Embed Size (px)
Citation preview

Canadian Association of Radiologists Journal 61 (2010) 217e222www.carjonline.org
Vascular and Interventional Radiology / Radiologie vasculaire et radiologie d’intervention
Ablative Technologies in the Management of Patients with Primaryand Secondary Liver Cancer: An Overview
Nasir A. Khan, HBSca, Mark O. Baerlocher, MDb, Richard J. T. Owen, MDc, Stephen Ho, MDg,John R. Kachura, MDb,d, Stephen T. Kee, MDe, Dave M. Liu, MDe,f,g,*
aUndergraduate Medical Education, Faculty of Medicine, University of Toronto, Toronto, Ontario, CanadabDepartment of Medical Imaging, Faculty of Medicine, University of Toronto, Toronto, Ontario, Canada
cDepartment of Radiology and Diagnostic Imaging, Faculty of Medicine, University of Alberta, Edmonton, Alberta, CanadadDepartment of Medical Imaging, Toronto General Hospital, University Health Network, Toronto, Ontario, CanadaeDepartment of Radiological Sciences, David Geffen School of Medicine, University of California, Los Angeles, CA
fDepartment of Radiology, Faculty of Medicine, University of British Columbia, Vancouver, British Columbia, CanadagDepartment of Radiology, Interventional Radiology Section, Vancouver General Hospital, Vancouver, British Columbia, Canada
Abstract
Interventional ablative technologies have played an increasingly important role in the management of patients with primary or secondaryliver malignancies. Ethanol and acetic acid ablation were the primary modalities available 2 decades ago. Today, several new technologies areavailable, including radiofrequency ablation, cryoablation, and microwave ablation. Radiofrequency ablation is the most widely practiced,however, cryoablation and microwave ablation are reasonable choices in certain situations. Irreversible electroporation is a newer technique,which has yet to enter clinical practice, but shows promising preliminary results. Herein, we provide a brief overview of the above-mentionedtechnologies with a focus on principles of ablation and technique. We also describe the use of these techniques in the context of cytor-eduction, a noncurative approach aimed at reducing the overall tumour burden and providing concomitant survival benefit.
Resume
Les technologies d’ablation interventionnelles (percutanees) jouent un role de plus en plus important dans la gestion des patients atteintsd’un cancer primitif ou secondaire du foie. L’ablation a l’ethanol et a l’acide acetique ont ete les premieres techniques utilisees il y a deuxdecennies. Aujourd’hui, plusieurs nouvelles technologies sont disponibles, dont l’ablation par radiofrequence, la cryo-ablation et l’ablationpar micro-ondes. L’ablation par radiofrequence est la technique la plus couramment utilisee, mais la cryo-ablation et l’ablation par micro-ondes se revelent des choix senses dans certaines situations. L’electroporation irreversible est une technique plus recente qui n’est pas encoreutilisee en pratique clinique, mais dont les resultats preliminaires sont prometteurs. Le present article fournit un bref apercu des technologiesmentionnees ci-dessus en mettant l’accent sur les principes d’ablation et la technique utilisee. Il decrit egalement l’utilisation des techniquesen cytoreduction, une approche novatrice visant a reduire le fardeau tumoral global et a produire un avantage concomitant de survie.� 2010 Canadian Association of Radiologists. All rights reserved.
Key Words: Liver; Hepatocellular carcinoma; Metastasis; Ablation; Ethanol; Cryoablation; Microwave; Radiofrequency; Cytoreduction
The prevalence of primary liver cancer, or hepatocellularcarcinoma (HCC), continues to rise, and it is now the fifthmost common cancer in the world. This is primarily relatedto the increase in the prevalence of chronic hepatitis B and Cviral infections worldwide [1]. Currently, HCC is primarily
* Address for correspondence: Dave M. Liu, MD, Department of Radi-
ology, Vancouver General Hospital, 855 West 12th Avenue, Vancouver,
British Columbia V5Z 1M9, Canada.
E-mail address: [email protected] (D. M. Liu).
0846-5371/$ - see front matter � 2010 Canadian Association of Radiologists. A
doi:10.1016/j.carj.2009.12.009
a surgically managed disease process, either through resec-tion or transplantation [2].
Because of limitations in organ allocation, costs, and thehigh rates of clinical ineligibility (‘‘Milan’’ and University ofCalifornia San Francisco [‘‘UCSF’’] criteria), many patientsfail to undergo transplantation. Surgical resection serves as thenext best alternative, either as a bridge to transplantation or asa primary treatment modality. However, a substantial propor-tion of patients are precluded from surgical options because ofa lack of hepatic reserve, extrahepatic disease, and comorbid
ll rights reserved.

218 N. A. Khan et al. / Canadian Association of Radiologists Journal 61 (2010) 217e222
disease [3]. As a result, image-guided therapies, eg, percuta-neous ablation, have taken on a greater role in the managementof patients with primary liver cancer who are unable to benefitfrom liver transplantation or surgical resection.
In addition to primary hepatic malignancies, the liver isa frequent site for metastatic spread of tumour from distantprimary sites, including colorectal, neuroendocrine, breast,and a host of other primary malignancies [4]. In patients withmetastatic liver disease, bilobar, nonresectable disease iscommon, and this presents unique challenges in the overallmanagement of these patients. Today, a variety of optionsexist for these patients in the context of locoregional therapy,including surgical resection [5], systemic or hepatic arterychemotherapy [6,7], and various ablative technologies [8,9].Patients often undergo a combination of these therapeuticmodalities in an effort to apply a patient-centered, evidence-based approach to therapy.
The objective of this article is to provide a brief overview ofthe various ablative technologies available in the managementof patients with primary and secondary liver malignancies,including chemical ablation (ethanol and acetic acid), radio-frequency ablation (RFA), cryoablation, microwave ablation,and irreversible electroporation (IRE). We also describe theuse of these techniques in the context of cytoreduction,a noncurative approach aimed at reducing the overall tumourburden while providing concomitant survival benefit.
Overview of Ablative Technologies
Chemical Ablation (Ethanol and Acetic Acid)
Figure 1. Representative, coronal, contrast-enhanced computed tomography
images through the upper abdomen in a patient with metastatic liver disease.
(A) Preablation image shows a well-demarcated, subscapular (arrows) lesion
within the liver. (B) Image that demonstrates the tip of the radiofrequency
electrode (arrow), with multiple metal tines situated within this lesion.
Chemical ablation, which involves the use of absoluteethanol or acetic acid, is the oldest of the ablative technolo-gies. In patients with small HCC, ethanol ablation was shownto be an effective treatment modality [10,11]. However, therole of chemical ablation in patients with metastatic disease islimited, because alcohol tends to spread preferentially intothe surrounding ‘‘soft’’ liver parenchyma as opposed toremaining within the higher density tumour mass [12].
The technique for percutaneous ethanol injection (PEI) issimilar whether used in the treatment of HCC or livermetastasis. The mechanism of action of ethanol and aceticacid ablation includes cellular dehydration, coagulativenecrosis, protein denaturation, and small-vessel thrombosis ofthe target lesion [13]. The low viscosity and limited ability tocontrol the distribution has remained a fundamental limita-tion. PEI can be performed under ultrasound or computedtomography guidance with monitored moderate sedation.Typically, a 20e22-gauge end-hole needle (Chiba) or conicaltip needle is used, more recently, 18-gauge multisided holeneedles were advocated [14]. Small lesions can beapproached by placing the needle at the most-distal aspect ofthe lesion with injection of ethanol during retraction, whereaslarger tumours require multiple repositionings of the needle,insertion of multiple needles, and/or multiple sessions. Thisprocedure is usually well tolerated by patients, with a repor-ted incidence of complications, less than 5% [15,16].
In addition to PEI, percutaneous acetic acid injection(PAI) with 50% acetic acid is another available option. Theprimary advantage with PAI is that the solution is able topenetrate the septae and the capsule of tumours, and, hence,a lower amount of acetic acid and fewer overall sessions areneeded compared with PEI to achieve the same results [17].Otherwise, the technique is similar to that of PEI. Overall,both PEI and PAI are safe, easy to perform procedures butwith limited indications because of the limitations in size andsite of treatable lesions, unpredictability of agent diffusion,and the inability to monitor the treatment area. Thus, PEI andPAI have been surpassed by newer ablative techniques, suchas RFA and cryoablation.
RFA
RFA is the most widely practiced ablative technology andis used in the management of patients with both primary andmetastatic liver disease. RFA relies on the generation ofhigh-frequency, alternating electrical currents within thetarget tissues, which results in ionic agitation. The frictionalforces lead to the generation of heat, which, in turn, results inthrombosis, thermally induced necrosis, protein denaturing,dehydration, coagulative necrosis, and apoptosis [18].Because of the small surface area of the needle electrode andthe large area of the ground pads, the heat generated isfocused in the area around the needle [19], with the amountof cell damage induced dependent on the temperature ach-ieved and the duration of treatment. The goal in RFA is toachieve target tissue temperatures of between 50�Ce100�Cfor 4e6 minutes, because this results in optimal cellularnecrosis and death [20].
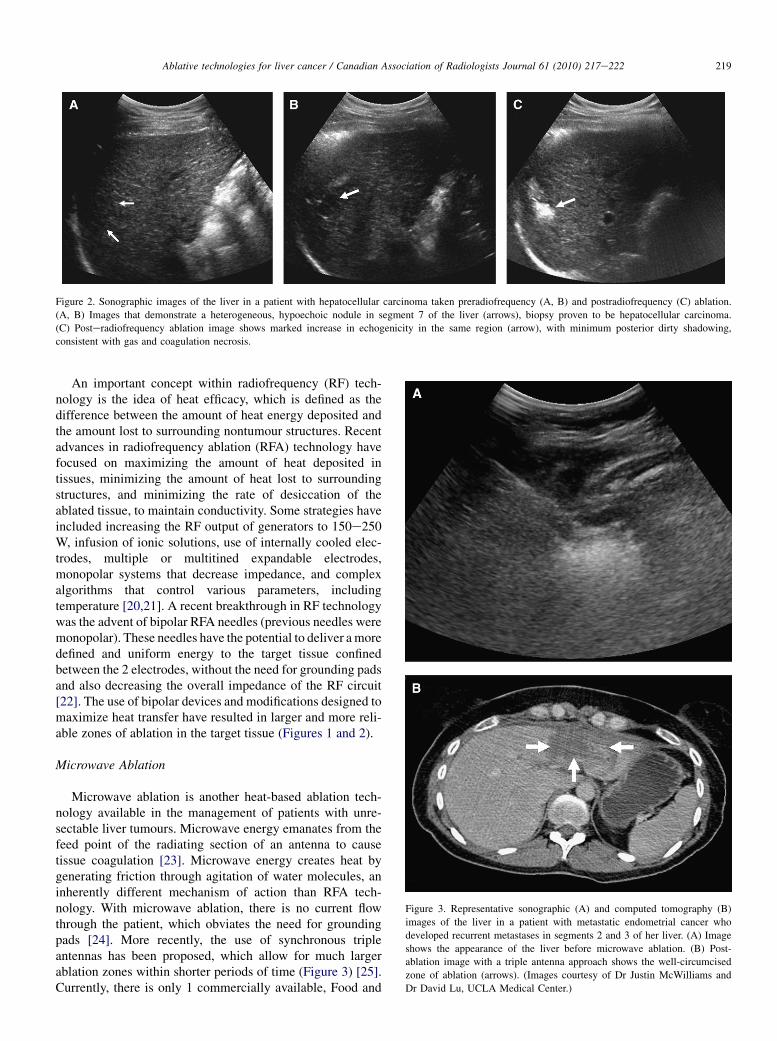
Figure 2. Sonographic images of the liver in a patient with hepatocellular carcinoma taken preradiofrequency (A, B) and postradiofrequency (C) ablation.
(A, B) Images that demonstrate a heterogeneous, hypoechoic nodule in segment 7 of the liver (arrows), biopsy proven to be hepatocellular carcinoma.
(C) Posteradiofrequency ablation image shows marked increase in echogenicity in the same region (arrow), with minimum posterior dirty shadowing,
consistent with gas and coagulation necrosis.
219Ablative technologies for liver cancer / Canadian Association of Radiologists Journal 61 (2010) 217e222
An important concept within radiofrequency (RF) tech-nology is the idea of heat efficacy, which is defined as thedifference between the amount of heat energy deposited andthe amount lost to surrounding nontumour structures. Recentadvances in radiofrequency ablation (RFA) technology havefocused on maximizing the amount of heat deposited intissues, minimizing the amount of heat lost to surroundingstructures, and minimizing the rate of desiccation of theablated tissue, to maintain conductivity. Some strategies haveincluded increasing the RF output of generators to 150e250W, infusion of ionic solutions, use of internally cooled elec-trodes, multiple or multitined expandable electrodes,monopolar systems that decrease impedance, and complexalgorithms that control various parameters, includingtemperature [20,21]. A recent breakthrough in RF technologywas the advent of bipolar RFA needles (previous needles weremonopolar). These needles have the potential to deliver a moredefined and uniform energy to the target tissue confinedbetween the 2 electrodes, without the need for grounding padsand also decreasing the overall impedance of the RF circuit[22]. The use of bipolar devices and modifications designed tomaximize heat transfer have resulted in larger and more reli-able zones of ablation in the target tissue (Figures 1 and 2).
Microwave Ablation
Figure 3. Representative sonographic (A) and computed tomography (B)
images of the liver in a patient with metastatic endometrial cancer who
developed recurrent metastases in segments 2 and 3 of her liver. (A) Image
shows the appearance of the liver before microwave ablation. (B) Post-
ablation image with a triple antenna approach shows the well-circumcised
zone of ablation (arrows). (Images courtesy of Dr Justin McWilliams and
Dr David Lu, UCLA Medical Center.)
Microwave ablation is another heat-based ablation tech-nology available in the management of patients with unre-sectable liver tumours. Microwave energy emanates from thefeed point of the radiating section of an antenna to causetissue coagulation [23]. Microwave energy creates heat bygenerating friction through agitation of water molecules, aninherently different mechanism of action than RFA tech-nology. With microwave ablation, there is no current flowthrough the patient, which obviates the need for groundingpads [24]. More recently, the use of synchronous tripleantennas has been proposed, which allow for much largerablation zones within shorter periods of time (Figure 3) [25].Currently, there is only 1 commercially available, Food and
220 N. A. Khan et al. / Canadian Association of Radiologists Journal 61 (2010) 217e222
Drug Administration approved product in this categorymarketed by Covidien (Boulder, CO), the Evident micro-wave ablation system, which was launched in 2008 [26].
Cryoablation
Cryoablation is an established ablation technique that isfundamentally different from the heat-based RFA andmicrowave ablation technologies. The technique itselfinvolves rapid freezing of the tissues to temperatures below0�C, which results in intra- and extracellular ice crystalformation and cellular damage by dehydration and destruc-tion of normal cellular architecture [24]. Liquid nitrogen wasused as the initial cryogen; however, this limited the tech-nology to the operative setting because the probe sizes weretoo large (in excess of 7 mm) [27]. The introduction of argongas based systems and smaller probe sizes that use theJoules-Thompson effect (with probes as small as 17 gauge)has made percutaneous use feasible [27].
In cryoablation, the number and placement of the probes isdependent on the tumour size. The ‘‘2 to 1’’ rule [28] outlinesthat multiple cryoprobes can be placed within 1 cm of thetumour edge, and there should not be more than a 2-cm gapbetween the probes. This configuration allows for synergisticachievement of target temperatures and maximal zones of celldeath, ideal in targeting large tumour masses and/or multipletumour masses concomitantly. The ability to place multipleprobes simultaneously is one potential advantage of cryoa-blation, because multiple probes may allow for the creation oflarger, synergistic zones of ablation compared with RFA in thetreatment of large hepatic masses (Figure 4) [27].
IRE
IRE is a novel, nonthermal ablation technology that hasyet to enter clinical practice. However, early in vitro and in
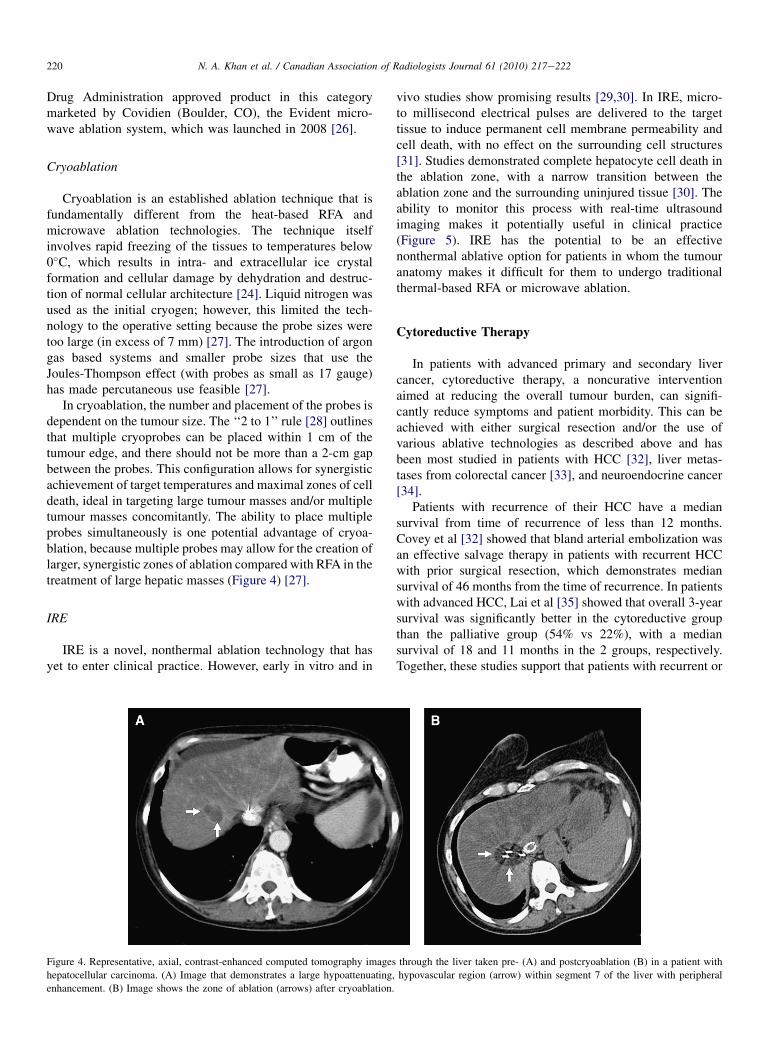
Figure 4. Representative, axial, contrast-enhanced computed tomography images
hepatocellular carcinoma. (A) Image that demonstrates a large hypoattenuating,
enhancement. (B) Image shows the zone of ablation (arrows) after cryoablation.
vivo studies show promising results [29,30]. In IRE, micro-to millisecond electrical pulses are delivered to the targettissue to induce permanent cell membrane permeability andcell death, with no effect on the surrounding cell structures[31]. Studies demonstrated complete hepatocyte cell death inthe ablation zone, with a narrow transition between theablation zone and the surrounding uninjured tissue [30]. Theability to monitor this process with real-time ultrasoundimaging makes it potentially useful in clinical practice(Figure 5). IRE has the potential to be an effectivenonthermal ablative option for patients in whom the tumouranatomy makes it difficult for them to undergo traditionalthermal-based RFA or microwave ablation.
Cytoreductive Therapy
In patients with advanced primary and secondary livercancer, cytoreductive therapy, a noncurative interventionaimed at reducing the overall tumour burden, can signifi-cantly reduce symptoms and patient morbidity. This can beachieved with either surgical resection and/or the use ofvarious ablative technologies as described above and hasbeen most studied in patients with HCC [32], liver metas-tases from colorectal cancer [33], and neuroendocrine cancer[34].
Patients with recurrence of their HCC have a mediansurvival from time of recurrence of less than 12 months.Covey et al [32] showed that bland arterial embolization wasan effective salvage therapy in patients with recurrent HCCwith prior surgical resection, which demonstrates mediansurvival of 46 months from the time of recurrence. In patientswith advanced HCC, Lai et al [35] showed that overall 3-yearsurvival was significantly better in the cytoreductive groupthan the palliative group (54% vs 22%), with a mediansurvival of 18 and 11 months in the 2 groups, respectively.Together, these studies support that patients with recurrent or
through the liver taken pre- (A) and postcryoablation (B) in a patient with
hypovascular region (arrow) within segment 7 of the liver with peripheral
Figure 5. Sonographic images through the liver in a swine model, before (A) and after (B) irreversible electroporation (IRE) embolization. (A) Image
demonstrates the positioning of the probes (arrows). (B) Post-IRE image shows the hypoechoic ablation zone (arrows). (Images courtesy of Dr Edward W. Lee,
UCLA Medical Center.)
221Ablative technologies for liver cancer / Canadian Association of Radiologists Journal 61 (2010) 217e222
advanced HCC disease may still derive a survival benefitfrom further cytoreductive measures.
Patients with liver metastases from colorectal cancer oftendevelop recurrence of their liver metastases after surgicalresection. In these patients, repeated hepatic resection wasshown to improve survival [36,37]. Results of other studieshave supported a role for surgery after downstaging of theinitial unresectable liver tumours with various forms ofchemotherapy, including intra-arterial chemotherapy [38]. Inselected patients with advanced, extrahepatic disease, liverresection has also been shown to increase survival, whichdisputes the earlier notion that extrahepatic disease should bean absolute contraindication for liver resection in thesepatients [39]. Substituting surgical resection with invasivepercutaneous RFA in the treatment of hepatic colorectalcarcinoma liver metastases may also provide a survivalbenefit [40].
Finally, in patients with hepatic neuroendocrine meta-static disease, cytoreductive therapies can play a major rolein helping to reduce the degree of symptomatic endo-crinopathies. McEntee et al [34] found that cytoreductivehepatic surgery produced complete relief of symptoms in 24of 26 patients who were symptomatic either from theprimary tumour or an associated endocrinopathy. Morerecently, the National Comprehensive Cancer Networkpublished its guidelines and outlined the role of variousablation technologies in the overall management of patientswith liver metastases from advanced primary neuroendocrinetumours [41].
Summary
Interventional ablative technologies have played anincreasingly important role in the optimal management ofpatients with primary and secondary hepatic malignancies.RFA is the most widely practiced of the ablative technolo-gies; however, other options, such as microwave ablation orcryoablation, are also available. IRE is a relatively newablative technology that will likely soon enter clinical
practice and offer another option to the interventional radi-ologist. In addition to their role as first- and second-linetreatment options, recent studies have also expanded therole of these technologies as cytoreductive therapies inpatients with noncurative, advanced disease. Cytoreductiveablation can reduce overall disease burden and improvemorbidity.
References
[1] El-Serag HB, Mason AC. Rising incidence of hepatocellular carcinoma
in the United States. N Engl J Med 1999;340:745e50.
[2] Mazzaferro V, Chun YS, Poon RT, et al. Liver transplantation for
hepatocellular carcinoma. Ann Surg Oncol 2008;15:1001e7.
[3] Sutherland LM, Williams J, Padbury R, et al. Radiofrequency ablation
of liver tumors: a systemic review. Arch Surg 2006;141:181e90.
[4] Pawlik TM, Choti MA. Surgical therapy for colorectal metastasis to the
liver. J Gastrointest Surg 2007;11:1057e77.
[5] Abdalla EK, Vauthey JN, Ellis LM, et al. Recurrence and outcomes
following hepatic resection, radiofrequency ablation, and combined
resection/ablation for colorectal liver metastases. Ann Surg 2004;239:
818e25.
[6] Tabernero J, Van Cutsem E, Dıaz-Rubio E. Phase II trial of cetuximab
in combination with fluorouracil, leucovorin, and oxaliplatin in the
first-line treatment of metastatic colorectal cancer. J Clin Oncol 2007;
25:5225e32.
[7] Moehler M, Sprinzl MF, Abdelfattah M, et al. Capecitabine and iri-
notecan with and without bevacizumab for advanced colorectal cancer
patients. World J Gastroenterol 2009;15:449e56.
[8] Lencioni R, Crocetti L, Cioni D, et al. Percutaneous radiofrequency
ablation of hepatic colorectal metastases: technique, indications,
results, and new promises. Invest Radiol 2004;39:689e97.
[9] Siperstein AE, Berber E, Ballem N, et al. Survival after radiofrequency
ablation of colorectal liver metastases: 10-year experience. Ann Surg
2007;246:559e65.
[10] Livraghi T, Giorgio A, Marin G, et al. Hepatocellular carcinoma and
cirrhosis in 746 patients: long-term results of percutaneous ethanol
injection. Radiology 1995;197:101e8.
[11] Shiina S, Tagawa K, Niwa Y, et al. Percutaneous ethanol injection
therapy for hepatocellular carcinoma: results in 146 patients. AJR Am J
Roentgenol 1993;160:1023e8.
[12] Amin Z, Bown SG, Lees WR. Local treatment of colorectal liver
metastasis: a comparison of interstitial laser photocoagulation (ILP)
and percutaneous alcohol injection (PAI). Clin Radiol 1993;48:
166e71.
222 N. A. Khan et al. / Canadian Association of Radiologists Journal 61 (2010) 217e222
[13] Giovannini M. Percutaneous alcohol ablation for liver metastasis.
Semin Oncol 2002;29:192e5.
[14] Clark TW. Chemical ablation of Liver cancer. Tech Vasc Interv Radiol
2007;10:58e63.
[15] Di Stasi M, Buscarini L, Livraghi T, et al. Percutaneous ethanol
injection in the treatment of hepatocellular carcinoma. A multi-center
survey of evaluation practices and complication rates. Scand J Gas-
troenterol 1997;32:1168e73.
[16] Gelczer RK, Charboneau JW, Hussain S, et al. Complications of
percutaneous ethanol ablation. J Ultrasound Med 1998;17:531e3.
[17] Ohnishi K, Nomura F, Ito S, et al. Prognosis of small hepatocellular
carcinoma (less than 3 cm) after percutaneous acetic acid injection:
study of 91 cases. Hepatology 1996;23:994e1002.
[18] Rhim H, Goldberg SN, Dodd III GD, et al. Essential techniques for
more successful radio-frequency thermal ablation of malignant hepatic
tumors. Radiographics 2001;21:17e35.
[19] Goldberg SN, Gazelle GS, Mueller PR. Thermal ablation therapy for
focal malignancies: a unified approach to underlying principles, tech-
niques, and diagnostic imaging guidance. AJR Am J Roentgenol 2000;
174:323e31.
[20] Lencioni R, Crocetti L. Radiofrequency ablation of liver cancer. Tech
Vasc Interv Radiol 2007;10:38e46.
[21] Solbiati L, Goldberg SN, Ierace T, et al. Hepatic metastasis: percuta-
neous radiofrequency ablation with cooled-tip electrodes. Radiology
1997;205:367e73.
[22] Eisele RM, Neuhaus P, Schumacher G. Radiofrequency ablation of
liver tumors using a novel bipolar device. J Laparoendosc Adv Surg
Tech A 2008;18:857e63.
[23] Garcea G, Llyod TD, Aylott C, et al. The emergent role of focal liver
ablation techniques in the treatment of primary and secondary liver
tumors. Eur J Cancer 2003;39:2150e64.
[24] Gannon CJ, Curley SA. The role of focal liver ablation in the treatment
of unresectable primary and secondary malignant liver tumors. Semin
Radiat Oncol 2005;15:265e72.
[25] Simon CJ, Dupuy DE, Iannitti DA, et al. Intraoperative triple
antenna hepatic microwave ablation. AJR Am J Roentgenol 2006;
187:w333e40.
[26] Refer to product monograph.
[27] Hinshaw JL, Lee FT. Cryoablation for liver cancer. Tech Vasc Interv
Radiol 2007;10:47e57.
[28] Wang H, Littrup PJ, Duan Y, et al. Thoracic masses treated with
percutaneous cryotherapy: initial experience with more than 200
procedures. Radiology 2005;235:289e98.
[29] Miller L, Leor J, Rubinsky B. Cancer cells ablation with irreversible
electroporation. Technol Cancer Res Treat 2005;4:699e705.
[30] Lee EW, Loh CT, Kee ST. Imaging guided percutaneous irreversible
electroporation: ultrasound and immunohistological correlation. Tech-
nol Cancer Res Treat 2007;6:287e94.
[31] Rubinsky B, Onik G, Mikus P. Irreversible electroporation: a new
ablation modalitydclinical implications. Technol Cancer Res Treat
2007;6:37e48.
[32] Covey AM, Maluccio MA, Schubert J, et al. Particle embolization of
recurrent hepatocellular carcinoma after hepatectomy. Cancer 2006;
106:2181e9.
[33] Meric F, Patt YZ, Curley SA, et al. Surgery after downstaging of
unresectable hepatic tumors with intra-arterial chemotherapy. Ann Surg
Oncol 2000;7:490e5.
[34] McEntee GP, Nagorney DM, Kvols LK, et al. Cytoreductive hepatic
surgery for neuroendocrine tumors. Surgery 1990;108:1091e6.
[35] Lai EC, Tang CN, Ha JP, et al. Cytoreductive surgery in multidisci-
plinary treatment of advanced hepatocellular carcinoma. ANZ J Surg
2008;78:504e7.
[36] Hamy A, Bennouna J, Heymann MF, et al. Repeat hepatectomy for
colorectal liver metastases. Int Surg 2005;90:189e97.
[37] Morise Z, Sugioka A, Fujita J, et al. Does repeated surgery improve the
prognosis of colorectal liver metastases? J Gastrointest Surg 2006;10:
6e11.
[38] Meric F, Patt YZ, Curley SA, et al. Surgery after downstaging of
unresectable hepatic tumors with intra-arterial chemotherapy. Ann Surg
Oncol 2000;7:490e5.
[39] Carpizo DR, Are C, Jarnagin W, et al. Liver resection for metastatic
colorectal cancer in patients with concurrent extrahepatic disease:
results in 127 patients treated at a single center. Ann Surg Oncol 2009;
16:2138e46.
[40] Gillams AR, Lees WR. Five-year survival in 309 patients with colo-
rectal liver metastases treated with radiofrequency ablation. Eur Radiol
2009;19:1206e13.
[41] Clark OH, Benson 3rd AB, Berlin JD, et al. NCCN Clinical Practice
Guidelines in Oncology: neuroendocrine tumors. J Natl Compr Canc
Netw 2009;7:712e47.

![Erasmus 2012 benign liver [Alleen-lezen] · B. Secondary benign liver lesions 1. Abscess C. Hepatic Pseudolesions 1. Focal Steatosis, Focal spared Area in Fatty Liver 2. ... • Incidental](https://img.pdfslide.us/doc/110x75/5b0382477f8b9a2e228c816d/erasmus-2012-benign-liver-alleen-lezen-secondary-benign-liver-lesions-1-abscess.jpg)