Embed Size (px)
Citation preview

1
First report of ceftazidime-avibactam resistance in a KPC-3 expressing Klebsiella 1 pneumoniae 2 3 Romney M. Humphries1*, Shangxin Yang1, Peera Hemarajata1, Kevin W. Ward1, Janet A. 4 Hindler1, Shelley A. Miller1 and Aric Gregson2 5 6 1Department of Pathology & Laboratory Medicine, University of California, Los Angeles, 7 USA 8 9 2 Department of Medicine, Division of Infectious Diseases, University of California, Los 10 Angeles, USA 11 12 Keywords: KPC, ceftazidime-avibactam, resistance 13 14 Running Title: Ceftazidime-avibactam resistance 15 16 *corresponding author: 17 18 Romney M. Humphries 19 11633 San Vicente Blvd 20 Los Angeles, CA 90049 21 310-794-3614 (phone) 22 310-794-2765 (fax) 23 [email protected] 24 25 *alternate author: 26 Janet Hindler 27 11633 San Vicente Blvd 28 Los Angeles, CA 90049 29 310-794-2763 (phone) 30 310-794-2765 (fax) 31 [email protected] 32 33 34 35
AAC Accepted Manuscript Posted Online 20 July 2015Antimicrob. Agents Chemother. doi:10.1128/AAC.01165-15Copyright © 2015, American Society for Microbiology. All Rights Reserved.
on June 5, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
2
Abstract 36 Ceftazidime-avibactam is the first antimicrobial approved by U.S. FDA for 37 treatment of carbapenem-resistant Enterobacteriaceae. Avibactam, a non-β-lactam β-38 lactamase inhibitor, inactivates class A serine carbapenemases, including KPC. We 39 report a case of a ceftazidime-avibactam resistant (MIC, 32/4 µg/mL) KPC-producing 40 Klebsiella pneumoniae, isolated from a patient with no prior treatment with 41 ceftazidime-avibactam. 42 43 Text 44 45 The emergence of carbapenemase-producing Enterobacteriacae (CPE) is a critical 46 threat to public health. Carbapenemases described in CPE are classified into three 47 functional groups: class A serine carbapenemases (including the Klebsiella pneumoniae 48 carbapenemase, KPC), class B metallo-β-lactamases (including the New Delhi β-49 lactamase, NDM) and class D β-lactamases (including the OXA-48-like enzymes) [1]. In 50 the United States, the CPE epidemic is almost exclusively driven by K. pneumoniae 51 isolates that produce KPC [2]. KPC efficiently hydrolyses the carbapenems, as well as the 52 extended-spectrum cephalosporins and aztreonam [1], and is resistant to the β-53 lactamase inhibitors clavulanic acid, tazobactam and sulbactam [3]. The KPC gene, 54 blaKPC, is located on a transmissible plasmid that also harbors resistant determinants for 55 several other antimicrobial classes. As such, isolates are often resistant to all agents 56 commonly used for Gram negative bacteria, with the exception of gentamicin or 57
on June 5, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

3
amikacin, for which variable susceptibility exists [4]. Resistance to the polymyxins 58 (colistin and polymyxin B) and tigecycline has been reported for these isolates [2], 59 making the management of patients with serious infections caused by CPE exceedingly 60 difficult. 61
In late 2014, the U.S. Food and Drug Administration (FDA) approved ceftazidime-62 avibactam (Avycaz®), for the treatment of complicated urinary tract infections and, 63 when combined with metronidazole, complicated intra-abdominal infections caused by 64 CPE and other multi-drug resistant Gram-negative bacteria. Avibactam is a novel non-β-65 lactam β-lactamase inhibitor that inactivates class A serine carbapenemases (including 66 KPC). The MIC50 and MIC90 for KPC-producing Enterobacteriaceae were recently 67 reported as 1/4 and 4/4 µg/ml, respectively, for a collection of 120 isolates recovered in 68 2013 from hospitals across the U.S. [5]. Avibactam does not inhibit the activity of the 69 class B, and has only variable activity against the class D, β-lactamases [6]. No clinical 70 isolates of KPC-producing K. pneumoniae have been reported to date that are resistant 71 to ceftazidime-avibactam, despite extensive surveillance programs of this drug’s 72 potency [2, 5]. Herein, we report the first case of a KPC-producing K. pneumoniae 73 resistant to ceftazidime-avibactam. This isolate was recovered from a patient with no 74 prior history of ceftazidime-avibactam therapy. 75 76 Case Report 77
A 62 year-old woman with a past medical history of splenic vein thrombosis, 78 status post splenectomy, and locally advanced pancreatic cancer, status post 79
on June 5, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
4
chemotherapy and radiation, underwent a pylorus preserving 80 pancreaticoduodenectomy at our institution. She was discharged home two weeks after 81 the operation. Seven days later, she presented to an outside hospital with vomiting and 82 fever to 102°F. An abdominal CT scan revealed rim-enhancing periductal fluid collections 83 in the central liver and left hepatic lobe, measuring up to 2 cm, suggestive of cholangitic 84 abscesses, and inflammatory ascites of new onset. The patient was transferred back to 85 our hospital for higher level of care. On admission, she was started on vancomycin 1g IV 86 q12 hours and piperacillin-tazobactam 3.375g q8 hours infused over four hours. White 87 blood cell count was 22,000/µL, hemoglobin 10.0 g/dL, and lactate 19 mg/dL. Two of 88 three blood cultures drawn on the day of admission grew Citrobacter freundii (resistant 89 only to ampicillin and ampicillin-sulbactam, data not shown) and a carbapenem-90 resistant K. pneumoniae (CRKP). At this time, antimicrobial therapy was changed to 91 gentamicin 7mg/kg IV q24 hours and cefepime 2g q8 hours. Over the next 6 days, 3 92 additional blood cultures grew a CRKP. Gentamicin and cefepime were discontinued in 93 favor of colistin 300mg load then 150mg q12 hours, meropenem 2g q8 hours infused 94 over four hours and tigecycline 100mg q12 hours, when resistance to cefepime was 95 confirmed. Altered mental status and worsening kidney injury, presumably due to the 96 combined effects of gentamicin, colistin and sepsis, required admission to the intensive 97 care unit and initiation of continuous renal replacement therapy for volume overload 98 and metabolic acidosis. At this time, our Institutional Review Board and Actavis were 99 contacted to obtain ceftazidime-avibactam for compassionate use. While no further 100
on June 5, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
5
blood cultures were positive for CRKP, CRKP was isolated from her hepatic drain on 101 hospital day 17. 102
Antimicrobial susceptibility testing was performed according to the Clinical and 103 Laboratory Standards Institute standards [7] with MIC testing done on panels prepared 104 in-house. Ceftazidime-avibactam was tested by both broth microdilution and disk 105 diffusion, using research-use only (RUO) labeled reagents provided by AztraZeneca 106 (London, UK). Ceftazidime-avibactam was tested using a constant concentration of 107 avibactam (4 μg/mL). MIC results were interpreted according to CLSI M100-S25 108 breakpoints [8], with the exception of tigecycline and ceftazidime-avibactam, which 109 were interpreted according to the FDA-cleared breakpoints. Colistin MICs were 110 interpreted using the EUCAST Enterobacteriaceae breakpoint of <4 μg/mL to indicate 111 susceptibility. 112
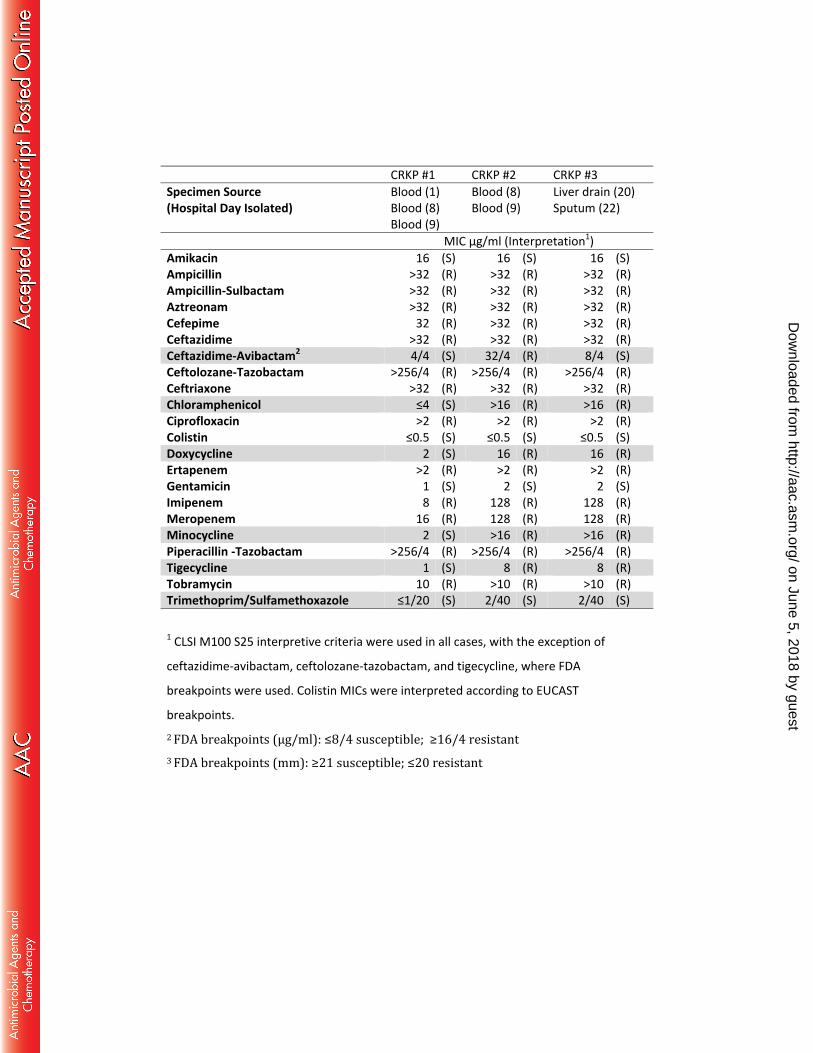
Results of susceptibility testing are presented in the Table, and yielded 3 113 different susceptibility patterns for the CRKP isolates (Table). All three were resistant to 114 the extended-spectrum cephalosporins and aztreonam, the carbapenems, ampicillin-115 sulbactam, piperacillin-tazobactam, ciprofloxacin, and tobramycin. All three isolates 116 were susceptible to amikacin, gentamicin, colistin and trimethoprim-sulfamethoxazole. 117 Surprisingly, CRKP-2 was resistant to ceftazidime-avibactam, both by disk (19 mm) and 118 MIC (32/4 µg/ml), a result confirmed by an outside reference laboratory (JMI, North 119 Liberty, Iowa). In addition, CRKP-2 was resistant to chloramphenicol and doxycycline, 120 minocycline and tigecycline, whereas CRKP-1 was susceptible to these agents. Isolate 121 CRKP-3 was similarly resistant to chloramphenicol and the tetracyclines, but susceptible 122
on June 5, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

6
to ceftazidime-avibactam. The isolates were tested for the presence of carbapenemases 123 using a laboratory-developed PCR assay that targets blaKPC, blaNDM-1, blaVIM, blaIMP, 124 blaOXA-48 and blaSME. blaKPC was the sole carbapenemase detected in the isolates. The KPC 125 gene was sequenced, revealing 100% homology to blaKPC-3 [9]. 126 We determined the MIC of CRKP-2 to meropenem-avibactam, which was tested 127 in doubling dilutions of meropenem at concentrations of 0.06 – 32 μg/mL and a 128 constant concentration of 4 µg/mL avibactam. The meropenem-avibactam MIC was 129 0.06/4 μg/mL, whereas the MIC for meropenem alone was >32 μg/mL. These data 130 further support that our isolate does not also harbor a class B metallo-β-lactamase, as 131 was reported elsewhere for a ceftazidime-avibactam resistant isolate that expressed 132 both blaKPC-2 and the metallo-β-lactamase gene, blaVIM-4 [5]. The addition of the efflux 133 pump inhibitor, phenyl-arginine β-naphthylamide, at 40 μg/mL did not result in 134 decrease in the ceftazidime-avibactam MIC of any of the patient’s isolates, suggesting 135 efflux is not the mechanism for resistance in this isolate. 136 On hospital day 21, ceftazidime-avibactam (2.5g q12 hours) was added to 137 meropenem 1g q8 hours, tigecycline 100mg q12 hours and polymyxin B 15,000U/kg q12 138 hours. The patient continued with an ICU stay complicated by intermittent altered 139 mental status, hypotension, continuous renal replacement therapy and two episodes of 140 respiratory failure, one of which was associated with CRKP in the respiratory culture and 141 multifocal pulmonary infiltrates. She continues treatment for ongoing hepatic abscesses 142 with IV trimethoprim-sulfamethoxazole 10mg/kg/day divided q12 hours and polymyxin 143 B 15,000U/kg q12 hours, with no further isolation of CRKP. 144
on June 5, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
7
Discussion 145 CPE were identified by the U.S. Centers for Disease Control and Prevention as 146 the highest priority for novel antimicrobial development in 2011. Despite this call to 147 arms, ceftazidime-avibactam is the only antimicrobial approved by the U.S. FDA for the 148 treatment of CPE. Importantly, ceftazidime-avibactam was approved via an expedited 149 process based on phase II data as part of the Generating Antibiotics Incentives Now 150 (GAIN) Act, and little clinical experience exists for the use of this antimicrobial for the 151 treatment of CPE. In this report, we document the first case of ceftazidime-avibactam 152 resistance in a KPC-producing K. pneumoniae, the most common CPE in the U.S. 153 Importantly, this isolate was recovered in February 2015, prior to the widespread 154 availability of ceftazidime-avibactam in the U.S., and in a patient with no prior 155 ceftazidime-avibactam treatment. 156
The resistance mechanism for ceftazidime-avibactam is currently under 157 investigation for this isolate, but does not appear related to mutation of blaKPC-3. 158 Avibactam-resistant variants of KPC-2 have been engineered through directed 159 mutagenesis of sites critical to avibactam’s activity. These mutations also abolished KPC-160 2’s ability to hydrolyze ceftazidime, and as a result, isolates transformed with these 161 engineered KPCs were susceptible to the ceftazidime component of the combination 162 [10]. Similarly, mutations to the class A SHV and CTX-M-15 β-lactamases have been 163 documented that confer resistance to avibactam, but again these mutations abolished 164 ceftazidime hydrolysis [11, 12]. Nonetheless, it is theoretically possible that a 165 combination of mutations to avibactam’s target site could result in both resistance to 166
on June 5, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
8
avibactam and to ceftazidime as a result of ceftazidime hydrolysis. Efflux and porin 167 mutations have been associated with ceftazidime-avibactam resistance in Pseudomonas 168 aeruginosa and Enterobacter cloacae [13-15]. The concomitant tetracycline resistance in 169 our isolate suggested efflux as a plausible explanation for the resistance mechanism, 170 since tetracycline resistance is commonly mediated by increased efflux in the 171 Enterobacteriaceae; however, the addition of phenyl-arginine β-naphthylamide did not 172 affect the ceftazidime-avibactam MIC. 173 174
A significant challenge to the clinical use of ceftazidime-avibactam is the current 175 lack of FDA-cleared susceptibility tests for this antimicrobial and it is unlikely that these 176 tests will be available in the short term. Research-use-only (RUO) disks and Etest strips 177 (bioMerieux, Durham NC) are available by request from Allergan, but the reliability of 178 these is unknown. Furthermore, per FDA regulations, laboratories that choose to use 179 RUO tests must sign a waiver indicating they will not release results of testing for 180 patient care. Because ceftazidime-avibactam resistance in KPC-expressing CPE was 181 hitherto unreported, confirmation of the KPC gene has been suggested as a means to 182 predict susceptibility to ceftazidime-avibactam among CRE. However, isolates resistant 183 to ceftazidime-avibactam due to the production of both KPC and class B metallo-β-184 lactamase may be undetected if laboratories only target KPC by PCR [8]. Furthermore, 185 few laboratories test for carbapenemase production using phenotypic tests, which are 186 no longer recommended as part of routine clinical testing by the CLSI [8]. Regardless, 187 our case clearly demonstrates that it is prudent to test for ceftazidime-avibactam 188
on June 5, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
9
susceptibility using MIC or disk diffusion tests, even in isolates that are positive for KPC 189 and negative for metallo-β-lactamases. This is particularly important if ceftazidime-190 avibactam may be used as monotherapy for KPC CRE infections. 191 192 Acknowledgements: The authors thank Helio Sader for confirmatory ceftazidime-193 avibactam testing, and Olga Lomovskaya for advice on efflux inhibitor testing. This study 194 was internally funded. 195 196
on June 5, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
10
References 197 1. Bush K. Proliferation and significance of clinically relevant beta-lactamases. 198 Annals of the New York Academy of Sciences 2013; 1277: 84-90. 199 2. Castanheira M, Farrell SE, Krause KM, Jones RN, Sader HS. Contemporary 200 diversity of beta-lactamases among Enterobacteriaceae in the nine U.S. 201 census regions and ceftazidime-avibactam activity tested against isolates 202 producing the most prevalent beta-lactamase groups. Antimicrobial Agents 203 and Chemotherapy 2014; 58(2): 833-8. 204 3. Papp-Wallace KM, Bethel CR, Distler AM, Kasuboski C, Taracila M, Bonomo 205 RA. Inhibitor resistance in the KPC-2 beta-lactamase, a preeminent property 206 of this class A beta-lactamase. Antimicrobial Agents and Chemotherapy 207 2010; 54(2): 890-7. 208 4. Pollett S, Miller S, Hindler J, Uslan D, Carvalho M, Humphries RM. Phenotypic 209 and molecular characteristics of carbapenem-resistant Enterobacteriaceae in 210 a health care system in Los Angeles, California, from 2011 to 2013. Journal of 211 Clinical Microbiology 2014; 52(11): 4003-9. 212 5. Castanheira M, Mills JC, Costello SE, Jones RN, Sader HS. Ceftazidime-213 avibactam activity tested against Enterobacteriaceae from United States 214 hospitals (2011-2013) and characterization of beta-lactamase producing 215 strains. Antimicrobial Agents and Chemotherapy 2015. 59 (7): 3509-17. 216 6. Mushtaq S, Warner M, Williams G, Critchley I, Livermore DM. Activity of 217 chequerboard combinations of ceftaroline and NXL104 versus beta-218
on June 5, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
11
lactamase-producing Enterobacteriaceae. The Journal of Antimicrobial 219 Chemotherapy 2010; 65(7): 1428-32. 220 7. CLSI. M07-A10. Method for Dilution Antimicrobial Susceptibility Tests for 221 Bacteria That Grow Aerobicaly; Approved Standard - Tenth Edition. Wayne, 222 PA: Clinical and Laboratory Standards Institue, 2015. 223 8. CLSI. M100-S25. Performance Standards for Antimicrobial Susceptibility 224 Testing; Twenty-Fifth Informational Supplement. Wayne, PA: Clinical and 225 Laboratory Standards Institue, 2015. 226 9. Woodford N, Tierno PM, Jr., Young K, et al. Outbreak of Klebsiella pneumoniae 227 producing a new carbapenem-hydrolyzing class A beta-lactamase, KPC-3, in a 228 New York Medical Center. Antimicrobial Agents and Chemotherapy 2004; 229 48(12): 4793-9. 230 10. Papp-Wallace KM, Winkler ML, Taracila MA, Bonomo RA. Variants of the 231 KPC-2 beta-lactamase which are resistant to inhibition by avibactam. 232 Antimicrobial Agents and Chemotherapy 2015. 59(7):3710-7. 233 11. Winkler ML, Papp-Wallace KM, Taracila MA, Bonomo RA. Avibactam and 234 inhibitor resistant SHV beta-lactamases. Antimicrobial Agents and 235 Chemotherapy 2015. 59(7):3700-9. 236 12. Livermore DM, Mushtaq S, Barker K, Hope R, Warner M, Woodford N. 237 Characterization of beta-lactamase and porin mutants of Enterobacteriaceae 238 selected with ceftaroline + avibactam (NXL104). The Journal of Antimicrobial 239 Chemotherapy 2012; 67(6): 1354-8. 240
on June 5, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

12
13. Lahiri SD, Johnstone MR, Ross PL, McLaughlin RE, Olivier NB, Alm RA. 241 Avibactam and class C beta-lactamases: mechanism of inhibition, 242 conservation of the binding pocket, and implications for resistance. 243 Antimicrobial Agents and Chemotherapy 2014; 58(10): 5704-13. 244 14. Winkler ML, Papp-Wallace KM, Hujer AM, et al. Unexpected challenges in 245 treating multidrug-resistant Gram-negative bacteria: resistance to 246 ceftazidime-avibactam in archived isolates of Pseudomonas aeruginosa. 247 Antimicrobial Agents and Chemotherapy 2015; 59(2): 1020-9. 248 15. Lahiri SD, Giacobbe RA, Johnstone MR, Alm RA. Activity of avibactam against 249 Enterobacter cloacae producing an extended-spectrum class C beta-250 lactamase enzyme. The Journal of Antimicrobial Chemotherapy 2014; 251 69(11): 2942-6. 252 253 254 on June 5, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

Table. Antimicrobial susceptibility results for K. pneumoniae isolates
on June 5, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
CRKP #1 CRKP #2 CRKP #3 Specimen Source (Hospital Day Isolated)
Blood (1) Blood (8) Blood (9)
Blood (8) Blood (9)
Liver drain (20) Sputum (22)
MIC µg/ml (Interpretation1) Amikacin 16 (S) 16 (S) 16 (S) Ampicillin >32 (R) >32 (R) >32 (R) Ampicillin-Sulbactam >32 (R) >32 (R) >32 (R) Aztreonam >32 (R) >32 (R) >32 (R) Cefepime 32 (R) >32 (R) >32 (R) Ceftazidime >32 (R) >32 (R) >32 (R) Ceftazidime-Avibactam2 4/4 (S) 32/4 (R) 8/4 (S) Ceftolozane-Tazobactam >256/4 (R) >256/4 (R) >256/4 (R) Ceftriaxone >32 (R) >32 (R) >32 (R) Chloramphenicol ≤4 (S) >16 (R) >16 (R) Ciprofloxacin >2 (R) >2 (R) >2 (R) Colistin ≤0.5 (S) ≤0.5 (S) ≤0.5 (S) Doxycycline 2 (S) 16 (R) 16 (R) Ertapenem >2 (R) >2 (R) >2 (R) Gentamicin 1 (S) 2 (S) 2 (S) Imipenem 8 (R) 128 (R) 128 (R) Meropenem 16 (R) 128 (R) 128 (R) Minocycline 2 (S) >16 (R) >16 (R) Piperacillin -Tazobactam >256/4 (R) >256/4 (R) >256/4 (R) Tigecycline 1 (S) 8 (R) 8 (R) Tobramycin 10 (R) >10 (R) >10 (R) Trimethoprim/Sulfamethoxazole ≤1/20 (S) 2/40 (S) 2/40 (S) 1 CLSI M100 S25 interpretive criteria were used in all cases, with the exception of
ceftazidime-avibactam, ceftolozane-tazobactam, and tigecycline, where FDA
breakpoints were used. Colistin MICs were interpreted according to EUCAST
breakpoints. 2 FDA breakpoints (µg/ml): ≤8/4 susceptible; ≥16/4 resistant 3 FDA breakpoints (mm): ≥21 susceptible; ≤20 resistant
on June 5, 2018 by guesthttp://aac.asm
.org/D
ownloaded from





























