Embed Size (px)
Citation preview

Access to Hepatitis B and C
Medicines
Morgane Ahmar, International Treatment
Preparedness Coalition (ITPC), Morocco
Conference on Liver Disease in Africa (COLDA)
Cairo, September 8 2019

EPIDEMIOLOGICAL DATA AND
TREATMENT ACCESS GAPS

Africa is covered by 2 WHO Regional Offices
➢ EMRO (Morocco, Tun is ia,
L ibya, E gypt, S udan ,
S om alia)
➢AFRO
No consolidated data

▪ HBV:
- 10% of PLHBV aware of their status (27 of 257M)
- 1,8% are on treatment (4,5M)
- 1.1M people newly infected in 2017
▪ HCV:
- 19% of PLHCV aware of their status (13 of 70M)
- 2,5% on treatment (1,8 M)
- 1.75M people newly infected in 2015
Smith S. & al “Global progress on the elimination of viral hepatitis as a major public health threat: An
analysis of WHO Member State responses”, 2017
Large treatment gaps to fill globally

Africa lagging behind

WHAT MEDICINES DO WE NEED

DAAs: A revolution and a cure for
HCV
Afdhal et al; NEJM 2014; Bansai et al; World J Hepatol
2015; Feld et al; NEJM 2014;Sulkowski et al; NEJM 2014
▪ WHO recommended pangenotypic medicines:
Sofosbuvir+ Daclatasvir/ Velpatasvir
▪ Oral, short duration, some are pangenotypic,
simplified diagnostics, monitoring and treatment, high
cure rates, safe and tolerable

HBV treatment: No cure but efficient
treatment
▪ WHO recommendations for preferred first-line:
tenofovir/entecavir
▪ High genetic barrier to resistance, high
efficacy, minor side-effects, once-daily oral,
potential for harmonizing treatment (HIV co-
infection, TB)
▪ Available and used in most countries for HIV
treatment

Slow uptake in Africa
▪ Only 26% of AFRO countries and 56% of
EMRO countries reported access to DAA
regimens as first line treatment for all
▪ Only 44% of AFRO countries and 63% EMRO
countries reported access to tenofovir or
entecavir to be the first-line treatment for
patients with chronic HBV
Tordrup D. & al. Additional resource needs for viral hepatitis elimination through universal
health coverage: projections in 67 low-income and middle-income countries, 2016–2030, 2019

DRIVERS AND BARRIERS TO
ACCESS IN AFRICA
1/ Affordability and access to generics

Affordability/Prices of medicines = linked
to Local Patents

Access to generics and price
decreases▪ HBV:
- Generic TDF and FTC widely available at low cost in LMICs as part of national ART programs (e.g. TDF = US$ 32 ppy without patent protection)
▪ HCV:
- Strong advocacy by CSOs for access to generic HCV drugs => drastic price reductions in very short time : 142.000$ to 78$ per cure, around 150 US$ in several LMICS
- Very few patents filed in the continent, rejection of patent applications in Morocco and Egypt
- Local production: Egypt, Morocco, Tunisia, Algeria, others?
- Inclusion in voluntary licenses granted by originators to Indian generic manufacturers, advocacy for inclusion of North African in the licences: “theoretical” access to generics
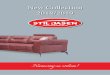
Andrieux-Meyer & al, Disparity in market prices for hepatitis C virus direct-
acting drugs, 2015

DRUG USA PRICE
GLOBAL
LOWEST
PRICE
ESTIMATED
COST
PATENT
EXPIRY
(US)
TDF/FTC
$17,258
(pppy) $67 $54Expired
Entecavir
$5,915
(pppy) $409 $36Expired
SOF+LDV
$91,207
(per cure) $307 $792028-2032
SOF+DCV
$142,710
(per cure) $78 $472028-2031
Prices and costs of drugs to treat HBV
and HCV (A. Hill)

DRIVERS AND BARRIERS TO
ACCESS IN AFRICA
2/ Transparency, regulatory and
procurement obstacles

From theoretical access to generics...

Towards effective access

Transparency and procurement
challenges
▪ TDF and FTC sometimes unavailable outside of
HIV programs and large price variance 50-
500 US$
▪ High price variances for DAAs and lack of
transparency for SOF costs US$500 in Côte
d’Ivoire vs. 150 in India (lack of transparency)
Andrieux-Meyer & al, Disparity in market prices for hepatitis C virus direct-
acting drugs, 2015

CHALLENGES AND
OPPORTUNITIES FOR SCALE-UP

Challenges for scale up
▪ National strategic planning and dedicated funding:
▪ Lack of epidemiological data to inform prevention, testing and
treatment strategies
Reported
having
hepatitis
national plan
Reported
having a
published
national plan.
Reported
inclusion of
impact targets in
national plan
Reported inclusion
of service
coverage targets
in national plan
Reported having
dedicated
funding for
national plan
AFRO 52% 19% 15% 30% 22%
EMRO 82% 38% 38% 63% 44%
Tordrup D. & al. Additional resource needs for viral hepatitis elimination through universal
health coverage: projections in 67 low-income and middle-income countries, 2016–2030, 2019

Challenges for scale up (2)
▪ Lack of involvement of civil society:
▪ Civil society played an important role in advocacy for treatment scale
up of HIV and demand creation for services
▪ Number of NGOs very limited
- Among the countries where MoH reported engagement with civil society, 84% with a
national viral hepatitis elimination plan (1)
- Only 48% of AFRO countries (56% for EMRO), reported engagement with civil
society (2)
▪ Lack of funding mechanisms nationally and globally
- US$ 6bn per year needed to reach hepatitis targets
- Current spending of US$ 0.5bn as of 2016
(1) Smith & al., JHEP Reports, August 2019
(2) Tordrup D. & al. Additional resource needs for viral hepatitis elimination through universal health
coverage: projections in 67 low-income and middle-income countries, 2016–2030, 2019

▪ Leadership and strong political will
▪ Ambitious planning and target setting:
- Decentralization
- More than 20 million people tested
- More than 2 million people treated
▪ Resource mobilization (National budget, fundraising through mobile technologies,
private sector…)
▪ Price reduction strategy:
- Negotiations with pharma
- Public health approach to patent examination (patents on SOF and DCV rejected)
- Local production of DAAs
▪ Involvement of media, community based organizations
What works: the example of Egypt

Conclusions
▪ Ambitious targets have been set globally, access to treatment is increasing but unequally and
remains low in Africa
▪ Limited portfolio of medicines (4 to 6) is needed to treat both HBV and HCV according to
WHO standards: generic versions are available on the global market at low price
▪ Price and affordability do not AND should not constitute an access barrier in Africa (limited
or expired patents, inclusion in voluntary licenses…)
▪ Lack of transparency in pricing, mark-ups and negotiation power, regulatory issues and
procurement procedures may constitute a barrier to price reductions
▪ High potential for local manufacturing: an opportunity for the continent to develop local
industries and create autonomy from Indian dependence (HIV)
▪ Leadership, National planning and ambitious target setting are key for successful scale up
▪ The role of civil society is key for advocacy and demand creation and needs to be promoted
and funded
▪ The funding GAP needs to be addressed globally and nationally (innovative funding
approaches? Integration in existing programs, role of the private sector to reconsider…)

Thank you.