
ly to
be
rela
ted
to th
e ex
posu
re
Ther
e is
evi
denc
e to
sug
gest
a li
kely
cau
sal r
elat
ions
hip
and
the
influ
ence
of o
ther
fact
ors
is u
nlik
ely.
• • • •
Eventorlaboratorytestabnormality,w
ith re
ason
able
tim
e re
latio
nshi
p to
dr
ug in
take
Unl
ikel
ytobeattributedtodiseaseorotherdrugs
Res
pons
e to
with
draw
al c
linic
ally
reas
onab
leR
e-ch
alle
nge
not r
equi
red
Possible
May
be
rela
ted
to th
e ex
posu
re
Ther
e is
som
e ev
iden
ce to
sug
gest
a c
ausa
l rel
atio
nshi
p (e
.g.
beca
use
the
even
t occ
urs
with
in a
reas
onab
le ti
me
afte
r adm
in-
istra
tion
of th
e tri
al m
edic
atio
n).
How
ever
, the
influ
ence
of o
ther
fa
ctor
s m
ay h
ave
cont
ribut
ed to
the
even
t (e.
g. th
e pa
tient
’s
clin
ical
con
ditio
n, o
ther
con
com
itant
trea
tmen
ts).
• • •
Eventorlaboratorytestabnormality,w
ithre
ason
able
tim
e re
latio
nshi
p to
dr
ug in
take
Couldalsobeexplainedbydiseaseorotherdrugs
Informationondrugwithdraw
almaybelackingorunclear
Unl
ikel
yD
oubt
fully
rela
ted
to th
e ex
posu
re
Ther
e is
littl
e ev
iden
ce to
sug
gest
ther
e is
a c
ausa
l rel
atio
nshi
p (e
.g. t
he e
vent
did
not
occ
ur w
ithin
a re
ason
able
tim
e af
ter a
d-m
inis
tratio
n of
the
stud
y re
gim
en).
Ther
e is
ano
ther
reas
onab
le
expl
anat
ion
for t
he e
vent
(e.g
. the
pat
ient
’s c
linic
al c
ondi
tion,
ot
her c
onco
mita
nt tr
eatm
ent).
• •
Eventorlaboratorytestabnormality,w
ith a
tim
e to
dru
g in
take
that
mak
es
a re
latio
nshi
p im
prob
able(butnotim
possible)
Dis
ease
or o
ther
dru
gs p
rovi
de p
laus
ible
exp
lana
tions
Con
ditio
nal o
r Unclassified
Ther
e is
insu
ffici
ent i
nfor
mat
ionabouttheADRstoallowfor
an a
sses
smen
t of c
ausa
lity.
• • •
Eventorlaboratorytestabnormality
Mor
e da
ta fo
r pro
per a
sses
smen
t nee
ded,
or
Add
ition
al d
ata
unde
r exa
min
atio
n
Unassessable
orUnclassifiable
ThereisinsufficientinformationabouttheADRstoallowforan
asse
ssm
ent o
f cau
salit
y an
d N
O M
OR
E is
exp
ecte
d.• • •
Rep
ort s
ugge
stin
g an
adv
erse
reac
tion
Cannotbejudgedbecauseinformationisinsufficientorcontradictory
Datacannotbesupplementedorverified
*Allpointsshouldbereasonablycom
pliedwith
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
24

SIGNAL DETECTIONAsignal isa reported informationonapossiblecausal relationshipbetweenanAEandaTBmedicine. Either the relationship was previously unknown or incompletely documented (e.g. a newaspectofaknownassociation)
Signal detection is an important process to improve knowledge on the new TB medicines and complete the safety profile of a new drug.WhenmonitoringAEs, it is important to lookbeyondalreadyknownadversereactionsandbiologicalpathways.Previouslyunknownorrareassociationsmayoccur,especiallyfornewandrepurposeddrugs.ReportsofAEstotheglobalaDSMDatabaseisexpectedtoimprovethelikelihoodofpickingupmoresignals.
Asignalisworthinvestigatingwhenthedataqualityisreliable,severalreportsshowacredibleand strong relationship betweenevent and drug, and the event is of sufficient importance orinterest (either to require regulatory action, to require advice to prescribers, or for scientific /clinicalpurposes).
Thefeaturesofasignalincludethefollowing:a)usually>1eventwithasimilar,strongrelationshiptoamedicine(“certain”or“probable“).Eventscodedas“possible”canbeusedassupportingevidence;b)aclusterofunexpecteddeathscodedas“possible”formsanexceptiontothegeneralruleandwillneedtobetakenseriously;c)occasionally,asingleevent(“certain”or“probable”)-notableforitsseverity,seriousnessordistinctiveness.
Signaldetectioncanaddknowledgetothedrugsafetyprofileofanagentwhichdescribesthebenefits,risksandtoxicityofagivenTBdrugorregimen,specifyinganyknownorlikelysafetyconcerns, contraindications, cautions, preventive measures and other features that the user shouldbeawareoftoprotectthehealthofaTBpatient.
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
25

ANNEXES
AnnexA Clinical, bacteriological and laboratorymonitoring duringMDR-TB treatmentRR-/MDR-TB patients
Annex B Programmatic indicators of aDSM
AnnexC MDR-TBTreatmentCard(DR-TBForm01)modifications
AnnexD NTPFormforReportingSeriousAdverseEvent(SAE)
Annex E Severity Grading Scales and suggested action of selected common AEs
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
26
ANN
EX A
–M
onito
ring
sche
dule
(Clin
ical
, bac
terio
logi
cal a
nd la
bora
tory
) dur
ing
M-/
XDR-
TB tr
eatm
ent o
n ne
w a
nd
repu
rpos
ed d
rugs
and
the
shor
ter r
egim
en18
Eval
uatio
n/Te
stB
asel
ine
Inte
nsiv
e ph
ase
(IP)
Con
tinua
tion
phas
e (C
P)Fo
llow
-up
afte
r tre
atm
ent
com
plet
ion
for 2
yea
rs
C L I N I C A L
Clin
ical
eva
luat
ion
(sym
ptom
s,
sideeffects&PE)
√DailyateveryDOTencounter;monthlybyMDRphysician
Mon
thly
M
onth
s 3,
6 &
12,
and
as
need
ed
Wei
ght
√M
onth
ly
Mon
thly
M
onth
s 6
& 1
2
Aud
iom
etry
√Monthlywhileoninjectable
Monthlywhileoninjectable;3&6
monthpost-injectable
No
need
Visual(S
nellen’sandIshihara
chart)
If on
long
-term
E a
nd/
orLzd
Whe
n in
dica
ted
Whe
n in
dica
ted
No
need
12-le
ad E
CG
√
Wee
k 2,
4, th
en m
onth
ly, a
nd a
d ho
c1M
onth
ly, a
nd a
d ho
c if
on B
dq o
r Dlm,MfxandCfz
1
No
need
Note:SpecialattentioninpatientsreceivingmorethanoneQTprolongingdrugs(B
dq,D
lm,M
fx,
Lfx,Cfz)orw
ithlowalbum
in(<
3,4g/dl)
Che
st X
-ray
√
Eve
ry 6
mon
th, a
nd a
d ho
cE
very
6 m
onth
, and
ad
hoc
Mon
ths
6 &
12,
and
as
clin
ical
ly in
dica
ted
B A C T E R I O L O G I C
Sm
ear
√M
onth
ly
Mon
ths
6 &
12
Cul
ture
√M
onth
ly
Mon
ths
6 &
12
Xpe
rt® M
TB/R
if√
If cl
inic
ally
indi
cate
d
SL-
LPA
√Incaseof+cultureafterconversion,andbaselineshow
ednoresistancetoFQandSLI
Whe
n cu
lture
+ a
nd R
R-T
B
byXpertorMDR-TBby
DS
T
DS
T (H
, R, M
fx, L
fx, K
m, A
m,
Cm),ifculturepositive
√Incaseof+culturebymonth3oftreatment,orreversion
In c
ase
of re
vers
ion
Whe
n cu
lture
+
18 G
ener
ic p
rogr
amm
atic
and
clin
ical
gui
de fo
r th
e in
trodu
ctio
n of
new
dru
gs a
nd s
horte
r re
gim
ens
for
the
treat
men
t of
multi-/extensivelydrug-resistanttuberculosis,ver0.19,20Feb2017(U
SAID,K
NCV,ChallengeTB
)
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
27
Eval
uatio
n/Te
stB
asel
ine
Inte
nsiv
e ph
ase
(IP)
Con
tinua
tion
phas
e (C
P)Fo
llow
-up
afte
r tre
atm
ent
com
plet
ion
for 2
yea
rs
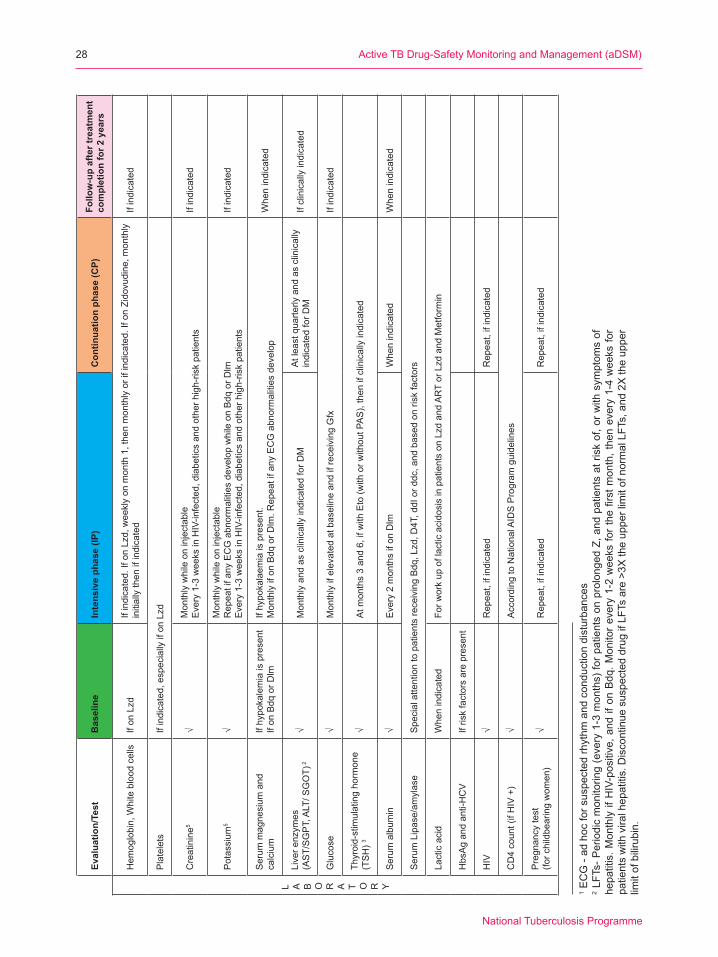
L A B O R A T O R Y
Hem
oglobin,W
hitebloodcells
IfonLzd
Ifindicated.IfonLzd,weeklyonmonth1,thenmonthlyorifindicated.IfonZidovudine,m
onthly
initi
ally
then
if in
dica
ted
If in
dica
ted
Pla
tele
tsIfindicated,especiallyifonLzd
Cre
atin
ine5
√Monthlywhileoninjectable
Every1-3weeksinHIV-infected,diabeticsandotherhigh-riskpatients
If in
dica
ted
Pot
assi
um5
√Monthlywhileoninjectable
RepeatifanyECGabnormalitiesdevelopwhileonBdqorD
lmEvery1-3weeksinHIV-infected,diabeticsandotherhigh-riskpatients
If in
dica
ted
Ser
um m
agne
sium
and
ca
lciu
m
If hy
poka
lem
ia is
pre
sent
If on
Bdq
or D
lmIf
hypo
kala
emia
is p
rese
nt.
MonthlyifonBdqorD
lm.R
epeatifanyECGabnormalitiesdevelop
Whe
n in
dica
ted
Liverenzym
es(AST/SGPT,ALT/S
GOT)
2√
Mon
thly
and
as
clin
ical
ly in
dica
ted
for D
MA
t lea
st q
uarte
rly a
nd a
s cl
inic
ally
in
dica
ted
for D
M
If cl
inic
ally
indi
cate
d
Glu
cose
√
MonthlyifelevatedatbaselineandifreceivingGfx
If in
dica
ted
Thyr
oid-
stim
ulat
ing
horm
one
(TSH)3
√Atm
onths3and6,ifwithEto(w
ithorw
ithoutPAS),thenifclinicallyindicated
Serum
album
in
√E
very
2 m
onth
s if
on D
lmW
hen
indi
cate
dW
hen
indi
cate
d
Ser
um L
ipas
e/am
ylas
eSpecialattentiontopatientsreceivingBdq,Lzd,D
4T,ddIorddc,andbasedonriskfactors
Lact
ic a
cid
Whe
n in
dica
ted
Forw
orkupoflacticacidosisinpatientsonLzdandARTorLzdandMetformin
HbsAgandanti-HCV
If ris
k fa
ctor
s ar
e pr
esen
t
HIV
√R
epea
t, if
indi
cate
dR
epea
t, if
indi
cate
d
CD4count(ifHIV+)
√A
ccor
ding
to N
atio
nal A
IDS
Pro
gram
gui
delin
es
Pre
gnan
cy te
st
(forchildbearingwom
en)
√R
epea
t, if
indi
cate
dR
epea
t, if
indi
cate
d
1 ECG-adhocforsuspectedrhythm
andconductiondisturbances
2 LFTs-Periodicmonitoring(every1-3months)forp
atientsonprolongedZ,andpatientsatriskof,orwithsym
ptom
sof
hepatitis.M
onthlyifHIV-positive,a
ndifonBdq.M
onitorevery1-2weeksfo
rthefirstm
onth,thenevery1-4weeksfo
rpa
tient
s w
ith v
iral h
epat
itis.
Dis
cont
inue
sus
pect
ed d
rug
if LF
Ts a
re >
3X th
e up
per l
imit
of n
orm
al L
FTs,
and
2X
the
uppe
r lim
itofbilirubin.
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
28

ANN
EX B
– P
rogr
amm
atic
indi
cato
rs fo
r aDS
M (W
HO G
uide
lines
, 201
4)
CLA
SSIM
POR
-TA
NC
E
IND
ICAT
OR
N
UM
BER
AN
D
NA
ME
CA
LCU
LATI
ON
STR
ATIF
ICAT
ION
EXPR
ESSE
D
AS
DAT
A SO
UR
CES
LEVE
LPE
RIO
D O
F A
SSES
SMEN
TN
OTE
S
Cov
erag
e(process)
Ess
entia
l1)TargetR
R/
MD
R-T
B p
atie
nts
incl
uded
in c
ohor
t ev
ent m
onito
ring
Num
berator:Num
ber
of T
B c
ases
sta
rted
on ta
rget
trea
tmen
t in
clud
ed in
aD
SM
du
ring
the
perio
d of
as
sess
men
t.Denom
inator:N
umber
of T
B c
ases
sta
rted
on ta
rget
trea
tmen
t du
ring
the
perio
d of
as
sess
men
t and
who
wereeligiblefora
aDS
M.
Non
eAbsolute
numbers,
prop
ortio
n
Num
berator:
aDS
M re
gist
er.
Denom
inator:
Sec
ond-
line
TB tr
eatm
ent
regi
ster
.
National:NTP
an
d na
tiona
l ph
arm
a co
vigi
lanc
e centre(N
PV)
3 m
onth
sTobecomputed
durin
ng th
e pe
riod
of
recr
uitm
ent
butnotinthe
post
-trea
tmen
t observation
phas
e
Com
plet
enes
s (process)
Opt
iona
l2)Timeto
stop
ping
targ
et
drug
The
diffe
rent
in d
ays
betweenthedateof
star
t of t
reat
men
t with
a
targ
et d
rug
and
the
date
of t
he s
topp
ing
the
targ
et d
rug.
The
ca
lcul
atio
n is
don
e fo
r eachmem
berofthe
coho
rt.
Rea
son
for
stop
ping
Num
ber
of p
atie
nts
incl
uded
in th
e ca
lcul
atio
n;
med
ian
inte
rval
and
in
terq
uarti
le
rang
e in
day
s
aDS
M re
gist
erNational:NTP
&
NP
V12
mon
ths
Stratifyby
reas
on fo
r st
oppi
ng (e
.g.
succ
ess,
die
d,
treat
men
t fai
led,
lo
ss to
follo
w
up, e
xclu
sion
cr
iterio
n de
velo
ping
af
ter s
tart
of
treat
men
t suc
h aspregnancy).
Ser
ious
ad
vers
e ev
ents
Ess
entia
l (but
Stratifica-
tion
optitonal)
3)RR-/M
DR-TB
patie
nts
incl
uded
in
aD
SM
with
any
se
rious
adv
erse
ev
ent
Num
berator:Num
ber
of T
B c
ases
incl
uded
in
aD
SM
dur
ing
the
perio
d of
ass
essm
ent
with
one
or m
ore
serio
us a
dver
se
even
ts.
Denom
inator:N
umber
of T
B c
ases
incl
uded
in
aD
SM
dur
ing
the
perio
d of
ass
essm
ent.
By
orga
n gr
oup;
byoutcome
Absolute
numbers,
prop
ortio
n
Num
berator:
aDS
M re
gist
er.
Denom
inator:
aDS
M re
gist
er.
NTP
& N
PV
3 m
onth
sTobecomputed
durin
g th
e pe
riod
of p
atie
nt
recr
uitm
ent
and
durin
g th
e po
st tr
eatm
ent
observation
phas
e. In
dica
te
outc
ome
(dea
ths,
ho
spita
lisat
ions
, disability)
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
29
CLA
SSIM
POR
-TA
NC
E
IND
ICAT
OR
N
UM
BER
AN
D
NA
ME
CA
LCU
LATI
ON
STR
ATIF
ICAT
ION
EXPR
ESSE
D
AS
DAT
A SO
UR
CES
LEVE
LPE
RIO
D O
F A
SSES
SMEN
TN
OTE
S
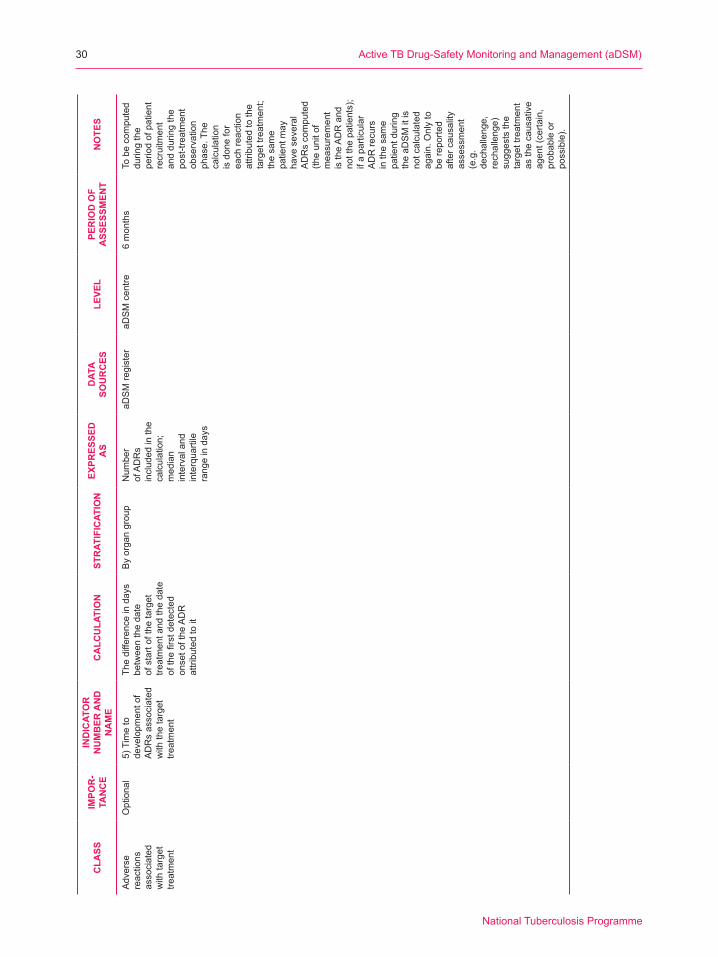
Adv
erse
re
actio
ns
asso
ciat
ed
with
targ
et
treat
men
t
Opt
iona
l5)Timeto
deve
lopm
ent o
f A
DR
s as
soci
ated
w
ith th
e ta
rget
tre
atm
ent
The
diffe
renc
e in
day
s betweenthedate
of s
tart
of th
e ta
rget
tre
atm
ent a
nd th
e da
te
ofthefirstdetected
onse
t of t
he A
DR
attributedtoit
By
orga
n gr
oup
Num
ber
of A
DR
s in
clud
ed in
the
calc
ulat
ion;
m
edia
n in
terv
al a
nd
inte
rqua
rtile
ra
nge
in d
ays
aDS
M re
gist
eraD
SM
cen
tre6
mon
ths
Tobecomputed
durin
g th
e pe
riod
of p
atie
nt
recr
uitm
ent
and
durin
g th
e po
st-tr
eatm
ent
observation
phas
e. T
he
calc
ulat
ion
is d
one
for
each
reac
tion
attributedtothe
targ
et tr
eatm
ent;
the
sam
e pa
tient
may
ha
ve s
ever
al
AD
Rs
com
pute
d (th
e un
it of
m
easu
rem
ent
is th
e A
DR
and
notthepatients);
if a
parti
cula
r A
DR
recu
rs
in th
e sa
me
patie
nt d
urin
g th
e aD
SM
it is
no
t cal
cula
ted
agai
n. O
nly
to
bereported
afte
r cau
salit
y as
sess
men
t (e
.g.
dech
alle
nge,
rechallenge)
sugg
ests
the
targ
et tr
eatm
ent
as th
e ca
usat
ive
agen
t (ce
rtain
, probableor
possible).
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
30
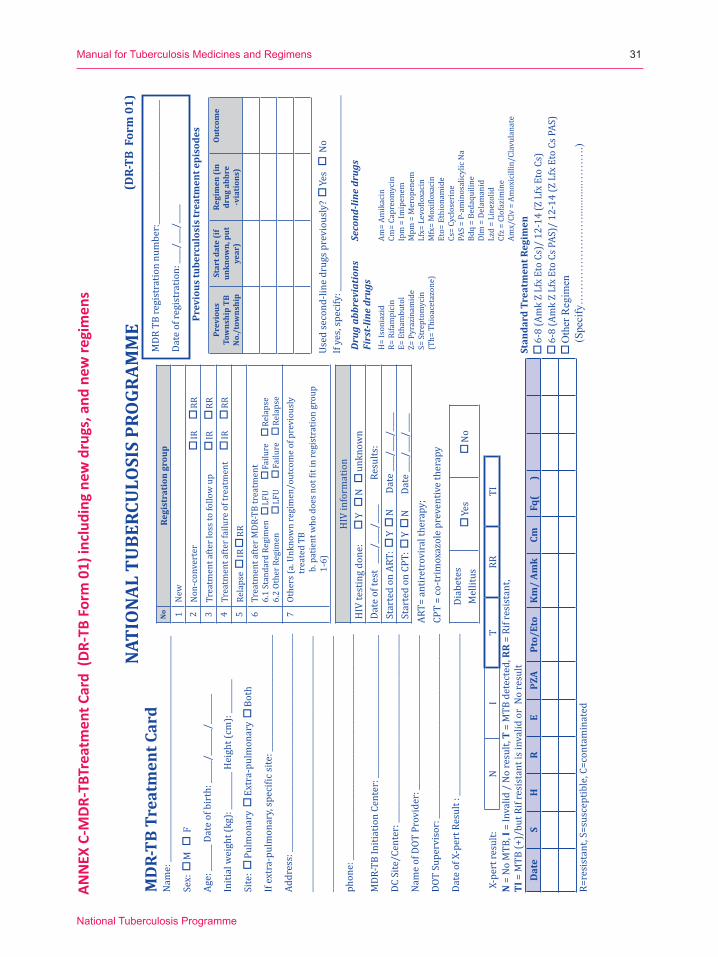
ANN
EX C
-MDR
-TBT
reat
men
t Car
d (D
R-TB
For
m 0
1) in
clud
ing
new
dru
gs, a
nd n
ew re
gim
ens
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
31
Nam
e: __
____
____
____
____
____
____
____
____
____
____
____
____
____
____
__
Sex:
M
F
Age:
____
___ D
ate
of b
irth
: ___
___/
____
___/
____
____
Initi
al w
eigh
t (kg
): __
____
____
Hei
ght (
cm):
____
____
_
Site
: P
ulm
onar
y
Ext
ra-p
ulm
onar
y
Bot
h
If ex
tra-
pulm
onar
y, sp
ecifi
c site
: ___
____
____
____
____
____
____
____
Addr
ess:
____
____
____
____
____
____
____
____
____
____
____
____
____
____
__
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
phon
e: __
____
____
____
____
____
____
____
____
____
____
____
____
____
____
__
MDR
-TB
Initi
atio
n Ce
nter
: ___
____
____
____
____
____
____
____
____
___
DC S
ite/C
ente
r: __
____
____
____
____
____
____
____
____
____
____
____
____
Nam
e of
DOT
Pro
vide
r: __
____
____
____
____
____
____
____
____
____
___
DOT
Supe
rvis
or: _
____
____
____
____
____
____
____
____
____
____
____
____
Date
of X
-per
t Res
ult :
____
____
____
____
____
____
____
____
____
____
___
No
Regi
stra
tion
gro
up1
New
2N
on-c
onve
rter
IR
R
R3
Trea
tmen
t afte
r los
s to
follo
w u
p
IR
R
R4
Trea
tmen
t afte
r fai
lure
of t
reat
men
t
IR
R
R5
Rela
pse
IR
R
R6
Trea
tmen
t afte
r MDR
-TB
trea
tmen
t6.
1 St
anda
rd R
egim
en
LFU
Fai
lure
R
elap
se6.
2 Ot
her R
egim
en
LFU
Fai
lure
R
elap
se7
Othe
rs (a
. Unk
now
n re
gim
en/o
utco
me
of p
revi
ousl
y tr
eate
d TB
b
. pat
ient
who
doe
s not
fit i
n re
gist
ratio
n gr
oup
1-6)
MD
R-TB
Tre
atm
ent C
ard
(DR-
TB F
orm
01)
Prev
ious
tube
rcul
osis
trea
tmen
t epi
sode
s
Prev
ious
Tow
nshi
p TB
N
o./t
owns
hip
Star
t dat
e (i
f un
know
n, p
ut
year
)
Regi
men
(in
drug
abb
re
-via
tion
s)
Out
com
e
Used
seco
nd-li
ne d
rugs
pre
viou
sly?
Y
es
No
If ye
s, sp
ecify
: ___
____
____
____
____
____
____
____
____
____
____
____
____
_
Dru
g ab
brev
iatio
nsFi
rst-
line
drug
sSe
cond
-line
dru
gs
H=
Ison
iazi
dR=
Rifa
mpi
cin
E= E
tham
buto
lZ=
Pyr
azin
amid
eS=
Str
epto
myc
in(T
h= T
hioa
ceta
zone
)
Am=
Amik
acin
Cm=
Capr
eom
ycin
Ipm
= Im
ipen
emM
pm =
Mer
open
emLf
x= L
evof
loxa
cin
Mfx
= M
oxifl
oxac
inEt
o= E
thio
nam
ide
Cs=
Cycl
oser
ine
PAS
= P-
amin
osal
icyl
ic N
aBd
q =
Beda
quili
ne
Dlm
= D
elam
anid
Lz
d =
Line
zolid
Cf
z =
Clof
azim
ine
Amx/
Clv
= Am
oxic
illin
/Cla
vula
nate
Stan
dard
Tre
atm
ent R
egim
en 6
-8 (A
mk
Z Lf
x Et
o Cs
)/ 1
2-14
(Z L
fx E
to C
s) 6
-8 (A
mk
Z Lf
x Et
o Cs
PAS
)/ 1
2-14
(Z L
fx E
to C
s PAS
) O
ther
Reg
imen
(Spe
cify
……
……
……
……
......
......
……
….)
X-pe
rt re
sult:
NI
TRR
TIN
= N
o M
TB, I
= In
valid
/ N
o re
sult,
T =
MTB
det
ecte
d, R
R =
Rif r
esis
tant
,TI
= M
TB (+
)/bu
t Rif
resi
stan
t is i
nval
id o
r N
o re
sult
Dat
eS
HR
EPZ
APt
o/Et
oK
m/
Amk
CmFq
(
)
HIV
info
rmat
ion
HIV
test
ing
done
:
Y
N
u
nkno
wn
Date
of t
est
____
/___
_/__
___
Res
ults
:St
arte
d on
ART
: Y
N
D
ate
____
/___
_/__
___
Star
ted
on C
PT:
Y
N
Dat
e __
__/_
___/
____
_AR
T= a
ntir
etro
vira
l the
rapy
; CP
T =
co-t
rim
oxaz
ole
prev
entiv
e th
erap
y
Diab
etes
Mel
litus
Yes
No
NATI
ONA
L TU
BERC
ULO
SIS
PRO
GRAM
ME
MDR
TB
regi
stra
tion
num
ber:
____
____
____
____
____
____
____
____
_
Date
of r
egis
trat
ion:
____
/___
_/__
___
R=re
sist
ant,
S=su
scep
tible
, C=c
onta
min
ated
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
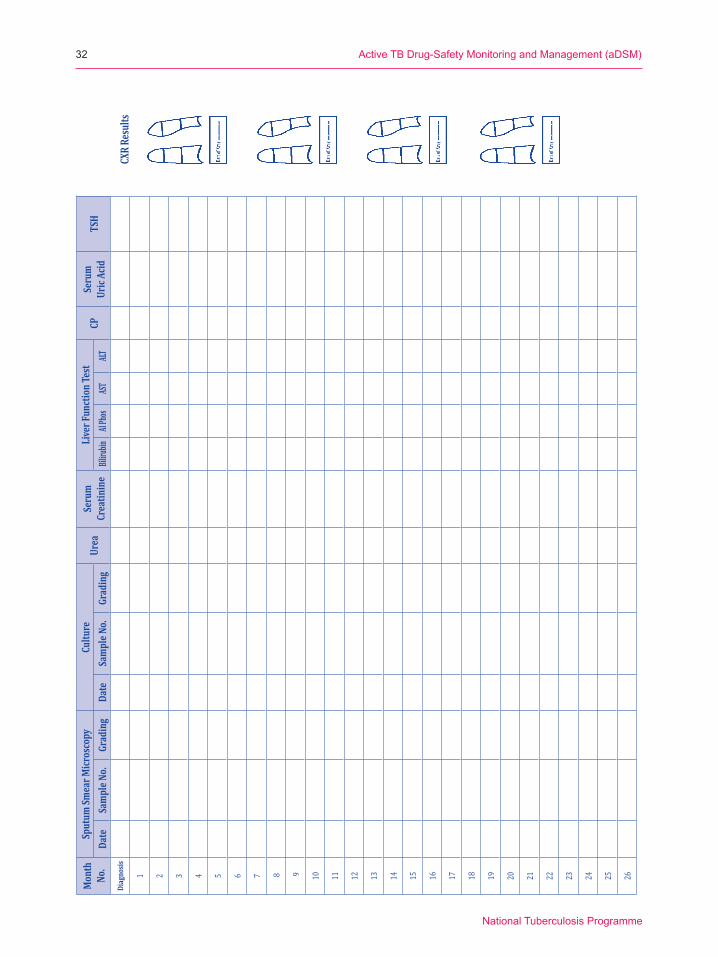
32
Mon
th
No.
Sput
um Sm
ear M
icros
copy
Cultu
reUr
eaSe
rum
Crea
tinin
eLi
ver F
unct
ion T
est
CPSe
rum
Uric
Acid
TSH
Date
Sam
ple N
o.Gr
adin
gDa
teSa
mpl
e No.
Grad
ing
Biliru
binAl
Phos
ASTALT
Diag
nosis
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
CXR
Resu
lts
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
33
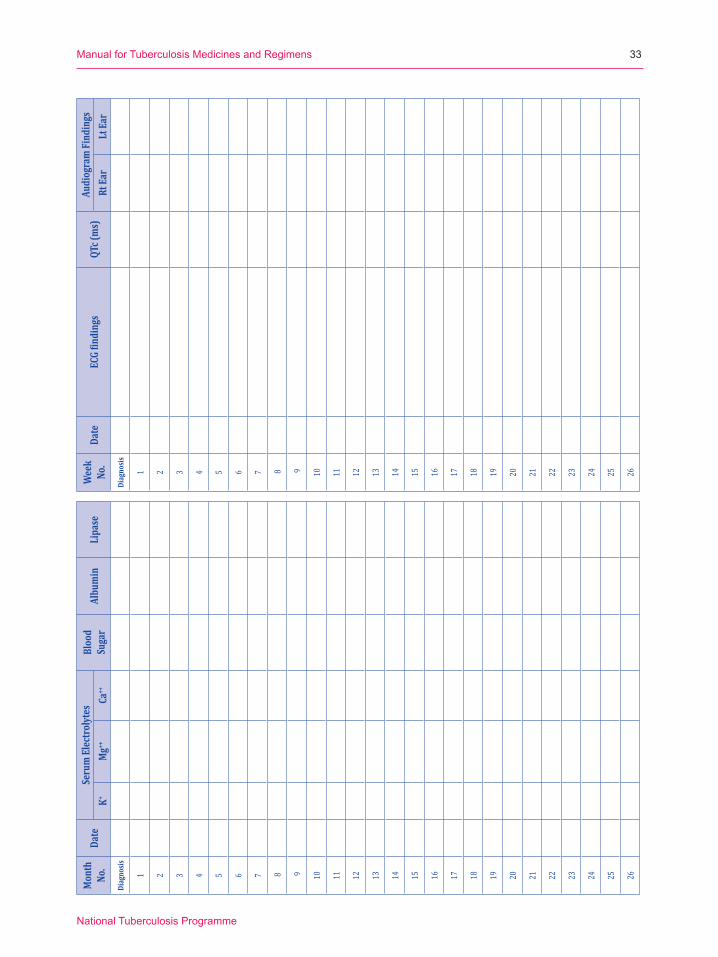
Mon
th
No.
Date
Seru
m El
ectro
lytes
Bloo
d Su
gar
Albu
min
Lipa
seK+
Mg++
Ca++
Diag
nosis
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
Wee
kNo
.Da
teEC
G fin
ding
sQT
c (m
s)Au
diog
ram
Find
ings
Rt Ea
rLt
Ear
Diag
nosis
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26

ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
34
ADM
INIS
TRAT
ION
OF D
RUGS
(one
line
per
mon
th):
Mth No
.m
m-y
yDa
ysW
eigh
t(k
g)1
23
45
67
89
1011
1213
1415
1617
1819
2021
2223
2425
2627
2829
3031
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
Mar
k in t
he bo
xes:
√ = d
irectl
y obs
erve
d, N
= no
t sup
ervis
ed, Ø
= dr
ugs n
ot ta
ken

ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
35
MDR-T
B RE
GIME
N (d
ate tr
eatm
ent s
tarted
and d
osag
e (mg
), fre
quen
cy of
dose
, cha
nge o
f dos
age,
and c
essa
tion o
f dru
gs):
Da
teH
ZE
S/Am
/Cm
FQ(
)Et
oCs
Lzd
Cfz
Bdq
Dlm
PAS
Imp/
Mpm
Amx/
Clv
Com
men
ts,SA
E (Y/
N)
(od =
Onc
e a da
y, bd
= 12
hour
ly: m
ornin
g and
even
ing do
ses)
DR-T
B Co
mm
ittee
/ Pan
el Di
scus
sion a
nd D
ecisi
ons
Date
Issue
s and
Disc
ussio
nDe
cisio
n
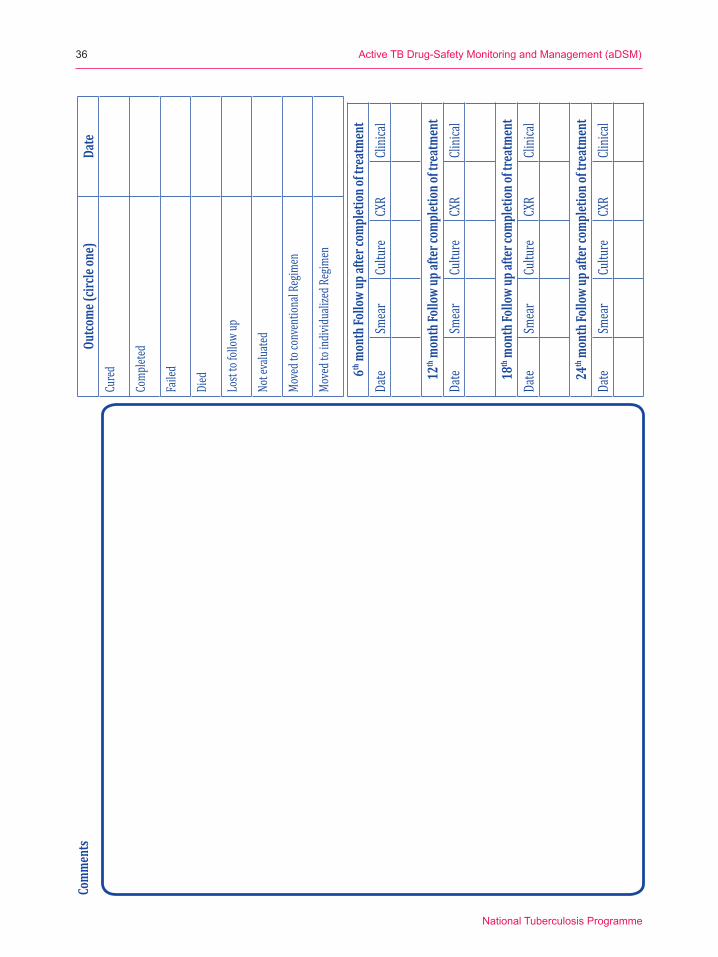
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
36
Outco
me (
circle
one)
Date
Cure
d
Comp
leted
Faile
d
Died
Lost
to fol
low up
Not e
valua
ted
Move
d to c
onve
ntion
al Re
gimen
Move
d to i
ndivi
duali
zed R
egim
en
6th m
onth
Follo
w up
afte
r com
plet
ion o
f tre
atm
ent
Date
Smea
rCu
lture
CXR
Clinic
al
12th
mon
th Fo
llow
up af
ter c
ompl
etio
n of t
reat
men
tDa
teSm
ear
Cultu
reCX
RCli
nical
18th
mon
th Fo
llow
up af
ter c
ompl
etio
n of t
reat
men
tDa
teSm
ear
Cultu
reCX
RCli
nical
24th
mon
th Fo
llow
up af
ter c
ompl
etio
n of t
reat
men
tDa
teSm
ear
Cultu
reCX
RCli
nical
Com
men
ts
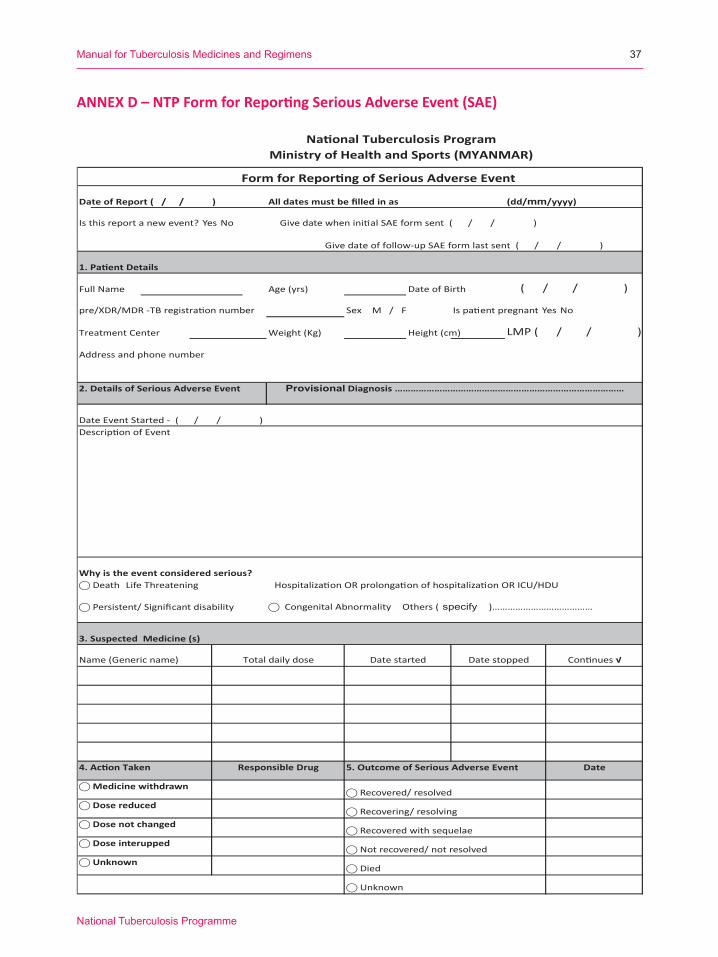
ANNEX D – NTP Form for Reporting Serious Adverse Event (SAE)
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
37
National Tuberculosis ProgramMinistry of Health and Sports (MYANMAR)
Date of Report ( / / ) All dates must be filled in as (dd/mm/yyyy)
Give date of follow-up SAE form last sent ( / / )
Full Name Age (yrs) Date of Birth
pre/XDR/MDR -TB registration number Sex M / F Is patient pregnant Yes No
Treatment Center Weight (Kg) Height (cm)
Address and phone number
2. Details of Serious Adverse Event
Why is the event considered serious?⃝ Death Life Threatening Hospitalization OR prolongation of hospitalization OR ICU/HDU
⃝ Persistent/ Significant disability ⃝ Congenital Abnormality Others ( specify )…………………………………
3. Suspected Medicine (s)
4. Action Taken 5. Outcome of Serious Adverse Event
⃝ Recovered/ resolved
⃝ Recovering/ resolving
⃝ Recovered with sequelae
⃝ Not recovered/ not resolved
⃝ Died
⃝ Unknown
Description of Event
Date
Form for Reporting of Serious Adverse Event
Is this report a new event? Yes No Give date when initial SAE form sent ( / / )
1. Patient Details
LMP ( / / )
( / / )
Continues √Date stoppedDate startedTotal daily doseName (Generic name)
Date Event Started - ( / / )
Provisional Diagnosis ……………………………………………………………………………
⃝ Unknown
Responsible Drug
⃝ Medicine withdrawn
⃝ Dose reduced
⃝ Dose not changed
⃝ Dose interupped

ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
38
National Tuberculosis ProgramMinistry of Health and Sports (MYANMAR)
Batch No
MM Reg: no
Expiry Date
⃝ IHD Hypertension Other Heart Disease (specify)…………………….. DM Renal disease
⃝ Viral Hepatitis Alcoholic Hepatitis Other Liver Disease (specify)…………………. Peptic Ulcer/ Gastritis
⃝ HIV Opportunistic Infection(s) (specify)……………………………... Last CD4/VL & date ……………………………...
⃝ Bronchial Asthma COPD Other Lung Disease (specify)…………………….. Other (specify) …………………
⃝ None
8. Concomitant Medicine (s)
Name of Reporter ………………………………………….
Address ……………………………………..
Designation ……………………………………………….. email …………………………………………………………
Signature ………………………….. Date ……………………………. Tel no. ……………………………….
9. Relevant Laboratory/ Investigation Results(s) - Clinical
Laboratory Test Date done Normal Value (unit) Patient's result (unit) Comment
Date started Date stopped Continues √Name (Generic name) Total daily dose
7. Co-morbidities
10. SOURCE OF REPORT
6. Details of suspected drug Drug 1 Drug 2 Drug 3
Brand Name (formulation/ dosage form)
Generic Name
Name of manufacturer, country of origin
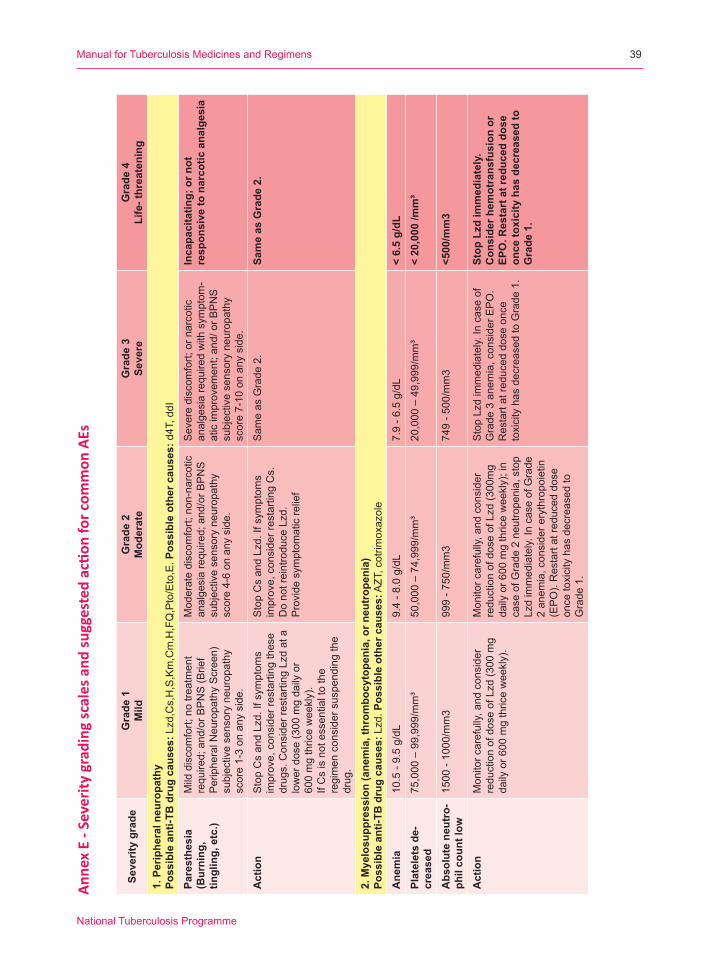
Anne
x E
- Sev
erity
gra
ding
scal
es a
nd su
gges
ted
actio
n fo
r com
mon
AEs
Seve
rity
grad
eG
rade
1
Mild
Gra
de 2
Mod
erat
eG
rade
3Se
vere
Gra
de 4
Life
- thr
eate
ning
1. P
erip
hera
l neu
ropa
thy
Poss
ible
ant
i-TB
dru
g ca
uses
:Lzd,Cs,H,S,Km,Cm,H,FQ,Pto/Eto,E.P
ossi
ble
othe
r cau
ses:
d4T
, ddI
Pare
sthe
sia
(Bur
ning
, tin
glin
g, e
tc.)
Mild
dis
com
fort;
no
treat
men
t re
quire
d; a
nd/o
r BP
NS
(Brie
f PeripheralN
europathyScreen)
subjectivesensoryneuropathy
scor
e 1-
3 on
any
sid
e.
Mod
erat
e di
scom
fort;
non
-nar
cotic
an
alge
sia
requ
ired;
and
/or B
PN
S
subjectivesensoryneuropathy
scor
e 4-
6 on
any
sid
e.
Sev
ere
disc
omfo
rt; o
r nar
cotic
an
alge
sia
requ
ired
with
sym
ptom
-at
ic im
prov
emen
t; an
d/ o
r BP
NS
subjectivesensoryneuropathy
scor
e 7-
10 o
n an
y si
de.
Inca
paci
tatin
g; o
r not
re
spon
sive
to n
arco
tic a
nalg
esia
Act
ion
StopCsandLzd.Ifsym
ptom
sim
prov
e, c
onsi
der r
esta
rting
thes
e drugs.ConsiderrestartingLzdata
low
er d
ose
(300
mg
daily
or
600mgthriceweekly).
If C
s is
not
ess
entia
l to
the
regi
men
con
side
r sus
pend
ing
the
drug
.
StopCsandLzd.Ifsym
ptom
sim
prov
e, c
onsi
der r
esta
rting
Cs.
DonotreintroduceLzd.
Pro
vide
sym
ptom
atic
relie
f
Sam
e as
Gra
de 2
.Sa
me
as G
rade
2.
2. M
yelo
supp
ress
ion
(ane
mia
, thr
ombo
cyto
peni
a, o
r neu
trop
enia
) Po
ssib
le a
nti-T
B d
rug
caus
es:Lzd.P
ossi
ble
othe
r cau
ses:AZT,cotrim
oxazole
Ane
mia
10.5
- 9.
5 g/
dL9.
4 - 8
.0 g
/dL
7.9
- 6.5
g/d
L<
6.5
g/dL
Plat
elet
s de
-cr
ease
d75
,000
– 9
9,99
9/m
m³
50,0
00 –
74,
999/
mm
³20
,000
– 4
9,99
9/m
m³
< 20
,000
/mm
³
Abs
olut
e ne
utro
-ph
il co
unt l
ow15
00 -
1000
/mm
399
9 - 7
50/m
m3
749
- 500
/mm
3<5
00/m
m3
Act
ion
Mon
itor c
aref
ully,
and
con
side
r reductionofdoseofLzd(300mg
dailyor600mgthriceweekly).
Mon
itor c
aref
ully,
and
con
side
r reductionofdoseofLzd(300mg
dailyor600mgthriceweekly);in
case
of G
rade
2 n
eutro
peni
a, s
top
Lzdimmediately.IncaseofGrade
2 an
emia
, con
side
r ery
thro
poie
tin
(EPO).Restartatreduceddose
once
toxi
city
has
dec
reas
ed to
G
rade
1.
StopLzdimmediately.Incaseof
Gra
de 3
ane
mia
, con
side
r EP
O.
Res
tart
at re
duce
d do
se o
nce
toxi
city
has
dec
reas
ed to
Gra
de 1
.
Stop
Lzd
imm
edia
tely
.C
onsi
der h
emot
rans
fusi
on o
r EP
O. R
esta
rt a
t red
uced
dos
e on
ce to
xici
ty h
as d
ecre
ased
to
Gra
de 1
.
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
39

Seve
rity
grad
eG
rade
1
Mild
Gra
de 2
Mod
erat
eG
rade
3Se
vere
Gra
de 4
Life
- thr
eate
ning
3. P
rolo
nged
QT
inte
rval
Poss
ible
ant
i-TB
dru
g ca
uses
:Cfz,B
dq,M
fx,D
lm,andLfx(amildQTprolongingdrug)
Poss
ible
oth
er c
ause
s:Otherdrugs,e.g.,erythrom
ycin,clarithrom
ycin,quinidine,ketoconazole,fluconazole,antipsychotics(allhavesom
erisk,includinghaloperidol,
chlorpromazineandrisperidone),m
anyanti-nauseadrugs(ondansetron/granisetron,dom
peridone),m
ethadone,andsom
eanti-retrovirals);geneticcausessuchas
longQTsyndrome;hypothyroidism
Prol
onge
d Q
TcF
QTcF450–480ms.
QTcFinterval481–500ms.
QTcF>
=501ms
with
out s
igns
/ sym
ptom
s of
ser
ious
ar
rhyt
hmia
.
QTc
F>=
501
or>6
0 m
s ch
ange
from
bas
elin
e an
d on
e of
the
follo
win
g:
Tors
ade
de p
oint
es o
r po
lym
orph
ic v
entr
icul
ar
tach
ycar
dia
or s
igns
/sym
ptom
s of
ser
ious
arr
hyth
mia
.A
ctio
nM
onito
r mor
e cl
osel
y; a
t lea
st
weeklyECGuntilQTcFhas
retu
rned
to le
ss th
an g
rade
1.
Rep
lete
ele
ctro
lyte
s as
nec
essa
ry.
Mon
itor m
ore
clos
ely;
at l
east
weeklyECGuntilQTcFhas
retu
rned
to le
ss th
an g
rade
1.
Rep
lete
ele
ctro
lyte
s as
nec
essa
ry.
Sto
p th
e su
spec
ted
caus
ativ
e drug(s).Hospitalizeandreplete
elec
troly
tes
as n
eces
sary
.
Stop
the
susp
ecte
d ca
usat
ive
drug
(s).
Hos
pita
lize
and
repl
ete
elec
trol
ytes
as
nece
ssar
y.
4. O
ptic
ner
ve d
isor
der (
optic
neu
ritis
)Po
ssib
le a
nti-T
B d
rug
caus
es:Lzd,E,Eto/Pto,Cfz,rifabutin,H,S.P
ossi
ble
othe
r cau
ses:
ddI
Opt
ic n
erve
di
sord
erA
sym
ptom
atic
; clin
ical
or
diagnosticobservationsonly
Lim
iting
vis
ion
of th
e af
fect
ed e
ye
(20/40[6/12]orbetter)
Lim
iting
vis
ion
in th
e af
fect
ed e
ye
(worsethan20/40[6/12]butbetter
than20/200[6/60])
Blin
dnes
s (2
0/20
0[6/
60] o
r w
orse
) in
the
affe
cted
eye
Act
ion
StopLzdimmediatelyifthereare
any
susp
icio
ns o
f opt
ic n
eurit
is. D
o no
t res
tart
it.
StopLzdimmediatelyifthereare
any
susp
icio
ns o
f opt
ic n
eurit
is. D
o no
t res
tart
it.
StopLzdimmediatelyifthereare
any
susp
icio
ns o
f opt
ic n
eurit
is. D
o no
t res
tart
it.
Stop
Lzd
imm
edia
tely
if th
ere
are
any
susp
icio
ns o
f opt
ic
neur
itis.
Do
not r
esta
rt it
.5.
Hep
atiti
sPo
ssib
le a
nti-T
B d
rug
caus
es:Z
,Lzd,Cfz,Bdq.P
ossi
ble
othe
r cau
ses:
unk
now
n
ALT
(SG
PT)
1.1
– 3.
0 x
uppe
r lim
it of
nor
mal
(ULN
)>3
.0 –
5.0
x U
LN>5
.0 –
20.
0 x
ULN
>20.
0 x
ULN
AST
(SG
OT)
1.1
– 3.
0 x
ULN
>3.0
– 5
.0 x
ULN
>5.0
– 2
0.0
x U
LN>2
0.0
x U
LNA
ctio
nC
ontin
ue tr
eatm
ent r
egim
en.
Patientsshouldbefolloweduntil
resolution(returntobaseline)or
stabilizationofAST/ALTelevation.
Con
tinue
trea
tmen
t reg
imen
. Patientsshouldbefolloweduntil
resolution(returntobaseline)or
stabilizationofAST/ALTelevation.
Sto
p al
l dru
gs, i
nclu
ding
ant
i- TB
dr
ugs;
mea
sure
LFT
s w
eekl
y.Treatmentm
aybereintroduced
afte
r tox
icity
is re
solv
ed.
Stop
all
drug
s, in
clud
ing
anti-
TB
drug
s; m
easu
re L
FTs
wee
kly.
Trea
tmen
t may
be
rein
trod
uced
af
ter t
oxic
ity is
reso
lved
.
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
40

Seve
rity
grad
eG
rade
1
Mild
Gra
de 2
Mod
erat
eG
rade
3Se
vere
Gra
de 4
Life
- thr
eate
ning
6. A
cute
kid
ney
inju
ry
Poss
ible
ant
i-TB
dru
g ca
uses
: S,K
m,A
m,C
m. P
ossi
ble
AR
T ca
uses
:Tenofovir(TDF)-rare
Acu
te k
idne
y In
jury
Cre
atin
ine
leve
l inc
reas
e of
>0
.3 m
g/dL
; cre
atin
ine
1.5-2.0xabovebaseline
Creatinine2-3xabovebaseline
Cre
atin
ine
>3 x
baselineor>4.0m
g/dL;
hospitalizationindicated
Life
-thre
aten
ing
cons
eque
nces
; di
alys
is in
dica
ted
Act
ion
Considerstoppinginjectable
until
cre
atin
ine
has
retu
rned
to
baseline.Considerrestartingthe
injectableatlow
erfrequency
(e.g.,MWF).
Stopinjectableuntilcreatininehas
returnedtobaseline.Consider
restartingtheinjectableatlow
er
frequency(e.g.,MWF)or
substitutewithanon-nephrotoxic
drug
.
Stopinjectableuntilcreatininehas
returnedtobaseline.Consider
restartingtheinjectableatlow
er
frequency(e.g.M
WF)orsubstitute
with
a n
on- n
ephr
otox
ic d
rug.
Stop
inje
ctab
le u
ntil
crea
tinin
e ha
s re
turn
ed to
bas
elin
e. C
on-
side
r res
tart
ing
the
inje
ctab
le a
t lo
wer
freq
uenc
y (e
.g. M
WF)
or
subs
titut
e w
ith a
non
- nep
hro-
toxi
c dr
ug.
7.
Hyp
okal
emia
and
hyp
omag
nese
mia
Po
ssib
le a
nti-T
B d
rug
caus
es: C
m,K
m,A
m,S
. Pos
sibl
e A
RT
caus
es:T
DF(rare)
Hyp
okal
emia
3.4
- 3.0
mE
q/L
2.9
- 2.5
mE
q/L
2.4
- 2.0
mE
q/L
or in
tens
ive
repl
acem
ent t
hera
py o
r hospitalizationrequired
< 2.
0 m
Eq/L
or a
bnor
mal
po
tass
ium
with
par
esis
, ile
us o
r lif
e-th
reat
enin
g ar
rhyt
hmia
Act
ion
Continueinjectable.S
tartoral
pota
ssiu
m re
plac
emen
t the
rapy
. C
heck
ser
um m
agne
sium
and
re
plac
e if
nece
ssar
y.
Continueinjectable.S
tart
aggr
essi
ve o
ral p
otas
sium
re
plac
emen
t the
rapy
. Rep
lace
m
agne
sium
as
nece
ssar
y.
Continueinjectable.S
tartIV
pota
ssiu
m re
plac
emen
t the
rapy
in
addi
tion
to o
ral.
Rep
lace
mag
-ne
sium
and
oth
er e
lect
roly
tes
as
nece
ssar
y.
Stop
inje
ctab
le te
mpo
raril
y.
Star
t IV
pota
ssiu
m re
plac
emen
t th
erap
y in
add
ition
to o
ral.
Rep
lace
mag
nesi
um a
nd o
ther
el
ectr
olyt
es a
s ne
cess
ary.
Hyp
omag
nese
-m
ia0.
60-0
.70
mm
ol/L
0.45
-0.5
9 m
mol
/L0.
30-0
.44
mm
ol/L
<0.3
0 m
mol
/L
8. H
ypot
hyro
idis
m
Pos
sibl
e an
ti-TB
dru
g ca
uses
: Eto
/Pto
, PA
S. P
ossi
ble
AR
T ca
uses
: d4T
Hyp
othy
roid
ism
Asy
mpt
omat
ic; c
linic
al o
r diagnosticobservationsonly;
inte
rven
tion
not i
ndic
ated
Sym
ptom
atic
; thy
roid
repl
acem
ent
indi
cate
d; li
miti
ng iA
DL
(inst
rum
en-
talactivitiesofdailyliving)*
Sev
ere
sym
ptom
s; li
miti
ng s
elf-
careADL*hospitalizationindicated
Life
-thre
aten
ing
cons
eque
nces
; ur
gent
inte
rven
tion
indi
cate
d
Act
ion
Con
tinue
ant
i-TB
dru
gs.
Con
tinue
ant
i-TB
dru
gs. S
tart
thyr
oxin
e.C
ontin
ue a
nti-T
B d
rugs
. Sta
rt th
yrox
ine.
Stop
all
anti-
TB d
rugs
. Sta
rt
thyr
oxin
e.
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
41
*https://w
ww.payingforseniorcare.com
/longtermcare/activities-of-daily-living.html#title2

Seve
rity
grad
eG
rade
1
Mild
Gra
de 2
Mod
erat
eG
rade
3Se
vere
Gra
de 4
Life
- thr
eate
ning
8. H
earin
g lo
ss
Po
ssib
le a
nti-T
B d
rug
caus
es: S
,Km
,Am
,Cm
,Clr.
Pos
sibl
e ot
her c
ause
s: n
one.
Hea
ring
loss
Adu
lt en
rolle
d in
mon
itorin
g program(ona1,2,4,3,6and8kH
zaudiogram):thresholdshiftof
15 -
25 d
B a
vera
ged
at
2 co
ntig
uous
test
freq
uenc
ies
in a
t leastoneearorsubjectivechange
intheabsenceofa
Gra
de 1
Thr
esho
ld s
hift.
Ped
iatri
c (o
n a
1, 2
, 4,3
, 6 a
nd
8kH
zaudiogram):thresholdshift
>20dB
at8kHzinatleastone
ear.
Adu
lt en
rolle
d in
mon
itorin
g program(ona1,2,3,4,6and8kH
zaudiogram):thresholdshiftof
>25
dB a
vera
ged
at 2
con
tiguo
us
test
freq
uenc
ies
in a
t lea
st o
ne e
ar.
Adu
lt no
t enr
olle
d in
mon
itorin
g program:hearinglossbuthearing
aid
or in
terv
entio
n no
t ind
icat
ed;
limiti
ng in
stru
men
tal A
DL.
Pediatric(ona1,2,3,4,6and8kH
zaudiogram):thresholdshift
>20dB
at4kHzandaboveinat
leas
t one
ear
.
Adu
lt en
rolle
d in
mon
itorin
g program(ona1,2,3,4,6and8kH
zaudiogram):thresholdshiftof
>25
dB a
vera
ged
at 3
con
tigu-
ous
test
freq
uenc
ies
in a
t lea
st
one
ear;
ther
apeu
tic in
terv
entio
n in
dica
ted.
Adu
lt N
ot e
nrol
led
in m
onito
ring
program:hearinglosswithhearing
aid
or in
terv
entio
n in
dica
ted;
lim
it-in
g se
lf-ca
re A
DL.
Ped
iatri
c (o
n a
1, 2
, 3, 4
, 6 a
nd
8kH
zaudiogram):hearingloss
sufficienttoindicatetherapeutic
inte
rven
tion,
incl
udin
g he
arin
g aids):Thresholdshift>20dBat
3kH
zandaboveinatleastone
ear;
addi
tiona
l spe
ech-
lang
uage
re
late
d se
rvic
es in
dica
ted.
Adu
lts: p
rofo
und
bila
tera
l he
arin
g lo
ss (T
hres
hold
>8
0 dB
HL
at 2
kH
z an
d ab
ove)
; no
n-se
rvic
eabl
e he
arin
g Pe
diat
ric: a
udio
logi
c in
dica
tion
for c
ochl
ear i
mpl
ant a
nd
addi
tiona
l spe
ech-
lang
uage
re
late
d se
rvic
es in
dica
ted.
Act
ion
Continueinjectable.
Considerdecreasinginjectable
frequ
ency
if fu
rther
hea
ring
loss
is
a co
ncer
n. In
itiat
e di
scus
sion
with
patientaboutrisksandbenefitsof
theinjectable.C
onsiderreplacing
injectableagentwith
a no
n- o
toto
xic
TB d
rug.
DoNOTsubstituteasingledrug
repl
acem
ent i
f the
trea
tmen
t is
faili
ng, a
dd a
dditi
onal
TB
dru
gs.
Con
side
r sto
ppin
g or
dec
reas
ing
injectablefrequency(e.g.M
WF).
Dis
cuss
with
pat
ient
the
risks
and
benefitsoffurtherinjectableuse.
In m
ost c
ases
of G
rade
3 h
earin
g losstheinjectableshouldbe
stop
ped
and
repl
aced
with
a
non-
otot
oxic
TB
dru
g.DoNOTsubstituteasingledrug
repl
acem
ent i
f the
trea
tmen
t is
faili
ng, a
dd a
dditi
onal
TB
dru
gs.
Con
side
r con
tinue
inje
ctab
le
if to
lera
ted
by th
e pa
tient
. (In
ca
ses
of c
ompl
ete
hear
ing
loss
, so
me
clin
icia
ns w
ill c
ontin
ue
the
inje
ctab
le a
gent
as
the
dam
age
is a
lread
y do
ne).
Con
side
r sus
pens
ion
of th
e in
ject
able
if o
ngoi
ng u
se
cont
ribut
es to
wor
seni
ng ti
nni-
tus
or v
estib
ular
dis
turb
ance
s (o
r if s
ome
hear
ing
mig
ht b
e st
ill
pres
erve
d). A
dd a
dditi
onal
TB
dr
ugs
as n
eede
d.
Source:EndTBClinicalandProgram
maticGuideforpatientmanagem
entw
ithnew
TBdrugs,ver3.3,25/11/2016,PartnersinHealth,IRD,M
SFandUNITAID
ActiveTBDrug-SafetyMonitoringandManagement(aDSM)
NationalTuberculosisProgramme
42

40dB
Slig
ht/M
ild41
-60
dBM
oder
ate
61-8
0 dB
Seve
reO
ver 8
1 dB
Prof
ound
Difficultyhearingandunderstand
-in
g so
ft sp
eech
, spe
ech
from
a
dist
ance
, or s
peec
h ag
ains
t a
backgroundofnoise
Difficultyhearingregularspeech,
even
at c
lose
dis
tanc
e.
May
onl
y he
ar v
ery
loud
spe
ech
or
loud
sou
nds
in th
e en
viro
nmen
t, suchasafiretrucksirenoradoor
slam
min
g. M
ost c
onve
rsat
ion
spee
ch is
not
hea
rd.
May
per
ceiv
e lo
ud s
ound
s as
vi
brat
ions
In th
e ca
se o
f mod
erat
e he
arin
g lo
ss, t
he ra
nge
for c
hild
ren
is 3
1-60
dB
.
WHO
Cla
ssifi
catio
n gr
adin
g sc
ale
for h
earin
g lo
ss
ManualforTuberculosisMedicinesandRegimens
NationalTuberculosisProgramme
43