Embed Size (px)
Citation preview

PICTURES IN DIGESTIVE PATHOLOGY
Liver metastasis secondary to primary mesenteric carcinoidJosé Francisco Juanmartiñena-Fernández1,2, Ignacio Fernández-Urién1,2, Irene Amat-Villegas3 and Carlos Prieto-Martínez2
Departments of 1Endoscopy, 2Digestive Diseases, and 3Pathology. Complejo Hospitalario de Navarra. Pamplona, Spain
1130-0108/2017/109/3/211-212Revista española de enfeRmedades digestivas© Copyright 2017. sepd y © ARÁN EDICIONES, S.L.
Rev esp enfeRm dig2017, Vol. 109, N.º 3, pp. 211-212
CASE REPORT
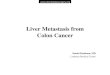
A 66 year-old male presented a one-year period of abdominal pain, iron-deficiency anemia and diarrhea. Computed tomography showed in portal phase a mesenteric mass with three liver metastasis and locoregional adenopa-thies (Fig. 1A and B). After fine needle aspiration (18G) of one metastatic lesion, multiple neoplastic cells with posi-tive immunohistochemistry markers for chromogranin and synaptophysin were identified. The Ki-67 proliferation rate was < 2%, and only 1 mitoses/10 HPF was detected (Fig. 2A-C). Normal values of 5-hydroxyindoleacetic acid in 24 h-urinary excretion and serum levels of chromogranin-A were detected. No other metastatic lesions were identified on octreoscan examination (Fig. 3 A and B). Therefore, metastatic primary mesenteric carcinoid tumor was the final pathological diagnosis. After two months of treatment with somatostatin analogs (Sandostatin® 30 mg/24 h) symptoms had improved, the diarrhea had disappeared and the disease was considered to be under control.
Fig. 1. A. Typical presentation of extra-digestive carcinoid tumor: heterogeneous, starry mass of soft tissue with central calcifications in the mesentery. B. Liver metastatic lesions enhanced in portal phase.
DISCUSSION
Carcinoid tumors are rare, slow-growing neoplasms that display neuroendocrine properties. The term carcinoid is generally applied to well-differentiated neoplasms, while neuroendocrine carcinoma is reserved only for poorly differentiated lesions. They can be found throughout the different regions of the gastrointestinal system, although they have predilection for the ileum (1). They often present an indolent growth and tend to infiltrate the gastrointesti-nal wall, extending to the mesentery in 40-80% of cases. Thus, solid neoplasms arising in the mesentery are usually metastatic lesions, while primary neoplastic involvement is extremely infrequent. Delayed diagnosis occurs frequently, typically 5-7 years from initial onset of symptoms, with 60-80% of patients diagnosed at an advanced stage (2). Surgical resection is generally preferred for patients with potentially resectable disease, while somatostatin analogs are the first line treatment for unresectable symptomatic disease (3).

212 J. F. JUANMARTIÑENA-FERNÁNDEZ ET AL. Rev esp enfeRm Dig
Rev esp enfeRm Dig 2017;109(3):211-212
Fig. 2. A. Neuroendocrine tumor infiltrates liver parenchyma (right side of the picture). Note the uniformity and organoid pattern. Tumor islands are separated by a delicate fibrous stroma (H-E x 200). B. Diffuse and granular cytoplasmatic staining for chromogranin in the tumor cells but not in hepa-tocytes (x200). C. Intense diffuse staining for synaptophysin, a neuroendocrine differentiation marker (x200).
Fig. 3. Octreoscan ruled out other lesions, confirming data obtained by computed tomography. A. Liver metastasis. B. Primary mesenteric carcinoid.
REFERENCES
1. Yamanuha J, Ballinger R, Coon D, et al. Carcinoid tumor presenting as a primary mesenteric mass: A case report and review of the literature. Hawaii Med J 2009;68:137-9.
2. Schimmack S, Svejda B, Lawrence B, el al. The diversity and commonalities of gastroenteropancreatic neuroendocrine tumors.
Langenbecks Arch Surg 2011;396:273-98. DOI: 10.1007/s00423-011-0739-1
3. Marazuela M, Bernabeu I. Tratamiento farmacológico de los tumores neuroendocrinos gastroenteropancreáticos: análogos de somatostatina. Endocrinol Nutr 2007;54:44-50.