Embed Size (px)
Citation preview

ACOSOG (NCCTG, CALGB) Alliance Thoracic Committee
Kemp H. Kernstine, MD PhD 7-12-12

ACOSOG Thoracic Committee
Chair: Bryan Meyers, M.D., MPH
Vice Chairs: Malcolm Brock, MD
Tom DiPetrillo, M.D.
Ramaswamy Govindan, M.D.
Carolyn Reed, MD



Aim #1: To individualize the care of thoracic malignancies through novel and local ablative therapies
Aim #2: To apply neoadjuvant and adjuvant therapeutic strategies for NSCLC and esophageal cancers
Aim #3: Enhance therapeutic efficacy through biological and molecular markers
Thoracic Committee Aims

Outline of ACOSOG Lung Cancer Trials
Z0030 Early Dx Lymphatic Sampling v Dissection
Z0040 Occult Metastases and Effect On Survival
Z4032 Wedge vs Wedge BrachyThx in Hi Risk Early Disease
Z4033 RFA in Hi Risk Early Disease
Z4099/RTOG-1041 IMRT vs Wedge in Hi Risk

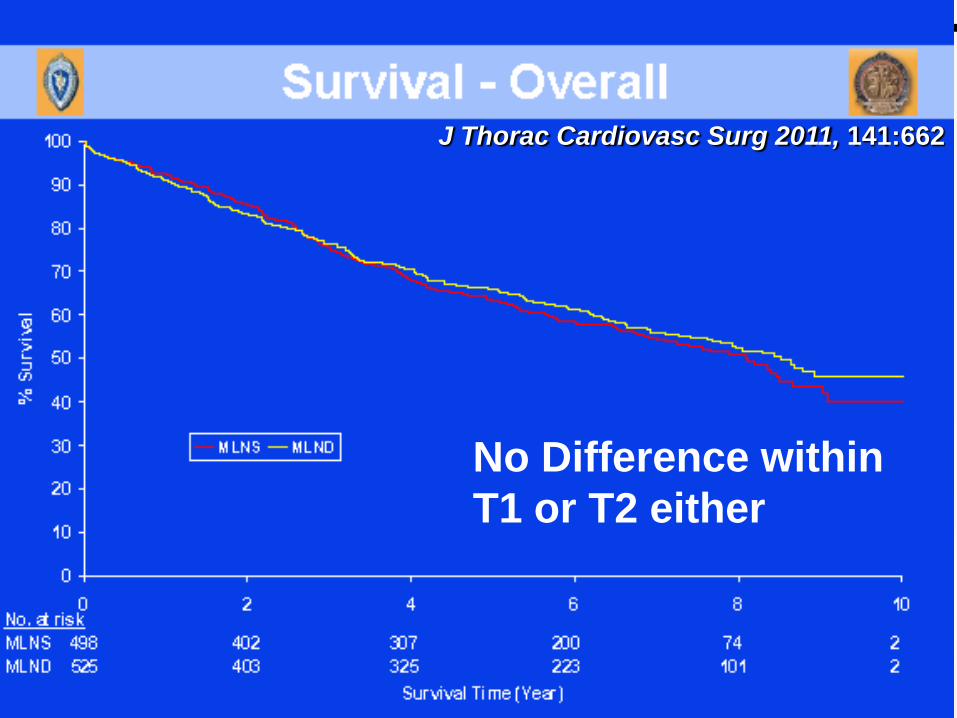
Z0030 Randomized Trial of Mediastinal Lymph Node Sampling versus Complete Lymphadenectomy During Pulmonary Resection in the Patient with N0 or N1 (less than hilar) Non-Small Cell Carcinoma
Improve Local Control Aim #1

No Differences in Complications: Lymph Node Sampling vs MSLD
Ann Thorac Surg 2006 81:1013

J Thorac Cardiovasc Surg 2011, 141:662

J Thorac Cardiovasc Surg 2011, 141:662
J Thorac Cardiovasc Surg 2011, 141:662
No Difference within
T1 or T2 either

J Thorac Cardiovasc Surg 2011, 141:662

J Thorac Cardiovasc Surg 2011, 141:662

How Many More Lymph Nodes? Sampling vs Dissection
• Dissection 18 more lymph nodes, Right
equaled Left
• Dissection 11-12 more N2 lymph nodes,
Right equaled Left
• 90% of Dissection patients had 10 nodes
harvested in each of 3 stations
Chest 2011; 139:1124

Z0040: A Prospective Study of the Prognostic Significance of Occult Metastases in the Patient with Resectable Non-small Cell Lung Carcinoma.
Enhance Therapy / Biomarkers Aim #3

Occult Metastases in Lymph Nodes Predict Survival in Resectable Non–Small-Cell Lung Cancer:
Report of the ACOSOG Z0040 Trial
Determine prevalence of occult metastases and it’s relationship to survival
•Eligible: previously untreated and
potentially resectable NSCLC
•Nodes reexamined after routine exam and
w cytokeratin IHC; saline lavage prior to
and after resection; bone marrow
examined

ACOSOG Z0040
• July, 1999 to March, 2004
• 1,047 acceptable patients (accrued 1310-20% excluded), median age 67.2 years
• 66% Stage I
• Pleural lavage positive in 29 (3.3%)
• Bone marrow positive in 66 (8%)
• N0 lymph nodes positive (anticytokeratin antibodies CAM 5.2 and AE-1) in 130 (22.4%)

Z0040-Conclusions
• Positive Bone Marrow and Pleural Wash did not worsen survival
• Occult metastases in the LN did worsen the survival, HR 1.59-1.63
• There was no correlation between the number of IHC involved nodes and survival.

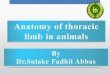
High-risk
patients with
suspected
or proven
NSCLC
Histological
confirmation
of NSCLC
Sublobar
resection
Sublobar
resection +
brachytherapy
R
A
N
D
O
M
I
Z
E
Z4032: A randomized phase III study of sublobar resection versus sublobar resection plus brachytherapy in high-risk patients with non-small cell lung cancer (NSCLC), 3cm
Improve Local Control Aim #1
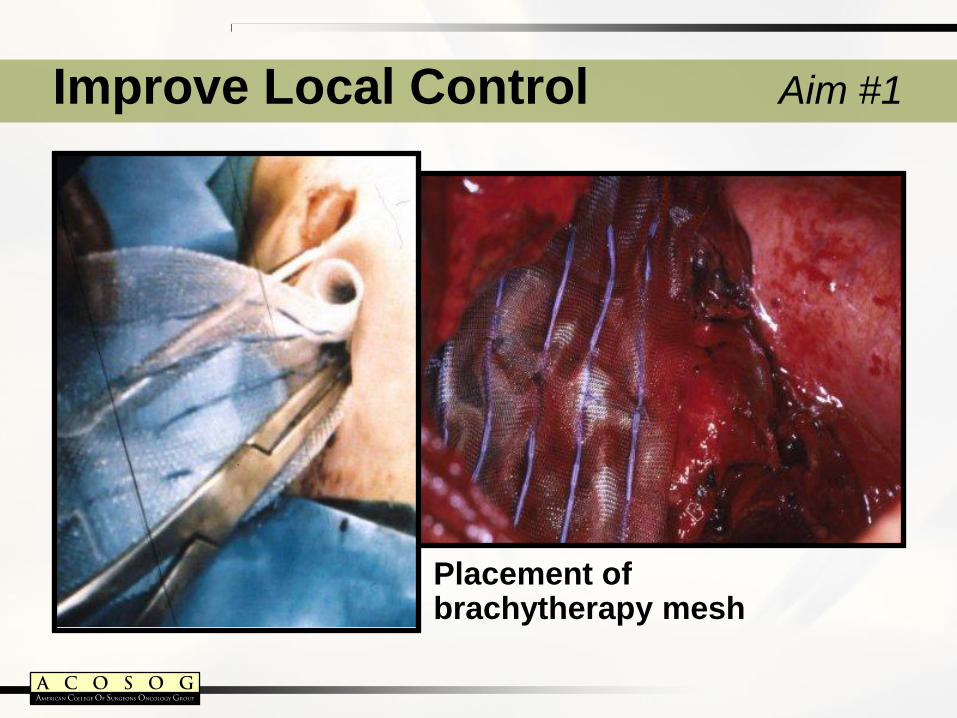
Placement of brachytherapy mesh
Improve Local Control Aim #1




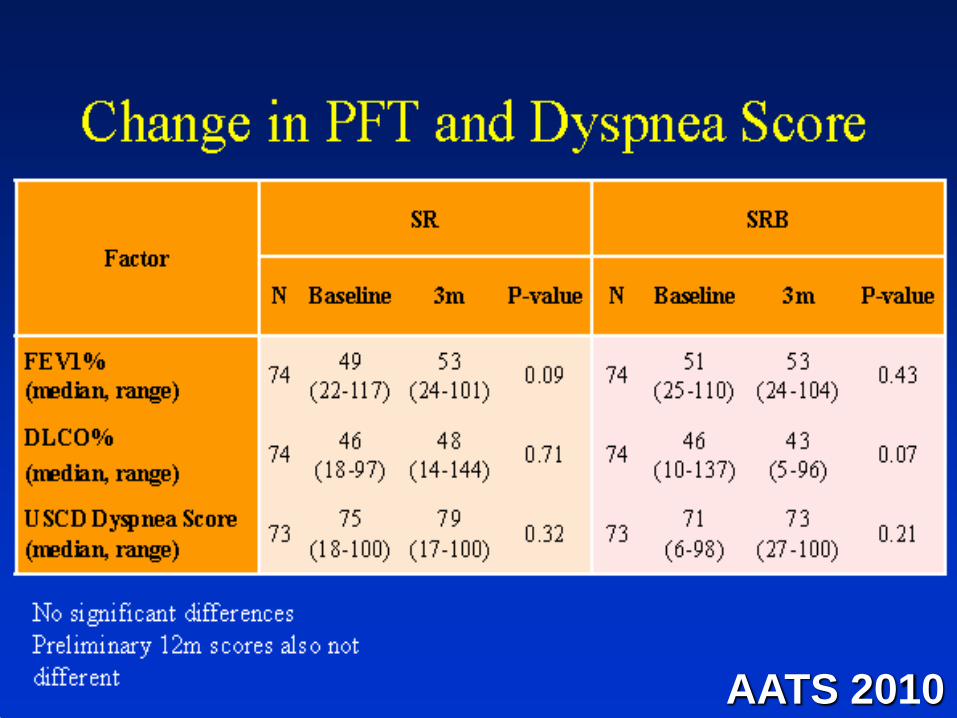
AATS 2010


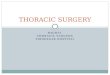
Z4033: A pilot study of radiofrequency ablation in high-risk patients with stage IA non-small cell lung cancer
High-risk
patients with
suspected or
proven
NSCLC
Non-
resectable
candidates
Radiofrequency
ablation (RFA)
+ NSCLC
CT image to
document site
and approach
Improve Local Control: Z4033 Aim #1

Putnam JB et al: SPIE Proceedings 75:139, 2000
RFA effects on soft tissues
• Preclinical studies
• Acute porcine model
• Normal lung
Improve Local Control: Z4033 Aim #1

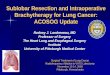
Pre-Radiofrequency Ablation RFA Procedure
48 hrs post-RFA
Complete metabolic response (uptake equivalent to blood pool)
Improve Local Control: Z4033 Aim #1

3 days post
RFA
Complete
Response
6 months post
RFA
Partial
Response
pre RFA

Preserve surgical effectiveness and minimize surgical morbidity for early stage NSCLC in the high-risk and more normal-risk patient
• From Z4032 – sublobar resection (+/- brachytherapy) vs. stereotactic body radiotherapy in high-risk patients
ACOSOG Z4099/RTOG 1021

A Randomized Phase III Study of
Sublobar Resection (+/- Brachytherapy) versus Stereotactic
Body Radiation Therapy in High Risk Patients with Stage I Non-
Small Cell Lung Cancer (NSCLC) ACOSOG Z4099/RTOG 1021
Same group of patients as in Z4032
Inclusion: FEV1 < 50% or DLCO < 50%; Minor (need 2): Age > 75, FEV1 DLCO, Pulm HTN sys > 40mmHG, LVEF < 40%, PaO2 < 55, PaCO2 45 mmHg, MMRC score > 3

A Randomized Phase III Study of Sublobar Resection versus Stereotactic Body Radiation Therapy in High Risk Patients with Stage I Non-Small Cell Lung Cancer. PI Chrish Fernando / Bob Timmerman
Improve Local Control: ACOSOG Z4099 / RTOG 1021
18 Gy x 3

Improve Local Control: ACOSOG Z4099 / RTOG 1021
Primary objective:
To ascertain whether patients treated by
SBRT have 3-year overall survival (OS) rate
that is no more than 10% less than patients
treated with SR.

Improve Local Control: ACOSOG Z4099 / RTOG 1021
Secondary objective(s): • To compare loco-regional recurrence-free survival and
disease-free survival between study arms. Locoregional recurrence
includes recurrence within the same lobe or hilum (N1 nodes), or progression
within 1cm of the staple line after SR, or within 1cm of the PTV after SBRT (local
progression) after treatment effects such as scarring have subsided.
• To compare treatment-related specific adverse event
profiles at 1, 3 and 12 months post therapy.
• To compare pulmonary function between arms
• To determine morbidity in each arm for patients with low or
high Charlson comorbidity index scores, and whether this
index can be used to select patients for SBRT or SR.

Intergroup Participation ECOG 1505 – postoperative adjuvant chemotherapy +/- bevacizumab (p stage IB >4 cm, II, select IIIA)
CALGB 30506 – metagene predictor model for adjuvant chemotherapy (p stage IA, IB <4 cm)
CALGB 140503 - A Phase III trial of lobectomy versus sublobar resection for small (≤ 2 cm) NSCLC
ECOG 2202 – minimally invasive esophagectomy
RTOG 1010 - A phase III trial evaluating Trastuzumab with trimodality therapy HER2-overexpressing EC
ACOSOG Z4099 - Adjuvant Mediastinal Observation or Radiotherapy Evaluation for occult N2

Translational Studies
Adjuvant therapy in early or locally advanced stage (resected) NSCLC based on a selected ‘high-risk’ molecular characteristic such as
• metagene model
• DNA methylation lymph nodes
• Simple (e.g. 2-gene) prognostic model
Summary
• Novel large thoracic surgical studies with innovative therapeutic aims completed which will impact choice and extent of care of patients with NSCLC
• Multidisciplinary participation embraced with rapid expansion of protocols.
• Engaging other cooperative groups as a strategic plan to complete high-priority surgical studies